Gajanan Maharaj College of Pharmacy, Chh, Sambhajinagar.
Rheumatoid arthritis is furthermost collective kind of inflammatory arthritis and a chief root of disability. Although it did not make it to European settlements until the 17th century, it had already been there for thousands of years among the first Native American populations. In the beginning, people thought that immune complexes and autoantibodies were the main culprits in the pathogenesis of RA. Independent of T-cells cytokine networks and T-cell-mediated antigen-specific responses are associated with aggressive tumor-like activity of rheumatoid synovium. The pathogenic factors of rheumatoid arthritis can inform the development of specific therapeutic techniques to decrease joint deterioration and inflammation in the synovium. Offers a thorough analysis of the psychological research on the causes, consequences, and management of rheumatoid arthritis (RA), a chronic condition with no known origin or cure that usually progresses in an unpredictable manner. There is also a succinct synopsis of the pertinent medical elements of RA. A review of the many effects of RA indicates that psychologists can contribute significantly to the creation of standardized evaluation methods to gauge the impact of RA.
An inflammatory autoimmune disorder known as RA can begin in tiny joints and spread to larger ones, as well as the skin, eyes, heart, kidneys, and lungs. It's a chronic condition that's symmetrical and inflammatory. Joint cartilage and bone are often destroyed, and ligaments and tendons degenerate as well [1]. The patient usually experiences excruciating pain as a result of the irregularities and bone erosion caused by all of this joint damage. Common symptoms of RA include subcutaneous rheumatoid nodules, fatigue, fever, decreased weight, and morning stiffness that lasts longer than thirty minutes in the affected joints. The average age of onset for this condition is 35–60, and it has the potential to both flare up and go into remission. Also affecting children younger than 16 years old, juvenile rheumatoid arthritis (JRA) is comparable to RA but lacks the rheumatoid factor [2-5]. In Western countries, RA affects an estimated 1% to 2% of the population [5,6,7]. Orthoarthritis (OA) usually shows up in the distal interphalangeal joint, although RA is more commonly observed in the proximal interphalangeal (PIP) and metacarpophalangeal (MP) joints in clinical practice. Wear and tear, not an inflammatory condition, is the main cause of OA, the most common form of arthritis. A person's immune system, cardiovascular system, or lungs are unaffected. In addition, OA typically impacts just one side of the body, in contrast to the symmetrical RA. Another telltale sign of RA is the morning stiffness that patients report, which typically persists for at least an hour. A common symptom of osteoarthritis is morning stiffness, which often subsides within twenty to thirty minutes [8,9]. Iconic representation of deformities in joints associated with rheumatoid disease. Hallux valgus manifests itself on the foot. Our goal in treating RA is to minimise joint discomfort and inflammation, maximise joint function, and protect joints from damage and deformity. Medications, weight training, education about the disease, and rest are all components of therapy programs. In most cases, the patient's needs and overall health are the determining factors in the treatment plan. This includes factors such as the progression of the disease, the joints that are impacted, age, overall health, occupation, adherence, and education about the disease [10,11].
Etiology
The etiology of RA remains a mystery. Viruses, hormones, genes, the environment, and the immune system could all have a role. The onset and progression of disease can be impacted by socioeconomic status, mental health, and lifestyle choices [12].
Genetic factor
A family history of RA accounts for 50% of the risk [13]. In the US, about 60% of people with RA share a similar epitope from the HLA-DR4 cluster. Peptides can connect to some HLA-DR molecules linked to RA, such as HLA-DR beta *0401, 0404, or 0405. This epitope is shared by HLA-DR1 (HLA-DR beta *0101), which makes some parts of southern Europe more likely to get sick. Different HLA-DR4 molecules, like HLA-DR beta *0402, don't have this epitope, so they don't protect [14]. Multiple genes are implicated, not only those belonging to the MHC complex. Genome sequencing in RA families has shown multiple genes, including PTPN22 and TRAF5, that can either protect against the disease or make it more severe [15,16]. Researchers have identified over 150 possible loci with RA-related polymorphisms; most of these are associated with seropositive disease [17]. There is a wide variety of disorders that manifest in children and adolescents, and among these is JRA, often called JIA. JIA is characterised by a lack of clear cause, starts before the age of 16, and lasts longer than six weeks. JIA is known to have complicated genetic features, with several genes playing a part in onset and symptoms of the disease [18]. There is evidence that the VTCN1 gene and the IL2RA/CD25 gene are JIA susceptibility loci [19]. Imprinting and epigenetics, according to some researchers, could form the basis of future RA treatments and research. Genetic imprinting from parents may play a role in manifestation of RA, since it is far more common in women than in males [20-23]. When a child's genes are imprinted, it's because the mother's genes express themselves differently than the father's genes due to differential chromosomal methylation in the parent of origin [24]. When environmental factors cause methylation changes in DNA rather than structural changes, this is known as epigenetics [17].
Infectious agents
Hormonal factors
More women than males experience RA, symptoms improve during pregnancy, reappear in early postpartum passé, and oral contraceptive users have a lower risk of developing the condition. One potential risk factor for RA is hyperprolactinemia [28].
Factors related to lifestyle and occupation
Primary existence peril factor for RA is tobacco smoking.
Smokers carrying two replicas of HLA-SE have a 40-fold increased chance of getting RA, highlighting the substantial impact of genetic variables on risk. The risk that a person has after quitting smoking might not go back to how it was before smoking for as long as twenty years [29].
These are some dietary risk factors for RA [29]:
Data from the Nurses' Health Study showed that a decreased incidence of RA was connected with a healthy lifestyle. Five aspects of a person's lifestyle were examined in the research: diet, exercise, BMI, smoking, and alcohol intake. An estimated 34% of RA cases may be prevented if people followed four healthy lifestyle variables, according to the population attributable risk estimate [30].
Occupational risk
Coal mining and other dusty occupations that expose workers to silica were found to be strongly associated with RA by Schmajuk et al. odds ratio for RA was 4.3 for individuals in group with the highest level of ergonomic exposure [31].
Pathophysiology
Joints and other affected organs are the primary sites of manifestation for RA, which mainly begins as a condition of chronic cellular activity that causes autoimmunity and immune complexes. Joint degeneration and inflammation of the synovial membrane are the main symptoms of the condition, and they are both caused by synoviocytes that resemble fibroblasts. There are three stages to RA progression, each marked by the involvement of distinct cytokines that cause tissue damage: initiation, amplification, and chronic inflammation [32-35].
Non-specific inflammation
Once set in motion, the mechanisms that allow for an abnormal immune response to continue and even become permanent [32]. These disorders impact the regulation of the adaptive immune response and are inherited. Cigarette smoking stands out among the many environmental and genetic factors that can increase the likelihood of RA [35,38]. Some environmental and hormonal factors, like postpartum anxiety and using hormonal drugs, may make women more likely to get cancer. Positive feedback mechanisms that typically maintain tolerance can be overridden by some antigens, such as IgG Fc bound by RAF and citrullinated fibrinogen coupled by antibodies to citrullinated peptides (ACPA, or anti-citrullinated protein antibody), leaving the immune system more susceptible. For thirty years, people have argued about the relative roles of T cell products and immunological complexes made by B cells in RA inflammation. Neither cell type is needed for inflammation, but autoantibodies against IgGFc (also called rheumatoid factors and ACPA) are, and ACPA is 80% accurate for diagnosing RA [38]. It is thought that antibodies that are not properly glycosylated cause RA and other inflammatory diseases to make joints swell [39].
Magnification in synovium
Plasma cells derived from B lymphocytes produce large quantities of rheumatoid factors and ACPA of the IgG and IgM classes once the systemic aberrant immune response has been set up; however, symptoms may not appear for years. Complement activates macrophages after connecting to the Fc receptor, exacerbating RA's already severe inflammation [40]. Due to alterations in the antibody's N-glycans that promote inflammation, autoreactive antibodies attach to Fc receptors in RA patients [39]. This exacerbates synovial inflammation by increasing joint oedema, vasoconstriction, and the recruitment of activated T-cells, namely CD4 in localized clusters and CD8 in more extensive infiltrates. Dendritic cells and synovial macrophages offer antigens that activate the immune response through the expression of MHC class II molecules [41].
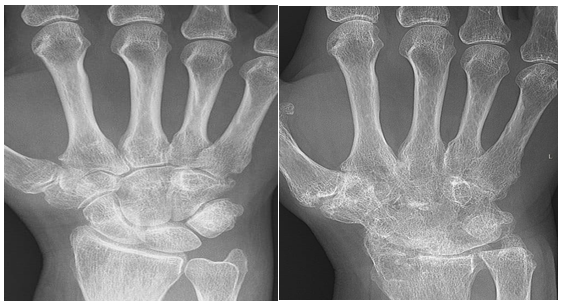
Fig. X-ray of a woman's wrist taken eight years after she began to experience rheumatoid arthritis
Pannus, which is characterized by extensive angiogenesis, enzymes that cause tissue destruction, and the development of granulation tissue at synovial lining edges are hallmarks of this disorder [42]. A rise in calprotectin levels is indicative of joint degeneration, synovial thickening, and underlying bone and cartilage breakdown [43]. Cytokines and chemokines attract and collect immune cells in the joint area. These cells include monocytes, activated fibroblast-like synoviocytes, and T- and B cells. The development of osteoclasts, which tear down bone tissue, is eventually caused by them through RANKL and RANK signaling [32]. The synovium's fibroblast-like synoviocytes in RA have a distinct phenotype in comparison to cells observed in healthy tissues. It is possible to identify characteristics that distinguish rheumatoid arthritis fibroblast-like synoviocytes from healthy ones, based on their aggressive nature and the impact these cells have on the joint environment. Rheumatoid arthritis synoviocytes, which resemble fibroblasts, have eight distinct features, four of which are cell-extrinsic and seven of which are cell-intrinsic. External to RA cells FLS features include an increase in osteoclasts and bone erosion, a function in cartilage breakdown, the development of new synovial blood vessels, and the recruitment and activation of immune cells [33].
Herbal Drugs used in rheumatoid arthritis [44]
|
Sr. No. |
Ingredients |
Purpose |
|
1. |
Aloe-vera Linn |
Anti-inflammatory |
|
2. |
Ashwagandha |
Insomnia |
|
3. |
Shallaki |
Anti-atherosclerotic |
|
4. |
Black pepper |
Pro-inflammatory cytokines |
|
5. |
Black cohosh |
Reduce inflammation |
|
6. |
Cats claw |
Reduce pain |
|
7. |
Ginger |
Reduce pain |
|
8. |
Turmeric |
Relieve symptoms of arthritis |
|
9. |
Milkweed |
Treating diarrhea |
|
10. |
Green tea |
Improve mental alertness |
|
11. |
Banyan tree |
Wound healing, Skincare |
|
12. |
Deodar cedar |
Anti- fungal fremedly and disinfectant |
|
13. |
Barringtonia |
Rid out intestinal worm |
|
14. |
Mango |
Treat heart stroke |
|
15. |
Tinospora gulancha |
Cancer, jaundice |
|
16. |
Night jasmine |
Reduces anxiety, Arthritis |
|
17. |
Indian sarsaparilla |
Detoxifying the body, Syphilis |
|
18. |
Chaste tree |
Menopause |
|
19. |
Abuta |
Migraine, joint pain |
|
20. |
Aginbuti |
Anti-arthritic activity |
Common Name- Lily of the desert, Curacao aloe
Biological Name- Aloe barbadense
Family- Liliaceae

Fig.1. Aloe.
Chemical constituents: Barbaloin, Aloe-emodin, anthranilic and aloetic acid, are anthraquinones found in aloe vera pulp, whereas 2′-O-feruloylaloesin and Aloe resin A are phenolic compound fractions found in aloe vera leaf skin.
Uses: Many skin issues, such as eczema, poison ivy, bruises, insect stings, and small cuts, could be alleviated with the help of aloe vera. Additionally, it has antifungal and antibacterial effects, and it purifies the blood, dilutes the urine, tones the uterus, stimulates spermatogenesis, induces laxation, reduces fever, and more. In Sprague Dawley rats, aloe vera extract reduced inflammation and arthritis when applied topically after adjuvant-induced arthritis.
Common Name- withania root, Winter cherry
Biological Name- Withania somnifea Linn.
Family- Solanaceae

Fig.2. Withania somnifera Linn.
Chemical composition- The primary medicinal secondary metabolites found in Ashwagandha are withanolides (steroidal lactones) and alkaloids. The most important component of the several alkaloids is withanine.
Uses- Animal and human studies on ashwagandha's effects on inflammation, anxiety, neurological disorders, and Parkinson's disease have yielded encouraging results. Ashwagandha, if consumed regularly, may inhibit or halt the progression of cancer in humans. Ageing, anaemia, arthritis, weariness, stress problems, and physical fitness are just some of the many health issues that it aids in addressing with progressive, long-lasting effects. In rats with adjuvant-induced arthritis, the anti-arthritic efficacy of withenia somnifera Linn., root powder when administered orally was seen.
Common Name- Boswellia/Indian Frankincense
Biological Name- Boswellia serrata Linn.
Family- Burseraceae

Fig.3. Boswellia serrata Linn.
Chemical composition- The only difference between alpha- and beta-boswellic acids, both of which have the molecular formula C30H48O3, is that the former has an additional hydroxyl group and the latter has a triterpene structure. One or more functional groups, a carboxyl group, and a pentacyclic triterpene characterise boswellic acids, an organic acid class.
Uses: Boswellia serrata extract has a natural anti-inflammatory activity in regions with prevalent chronic inflammation by suppressing the generation of pro-inflammatory cytokines and mediators. Arthritis patients taking non-steroidal anti-inflammatory drugs may experience accelerated joint damage because these drugs break down glycosaminoglycan synthesis. Boswellia serrata Linn., on the other hand, slows down this metabolism.
Common Name- Pepper
Biological Name- Piper nigrum Linn.
Family- Piperaceae

Fig. 4: Black pepper
Chemical composition: Black pepper is rich in volatile flavourings called terpenes, and it also contains nitrogen-containing compounds in its oils. The principal fragrance components of black pepper include myrcene, butyric acid, α- and β-pinene, α-phellandrene, linalool, limonene, methyl propanal, 2- and 3-methylbutanal, and 3-methylbutyric acid.
Uses- It has stimulating, stomachic, carminative, and fragrant properties. It causes more stomach juices to be secreted. Additionally, it makes some medications more bioavailable. Black pepper is separated from piperine. When piperine is taken orally for eight days at doses of 20 and 100 mg/kg/day, it reduces the symptoms of acute paw arthritis caused by carrageenan.
Common Name- Black snakeroot, bugwort
Biological Name- Actaea racemosa Linn.
Family- Ranunculaceae

Fig. 5: Actaea racemosa Linn.
Chemical composition: Caffeic acid, ferulic acid, isoferulic acid, hydroxycinnamic acids, and their compression products via glycolyl phenylpropanoids—also referred to as cimicifugic acids, such as fukinolic acid—are the main phenolic components of black cohosh.
Uses: Some of the many ailments it helps alleviate include arthritis, snake bites, kidney difficulties, diarrhea, dieresis, dyspepsia, and malaria. Additionally, it has insect-repellent properties. It helps with a lot of women's health issues, such menopause. Black cohosh can reduce the inflammatory symptoms of arthritis.
Common Name- Hawk's claw, saventaro
Biological Name- Uncaria tomentosa
Plant family- Rubiaceae

Fig. 6: Uncaria Tomentosa
Chemical composition: Aquamarine, corynanthidine, corynoxeine, cinchocaine, epicatechin, daucosterol, hirsutine, harmane, hirsuteine, lyaloside, Iso-pteropodine, loganic acid, oleanolic acid, mitraphylline, procyanidins, palmitoleic acid, rutin, pteropodine quinovic acid glycosides, rhynchophylline, speciophylline, sitosterol, stigmasterol, and strictosamides are some of the phytochemicals that can be found in it.
Uses: Cancer, HIV infection, stomach ulcers, Charon's disease, malignancies, diabetes, and chronic fatigue are among the conditions for which it is utilized. Additionally, it serves as an antibacterial agent.
Common Name- Giant Swallow Wort
Biological Name- Calotropis Procure Linn.
Family- Asclepiadaceae

Fig. 7: Calotropis procure Linn.
Chemical composition: Among the several biologically active chemical groups discovered in Calotropis obtain were cardenolidestannins, steroids, glycosides, terpenoids, phenols, sugars, flavonoids, alkaloids, and saponins.
Uses- Different parts of this plant have been said to have anti-inflammatory, pain-relieving, antioxidant, and antifungal qualities. The latex from this plant has strong anti-inflammatory effects on a number of animal models. The latex petroleum extract35 is very good at killing germs. It has been shown that rubber and its methanolic extract both stop inflammatory cells from getting in and stop oedema from different types of inflammation from getting worse. It also improves the ability of rats with monoarthritis that was caused by an experiment to move around.
Biological Name- Camellia sinensis Linn.
Family- Theaceae

Fig. 8: Camellia sinensis Linn.
Chemical composition: Flavanols, catechins, polysaccharides, proteins, alkaloids, saponins, spermidine derivatives, and anthocyanins are among the chemical substances present in tea blossoms.5 May suppression of TNFα, IFNγ, and COX-2, inflammatory mediators in 2024
Uses: (-) Green tea's most important catechin is epigallocatechin, which is a powerful antioxidant. It reduced frequency and strictness of collagen-induced arthritis.
Common Name- Banyan tree or Barga
Biological Name- Ficus bengalensis Linn.
Family- Moraceae

Fig. 9: Ficus bengalensis Linn
Chemical composition: significance in chemophenetic investigations. Many species of Ficus include bioactive secondary metabolites, such as phenolic compounds, ceramides, stilbenes, triterpenoids, xanthones, cerebrosides, and steroids.
Uses: The medicinal ingredients extracted from this plant are said to be quite beneficial for a number of ailments, including tonic, astringent, diabetic, leucorrhea, menorrhea, mental disorders, and dysentery. This group's bark, leaves, and fruits have anti-inflammatory, anti-septic, astringent, hemostatic, antioxidant, and anticancer properties.
Common Name- Marathi Deodar, Deva Daru, Cedar
Biological Name- Cedrus deodara
Family- Pinaceae

Fig. 10: Cedrus Deodara
Chemical composition: The two main components of the C. deodara samples were Atlantan (15.0-61.6%) and Himachalane (23.5-68.5%). The wood of C. deodara also included cis-α-bisabolene, oxidohimachalene, dehydro-ar-himachalane, himachalane oxide, and himachalol.
Uses: Since ancient times, rheumatoid arthritis and inflammation have been treated using Cedrus deodara wood in Ayurvedic medicine.
Marketed Formulation Available [45]:
REFERENCES






Sanika Gurav*, Shruti Choudhari, Shweta Patil, Tejasvini Kamble, Shradha Lokare, Dr. Jadge D. R., A Comprehensive Review of Insights into Rheumatoid Arthritis: From Pathophysiology to Herbal Remedies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2678-2689. https://doi.org/10.5281/zenodo.15655436
 10.5281/zenodo.15655436
10.5281/zenodo.15655436
