Dr. CNS Institute of Pharmacy, Bhimavaram, India.
Precision medicine aims to tailor therapeutic interventions to the unique biological characteristics of individual patients, yet its success depends heavily on the ability to measure drug activity accurately and in real time. Pharmacodynamic (PD) biomarkers—objective indicators of a drug’s molecular or physiological effects—have emerged as essential tools for optimizing treatment selection, dosing strategies, and early assessment of clinical response. This work highlights current advances and challenges in the development, validation, and clinical integration of PD biomarkers across therapeutic areas, with a particular emphasis on oncology, immunology, and targeted therapies. We discuss innovative approaches leveraging multi-omics technologies, high-resolution imaging, and computational modeling to identify mechanistically relevant PD markers that reflect pathway modulation and therapeutic efficacy. Additionally, regulatory considerations, assay standardization, and the need for robust analytical and clinical qualification frameworks are explored as key determinants for successful translation. By unlocking reliable PD biomarker strategies, researchers and clinicians can enhance drug development efficiency, reduce trial failures, and ultimately realize the full potential of precision medicine in delivering safer, more effective, and patient-specific treatments.
Technological advancements in the molecular characterization of cancers have enabled researchers to identify an increasing number of key molecular drivers of cancer progression. These discoveries have led to multiple novel anticancer therapeutics, and clinical benefit in selected patient populations. Despite this, the identification of clinically relevant predictive biomarkers of response continues to lag behind. In this review, we discuss strategies for the molecular characterization of cancers and the importance of biomarkers for the development of novel antitumor therapeutics. We also review critical successes and failures in oncology, and detail the lessons learnt, which may aid in the acceleration of anticancer drug development and biomarker discovery.
The process of novel drug development from first-in-human studies to registration phase III clinical trials is associated with an unacceptably high attrition rate. Reversing such alarming trends requires rational patient and drug selection to achieve precision medicine in clinical studies. The recognition that intracellular processes drive multiple hallmarks of cancer, including angiogenesis, apoptosis, invasion and metastasis, has highlighted the potential to affect oncogenesis and cancer progression by manipulating these critical processes at a molecular level. Sequencing the cancer genome is a vital component to understanding the molecular basis of cancer; for example, tumor sequencing undertaken at an individual patient level can be utilized to identify specific molecular dependencies and vulnerabilities that may be targeted with antitumor therapies. The BCR-ABL translocation product in chronic myelogenous leukemia (CML), the anaplastic lymphoma kinase (ALK) mutation in lung cancer and the BRAF V600E mutation in melanoma are prime examples of specific subsets of cancers that are exquisitely sensitive to rationally selected molecularly targeted antitumor agents.
Cancer is a complex and heterogeneous disease, with multiple genetic, epigenetic, and environmental factors influencing tumor development. [1]
2. BIOMARKERS: DEFINITION AND TYPES
Definition
Biomarkers are measurable indicators or characteristics that can provide information about various biological processes in the body. They can be found in blood, urine, tissue samples, and even genetic material. These markers give us insight into the state of our health and can detect diseases, track progress, and guide treatment decisions.
Types of Biomarkers
Genetic Biomarkers: Unlocking the Code of Life
Genetic biomarkers delve into an individual’s DNA, offering a glimpse into their unique genetic makeup. These markers can identify genetic variations, mutations, and predispositions to certain conditions, paving the way for personalized medicine and targeted therapies.
Protein Biomarkers: The Messengers of Health
Proteins, the workhorses of the body, leave behind important clues about various physiological processes. Protein biomarkers, such as enzymes, antibodies, and hormones, are instrumental in diagnosing diseases, monitoring treatment responses and detecting conditions like cancer or cardiovascular disorders.
Metabolic Biomarkers: Insights into Body’s Chemical Symphon
Metabolic biomarkers provide a snapshot of the body’s chemical processes. These often found in blood or urine, offer valuable information about metabolic pathways can be crucial in conditions like diabetes or metabolic disorders.
Imaging Biomarkers: Visualizing Health
In the era of advanced medical imaging, imaging biomarkers play a vital role in visualizing and quantifying biological processes within the body. From identifying tumors to assessing organ function, these biomarkers contribute significantly to diagnostic accuracy.
Cellular Biomarkers: Tracking Cellular Health
Focusing on the microscopic level, cellular biomarkers assess the health of individual cells. Changes in cell structure, function, or expression can provide early indications of diseases, making cellular biomarkers essential in fields like cancer research and regenerative medicine.
These are used to detect the presence of a disease or condition. For example, the HER2 protein is a diagnostic biomarker for breast cancer. A high level of HER2 can indicate an aggressive form of the disease.
These biomarkers predict the likely outcome of a disease, such as the chance of recurrence or survival, regardless of the treatment received. A TP53 gene mutation is an example, as it can indicate a poor prognosis in some cancers.
These are used to predict how a patient will respond to a specific treatment. For instance, the KRAS mutation can predict that a patient with colorectal cancer will not respond to cetuximab therapy. This helps doctors choose the most effective treatment for a patient.
These biomarkers show the biological response to a therapy. They can be used to determine if a drug is having its intended effect. The Ki-67 proliferation index, which measures cell growth, is a pharmacodynamic biomarker; a decrease in this index after tamoxifen therapy indicates that the drug is working to slow cancer cell proliferation.
These are used to track the progression of a disease or to detect its relapse. Circulating tumor DNA (ctDNA) is an example used to monitor for the recurrence of cancer after initial treatment. Similarly, monitoring viral loads is crucial for managing chronic infections like hepatitis B. [2]
3. ROLE OF BIOMARKERS IN DRUG DEVELOPMENT
The 21st Century Cures Act, approved in the USA in December 2016, has encouraged the establishment of the national Precision Medicine Initiative and the augmentation of efforts to address disease prevention, diagnosis and treatment on the basis of a molecular understanding of disease. The Act adopts into law the formal process, developed by the FDA, of qualification of drug development tools, including biomarkers and clinical outcome assessments, to increase the efficiency of clinical trials and encourage an era of molecular medicine.
The FDA and European Medicines Agency (EMA) have developed similar processes for the qualification of biomarkers intended for use as companion diagnostics or for development and regulatory approval of a drug or therapeutic.
Biomarkers that are used exclusively for the diagnosis, monitoring or stratification of patients in clinical trials are not subject to regulatory approval, although their qualification can facilitate the conduct of a trial. In this Review, the salient features of biomarker discovery, analytical validation, clinical qualification and utilization are described in order to provide an understanding of the process of biomarker development and, through this understanding, convey an appreciation of their potential advantages and limitations.
A biomarker is a characteristic that is objectively measured and evaluated as an indicator of a normal biological process, a pathological process or a biological response to a therapeutic intervention. Biomarkers increase the success rate of drug development programmes and there by accelerate the availability of new therapeutics.
Biomarker development is a multistep and iterative process beginning with biomarker discovery in disease and non-disease samples. The analytical validation phase of biomarker development is characterized by analysis of the performance metrics of the biomarker to ensure that the test is reliable, reproducible and of adequate sensitivity and specificity. Qualification is a graded evidentiary process that links a biomarker with biological and clinical end points. Utilization of biomarkers for clinical applications is dependent on their clinical utility for disease diagnosis, disease staging and treatment selection. Biomarkers accelerate oncology drug development by reducing costs and improving success rates.
Target Identification:
Determines which molecules or pathways are critical for tumor growth.
4. IMPORTANCE OF PHARMACODYNAMIC BIOMARKERS
Pharmacodynamic Biomarkers
As clinical trials are designed for increasingly smaller, molecularly defined patient populations, PD biomarkers are likely to grow in importance. In particular, PD studies may provide insights into optimal biologic dosing, toxicity, and proof of mechanism for targeted therapies.
Serial tumor biopsies. Ideally, PD studies are performed directly on tumor specimens, allowing investigators to evaluate the functional and molecular effects of targeted agents within the tissue of interest. As illustrated in Table 1, PD endpoints may include assessments of protein phosphorylation markers, measures of cellular proliferation/apoptosis, cell-cycle regulation biomarkers, and epigenetic changes
Importance of Pharmacodynamic (PD)
Biomarkers Pharmacodynamic biomarkers measure a drug’s effect on the body. The image highlights four main reasons for their importance:
Early Drug Evaluation:
PD biomarkers can indicate whether a drug is having its intended effect on the target pathway, even before physical changes like tumor shrinkage are visible. This allows for earlier and more efficient assessment of a drug’s potential efficacy.
Reduced Adverse Effects:
By using PD biomarkers, doctors can determine the minimum effective dose of a drug, which helps to avoid unnecessarily high doses that could lead to severe side effects.
Guides Combination Therapy:
Biomarker data can reveal which biological pathways are active or inhibited by a drug. This information is valuable for selecting complementary drugs that target different pathways, leading to more effective combination therapies.
Supports Personalized Medicine:
Because each patient’s disease, such as a tumor, is unique, PD biomarkers can help guide the selection of the most appropriate therapy for an individual patient, moving beyond a one-size-fits-all Biomarkers are crucial in healthcare for detecting diseases early, predicting outcomes, tailoring treatments to individual patients, and monitoring treatment effectiveness by measuring biological processes, genes, or substances in the body. They facilitate personalized medicine, drug development by evaluating drug efficacy and safety, and public health by understanding disease risk and environmental impacts. [4]
5. DEVELOPMENTAL STAGES OF PD BIOMARKER
Model-based drug development (MBDD) is recognized as an initiative able to improve success rates in the development of new anti-cancer agents. The use of pharmacodynamic (PD) biomarkers may be valuable in this context. The implementation of biomarkers in MBDD in oncology is the subject of this review.
Methods:
Literature was searched for articles and relevant conference abstracts concerning application of biomarkers in MBDD in oncology. First, papers are discussed concerning the use of biomarkers in modeling and simulation analyses in preclinical and early clinical phases of drug development. Subsequently, articles concerning late-stage clinical drug development are discussed.
Results:
Only a limited set of articles and conference presentations were identified. As expected, the majority of publications are concerned with targeted anti-cancer drugs. In the early development of novel anti-cancer agents, most publications concerned to the evaluation of dosing regimens for further clinical evaluation, or the identification of the required levels of target modulation. In general, combined analysis of clinical and preclinical data provide the most informative analyses. The use of biomarkers in late-stage drug development has mainly been confined to the prediction of phase III outcome on the basis of tumor growth data obtained from phase II trials, with tumor growth as biomarker for outcome.
Biomaeker Development Process
Target Identification:
The first step involves selecting specific genes or proteins that are critical for the survival of cancer cells. Examples include HER2, EGFR, and VEGF. These targets are chosen because they play a significant role in the disease and can be used to monitor its progression or a patient’s response to treatment.
Biomarker Discovery:
This stage uses advanced “omics” technologies, such as genomics, proteomics, and metabolomics, to find potential biomarkers. These technologies analyze large sets of biological molecules to identify candidate biomarkers that show a difference between diseased and healthy states.
Preclinical Validation:
Once a biomarker is promising in preclinical studies, it is confirmed in patient samples to ensure it correlates with the treatment outcome. This step is crucial for determining the biomarker’s clinical utility.
Assay Standardization & Qualification:
This final stage ensures the test for the biomarker is reliable and reproducible. The assay is validated by regulatory bodies like the FDA and EMA to ensure its accuracy and consistency.[5]
6. TECHNIQUES USED IN BIOMARKER DEVELOPMENT
Technical considerations regarding the analytical set up for biomarker development.
The complexity of the biological fluid may generate a need for a combination of different techniques such as fractionation approaches. In general, the basic requirements of the methodology that is selected are: simplicity of use, robustness, high accuracy and performance.
The biomarker workflow can be divided into 3 main parts:
Discovery, verification and validation.
Depending on the specific aim of the study, various proteomic platforms can be applied from the unbiased discovery setting to the targeted quantification in the verification and validation stages. The basic characteristics of the objectives and platforms that can be employed at the different stages a technical description of the available proteomic technologies for discovery, verification and validation stages is presented, together with certain recent applications particularly in the field of clinical proteomics in the quest of bladder cancer.
There are a variety of bio-molecules which are used as biomarkers including antigens, DNA, mRNA, and enzymes. However, protein biomarkers are the most common type of biomarkrs used in medical diagnostics. Therefore this article is focused on the use of antigens as biomarkers and their detection technologies. Biomarkers are present in tumour tissues, serum, and other body fluids. The ultimate goal of researchers in the field of biomarker detection is to develop a reliable, cost-effective, powerful detection tool for prognosis, diagnosis, and monitoring the recurrence of a particular disease. Furthermore, biomarkers can also be used for the follow-up of a treatment by monitoring the constant decrease in its concentration to a certain level. There has been huge progress in the field of biomarker detection technologies. Various biomarker detection methods based on highly specific recognition biomarkers have been developed. The enzyme-linked immunosorbent assay (ELISA), gel electrophoresis, surface plasmon resonance (SPR), Mass-sensing BioCD protein array, surface enhanced Raman spectroscopy (SER colorimetric assay, electrochemical assay, and fluorescence methods, are few of the biomarker detection methods. Many of these methods are based on the conventional immunoassays in which a capture antibody is functionalized on a solid support for target capture and a reporter antibody for assay read-out. These technologies suffer from a common drawback of nonspecific adsorption of non-target proteins onto the surface of a bio-sensor.
Considering the enormous number of antigens used for the diagnosis of various diseases and disorders it is impractical to review all of them. Furthermore, even though the antigens have different sizes, shapes, and stability profiles the technologies used for their detection are common. Therefore, in this article we have focused on the technologies and methods used for the detection of biomarkers for the diagnosis of prostate cancer (Pca). It is evident from many observations that the recurrence rate of cancer is very high in patients after radical prostactomy The PSA levels 4 ng mL−1 and lower are considered as normal. After radical Prostactomy these levels drop much below 1 ng mL−1, however in recurring cancer the level of PSA starts to increase again. Therefore, for accurate diagnosis and treatment follow-up it is essential for a biomarker detection technology to allow the detection of a concerned biomarker at a very low concentration such as far below 100 pg mL−1.
The ultimate goal behind the use of biomarkers for diagnosis is to develop reliable and cost-effective powerful detection tools for early diagnosis of diseases and disorders. Therefore, by using biomarker detection technologies, physicians can choose precise and accurate therapy for their patients. Furthermore, it can help physicians to effectively monitor the disease progression, and recurrence. There are several reports on the various biomarkers evaluated for their diagnostic and prognostic values in the Pca diagnosis. The biomarker genes evaluated for diagnosis of Pca includes the prostate cancer antigen 3 (PCA3) gene and the transmembrane protease serine 2 (TMPRSS2-ERG) gene. The biomarker proteins evaluated for the diagnosis of Pca include early prostate cancer antigen-2 (EPCA-2), human glandular kallikrein (hK2), cluster of differentiation 147 (CD 147), acid phosphatase (PAP), and prostate specific antigen (PSA), respectively . [5]
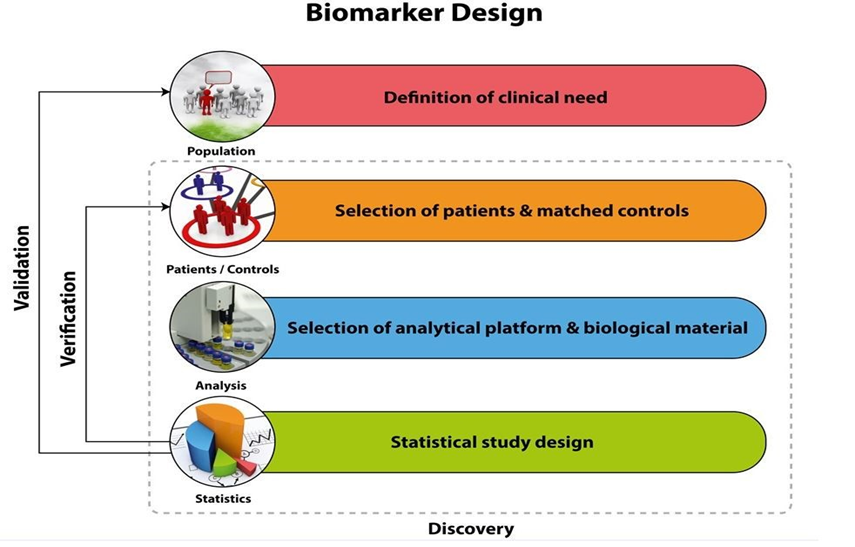
Fig 1.Technical used in Biomarker [1]
7. VALIDATION AND QUALIFICATION OF PD BIOMARKERS
In a recent publication, analytical method validation of three different PD biomarker assays was reported: quantitative RT–PCR (qRT–PCR) for XIAP mRNA expression, Western blot analysis for XIAP protein expression, and a novel plasma Elisa assay (M30 Apoptosense) as a surrogate marker of tumour cell apoptosis (Cummings et al, 2005). During that study method validation was conducted in accordance with available internationally recognised bioanalytical guidelines established by the pharmaceutical industry, but primarily utilised in drug and safety monitoring (Shah et al, 2000; Miller et al, 2001). There is a growing acknowledgement that these guidelines are not sufficiently flexible to accommodate the many different categories of PD assays that are employed during anticancer drug development of molecularly targeted agents (Lee et al, 2005). It is now also evident that qualification of a biomarker is a multistage process requiring a concerted team effort often paralleling the drug development cycle (Colburn, 2003; Benowitz, 2004; Ransohoff, 2004; Ludwig and For PD biomarker assays at least four distinct categories were identified each requiring evaluation of a different set of performance criteria: definitive quantitative (e.g. mass spectrometry), relative quantitative , quasiquantitative (e.g. qRT–PCR) and qualitative (e.g. immunohistochemistry) A vital component in PD biomarker validation is the establishment of its pretreatment range and inherent biovariability, in order to assess the likelihood that the technology of choice and trial design have the statistical and technological resolving power to discriminate between normal background biologic variation and a drug-induced In the present paper, analytical validation of a fourth PD assay, the M65 Elisa is described, along with long term stability studies on the antigens for this assay as well as for M30 Apoptosense . In addition, an evaluation of predose biomarker variability in cancer patients is presented for the M30 and M65 cell death Elisa’s and a qRT–PCR method for XIAP mRNA [6]
Although many imaging biomarkers have been described for cancer research, few are sufficiently robust, reliable and well-characterised to be used as routine tools in clinical cancer research. In particular, biomarkers which show that investigational therapies have reduced tumour cell proliferation, or induced necrotic or apoptotic cell death are not commonly used to support decision-making in drug development, even though such pharmacodynamic effects are common goals of many classes of investigational drugs. Moreover we lack well-qualified biomarkers of propensity to metastasise. The qualification and technical validation of imaging biomarkers poses unique challenges not always encountered when validating biospecimen biomarkers. These include standardisation of acquisition and analysis, imaging-pathology correlation, cross-sectional clinical–biomarker correlations and correlation with outcome. Such work is ideally suited to precompetitive research and public–private partnerships, and this has been recognised within the Innovative Medicines Initiative (IMI), a Joint Undertaking between the European Union and the European Federation of Pharmaceutical Industries and Associations, which has initiated projects in the areas of drug safety, drug efficacy, knowledge management and training.
This section outlines three types of validation:
Analytical Validation:
Focuses on the accuracy, precision, sensitivity, and specificity of the assays.
Clinical Validation:
Establishes the correlation between biomarker changes and clinical outcomes.
Regulatory Qualification:
Requires biomarkers to be approved by regulatory bodies like the FDA or EMA for development. An example given is the FDA-approved PD-L1 assay for guiding . [7]
8. APPLICATIONS OF PD BIOMARKERS IN ONCOLOGY
Biomarker Identification:
Biomarkers are indispensable for identifying the mechanisms underlying a disease to find potential new therapeutic crucial targets. They can be used to screen healthy patients for malignancy, estimate the prognosis, predict the outcome from therapy, and monitor disease. In accordance with the National Cancer Institute definition, “a biomarker is a biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process, or of a condition or disease”. It may be used to see how well the body responds to a treatment of a the disease or condition, which is called molecular marker or a signature molecule. Moreover, it can be useful in epidemiology to reduce misclassification of exposures and disease, enhance detection of exposure-disease associations, or increase opportunities for intervention, ultimately turning examination findings into a practical application to public health. Identifying and describing biomarkers will help with formulating detailed biomarker descriptions, such as the specific analyte (e.g., fibrinogen), anatomic feature (e.g., joint angle), or physiological characteristic (e.g., blood pressure) that is measured. If applicable (e.g., for molecular biomarkers), the unique identifier of the the biomarker can be described [6, 24]. It has become a powerful tool to classify the risk of progression, identify the severity of the disease, and guide therapy. In addition, biomarkers can be used as indicators of the safety and efficacy of therapeutic interventions
Biomarker discovery and development are popular for detecting the subtle diseases. However, biomarkers are needed to be validated and approved, and even fewer are ever used clinically. Imaging biomarkers have a crucial role in the treatment of cancer patients because they provide objective information on tumor biology, the tumor’s habitat, and the tumor’s signature in the environment. Tumor changes in response to an intervention complement molecular and genomic translational diagnosis as well as quantitative information. Neuro-oncology has become more prominent in diagnostics and targeted therapies.
Biomarker Identification
Biomarkers are indispensable for identifying the mechanisms underlying a disease to find potential new therapeutic crucial targets. They can be used to screen healthy patients for malignancy, estimate the prognosis, predict the outcome from therapy, and monitor disease. In accordance with the National Cancer Institute definition, “a biomarker is a biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process, or of a condition or disease”. It may be used to see how well the body responds to a treatment of a the disease or condition, which is called molecular marker or a signature molecule. Moreover, it can be useful in epidemiology to reduce misclassification of exposures and disease, enhance detection of exposure-disease associations, or increase opportunities for intervention, ultimately turning examination findings into a practical application to public health. Identifying and describing biomarkers will help with formulating detailed biomarker descriptions, such as the specific analyte (e.g., fibrinogen), anatomic feature (e.g., joint angle), or physiological characteristic (e.g., blood pressure) that is measured. If applicable (e.g., for molecular biomarkers), the unique identifier of the biomarker can be described. It has become a powerful tool to classify the risk of progression, identify the severity of the disease, and guide therapy. In addition, biomarkers can be used as indicators of the safety and efficacy of therapeutic interventions or new pharmacological treatments in clinical trials. Several types of biomarker measurements can refer to characteristics such as molecular, physiologic, histologic, and radiographic characteristics. Additionally, these attributes can be objectively estimated and evaluated as an index of normal biological and pathogenic processes or pharmacological responses to a therapeutic intervention. According to the FDA-NIH Biomarker Working Group definition, biomarker categories follow alongside the clinical continuum from prediagnosis of disease (prevention), pretreatment (personalized in precision medicine), and even to posttreatment (outcomes and endpoints) as the basis for clinical guidance application a representative categories placed along this continuum order, and
Categories of biomarkers and diseases for which different markers have clinical relevance
Diagnostic biomarkers
From the 2016 WHO classification of CNS diseases, the 2021 WHO update makes substantial progress in the classification and treatment of gliomas, incorporating several molecular parameters in addition to the histopathology of formerly and newly defined molecularly defined entities. For instance, isocitrate dehydrogenase (IDH) mutations have different attributes with diagnostic clarity to ensure optimal management and essential regulations for defining clinical trial populations. Assigning the molecular heterogeneity of gliomas and classifying them into dissimilar clinical groups based on codeletion of chromosome arms 1p/19q, IDH mutations, and telomerase reverse transcriptase (TERT) promoter mutations that are characterized by different mechanisms of pathogenesis is important. Previously, glioblastoma (GBM), including both IDH wild-type (90%) and IDH-mutated (10%) tumors, were diagnosed as one entity despite their dissimilar biology and prognosis. Now, diagnostic GBM IDH wild-type diffuse astrocytic tumors in adults only retain one or more of the following three genetic parameters: mutations in the promoter of the TERT, epidermal growth factor receptor (EGFR) gene amplification (tumor-specific aberrations), or both gain of entire chromosome 7 and loss of the entire chromosome 10. Generally, these tumors will be classified as GBM because the of release of circulating tumor cells is associated with EGFR gene amplification, indicating that hematogenous GBM spread out is an intrinsic feature of GBM biology .In addition, the promoter methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) gene has been suggested as the most important predictor of the chemotherapeutic response and patient survival in GBM. Determining MGMT promoter methylation status by multiparametric MRI would help to preoperatively determine the surgical and overall treatment strategy. Diagnostic biomarkers are the key elements to diagnose a disease or a pathogenic process through monitoring situations. It not only serves as a predictive or prognostic marker to support precision medicine but also identifies different subpopulations of patients most likely to benefit from predetermined treatments.
Monitoring biomarkers
Safety and non-invasiveness are measured continuously or sequentially to detect a changes in the different grades of disease (e.g., imaging). Disease progression and the response of a condition to a treatment, either favourable or unfavourable, the occurrence of new disease effects, can be detected by biomarkers of many categories, e.g., safety biomarkers, pharmacodynamic/response biomarkers, and prognostic biomarkers. These biomarkers would then be used to make treatment decisions and surveil the disease. MRI examination is a routine work and requisite modality for various studies to monitor disease status, especially before surgery and after treatment in neuro-oncology. The 2015 consensus recommendations for a standardized brain tumor imaging protocol in clinical trials have been developed to help researchers utilize imaging for validation in order to use quantitative imaging surrogates as endpoints in clinical trials for GBM drugs. Moreover, making the best use of different pulse sequences of MR imaging acquisition will further elucidate the tumor’s progress and has the potential to improve treatment evaluation with overall survival as the key endpoint. Several studies have shown that circulating tumor cells have been identified in many tumor types and may be perceived in GBM patients. Circulating biomarkers, such as circulating tumor cells, extracellular vesicles and circulating tumor DNA from liquid biopsy are quick, minimally invasive, highly sensitive, and lower-cost samples with the potential non-to help control the treatment of patients with GBM. Tumors shed tumoral content, for instance, circulating tumor cells, cell-free nucleic acids, extracellular vesicles, and proteins, into the circulation, and these biomarkers can cross the blood–brain barrier. Circulating RNAs have been detected in the blood and CSF of glioma patients and may act as biomarkers for diagnosis, prognosis, and treatment monitoring.
Pharmacodynamic biomarkers / Response biomarkers
In recent decades, tumor immunotherapy has shown promise by virtue of its extraordinary efficacy in treating cancer, which has been enabled by the increasing use of molecular imaging. Recently, neoantigen?based vaccines have demonstrated potential for cancer therapy, primarily by augmenting T?cell responses. Additionally, targeted radionuclide therapy, namely, molecular radiotherapy, involves a radioactive drug or a radiopharmaceutical that targets cancer cells to assess disease at the molecular level, allowing individual diagnosis. PET imaging can be used in diagnostic settings to identify multimodal molecular and metabolic processes and combines the transport and cellular mechanism of routinely used PET tracers in many neurological diseases, in diagnosis and in the guidance of targeted therapy. This molecular imaging modality is used to examine and reveal human
physiology through the detection of positron-emitting radiation.[8]
9. EXAMPLES OF PD BIOMARKERS IN CANCER TREATMENT
Examples of Biomarker Applications
Cancer Diagnostics: Detecting Early Signs for Better Prognosis
Biomarkers have become indispensable in cancer diagnostics. For instance, elevated levels of prostate specific antigen (PSA) serve as a biomarker for prostate cancer, enabling early detection and timely intervention. Similarly, HER2/neu status in breast cancer is determined through biomarker testing, guiding the choice of targeted therapies for more effective treatment.
Cardiovascular Health; Monitoring with Troponin and B-type Natriuretic Peptide (BNP)
In cardiovascular medicine, troponin and BNP are examples of biomarkers used to assess heart health. Elevated troponin levels indicate heart muscle damage, aiding in the diagnosis of conditions like heart attacks. BNP, on the other hand, helps in evaluating heart failure and guiding appropriate treatment strategies.
Diabetes Management: Glycated Hemoglobin (HbA1c) as a Key Biomarker
Glycated Hemoglobin (HbA1c) is a vital biomarker in diabetes management. It provides a long-term average of blood sugar levels, offering insights into how well glucose is controlled over time. This biomarker is crucial in tailoring treatment plans and reducing the risk of diabetes-related complications.
Alzheimer’s Disease Research: Amyloid Beta and Tau Proteins
Biomarkers play a crucial role in Alzheimer’s disease research. Levels of amyloid beta and tau proteins in cerebrospinal fluid or blood serve as indicators of neurodegenerative changes. These biomarkers aid in early diagnosis, tracking disease progression, and evaluating the efficacy of potential treatments.
Infectious Disease Detection: PCR and Viral Load as Biomarker Tools
Polymerase Chain Reaction (PCR) and viral load measurements are biomarker applications extensively used in infectious disease diagnostics. They enable the detection of viral or bacterial genetic material, facilitating accurate and rapid identification of pathogens, crucial in managing outbreaks and pandemics.[9]
Applications of PD Biomarkers in Oncology:-
The image expands on five key applications:
Examples of PD Biomarkers in Cancer Treatment
The image provides specific examples of biomarkers, the drugs they are associated with, the cancer type they are used for, and their mechanism or role:
10. CASE STUDIES OF APPROVED BIOMARKERS
The notes provide three case studies of approved biomarkers and their clinical use:
Personalized Medicine
The document explains the expanded role of biomarkers in personalized medicine:
Example: Monitoring ctDNA in colorectal cancer allows doctors to switch to alternative drugs early if the initial treatment is not working, before the tumor progresses.
This review focuses on molecular biomarkers in drug development. It contains sections on how biomarkers are used to assess target engagement, pharmacodynamics, safety, and proof-of-concept. It also covers the use of biomarkers as surrogate end points and patient selection/companion diagnostics and provides insights into clinical biomarker discovery and biomarker development/validation with regulatory implications. To survey biomarkers used in drug development—acknowledging that many pharmaceutical development biomarkers are not published—we performed a focused PubMed search employing “biomarker” and the names of the largest pharmaceutical companies as keywords and filtering on clinical trials and publications in the last 10 years. This yielded almost 500 entries, the majority of which included disease-related (approximately 60%) or prognostic/predictive (approximately 20%) biomarkers. A notable portion (approximately 8%) included HER2 (human epidermal growth factor receptor 2) testing, highlighting the utility of biomarkers for patient selection. The remaining publications included target engagement, safety, and drug metabolism biomarkers. Oncology, cardiovascular disease, and osteoporosis were the areas with the most citations, followed by diabetes and Alzheimer disease.
Interest is increasing rapidly in the use of surrogate markers as primary measures of the effectiveness of investigational drugs in definitive drug trials. Many such surrogate markers have been proposed as potential candidates for use in definitive effectiveness trials of agents to treat neurologic or psychiatric disease, but as of this date, there are no such markers that have been adequately “validated,” that is, shown to predict the effect of the treatment on the clinical outcome of interest. While the current law and regulations permit the United States Food and Drug Administration to base the approval of a drug product on a determination the effect of the drug on an unvalidated surrogate marker (that is, one for which it is not known that an effect on the surrogate actually predicts the desired clinical benefit), there are a number of difficulties in interpreting trials that use surrogate markers as primary measures of drug effect. In this article, the relevant regulatory context will be discussed, as well as the epistemological problems related to the interpretation of clinical trials in which unvalidated surrogate markers are used as primary outcomes.[10]
11. ROLE IN PERSONALIZED MEDICINE
Biomarkers help to identify which patients will respond to a particular treatment (responders vs. non-responders). This approach reduces unnecessary treatment and toxicity, and enables the use of tailored combination therapies. An example provided is using circulating tumor DNA (ctDNA) to monitor colorectal cancer, which allows for an early switch to alternative drugs if needed.
Use of AI and Omics:
Artificial intelligence and machine learning are used to predict a patient's response to treatment based on biomarker patterns. Multi-omics combines different types of biological data (genomics, proteomics, metabolomics) for better predictions. The image also mentions digital pathology, where AI assists in scoring biomarkers from tissue slides, such as predicting PD-L1 expression.
Challenges in Biomarker Development:
The image briefly mentions "Tumor Heterogeneity" as a challenge, which refers to the fact that different areas of a tumor can have different characteristics.
Cancer is a devastating disease that takes the lives of hundreds of thousands of people every year. Due to disease heterogeneity, standard treatments, such as chemotherapy or radiation, are effective in only a subset of the patient population. Tumors can have different underlying genetic causes and may express different proteins in one patient versus another. This inherent variability of cancer lends itself to the growing field of precision and personalized medicine (PPM). There are many ongoing efforts to acquire PPM data in order to characterize molecular differences between tumors. Some PPM products are already available to link these differences to an effective drug. It is clear that PPM cancer treatments can result in immense patient benefits, and companies and regulatory agencies have begun to recognize this. However, broader changes to the healthcare and insurance systems must be addressed if PPM is to become part of standard cancer care.[11
USE OF ARTIFICIAL INTELLIGENCE AND OMICS
Artificial Intelligence:-
Artificial Intelligence (AI) aims to understand and replicate intelligent behaviour by creating computer programs, seeking to uncover the underlying principles that govern both artificial and biological system. Artificial Intelligence (AI) can be classified into two different categories based on the capability and functionality. The detailed classification is presented as Below Figure
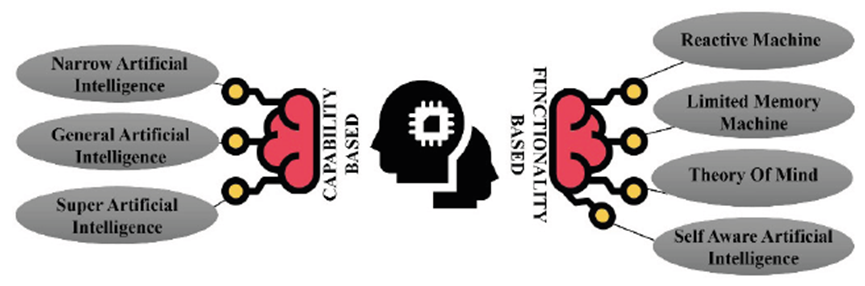
Fig 2;AI classification based on capability and functionality .[2]
Narrow AI is a weak AI, which is trained to perform specific but limited predetermined parameters. General AI is strong AI, having thinking capability. Super AI can surpass human intelligence with its capacity of thinking, reasoning, solving a puzzle, making judgments, learning, and communicating on its own.
Reactive machines respond to stimuli using pre-defined rules and lacks the ability to remember past experiences. Limited memory machines are able to learn and improve over time using data, typically by using artificial neural networks or another programming model. Deep learning, which is a subtype of machine learning, falls into this category. Theory of mind is a hypothetical stage of AI that has human-like decision-making abilities and can understand and recall emotions, as well as respond to social situations. Self-aware AI refers to machines that have an awareness of their own existence and have human-like intellectual and emotional capabilities. Theory of mind and self-aware AI are under developmental stage.
Omics Data Studies:-
Omics data study involves analysing large datasets that capture information about various biological molecules, such as genes, proteins, and metabolites. This approach can provide a comprehensive view of biological systems and help researchers understand how different molecules interact and contribute to cellular processes and disease. To analyse omics data, researchers typically use computational and statistical methods to identify patterns and relationships among different molecules and to gain insights into their functions and roles in biological systems. Gives an Overview of different Omics data studies.[12]
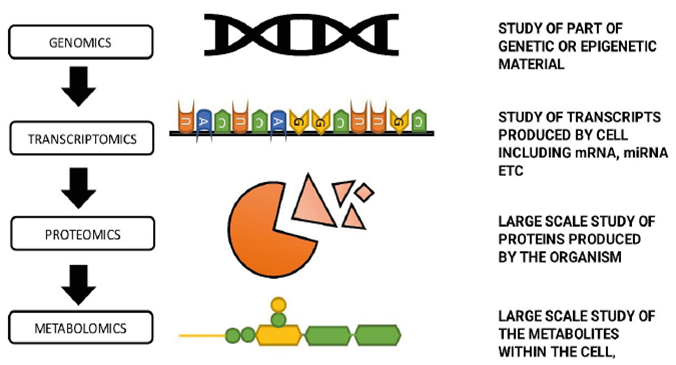
Fig 3;omics data studies [3]
A Comprehensive Overview of Omics Data Studies: From Genomics to Proteomics and Beyond.
Genomics:
Genomics is the study of all genes within an organism, including their interactions and effects. It enables the identification of genetic variants that are linked to health, disease, and therapeutic response. Genomics provides an extensive insight into the genetic makeup of an organism and how it influences its health and well-being. The technology used for this purpose includes high-throughput sequencing, genotyping, and gene expression analysis .Genomic studies have changed the way we view complex diseases by identifying specific biomarkers.
Proteomics:
The proteome refers to the full collection of proteins produced by a cell, tissue, or organism during a specific period. Proteomics is a technology used to investigate the expression levels, structure, and functions of proteins and to study the dynamics of their changes over time. Proteomics can be used to identify protein expression patterns in response to external stimuli, to investigate the effects of disease on the proteins expressed in a tissue, and to comprehend the complex interaction networks of proteins at the cellular and tissue level.
Transcriptomics:
Transcriptomes are collections of all transcripts produced by a particular cell or tissue, including mRNA, miRNA, lncRNA, and other non-coding RNAs. RNA-seq is a powerful technique used to study transcriptomes, producing vast amounts of data that can be used to uncover new insights about gene expression, gene regulation, and other biological processes. Transcriptomes can provide valuable insights into cellular processes, gene expression patterns, and the underlying mechanisms of disease .
Metabolome:
The metabolome consists of all the metabolites, which are small-molecule groups like carbohydrates, proteinogenic amino acids, sugars, and lipid acids. Metabolomics studies can focus on different levels of metabolites and deviations or imbalances in their relative levels can indicate disease when they fall outside of normal ranges .There are databases, such as the Human Metabolome Database .METLIN and MetaboLights that gather information on metabolites found in biological samples using techniques such as chromatography, NMR, and MS. Efforts are underway to standardize metabolomics data through initiatives like the Metabolomics Standard Initiative and the Coordination of Standards in MetabolOmics. Changes in metabolite levels can reveal an individual’s genetic makeup and environmental exposures, making them useful for diagnosing conditions and understanding the molecular pathways involved in patient care.[12]
13. CHALLENGES IN BIOMARKER DEVELOPMENT
Recent success of companion diagnostics along with the increasing regulatory pressure for better identification of the target population has created an unprecedented incentive for drug discovery companies to invest in novel strategies for biomarker discovery. In parallel with the rapid advancement and clinical adoption of high-throughput technologies, a number of knowledge management and systems biology approaches have been developed to analyze an ever increasing collection of OMICs data. This review discusses current biomarker discovery technologies highlighting challenges and opportunities of knowledge capturing and presenting a perspective of the future integrative modeling approaches as an emerging trend in biomarker prediction.
Highlights
Challenges and opportunities for oncology biomarker discovery.
Challenges in the identification and testing of biomarkers
The initial companion diagnostic tests developed for matching patients rationally with molecularly targeted agents consisted mainly of single-gene assays. With the advances in molecular profiling technologies, our improved knowledge in tumor genomics, and the decrease in costs associated with next-generation sequencing (NGS) assays, there has been an exponential increase in the number of genes tested within multiplex panels using sophisticated platforms. This wider tumor genomic profiling has in turn led to further gains in our understanding of tumor biology and the dissection of resistance pathways related to a range of modern therapies. This has led to the development of rational combination therapies designed to overcome monotherapy drug resistance, e.g. regimens involving MEK and BRAF inhibitors [Citation20]. NGS is now a commonly utilized research tool integrated in different clinical settings, including molecular screening efforts set up to personalize antitumor therapies through the enrolment of patients onto genomically guided clinical trials.
It is clear that NGS offers undisputable benefits, but carries several challenges. The high-resolution data achieved with NGS allow the identification of a large number of genomic alterations, with a considerable increase in computational analysis and bioinformatics support that are now needed for the production and interpretation of these data. Although the large amount of data could potentially be used for the discovery of novel biological mechanisms underlying cancer progression and drug resistance, ultimately only a small fraction of the sequenced data is useful in the clinic for personalized treatment selection based on our current knowledge and availability of genomically matched therapies.
Although comprehensive molecular testing integrating the different ‘omics,’ such as proteomics and metabolomics, could help identify new predictive biomarkers of response and resistance, the lack of data reproducibility between multiple platforms and the associated challenges of analytical validation has limited their implementation in routine clinical practice. Currently, necessary efforts such as the mandatory validation of biomarkers in CLIA (clinical-laboratory improvement amendments)-certified laboratories prior to their use in the clinic to assure accuracy and reproducibility of laboratory procedures has served to ensure high-quality biomarker testing. In the future, the establishment of large knowledge bases of NGS data, increased collaborations between clinicians, scientists, clinical centers, and regulatory entities, as well as the redefinition of validation criteria may prove useful in improving biomarker development. Apart from these factors, tissue availability and tumor quality are other important challenges that need to be addressed for the application of multiple molecular and genomic analyses using current technologies.
Challenges in the implementation of biomarkers in clinical drug development
The next generation of clinical trials will need to take into account co-alterations that may drive resistance to single agent targeted therapies and to use such knowledge to rationally combine different anticancer drugs. However, the design of such drug regimens will require a deep understanding of the tumor biology involved, as well as preclinical and clinical pharmacology of drugs to avoid overlapping toxicities .
Actionability of an alteration can be based on their diagnostic or prognostic value; however, the common accepted definition of an actionable alteration in precision oncology is based on the predictive response (sensitivity or resistance) to a currently genomically matched treatment that is FDA approved or available in clinical trials [Citation4]. Although some alterations may occur within an actionable gene, the alteration itself may not ultimately lead to functional change of the protein, and treating physicians should be aware of these challenges. Absence of genomic decision support for physicians can lead to the suboptimal treatment of patients by not offering genotype-matched treatments in the setting of a known pathogenic actionable genomic alteration or by targeting a non-actionable variant. [13]
14. REGULATORY ASPECTS (FDA, EMA)
The European Medicines Agency (EMA) and FDA have policy goals of strengthening benefit–risk (B–R) capabilities; but how this has been translating into regulatory practice is unclear. A systematic review of oncology drug approvals between 2015 and 2020 was conducted with approvals identified through review of FDA and EMA annual reports, with extraction of information on submission, clinical program and B–R assessment from publicly available review documents. Data were extracted from 236 reviews (EMA: 66 new submissions, 100 label extensions; FDA: 70 new submissions). The standard of evidence for B–R assessments seems to have diversified over time; yet, despite policy targets to extend their use, these assessments rarely include patient experience or real-world data.
A benefit–risk (B–R) assessment continuously examines the favorable and unfavorable effects of a specific treatment to determine whether benefits outweigh risks in a specific condition.1, 2 A B–R assessment is a complex and essential activity that pharmaceutical companies and regulators must perform throughout the entire medical product lifecycle to account for more information accumulating over time.3 Although no single B–R methodology can fully capture all aspects of the assessment, use of a clear structured or descriptive framework that clearly identifies and communicates key issues, evidence and uncertainties used in the assessment – and the documentation used in the decision-making process – can facilitate transparency for the B–R assessment [14]
Table 1; Different therapeutic clases [1]
|
Therapeutic class |
Approved first by FDA |
Approved first by EMA |
Median time difference between aaprovals in days |
|
Kinase inhibitor |
37 |
0 |
281[137-367] |
|
Monoiclonal antibody |
18 |
2 |
171[100-265] |
|
Antibody drug conjugate |
4 |
4 |
266[220-395] |
|
Cytotoxic chemotherapy |
5 |
5 |
245[145-336] |
|
Other |
16 |
2 |
242[179-328] |
|
Total |
80 |
6 |
227[124-357] |
CONCLUSION
The central goal of biomarker-based personalized cancer therapy is to make treatment decisions based on tumor genotypes and genetic profiles. Matching targeted therapies against specific genetic aberrations is an important step for personalized cancer therapy. Such an approach holds promise in ultimately improving measurable clinical outcomes: response rates, survival and safety .A new molecular classification of many cancers has evolved based on chromosomal aberrations, gene.
Biomarkers are the silent heroes of modern medicine, providing insight, hope, and innovation in the realm of health. As technology and research advance, the world of biomarkers will continue to unlock the mysteries of our well-being. Embracing this knowledge can empower individuals to take control of their health and lead to groundbreaking discoveries in medicine.
To provide the facility of biomarkers in a university, you would typically follow these steps:
Needs Assessment: Identify the demand for biomarker research and testing facilities within your university community. Consult with faculty, researchers, and relevant departments to gauge interest and need.
Resource Allocation: Allocate the necessary budget, space, and personnel for establishing a biomarker facility. This may involve obtaining grants, donations, or securing university funding.
Infrastructure and Equipment: Procure the required infrastructure and equipment for biomarker research. This may include laboratory space, specialized instruments, and consumables.
Qualified Staff: Hire or train qualified staff, including researchers, technicians, and lab managers, with expertise in biomarker analysis and research.
Regulatory Compliance: Ensure that your facility complies with all relevant regulations and standards, including biosafety and ethical guidelines.
Collaborations: Foster collaborations with relevant departments, research centers, and external partners to enhance the facility's capabilities and research scope.
Education and Training: Offer training programs and workshops for students, researchers, and faculty to develop skills in biomarker research.[15].
REFERENCES






Pattem Sirisha, Mekala Alekya, Irinjala Lakshmi Sruthi, Maddala Maheswari, Guddati Sri Teja, Gannapureddy Sai Gopala Krishna, Vanum Vinay, Unlocking Precision Medicine: Development of Pharmacodynamic Biomarker, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3475-3496. https://doi.org/10.5281/zenodo.18034329
 10.5281/zenodo.18034329
10.5281/zenodo.18034329
