1,2,5 PharmD Intern , Parul Institute of Pharmacy and Research, Vadodara, Gujarat, India.
3,4 Assistant Professor, Parul Institute of Pharmacy and Research, Vadodara, Gujarat, India.
Background: Adolescent drug misuse is a serious health concern that is also a grave threat in India. This study assesses the costs of substance abuse and the financial burden that it places on the sufferer. The purpose of the study is to inform the patient about the expenses of their substance-seeking behaviours and how those expenditures influence their health and finances. Thus, this can aid the patient in comprehending the costs and risks of substance use. Such information could aid in the creation of appropriate policies for the benefit of addicts and the growth of de-addiction facilities. Objective: This study is planned to analyze the pharmaco-economics of substance addiction amongst college-going youth and to understand the financial burden associated with it. Methods: This cohort observational study was conducted online via a self-assessment query form circulated amongst the students of various institutions. The information collected was analyzed and descriptive statistics were performed along with the use of MS Excel to evaluate the cost of purchasing substances and associated medical costs. Result: A total of 209 subjects filled out the form, of which 164 subjects (76.63%) reported consuming caffeine. 31 subjects (14.48%) reported consuming alcohol, 26 subjects (12.14%) smoked cigarettes, 13 subjects (6.07%) chewed tobacco, 7 subjects (3.27%) reported to have consumed recreational drugs which were cannabis, and 1 subject (0.46%) reported to have consumed sopari/ areca nut. Conclusion: This study concluded that substance abuse, addiction, and a decline in quality of life come at a large financial cost. Male individuals took dangerously high amounts of drugs and were more likely to develop addictions than female ones. Addiction to any substance harms the family's annual income as well as direct costs to the user. There is a need for patient counselling and education regarding addictive habits and coping mechanisms, and there are numerous de-addiction counsellors and helplines, but their efficacy depends on the addict's efforts.
Substance addiction is a neuropsychiatric disorder characterized by a recurring desire to continue taking the drug despite harmful consequences. WHO defines substance addiction as – The repeated use of a psychoactive substance or substances, to the extent that the user (addict) is periodically or chronically intoxicated , shows a compulsion to take the preferred substance, has great difficulty in voluntarily ceasing or modifying substance use, and exhibits determination to obtain psychoactive substance by almost any means. The term addiction also conveys the sense that such substance use has a detrimental effect on society, as well as on the individual. In India, substance use disorders (SUDs) are the most prevalent mental health morbidity observed in data compiled by the National Mental Health Survey of India, 2015-16 [1], as well as it is one of the most worrisome public health concerns. According to the 2019 survey on substance use in India, over 57 million of the population in India require professional assistance for alcohol use disorders and around 7.7 million for opioid use disorders [2]. Tobacco use is one of the major causes of death and disease in India and accounts for nearly 1.35 million deaths every year. India is also the second largest consumer and producer of tobacco. A variety of tobacco products are available at very low prices in the country. Nearly 267 million adults (15 years and above) in India (29% of all adults) are users of tobacco, according to the Global Adult Tobacco Survey India, 2016-17 [3]. Caffeine is an active and addictive constituent found in tea, coffee, soft drinks and energy drinks. Caffeine addiction, although not stigmatized, is an issue that plagues a majority of people. People have reported being unable to function without their morning dose of caffeine. Hospitalization, fatal conditions or even mortality arising from large amounts of caffeine intake are not reported as much as other substance addictions, albeit it does cause dependence and tolerance like any other addictive substance. It can also lead to withdrawal symptoms if stopped abruptly and can exacerbate other underlying conditions such as hypertension, diabetes, COPD, Ischemia and arrhythmias [4,5,6]. The active addictive substance in tobacco is nicotine, a natural alkaloid. The most common forms of tobacco that are consumed are cigarettes and smokeless tobacco (chewing). They are also growing in popularity as e-cigarettes. Tobacco addiction is maintained in the user by nicotine dependence, as nicotine can easily cross the blood-brain barrier and exerts its pharmacological effects via the CNS nicotinic receptors and induces the secretion of neurotransmitters [7]. Other recreational drugs that we found to be commonly used by students are ganjaa /weed scientifically known as cannabis, and rarely cocaine.The active constituents in cannabis are cannabinoids; mainly THC and cannabidiol, which are psychoactive substances. Cannabis can be consumed by smoking it in joints or via inhaling the vapour. Cannabis is also termed as a gateway drug to opioid use and cocaine use as they have a similar pharmacologic interaction with the receptors in the human body, and secrete endogenous opioids in the body [8].
MATERIALS AND METHODS:
The study was an observational Study, conducted via online self-filled survey form. A predesigned and pretested questionnaire was prepared with questions relating to addiction and its pharmacoeconomics. The form was distributed amongst university students and staff in and around Waghodia. Patients in the age group of less than 18 years were excluded from this study. The online survey form generated an Excel sheet composed of all the data filled in by the users. The data was further sorted and filtered out for subjects who left the survey incomplete or denied consent for the survey. The data was summarised in an Excel sheet and the data was run through various Excel programs and summarised tables and charts were generated. Statistical analysis methods were calculated. The results were represented pictorially and theoretically.
OBSERVATION & RESULTS:
A total of 209 subjects filled out the form, of which 164, (76.63%) reported consuming caffeine. 31 subjects (14.48%) reportedly consumed alcohol, 26 subjects (12.14%) smoked cigarettes, 13 subjects (6.07%) chewed tobacco, 7 subjects (3.27%) reported to have consumed recreational drugs which were cannabis, and 1 subject (0.46%) reported to have consumed sopari/ areca nut. The average annual income of each family was found to be 9.6lacs per annum, which bore the cost of substance-seeking behaviours of the addict.

Table 1: Pharmaco-economics and demographic characteristics of subjects who consumed caffeinated drinks
Table 1 shows information about participants who had consumed caffeine, amongst other addictive substances, such as duration of consumption, annual income of participants and their families, cost of hospital visits, overdose, clinical difficulties, and drug usage cessation. From 30 subjects, a majority (70%, n=21) of subjects who consumed alcohol belonged to 20-25 years of age. The other participants who consumed alcohol belonged to the age group of 35-40 years (n=4, 13%), 25-30 years (n=2, 6.6%), 30-35 years age (n=2, 6.6%) and 45-50 years of age (n=1, 3.3%). The mean age of male participants who reported consuming alcohol is 24.6 years which is nearly the mean of female age which is 24.5 years of age. The subjects were segregated based on their annual income. A majority of subjects (n=107) earned an average of 2.5 lacs to 10 lacs per year. 29 subjects reported to have an income of 10 lacs to 25 lacs per annum, 6 subjects earned more than 25 lacs per annum and one subject reported to earn less than 2.5 lacs per year. According to the findings of this study, most of the subjects who consume caffeinated drinks were from families that earned 2.5 lacs to 10 lacs per year. Each hospital visit cost is assessed for influencing the cost of caffeine consumption to the subject. We factor in hospital visit costs ranging from 0 to 50,000 rupees. 11 subjects reported having visited clinics seeking medical help. 4 subjects spent between INR 0 to 1,000 on each of the hospital visits, 3 subjects spent INR 1,000-5,000 and another 3 spent in the range of INR 20,000-50,000. One subject spent between 5000-10000 rupees. These subjects spent an average of INR 11,227.00 for hospital visits regarding caffeine overdose or for other caffeine-associated symptoms, which are the direct costs incurred by the patient. These are in addition to caffeine procurement costs which range from INR 10 and can range up to INR 100 per 150ml of caffeinated drinks for each subject. 9 of the 164 participants reported to have overdosed on caffeine at least once. 31 subjects attempted de-addiction of caffeine usage of which a majority (n=25) were successful in doing so. 6 subjects experienced withdrawal symptoms and had relapsed.
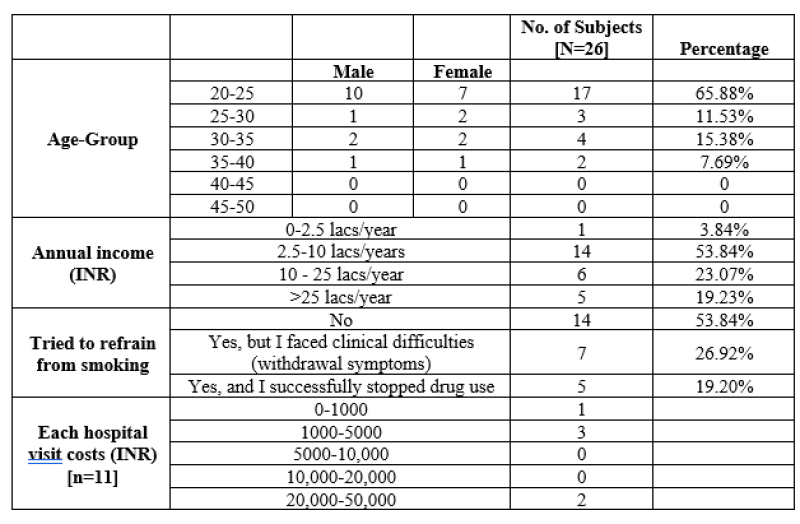
Table 2: Pharmaco-economics and demographic characteristics of subjects who consumed nicotine by smoking in the form of cigarettes or beedis
Table 2 contains information about participants who had consumed nicotine, in the form of smoking cigarettes or beedis and the data of participants such as duration of consumption, annual income of participants and their families, cost of hospital visit, overdose, clinical difficulties, and drug usage cessation. From 26 subjects who reported consuming nicotine by smoking, a majority (n=17, 65%) of those belonged to 20-25 years of age. The segregation across genders was comparable as there were 14 male participants (53.8%) and 12 female participants (46.1%). A majority of subjects (n=17, 65.3%) who smoked nicotine were of the ages ranging from 20-25 years. From this, it was also observed that there were more males as compared to females in this age group who smoked nicotine. The other participants who consumed nicotine by smoking belonged to the age group of 30-35 years (n=4, 15%). The mean age of male participants who reported to consume nicotine by smoking is 25.3 years as compared to the mean of female age which is 26.2 years of age. According to the findings of this study, most of the participants who smoked nicotine were from families that earned 2.5lacs to 10 lacs per year. Each hospital visit cost is assessed for influencing the cost of nicotine consumption to the subject. We factored in hospital visit costs ranging from 0 to 50,000 rupees. 6 subjects reported to have visited clinics seeking medical help. 3 subjects spent between INR 1,000-5,000 on each of the hospital visits and 2 participants spent in the range of INR 20,000-50,000. One subject spent between 5000-10,000 rupees. These subjects spent an average of INR 13,250.00 for hospital visits regarding nicotine associated diseases, which are the direct costs incurred to the patient. These are in addition to cigarettes or beedi procurement costs which range from INR 1 and can range up to INR 100 per unit of cigarette or beedi for each subject. 12 subjects attempted de-addiction of cigarettes usage of which a majority (n=7) were unsuccessful in doing so and had experienced withdrawal symptoms and had relapsed. 5 subjects had reported to have successfully quit smoking.
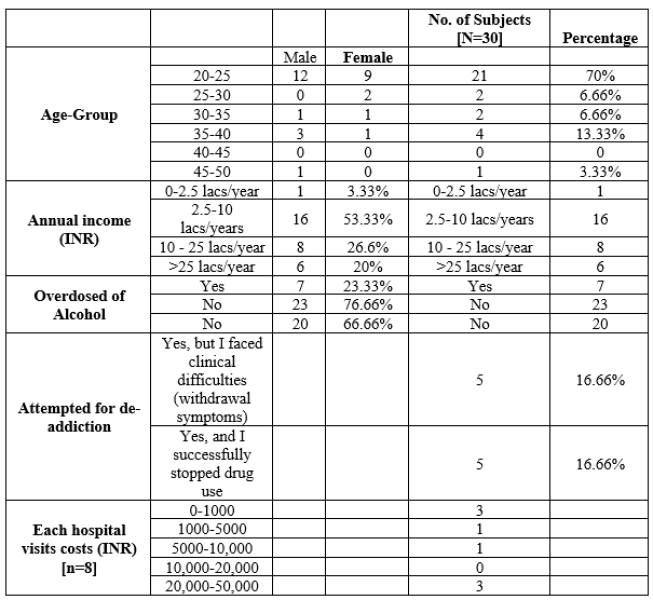
Table 3: Pharmacoeconomics and demographic characteristics of subjects who consumed alcohol.
The above table shows the comparison of alcohol consumption between males and females. A total of 30 subjects responded to this question. From 30 subjects, a majority (70%, n=21) of subjects who consumed alcohol belonged to 20-25 years of age. The other participants who consumed alcohol belonged to the age group of 35-40 years (n=4, 13%), 25-30 years (n=2, 6.6%), 30-35 years age (n=2, 6.6%) and 45-50 years of age (n=1, 3.3%). The mean age of male participants who reported consuming alcohol is 24.6 years which is nearly the mean of female age which is 24.5 years of age. Subjects were segregated based on their annual income. The majority of subjects (n=16) earned an average of 2.5 lacs to 10 lacs per year. 8 subjects 10 lacs to 25 lacs per annum, 6 subjects earned more than 25 lacs per annum and one subject reported to earn less than 2.5 lacs per year. According to the findings of this study, most of the subjects who consume alcohol were from families that earned 2.5 lacs to 10 lacs per year. Each hospital visit cost is assessed for influencing the cost of alcohol consumption to the subject. We factor in hospital visit costs ranging from 0 to 50,000 rupees. 8 subjects reported to have visited clinics seeking medical help. 3 subjects spent between INR 0 to 1000 on each of the hospital visits, and another 3 spent in the range of INR 20,000-50,000. One subject spent INR 1,000-5,000 and similarly, another subject spent between 5,000-10,000 rupees. The subjects spent an average of INR 14,625.00 for hospital visits regarding alcohol-associated diseases, which are the direct costs. These are in addition to alcohol procurement costs which range from INR 100.00 and can range up to INR 10,000.00 per bottle of 500ml for each subject. Seven of the 53 participants reported to have overdosed on alcohol at least once
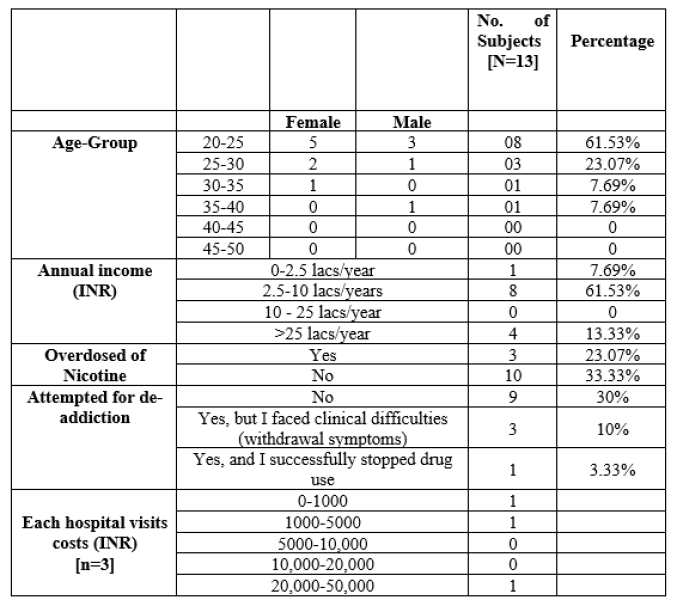
Table 4: Pharmaco-economics and demographic characteristics of subjects who chew on tobacco.
The above Table-4 contains information about participants who had chewed nicotine as tobacco, such as duration of consumption, annual income of subjects and their families, cost of hospital visits, overdose, clinical difficulties, and drug usage cessation. Of 13 subjects who reported chewing tobacco, a majority (n=8, 61%) of subjects belonged to 20-25 years of age. The other participants who chewed tobacco belonged to the age group of 25-30 years (n=3, 23%), 30-35 years (n=1, 7.69%), and 35-40 years (n=1, 7.69%,). The mean age of male participants who reported to consume tobacco is 25 years as compared to the mean of female age which is 26.5 years of age. The subjects were segregated based on their annual income. A majority of subjects (n=8) earned an average of 2.5 lacs to 10 lacs per year. 4 subjects reported to have an income of more than 25 lacs per annum and one subject reported to earn less than 2.5 lacs per year. According to the findings of this study, most of the subjects who chew tobacco were from families that earned 2.5 lacs to 10 lacs per year. Each hospital visit cost is assessed for influencing the cost of tobacco consumption to the subject. We factor in hospital visit costs ranging from 0 to 50,000 rupees.3 subjects reported to have visited clinics seeking medical help. 1 subject spent between INR 0 to 1,000 on each of the hospital visits, 1 subject spent INR 1,000-5,000 and another 1 spent in the range of INR 20,000-50,000. These subjects spent an average of INR 12,833.00 for hospital visits regarding nicotine overdose or for other nicotine-associated symptoms, which are the direct costs incurred by the patient. These are in addition to tobacco procurement costs which range from INR 8.00 and can range up to INR 50.00 per 10gm of tobacco for each subject. 3 of the 13 subjects reported to have overdosed on nicotine at least once. 4 subjects attempted de-addiction of which a majority (n=3) were unsuccessful in doing so, and experienced withdrawal symptoms and had relapsed. Only one subject reported to have successfully quit tobacco consumption.
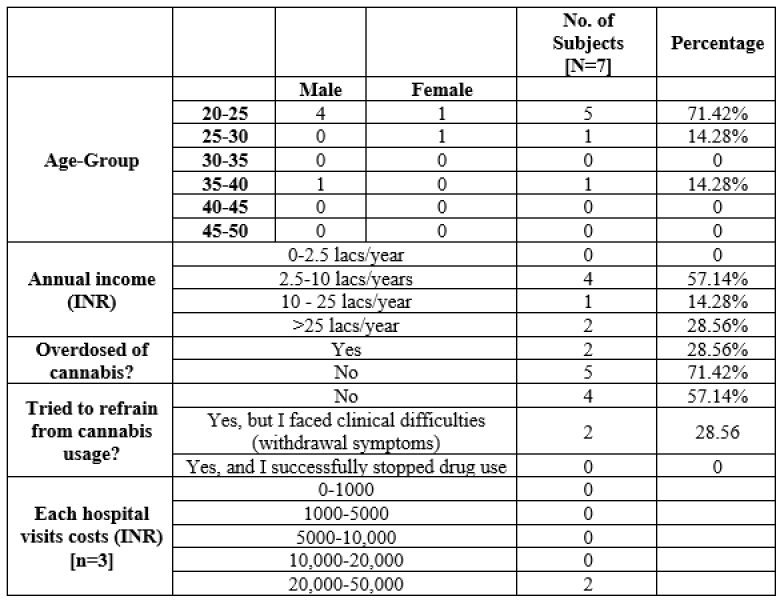
Table 5: Pharmaco-economics and demographic characteristics of subjects who consume cannabis.
From 7 subjects who responded to the questionnaire, a majority (n=5, 71.42%) of subjects who consumed cannabis belonged to 20-25 years of age of which, males were the predominant majority (n= 4 of 5) The mean age of male participants who reported to consume cannabis is 22.5 years as compared to the mean of female age which is 29.1 years of age. The subjects were segregated based on their annual income. A majority of subjects (n=4) earned an average of 2.5 lacs to 10 lacs per year. 2 subjects reported to have an income of more than 25 lacs per annum and one subject reported to earn 10 lacs to 25 lacs per year. According to the findings of this study, most of the subjects who consume cannabis were from families that earned 2.5 lacs to 10 lacs per year. Each hospital visit cost is assessed for influencing the cost of cannabis consumption to the subject. We factor in hospital visit costs ranging from 0 to 50,000 rupees. 2 subjects reported to have visited clinics seeking medical help. Both of the subjects reported to have spent between INR 20,000 to 50,000 on each of the hospital visits. These subjects spent an average of INR 35,000.00 for hospital visits regarding cannabinoid overdose or for other cannabinoid-associated symptoms, which are the direct costs incurred by the patient. These are in addition to cannabis procurement costs which range from INR 500.00 and can range up to INR 5,000.00 per 1gm of cannabis for each subject. 2 of the 7 subjects reported to have overdosed on nicotine at least once. 2 subjects attempted de-addiction, but both reported to be unsuccessful in doing so and experienced withdrawal symptoms and relapsed.
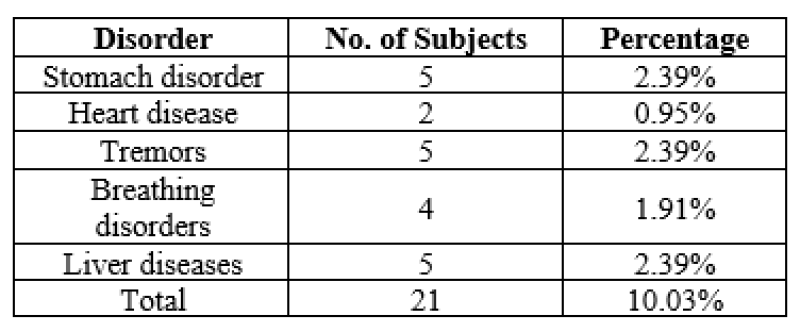
Table 6: Prevalence and occurrence of medical disorders associated with addictive behaviours.
Out of the total 209 subjects who consume addictive substances, 23 reported having had visits to medical professionals regarding their addictive behaviours. This table represents the medical problems of the addicted subject. A total of 21 participants responded to this question.Of the total 209 respondents, 21 subjects (10%) reported to have diagnosed with a medical condition. 2% of patients (n=5) reported were diagnosed and treated for stomach disorders (peptic ulcers, gastric bleeding), tremors (convulsions due to withdrawal) and liver diseases (cirrhosis, fatty liver and alcoholic liver disease), respectively. 2% (n=4) of patients reportedly were diagnosed with breathing disorders (COPD, asthma). 1% (n=2) of the patients reported to have been treated for heart-related disorders (CHF, Arrhythmia).
DISCUSSION:
The results of our study showed that the subjects consume caffeine (164, 76.6%), alcohol (30, 14.4%), cigarettes (26, 12.1%), smokeless tobacco (13, 6%) and cannabis (7, 3.2%). When compared to a study conducted by Kumar S et al in Rewa, MP in 2015 which showed that students use cigarettes (80.6%), alcohol (59.7%), cannabis (13.4%), gutkha/pan (10.4%), tobacco (7.5%), and nasal snuff (3.0%) the most frequently [9]. Of the subjects who consumed caffeinated drinks, a large majority of a portion (127, 77.4%) belonged to the age group of 21-25 years of age. Also, there were 21 (14%) of subjects who consumed 450ml or more caffeinated drinks on an average per day. Our findings also stated that 54 (32.9%) subjects had been consuming caffeine for more than 10 years. The data corresponds with a study performed by Pathan A W et al in 2019 whose findings stated that 14% of students had a serious caffeine addiction [10]. Of the subjects who consumed caffeinated drinks amongst other substances, 11 (6.7%) subjects had hospital visits seeking professional help. The average direct cost of each hospital visit incurred by single patient was INR 11,227.00. Of all the subjects addicted to caffeine, 31 (19.4%) of subjects tried to refrain from caffeine consumption, of which 26 (15.7%) were successful in doing so. Approximately 30 1(4.4%) of subjects were consuming alcohol, from which there were 56.6% (n=17) of males and 43.3% (n=13) of females. A large number of the subjects (70%) who consumed alcohol belonged to the age group of 20-25 years. The data thus shows that a majority of subjects, who consume alcohol, begin at a young age. When Girish N et al conducted a study on alcohol usage patterns in 2011, they summarised that more than two-thirds (66%) of the users were in the 26–45 years age–group and 10?longed to the 16-25 years of age [11]. Singh P S et al observed in their study, in Odisha that the average hospitalization for alcohol-related problems was 2.6 times/year with an average expenditure of INR 30,000.00 during each hospitalization. For treatment expenses, 86% of patients borrowed money from friends/relatives, 36% used saving deposits, 04% sold personal belongings, and 03% sold lands [12]. In comparison, in our study, we observed that 23.3% of subjects had reported having consumed excessive alcohol or overdosed on it at least once and that the average expenditure for each patient was INR 14,625.00 for hospital visits. This included doctors visiting fees, medication charges and other diagnostic test charges, which are all direct costs incurred by the patient. The cost of achieving healthcare in Gujarat is comparatively quite low when compared to that of Odisha, the difference could be due to differences in healthcare penetration and how much the patient has to travel, amongst various other factors.Of the subjects who had been consuming alcohol, 66.7% did not attempt to refrain from alcohol consumption. Of the 33.3% of subjects who tried de-addiction, half of them were unsuccessful and had relapsed or suffered from withdrawal symptoms. This study enumerates that a total of 18.2% (n=39) subjects, consumed tobacco in any form. Out of those, 12.1% (n=26) of the participants smoke tobacco as cigarettes or beedis and 6.1% (n=13) consume smokeless tobacco or sublingual tobacco. A study conducted by Gupta P C et al in 2005, summarised that 27.4% smoked and 46.1% used smokeless tobacco in the study arm of only males. In the other arm consisting exclusively of females, they observed that 0.4% smoked and 59.3% consumed smokeless tobacco [13]. Of the subjects who smoked cigarettes, 48% (n=12) subjects had tried to refrain from smoking, but less than half (n=5, 35.7%) were successful in doing so. A majority (n=7, 58.3%) had relapsed or experienced withdrawal symptoms. Of all the subjects who smoked, 23% had sought out professional medical help. The average cost of each hospital visit incurred by the patient was INR 13,250.00. Of the subjects who chewed tobacco, 30.6% (n=4) subjects had attempted to refrain from tobacco usage, of which only 25% (n=1) were successful in doing so. The others (n=3, 75%) had relapsed or suffered from withdrawal symptoms. 23% of subjects had reached out to professionals seeking to reduce or stop their tobacco chewing habits or for diagnosis & treatment of tobacco-associated health complications. The average cost incurred by each patient for one hospital visit was INR 12,833.00, which are the direct costs incurred by the patients. 3.27% (n=7) of the subjects reported to use recreational drugs. All of the subjects reported the substance in question as ganjaa or weed, scientifically known as cannabis. 57.1% (n=4) of the subjects who consumed cannabis were males, all belonging to the age group of 20-25 years old. 42.95% (n=3) of the subjects were females, who were of different age groups. 28.5% (n=2) of subjects reported to have overdosed on cannabis, experiencing symptoms such as hallucinations and nausea, associated with cannabis toxicity.
CONCLUSION:
From this present study concludes that there are significant costs associated with substance usage and addiction not to mention the deterioration of quality of life. We observed that male participants were more prone to fall prey to addiction as compared to female participants although the difference is small. Also, quite many of the subjects consumed dangerously high amounts of substances such as smoking 60 cigarettes on average or consuming 600ml of caffeinated drinks every day. These subjects are at very high risk for various addiction-related clinical manifestations such as dependence and withdrawal, and they are also more prone to suffer from diseases. According to present study observations, sustaining a substance addiction to any addictive substance, for instance, caffeine, alcohol, and/or tobacco, will greatly affect the user and their family members, as different parameters such as direct costs of the substance to the user, procurement costs, and hospitalisation cost will invariably affect the survival of the family members.
ACKNOWLEDGEMENT:
We are Thankful to Dr. G.S.Chakraborthy (Professor and Principal), Dr. Snigdha D Mandal, (Associate professor and HOD), Mr. Anas A Jamsa (Assistant Professor), Dr. S.P. Nayak (Assistant Professor) Parul Institute of Pharmacy and Research, Parul University, Waghodia, Vadodara, Gujarat for promoting and motivating for carried out this study.
REFERENCES





Vatsalkumar N. Patel, Parita J. Bhalodiya, Mohammed Tousif Idrisi, Mohit D. Buddhadeva, Ashka S. Soni , Understanding Pharmaco-Economics Of Substance Addiction: An Observational Study., Int. J. of Pharm. Sci., 2024, Vol 2, Issue 3, 278-288. https://doi.org/10.5281/zenodo.10802198
 10.5281/zenodo.10802198
10.5281/zenodo.10802198
