Bapatla College Of Pharmacy, Bapatla, Andhra Pradesh, India 522101
Polycystic Ovary Syndrome (PCOS) is a common and complex endocrine–metabolic disorder affecting women of reproductive age worldwide, characterised by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. Beyond reproductive impairment, PCOS is strongly associated with insulin resistance, obesity, dyslipidemia, psychological distress, and increased long-term cardiometabolic risk, making it a major public health concern. This systematic review synthesises evidence published over the past five years to provide an updated overview of the epidemiology, pathophysiology, diagnostic approaches, clinical manifestations, complications, and management strategies of PCOS. Recent literature highlights the heterogeneous nature of PCOS, arising from the interaction of genetic susceptibility, neuroendocrine dysregulation, insulin resistance, ovarian dysfunction, inflammation, and environmental factors. Variability in diagnostic criteria, including those from the Rotterdam, NIH, and AES definitions, contributes to inconsistent prevalence estimates and underdiagnosis, particularly in low- and middle-income countries. Clinical presentations range from classical reproductive symptoms to atypical and metabolic-dominant phenotypes, with a substantial psychological burden affecting quality of life. Management of PCOS requires an individualised and multidisciplinary approach, with lifestyle modification as first-line therapy, supported by pharmacological and fertility-directed treatments tailored to patient goals. Emerging applications of artificial intelligence show promise in improving diagnostic accuracy, risk prediction, and personalised treatment planning. Overall, this review underscores the need for early diagnosis, standardised diagnostic frameworks, holistic management, and continued research to reduce long-term complications and improve outcomes in women with PCOS.
Polycystic Ovary Syndrome (PCOS) is a multifaceted endocrine and metabolic disorder affecting women of reproductive age worldwide [1,9]. It is characterised by a combination of hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology, often accompanied by metabolic disturbances such as insulin resistance, obesity, and dyslipidaemia [3,5,8]. PCOS represents a significant public health concern due to its high prevalence and wide range of clinical manifestations that extend beyond reproductive health to include cardiometabolic and psychological comorbidities. Recent epidemiological analyses estimate that PCOS affects approximately 8–13% of women of reproductive age globally, with variations depending on diagnostic criteria and population studied[6,7,34].
Over the past five years, research on PCOS has intensified, aiming to clarify its pathophysiology, diagnostic challenges, long-term health consequences, and management strategies. Despite being one of the most common endocrine disorders in women, the etiology and underlying mechanisms of PCOS remain incompletely understood. Contemporary evidence suggests a complex interplay of genetic predisposition, environmental factors, metabolic dysfunction, inflammatory processes, and hormonal imbalances, with insulin resistance playing a central role in disease progression[5,25,36].
The heterogeneous nature of PCOS poses challenges in both clinical diagnosis and management. Multiple diagnostic criteria have been used internationally — including the Rotterdam, NIH, and Androgen Excess and PCOS Society (AES) definitions — which contribute to inconsistencies in prevalence estimates and clinical practice. Recent meta-analytic evidence, using various criteria, reports global prevalence rates ranging from approximately 5.5% to over 11%, underscoring the impact of diagnostic definitions on epidemiological findings [3, 7].
In addition to reproductive and metabolic dysfunction, PCOS is increasingly recognised for its psycho-social burden, influencing quality of life and mental health outcomes. Studies have linked PCOS with elevated risks of depression, anxiety, and other psychological stressors, highlighting the need for a holistic approach to care[20,30,31].
Emerging research over the recent years has also focused on novel diagnostic and predictive tools, including artificial intelligence (AI) applications that aim to improve diagnostic accuracy and risk prediction by integrating multimodal clinical and biochemical data. These advancements reflect a broader shift toward precision and personalised medicine in the research of PCOS[5,3].
Given the expanding body of literature, there is a clear need to systematically synthesise current evidence on PCOS to inform clinical practice, identify knowledge gaps, and guide future research priorities. This review therefore examines recent studies published over the past five years on PCOS, focusing on prevalence, diagnostic frameworks, pathophysiological insights, clinical outcomes, and emerging interventions.
Polycystic ovary syndrome (PCOS) is a complex, chronic endocrine–metabolic disorder affecting individuals of reproductive age. It is characterised by ovulatory dysfunction, clinical or biochemical hyperandrogenism, and/or polycystic ovarian morphology, with diagnosis established when at least two of these features are present after exclusion of related disorders[3,5]. PCOS is associated with disturbances in gonadotropin secretion, insulin signalling, and ovarian steroidogenesis, resulting in a broad spectrum of reproductive, metabolic, and psychological manifestations[5,8,26]]. Beyond menstrual irregularities and infertility, individuals with PCOS have an increased risk of insulin resistance, dyslipidemia, obesity, type 2 diabetes mellitus, and endometrial pathology, making PCOS a lifelong condition with multisystem involvement[9,16,20,41].
Epidemiology

Polycystic ovary syndrome (PCOS) is among the most frequently encountered endocrine disorders affecting individuals of reproductive age across the globe [1,6]. Epidemiological estimates indicate that PCOS affects a substantial proportion of this population; however, reported prevalence rates show considerable variability. This variation largely reflects differences in diagnostic criteria, population characteristics, study methodology, and geographic location[7,34].
Population-based studies generally report prevalence rates ranging from approximately 6% to 20% among reproductive-age women[6,7]. Studies applying stricter diagnostic definitions tend to yield lower prevalence estimates, whereas those using broader criteria identify a greater proportion of affected individuals. Hospital-based and clinic-based studies often report higher prevalence than community surveys, likely due to symptom-driven healthcare utilisation[10].
PCOS has been documented in diverse ethnic and racial groups worldwide, but its clinical expression and metabolic consequences differ between populations. Women from South Asian, Middle Eastern, and Hispanic backgrounds frequently demonstrate a higher tendency toward insulin resistance, dyslipidemia, and glucose intolerance, even at relatively lower body mass indices. Conversely, some East Asian populations exhibit lower rates of obesity but still show reproductive and endocrine abnormalities consistent with PCOS[16,48].
From an age perspective, PCOS often becomes apparent during adolescence or early adulthood, typically following menarche[19]. Menstrual irregularities, acne, and hirsutism are common early manifestations. As affected individuals age, the reproductive features may lessen, while metabolic complications, including impaired glucose tolerance, type 2 diabetes mellitus, and cardiovascular risk factors, become increasingly prominent[16,37].
Epidemiological evidence also suggests that PCOS remains significantly underdiagnosed, particularly in low- and middle-income countries. Limited access to healthcare services, lack of awareness, and sociocultural factors contribute to delayed diagnosis or non-recognition of the condition. Consequently, the true global burden of PCOS is likely underestimated.
Given its high prevalence, early onset, and association with long-term reproductive and metabolic morbidity, PCOS represents a major public health concern. Improved epidemiological surveillance, standardised diagnostic practices, and increased awareness are essential for accurate burden estimation and effective long-term management[33,34].
Etiology
Polycystic ovary syndrome (PCOS) is among the most frequently encountered endocrine disorders affecting individuals of reproductive age across the globe. Epidemiological estimates indicate that PCOS affects a substantial proportion of this population; however, reported prevalence rates show considerable variability. This variation largely reflects differences in diagnostic criteria, population characteristics, study methodology, and geographic location.
Population-based studies generally report prevalence rates ranging from approximately 6% to 20% among reproductive-age women. Studies applying stricter diagnostic definitions tend to yield lower prevalence estimates, whereas those using broader criteria identify a greater proportion of affected individuals. Hospital-based and clinic-based studies often report higher prevalence than community surveys, likely due to symptom-driven healthcare utilisation.
PCOS has been documented in diverse ethnic and racial groups worldwide, but its clinical expression and metabolic consequences differ between populations. Women from South Asian, Middle Eastern, and Hispanic backgrounds frequently demonstrate a higher tendency toward insulin resistance, dyslipidemia, and glucose intolerance, even at relatively lower body mass indices. Conversely, some East Asian populations exhibit lower rates of obesity but still show reproductive and endocrine abnormalities consistent with PCOS.
From an age perspective, PCOS often becomes apparent during adolescence or early adulthood, typically following menarche. Menstrual irregularities, acne, and hirsutism are common early manifestations. As affected individuals age, the reproductive features may lessen, while metabolic complications, including impaired glucose tolerance, type 2 diabetes mellitus, and cardiovascular risk factors, become increasingly prominent.
Epidemiological evidence also suggests that PCOS remains significantly underdiagnosed, particularly in low- and middle-income countries. Limited access to healthcare services, lack of awareness, and sociocultural factors contribute to delayed diagnosis or non-recognition of the condition. Consequently, the true global burden of PCOS is likely underestimated.
Given its high prevalence, early onset, and association with long-term reproductive and metabolic morbidity, PCOS represents a major public health concern. Improved epidemiological surveillance, standardised diagnostic practices, and increased awareness are essential for accurate burden estimation and effective long-term management.
The etiology of polycystic ovary syndrome (PCOS) is multifactorial and complex, involving an interplay of genetic susceptibility, neuroendocrine dysregulation, metabolic abnormalities, and environmental influences. Rather than arising from a single causative factor, PCOS develops through the interaction of multiple biological pathways that collectively disrupt normal ovarian and metabolic function.
Genetic predisposition plays a significant role in the development of PCOS. Familial clustering of the syndrome and higher concordance rates among first-degree relatives suggest a heritable component[5,7]. Multiple genes involved in androgen biosynthesis, insulin signalling, gonadotropin action, and ovarian follicular development have been implicated. However, PCOS is considered a polygenic disorder, with each genetic variant contributing modestly to disease risk rather than acting as a sole determinant[25].
Abnormal regulation of the hypothalamic–pituitary–ovarian axis is a central etiological mechanism in PCOS[. Increased frequency of gonadotropin-releasing hormone (GnRH) pulses favours excessive secretion of luteinizing hormone (LH) relative to follicle-stimulating hormone (FSH). This hormonal imbalance stimulates ovarian theca cells to produce excess androgens while impairing normal follicular maturation, leading to chronic anovulation[26,27].
Excess androgen production is a hallmark of PCOS and contributes both to its reproductive and metabolic manifestations. Androgens originate primarily from the ovaries, with a contributory role from the adrenal glands[17]. Elevated androgen levels disrupt folliculogenesis, promote follicular arrest, and manifest clinically as hirsutism, acne, and alopecia. Hyperandrogenism may also worsen insulin resistance, creating a self-perpetuating cycle [3].
Insulin resistance is a key etiological factor in many individuals with PCOS, affecting both obese and lean phenotypes. Compensatory hyperinsulinemia enhances ovarian androgen production and suppresses hepatic synthesis of sex hormone–binding globulin, thereby increasing circulating free androgens. Insulin resistance also contributes to the long-term metabolic complications associated with PCOS, including impaired glucose tolerance and type 2 diabetes mellitus[8,16,18].
Intrinsic ovarian abnormalities contribute to the etiology of PCOS. Increased sensitivity of ovarian theca cells to LH and insulin results in exaggerated androgen synthesis. Additionally, altered intra-ovarian signalling disrupts follicle selection and maturation, leading to the accumulation of small antral follicles characteristic of polycystic ovarian morphology[28,29].
Environmental and Lifestyle Factors
Environmental influences, such as dietary habits, sedentary lifestyle, obesity, and exposure to endocrine-disrupting chemicals, may exacerbate underlying genetic and hormonal susceptibilities[10,23]. Weight gain and central adiposity amplify insulin resistance and androgen excess, thereby worsening PCOS manifestations. Early-life factors, including prenatal androgen exposure, have also been proposed as contributors to disease development[24,46].
Inflammation and Oxidative Stress
Low-grade chronic inflammation and increased oxidative stress have been observed in individuals with PCOS. These factors may further impair insulin signalling, promote androgen excess, and contribute to cardiovascular risk, suggesting an additional pathogenic layer in the etiology of the syndrome[35,36].
Mechanism of Action (MOA) of Polycystic Ovary Syndrome (PCOS)
A single defect does not cause polycystic ovary syndrome (PCOS); rather, it develops through a network of interacting endocrine, metabolic, and ovarian mechanisms. The mechanism of action of PCOS explains how abnormalities in hormonal signalling and insulin metabolism lead to hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology.
The initiating mechanism in PCOS involves dysregulated gonadotropin-releasing hormone (GnRH) pulsatility from the hypothalamus. An increased frequency of GnRH pulses selectively stimulates excessive secretion of luteinizing hormone (LH) relative to follicle-stimulating hormone (FSH) from the anterior pituitary gland[4].
This hormonal imbalance increases the LH/FSH ratio, a characteristic biochemical feature of PCOS. Elevated LH overstimulates ovarian theca cells, initiating excessive androgen synthesis[26,27].
In PCOS, ovarian theca cells exhibit heightened sensitivity to LH and insulin, resulting in increased production of androgens such as testosterone and androstenedione. Upregulation of key steroidogenic enzymes enhances androgen biosynthesis beyond physiological levels.
Excess androgens disrupt granulosa cell function, impair estrogen conversion, and interfere with follicular maturation, thereby preventing ovulation[25,27].
Insulin resistance is a central mechanism in PCOS. Reduced insulin sensitivity in peripheral tissues leads to compensatory hyperinsulinemia. Elevated insulin levels act directly on the ovaries to:
This mechanism establishes a vicious cycle, where hyperinsulinemia worsens hyperandrogenism, which in turn aggravates insulin resistance[8,16,48].
Normal follicular development requires adequate FSH stimulation. In PCOS, relatively low FSH levels, combined with androgen excess, result in the arrest of follicle growth at the small antral stage[29].
Elevated intraovarian factors, particularly anti-Müllerian hormone (AMH), reduce follicular sensitivity to FSH. As a result, multiple immature follicles accumulate in the ovary, producing the classic polycystic appearance on ultrasound[30].
The arrested follicles fail to achieve dominance, preventing ovulation. Chronic anovulation leads to irregular or absent menstrual cycles and contributes to infertility. Persistent estrogen exposure without progesterone opposition also increases the risk of endometrial hyperplasia[18,42].
Adipose tissue dysfunction further modifies PCOS mechanisms. Increased visceral fat secretes abnormal levels of adipokines and inflammatory mediators, which:
Low-grade chronic inflammation acts as a reinforcing factor, sustaining metabolic and reproductive abnormalities[10,38].
Genetic susceptibility influences ovarian steroidogenesis, insulin action, and gonadotropin regulation. Environmental and epigenetic factors, such as prenatal androgen exposure and lifestyle changes, modulate gene expression, contributing to phenotypic variability in PCOS[5,26,49].
CASE STUDIES
Case Study 1: Typical PCOS With Menstrual Irregularity and Hyperandrogenism

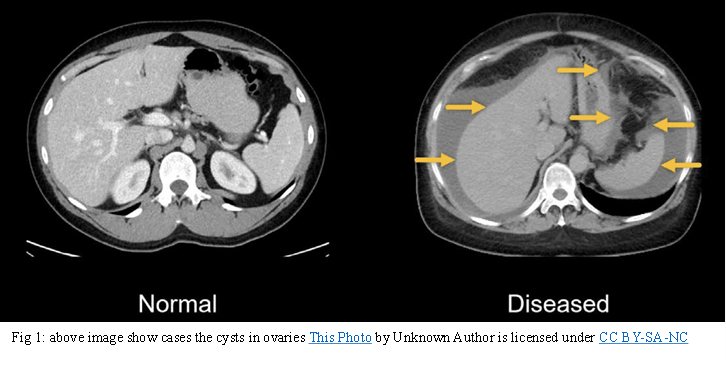
A 22-year-old female presented with complaints of irregular menstrual cycles since menarche, excessive facial hair growth, and acne. Physical examination revealed mild obesity and hirsutism. Laboratory investigations revealed elevated serum testosterone levels and an altered luteinizing hormone-to-follicle-stimulating hormone ratio. Pelvic ultrasonography revealed enlarged ovaries with multiple small peripheral follicles [1].
The patient was diagnosed with Polycystic Ovary Syndrome based on clinical, biochemical, and radiological findings. Lifestyle modification, along with hormonal therapy was initiated. After six months of treatment, the patient showed improvement in menstrual regularity and a reduction in androgen-related symptoms. This case highlights the classic presentation and positive response to early intervention in PCOS[18].
Case Study 2: PCOS With Severe Insulin Resistance and Obesity
A 28-year-old woman reported irregular menstruation, progressive weight gain, and fatigue. She had a family history of type 2 diabetes mellitus. Clinical examination revealed central obesity and acanthosis nigricans. Biochemical evaluation showed hyperinsulinemia, impaired glucose tolerance, and elevated androgen levels. Ultrasonography confirmed polycystic ovarian morphology.
The patient was managed with structured lifestyle intervention focusing on diet and physical activity along with insulin-sensitising therapy. Over a one-year follow-up period, significant improvements in insulin sensitivity, weight reduction, and menstrual regularity were observed. This case emphasises the strong association between PCOS and metabolic dysfunction[20].
Case Study 3: PCOS Presenting With Infertility
A 32-year-old woman presented with primary infertility for four years. She reported infrequent menstruation and weight gain. Hormonal analysis indicated anovulation and elevated androgen levels. Ultrasound examination revealed polycystic ovaries.
Initial management included lifestyle modification and ovulation induction therapy. Due to inadequate response, assisted reproductive techniques were employed with careful hormonal monitoring. The patient successfully conceived following individualised fertility treatment. This case demonstrates that infertility associated with PCOS can be effectively managed with a stepwise and personalised approach[21].
Case Study 4: Atypical PCOS Requiring Differential Diagnosis
A 19-year-old adolescent presented with rapidly progressive hirsutism, acne, and menstrual irregularity. Initial evaluation suggested PCOS; however, androgen levels were markedly elevated, and symptoms quickly progressed. Further endocrine evaluation and imaging were performed to rule out alternative causes of hyperandrogenism.
Advanced investigations identified a non-PCOS endocrine pathology contributing to androgen excess. Appropriate treatment led to the resolution of symptoms. This case highlights the importance of detailed evaluation and differential diagnosis in patients with atypical PCOS features[31].
Case Study 5: Psychological Impact of PCOS
A 25-year-old woman diagnosed with PCOS presented with anxiety, low self-esteem, and poor quality of life in addition to menstrual irregularities and weight gain. Clinical and laboratory findings confirmed PCOS. Along with medical and lifestyle management, psychological counselling was included in her treatment plan[50].
Over time, improvement was observed not only in physical symptoms but also in mental well-being and treatment adherence. This case emphasises the psychological burden of PCOS and the importance of holistic management[42].
Diagnosis of Polycystic Ovary Syndrome requires a comprehensive evaluation because no single test can confirm the condition. In addition to clinical assessment and ultrasound imaging, several other diagnostic measures are used to identify PCOS and rule out related disorders accurately.
A detailed clinical history is the first step in diagnosing PCOS. This includes evaluation of menstrual irregularities such as oligomenorrhea or amenorrhea, signs of hyperandrogenism including hirsutism, acne, and alopecia, and assessment of body weight and fat distribution. Family history of PCOS, diabetes, or metabolic disorders is also considered [3,18,36].
Hormonal profiling plays a key role in PCOS diagnosis. Commonly assessed hormones include luteinizing hormone (LH), follicle-stimulating hormone (FSH), total and free testosterone, and dehydroepiandrosterone sulfate (DHEAS). An increased LH to FSH ratio and elevated androgen levels support the diagnosis of PCOS. Thyroid hormones and prolactin levels are also measured to exclude other endocrine disorders that mimic PCOS[17,18,28].
Since PCOS is closely linked with metabolic dysfunction, biochemical investigations are essential. Fasting blood glucose, oral glucose tolerance test, insulin levels, and lipid profile are used to detect insulin resistance, dyslipidemia, and risk of diabetes. These tests help in identifying metabolic complications at an early stage[8,16].
A pelvic ultrasound is commonly used to assess ovarian morphology. The presence of enlarged ovaries with multiple small follicles arranged peripherally supports PCOS diagnosis. Transabdominal or transvaginal ultrasoography is selected based on patient age and marital status. Ultrasound findings are interpreted along with clinical and biochemical data [3,29].
Anti-Müllerian hormone levels are often elevated in women with PCOS due to increased follicle number. AMH serves as a useful adjunct diagnostic marker, particularly when ultrasound results are inconclusive. It also helps assess ovarian reserve and reproductive potential[29,30].
Several conditions share symptoms similar to PCOS. Therefore, diagnostic evaluation includes ruling out disorders such as congenital adrenal hyperplasia, Cushing’s syndrome, androgen-secreting tumours, thyroid dysfunction, and hyperprolactinemia. This step ensures accurate diagnosis and prevents inappropriate treatment[18,40].
Although not routinely used in clinical practice, genetic studies help identify susceptibility genes associated with PCOS. Molecular research contributes to understanding disease mechanisms and may support early identification in high-risk individuals[5,49].
H. AI-Assisted Diagnostic Tools
Artificial intelligence-based systems integrate clinical, biochemical, and imaging data to improve diagnostic accuracy. AI helps in early detection, especially in atypical cases, and reduces observer variability in ultrasound interpretation[55].
Women with PCOS are at increased risk of chronic anovulation, leading to infertility and subfertility. Prolonged menstrual irregularity may also increase the risk of endometrial hyperplasia and, in severe cases, endometrial carcinoma due to unopposed estrogen exposure. Recurrent pregnancy loss and pregnancy-related complications such as gestational diabetes and preeclampsia are also more common in women with PCOS[18,42,54].
PCOS is strongly associated with insulin resistance, obesity, and dyslipidemia. Over time, these metabolic abnormalities can progress to type 2 diabetes mellitus and metabolic syndrome. Long-standing insulin resistance may also increase the risk of non-alcoholic fatty liver disease and cardiovascular disorders[16,45,48].
Cardiovascular Risks
Women with PCOS often develop hypertension, abnormal lipid profiles, and chronic low-grade inflammation. These factors collectively increase the long-term risk of cardiovascular disease, including coronary artery disease and stroke, especially if preventive measures are not implemented early[14,38,45].
Chronic symptoms such as infertility, obesity, acne, and hirsutism can significantly affect mental health. Women with PCOS have a higher prevalence of anxiety, depression, and reduced self-esteem. If untreated, these psychological complications can negatively impact social functioning and treatment adherence[20,21,31].
Without appropriate management, androgen excess may worsen over time, leading to severe hirsutism, persistent acne, scalp hair thinning, and voice changes. These symptoms can become resistant to treatment in advanced stages[17,28].
Early identification of PCOS, especially in adolescents and young women, allows timely intervention. Regular monitoring of menstrual patterns, metabolic parameters, and hormonal levels helps prevent long-term complications [2, 36].
Lifestyle changes remain the cornerstone of PCOS prevention and management. Maintaining a balanced diet, engaging in regular physical activity, and achieving a healthy body weight can improve insulin sensitivity, restore ovulation, and reduce cardiovascular risk[12,24].
Routine screening for glucose intolerance, lipid abnormalities, and blood pressure should be conducted. Early detection of metabolic abnormalities enables prompt intervention and prevents disease progression[16,45].
Medications should be tailored according to patient symptoms and risk factors. Insulin-sensitising agents, hormonal therapy, and ovulation-inducing drugs should be used judiciously to prevent complications while minimising adverse effects[13,22,51].
Women of reproductive age should receive counselling regarding fertility planning, menstrual regulation, and pregnancy-related risks. Timely fertility intervention can improve reproductive outcomes[11,54].
Incorporating mental health assessment and counselling into PCOS management improves overall well-being and treatment compliance. Addressing psychological health is essential for long-term disease control[20,31,50].

Polycystic Ovary Syndrome (PCOS) presents with a wide range of clinical features that vary in severity among affected individuals. The symptoms involve reproductive, endocrine, metabolic, dermatological, and psychological systems.
Polycystic Ovary Syndrome (PCOS) is a chronic, multisystem disorder. Therefore, its management is individualised and depends on the patient’s symptoms, metabolic status, and reproductive goals. The treatment approach focuses on symptom control, prevention of complications, and improvement of quality of life.
Mechanism of Action
Lifestyle modification improves insulin sensitivity, reduces hyperinsulinemia, and lowers androgen production from the ovaries. Even modest weight loss helps restore ovulation and menstrual regularity.
Clinical Importance
Lifestyle intervention forms the foundation of all PCOS treatments and enhances drug effectiveness.
2. Treatment of Menstrual Irregularity and Hyperandrogenism[15,28]
A. Combined Oral Contraceptive Pills (COCPs)
Examples: Ethinyl estradiol + levonorgestrel / drospirenone
Mechanism of Action
Clinical Use
B. Anti-Androgen Drugs
I. Spironolactone
Mechanism:
Use:
II. Finasteride
Mechanism:
Use:
3. Treatment of Insulin Resistance and Metabolic Abnormalities[22,48]
I. Metformin (Insulin Sensitiser)
Mechanism of Action
Clinical Benefits
II. Thiazolidinediones (Less commonly used)
Example: Pioglitazone
Mechanism
4. Ovulation Induction and Infertility Treatment[11,54]
Mechanism of Action
Advantage
Mechanism
Use
Examples: FSH injections
Mechanism
Use
5. Treatment of Dermatological Symptoms[28]
6. Psychological and Emotional Support[20,31,50]
Management
Importance
7. Long-Term Prevention of Complications[33]
Preventive Measures
Artificial Intelligence (AI) is being increasingly utilised in healthcare to enhance disease diagnosis, prediction, and personalised management. In the context of Polycystic Ovary Syndrome (PCOS), AI has shown promising applications in early detection, accurate diagnosis, risk prediction, and treatment planning. Given the heterogeneous nature of PCOS, AI-based systems help overcome limitations of conventional diagnostic approaches.
Traditional PCOS diagnosis relies on clinical symptoms, hormonal tests, and ultrasonography, which may lead to delayed or incorrect diagnosis. AI models use machine learning algorithms to analyse large datasets containing clinical, biochemical, and imaging parameters.
By integrating features such as menstrual history, body mass index, hormone levels, and ovarian morphology, AI systems can identify PCOS patterns at an early stage. This is particularly useful in adolescents and women with borderline or atypical presentations, reducing misdiagnosis and delayed treatment.
AI is being used to enhance ultrasound interpretation by automatically detecting and counting ovarian follicles and assessing ovarian volume. Deep learning algorithms reduce observer variability and improve diagnostic accuracy.
In PCOS, where polycystic ovarian morphology is a key feature, AI-assisted imaging ensures consistent and objective evaluation, supporting clinicians in confirming diagnosis more reliably.
AI models can predict future complications of PCOS by analysing patient-specific risk factors. These systems evaluate patterns related to insulin resistance, obesity, lipid profile, and glucose metabolism.
Using predictive analytics, AI helps identify women at higher risk of developing type 2 diabetes, metabolic syndrome, cardiovascular disease, or infertility. Early risk prediction enables preventive interventions before complications occur.
AI supports personalized medicine by recommending individualized treatment strategies based on patient data. Machine learning algorithms analyze treatment responses from previous cases and predict which therapies are most effective for a specific patient.
This approach helps clinicians select appropriate lifestyle interventions, pharmacological therapies, or fertility treatments, improving outcomes and reducing trial-and-error prescribing.
In PCOS-related infertility, AI assists in optimizing ovulation induction protocols and assisted reproductive techniques. AI-based systems help determine optimal drug dosage, stimulation protocols, and timing of interventions.
This reduces the risk of complications such as ovarian hyperstimulation syndrome and increases the chances of successful conception.
AI-powered mobile applications and wearable devices are being developed to track menstrual cycles, physical activity, weight changes, and symptoms in women with PCOS. These tools promote patient engagement and self-management.
Continuous data collection allows real-time monitoring and timely medical intervention, improving long-term disease control.
With advancements in data science, AI has the potential to integrate genetic, hormonal, metabolic, and lifestyle data to create comprehensive PCOS risk profiles. AI-driven decision support systems may soon assist clinicians in standardised diagnosis, early prevention, and long-term follow-up.
CONCLUSION
Polycystic Ovary Syndrome (PCOS) is a complex, lifelong endocrine–metabolic disorder with heterogeneous clinical presentations affecting reproductive, metabolic, psychological, and cardiovascular health. This review highlights that PCOS arises from an intricate interaction of genetic susceptibility, neuroendocrine dysregulation, insulin resistance, hyperandrogenism, ovarian dysfunction, inflammation, and environmental factors. Variability in diagnostic criteria and clinical expression contributes to under diagnosis and inconsistent prevalence estimates, particularly in low- and middle-income countries, reinforcing the need for standardized diagnostic frameworks and improved awareness.Evidence consistently identifies insulin resistance and hyperandrogenism as central mechanisms linking reproductive dysfunction with long-term metabolic and cardiovascular complications. Case-based findings demonstrate the broad disease spectrum—from classical presentations to atypical forms requiring careful differential diagnosis—and emphasize the substantial psychological burden associated with PCOS. These insights confirm that PCOS is not merely a reproductive disorder but a multisystem condition requiring lifelong monitoring and comprehensive care. Effective management of PCOS necessitates an individualized, multidisciplinary approach, with lifestyle modification as the foundation and pharmacological and fertility-directed therapies tailored to patient needs. Early diagnosis, regular metabolic screening, and integration of psychological support are crucial to preventing long-term complications and improving quality of life. Emerging applications of artificial intelligence show promise in enhancing diagnostic accuracy, risk prediction, and personalized treatment planning. Future research should prioritize unified diagnostic criteria, long-term outcome studies, and validation of AI-based tools to reduce disease burden and advance precision medicine in PCOS care.
REFERENCES

Mule Venkatachennakesavareddy, Kolasani Venkata Ramaiah, Mandru Ramya Kumari, Unravelling the Complexity of Polycystic Ovarian Syndrome: A Systematic Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2776-2796. https://doi.org/10.5281/zenodo.18673305
 10.5281/zenodo.18673305
10.5281/zenodo.18673305
