C. L. Baid Metha College of Pharmacy, Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai-600097, Tamil Nadu, India
Migraine is a recurrent neurological disorder often managed with triptans, but oral therapy with rizatriptan suffers from limitations such as low bioavailability (\~45%), short half-life (2–3 hours), and first-pass metabolism. To overcome these drawbacks, the present study aimed to develop and evaluate transdermal patches of rizatriptan benzoate for sustained anti-migraine therapy. Patches were prepared using the solvent casting method with hydroxypropyl methylcellulose (HPMC K100) as the polymer, ethanol and isopropyl alcohol as solvents, and glycerol as plasticizer. Pre-formulation studies confirmed drug purity, solubility, ?max at 227 nm, and compatibility with excipients (FTIR). Three formulations (P1, P2, P3) were developed and evaluated for physicochemical and mechanical properties, including thickness, weight uniformity, folding endurance, tensile strength, moisture content, and drug content uniformity. In vitro drug release and permeation studies were carried out using a Franz diffusion cell. Among the formulations, P1 exhibited optimal performance with uniform thickness (0.132 ± 0.01 mm), highest drug content (86.2 ± 0.59%), tensile strength (2.90 ± 0.23 kg/cm²), lowest moisture uptake (2.97 ± 0.40%), and maximum cumulative drug release (95.45 ± 0.22% within 360 min). Stability studies under accelerated conditions (40 °C ± 2 °C / 75% RH ± 5% RH for 3 months) confirmed that P1 retained its physical integrity, drug content, and release profile without significant changes. The findings suggest that the optimized rizatriptan benzoate transdermal patch (P1) offers a stable, efficient, and patient-friendly alternative to oral therapy, with potential to improve bioavailability, sustain drug release, and enhance therapeutic outcomes in migraine management
Migraine is a prevalent neurological disorder characterized by recurrent headache episodes often accompanied by nausea, vomiting, photophobia, and phonophobia. It significantly affects the quality of life and work productivity of patients worldwide [1]. Among various therapeutic options, triptans remain the first-line drugs for acute migraine management due to their high efficacy in relieving headache and associated symptoms [2]. Rizatriptan, a selective serotonin 5-HT1B/1D receptor agonist, is one of the most effective antimigraine drugs with a rapid onset of action [3]. However, oral rizatriptan therapy is limited by its low bioavailability (~45%), short elimination half-life (2–3 h), and extensive first-pass metabolism, leading to the recurrence of migraine and reduced patient compliance [4].
Transdermal drug delivery systems (TDDS) provide an innovative approach to overcome these drawbacks. TDDS allows the drug to directly penetrate through the skin into systemic circulation, bypassing the gastrointestinal tract and hepatic first-pass metabolism [5]. This mode of delivery offers several advantages, including sustained and controlled release, improved bioavailability, ease of administration, and enhanced patient compliance [6]. Moreover, the ability to terminate drug action simply by removing the patch provides an additional safety advantage [7]. An ideal candidate for TDDS should possess a low molecular weight (<500 Da), sufficient lipophilicity, and high potency at low doses [8]. Rizatriptan, with a molecular weight of 269 Da, low plasma protein binding (~14%), and efficacy at doses of 5–10 mg, fulfills these requirements, making it a suitable candidate for transdermal patch formulation [3,4]. Therefore, the present study aims to formulate and evaluate rizatriptan benzoate transdermal patches using hydroxypropyl methylcellulose (HPMC) as the polymer, along with suitable permeation enhancers and plasticizers. The patches were subjected to physicochemical characterization, in-vitro drug release, permeation, and stability studies to establish their potential as a sustained-release, patient-friendly alternative for migraine therapy.
MATERIALS AND METHODS
Materials
The drug Rizatriptan benzoate was obtained as a gift sample for the present study. Hydroxypropyl methylcellulose (HPMC K100), ethanol and isopropyl alcohol were procured from Loba Chemie Pvt. Ltd., Mumbai, while polyvinyl alcohol (PVA) was purchased from S.D. Fine Chemicals, Mumbai. Glycerol was obtained from Merck Specialties Pvt. Ltd., Mumbai. All the chemicals and reagents employed were of analytical grade.
Methods
Preformulation Study
Organoleptic characters
Organoleptic character like colour, odour were observed and recorder using descriptive terminology [9].
Determination of solubility
Rizatripta solubility has been evaluated by dissolving excess quantities of the drugs in the solvent [10].
Melting point determination
Melting point apparatus was used to determine the drug sample's melting point using the capillary method. Small quantity of drug was taken in capillary tube (fused at one end) and placed in melting point apparatus, and the melting temperature was recorded [11].
Calibration curve of rizatriptan
Preparation of standard curve for rizatriptan benzoate
Standard drug solution of rizatriptan benzoate was prepared by dissolving 10mg rizatriptan benzoate in distilled water and made to 10ml with distilled water to obtain stock solution of 1 mg/ml or 1000µg/ml concentration. From the stock solutions, 1.0ml of Rizatriptan Benzoate was transferred to 100ml volumetric flask and the volume was adjusted to the mark with distilled water to obtain strength of 10µg/ml. The solution was scanned in the UV range 200-400 nm.First, second, third, fourth order derivative UV spectra for the solutions of Rizatriptan Benzoate were recorded in a 10mm cell over the range 200-400nm using distilled water in the reference cell. Each spectrum was recorded in triplicate. The zero-crossing point (ZCP) for Rizatriptan Benzoate were recorded. Characteristic wavelengths (ZCPs) for Rizatriptan Benzoate were confirmed by varying the concentration of the drug. For each replicate measurement, the cell was refilled with fresh solution.Average of 5 sets of values were taken and summarised in (Table 1 and Figure 19) and the standard curve was plotted [12].
Compatibility studies
The incompatibility between the drug and excipients are studied by FTIR spectroscopy. .
Fourier Transform Infrared (FTIR)
The FTIR spectra of Rizatriptan benzoate, HPMC, ethanol, isopropyl alcohol, and the optimized formulation (P1) were recorded using a Bruker FTIR spectrophotometer to study drug–excipient interactions. Samples were prepared by mixing 2 mg of drug or formulation with 200 mg of dry KBr, compressed into pellets, and scanned over 400–4000 cm?¹ at a resolution of 4 cm?¹. The spectra were compared to detect any shifts or changes in characteristic peaks [13].
Dose Calculation of Drugs
Transdermal dose = Oral dose × Bioavailability fraction [14]
Oral dose = 10 mg
Bioavailability fraction = the fraction of drug that reaches systemic circulation orally (as a decimal, e.g., 45% = 0.45)
Transdermal dose of Rizatriptan = 10 × 0.45 = 4.5 mg
Formulation of Rizatriptan benzoate patch
The Rizatriptan benzoate transdermal patch was prepared using the solvent casting method. Accurately weighed amounts of hydroxypropyl methylcellulose (HPMC) were dissolved in ethanol and stirred until completely solubilized. Rizatriptan benzoate was separately dissolved in a mixture of ethanol and isopropyl alcohol and then added to the polymer solution. The combined solution was mixed thoroughly to ensure complete solubilization of the drug. Glycerol was added dropwise to the polymer–drug solution to improve flexibility and prevent brittleness, followed by continuous stirring to achieve uniform distribution of all components. The final solution was poured onto a levelled petri dish or glass plate to form an even film of uniform thickness. The solvent was allowed to evaporate at room temperature under controlled conditions, and the film was completely dried to obtain the transdermal patch. After drying, the patch was carefully peeled from the surface and stored in a sealed container to prevent moisture absorption. The prepared patch was visually inspected for homogeneity, clarity, and color, and its melting point was measured at room temperature before storage in a cool, dry place. As shown in table 1[15].
Table 1 : Formulation of Rizatriptan benzoate patch
|
INGREDIENTS |
P1 |
P2 |
P3 |
|
Rizatriptan (mg) |
4.5 |
4.5 |
4.5 |
|
Hydroxypropyl methyl cellulose (g) |
1
|
1.25 |
1.50 |
|
Isopropyl alcohol (ml) |
5 |
5 |
5 |
|
Ethanol (ml) |
5 |
5 |
5 |
|
Glycerol (ml) |
0.3 |
0.3 |
0.3 |
POST EVALUATION STUDIES OF TRANSDERMAL PATCHES
Physical appearance
Visual evaluations for colour, clarity, flexibility, and smoothness were made for each prepared patch[11].
Film thickness
At three different points on the drug-loaded patches, the thickness of the patches was measured using a screw gauge micrometre. For each drug-loaded patch, the average and standard deviation of the three measures were calculated [15].
Weight variation
Weight variations of the transdermal patches were done by cutting the patches into 1cm2 from 3 different points of the patches and weight of each patch was determined by using the digital balance. The average weight and its standard deviations was calculated [16].
Folding endurance
The evaluation of folding endurance of the transdermal patches was done to determine the folding capacity of the film subjected to frequent extreme condition of folding. A strip of specific area 2.5 cm2 was cut evenly and repeatedly folded at the same place till it breaks. The number of times the patches folded at same place without breaking was noted as its folding endurance value [11].
Drug content uniformity
The patch of 2.5 cm2 transferred into a glass stopper flask-containing methanol. The flasks were closed and shaken till the patch was completely dissolved. This solution was filtered and the volume was made upto 100 ml by using buffer of pH 7.4, from this 1 ml of solution was pipette out and was diluted upto 10 ml and the absorbance was measured by UV spectrophotometer at 227 nm [12].
Tensile strength
The tensile strength of the patch had been evaluated by using the tensiometer. It consists of two load cell grips of which the lower one was fixed and upper one was movable. Film strips with the dimensions of 2 × 2 cm were fixed between these cell grips, and force should be gradually applied until the film get broke [15].
Percentage moisture content
The formed films must be weighed individually and kept at room temperature in a desiccator together with fused calcium chloride for 24 hours. The films must be reweighed after 24 hours in order to calculate the percentage moisture content using the formula below [16].
% Moisture Content = (Final weight - Initial weight) / Initial weight ×100
In-Vitro Permeation study
The in vitro drug release from the rizatriptan transdermal patch was studied using a Franz diffusion cell with a dialysis membrane (or specified synthetic membrane) as the diffusion barrier. The receptor compartment was filled with phosphate buffer (pH 7.4) and maintained at 37 ± 0.5 °C with continuous stirring. A known area of the patch was placed in contact with the membrane, with the drug-loaded side facing the receptor medium. At predetermined time intervals, 1 mL of the receptor medium was withdrawn and replaced with fresh buffer to maintain sink conditions. The samples were analyzed using a UV–Visible spectrophotometer at 227 nm

Stability study
The stability study was carried out for the most satisfactory formulation as per ICH guidelines. The selected formulation was subjected to stability testing for a period of 3 months under accelerated conditions at 40 °C ± 2 °C / 75% RH ± 5% RH. The formulation was periodically analyzed for changes in appearance, pH, percentage drug content, and in-vitro diffusion profile [14].
RESULT AND DISCUSSION
PREFORMULATION STUDIES
Organoleptic characters
The organoleptic evaluation of rizatriptan benzoate confirmed its authenticity and purity. The drug was observed to be a white to off-white, odourless, crystalline powder with a bitter taste, which complied with the standard reference data. These findings confirm its suitability for pharmaceutical applications, as presented in Table 2.
Table 2: Test for pure rizatriptan benzoate drug
|
Test |
Results of Analysis |
Inference |
|
Colour |
White to off-white |
Complies with data |
|
Odour |
Odourless |
Complies with data |
|
Taste |
Bitter |
Complies with data |
|
Appearance |
Crystalline powder |
Complies with data |
Determination of solubility
The solubility study of the drug in various solvents revealed significant differences. As shown in Table 8, the drug exhibited good solubility in water (42 mg/ml), methanol (8 mg/ml), ethanol (1 mg/ml), and chloroform (15 g/ml). Among these solvents, the highest solubility was observed in water, followed by methanol, chloroform, and ethanol. This indicates that water is the most suitable solvent for the drug, while ethanol shows the least solubility.
Melting point determination:
The melting point of Rizatriptan benzoate was determined by placing a small quantity of the drug in a capillary tube and subjecting it to analysis using a melting point apparatus. The observed melting point was found to be 179 °C, which is in agreement with the reported range, thereby indicating the purity of the drug sample.
Determination of λmax
The UV absorption spectrum of Rizatriptan benzoate was recorded using a UV–Visible spectrophotometer. The drug exhibited a maximum absorption at 227 nm, which was selected as the analytical wavelength (λmax) for further quantitative studies. The obtained UV spectrum is shown in Figure 1.
Calibration curve of Rizatriptan benzoate
A calibration curve for Rizatriptan benzoate was constructed by measuring the absorbance of standard drug solutions of different concentrations at 227 nm using a UV–Vis spectrophotometer. The absorbance values were plotted against concentration to obtain the calibration plot. The high correlation value (R² = 0.998). The high correlation value indicates excellent linearity, confirming adherence indicates excellent linearity, confirming adherence to Beer-Lambert’s law. The results are presented in Table 3 and Figure 2
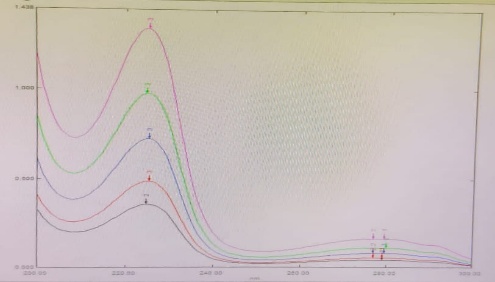
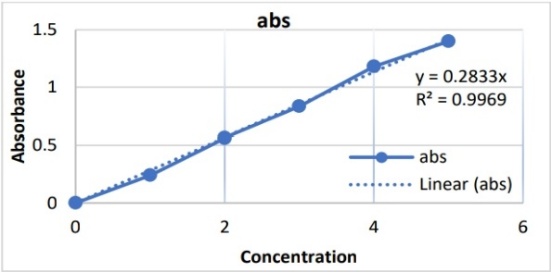
Figure 1: λmax curve of Rizatriptan Figure 2 : Calibration curve of Rizatriptan
Table 3: Standard curve of rizatriptan benzoate
|
S.NO |
Concentration (µg/ml) |
Absorbance (nm) |
|
1 |
10 |
0.241 |
|
2 |
20 |
0.562 |
|
3 |
30 |
0.834 |
|
4 |
40 |
1.180 |
|
5 |
50 |
1.399 |
Compatibility studies:
The incompatibility between the drug and excipients was studied by FTIR spectroscopy. The results indicate that there was no chemical incompatibility between drug and excipients used in the formulation.
FTIR Study:
The FTIR spectrum of Rizatriptan benzoate is shown in Figure 22, while the spectrum of the Rizatriptan benzoate transdermal patch (P1) is presented in Figure 23. The comparison of characteristic peaks of the pure drug and the formulation showed no significant shifts or disappearance of major functional group peaks, indicating the absence of chemical interaction between Rizatriptan benzoate and the selected excipients (HPMC, ethanol, and isopropyl alcohol). This confirms that the excipients did not alter the physicochemical properties, stability, or efficacy of the drug in the best transdermal patch (P1).
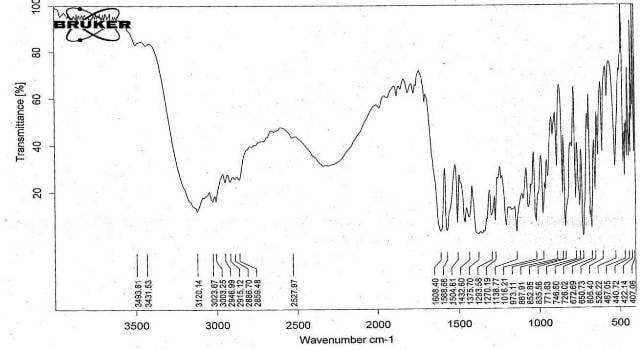
Figure 3: FTIR Spectrum of pure drug of Rizatriptan
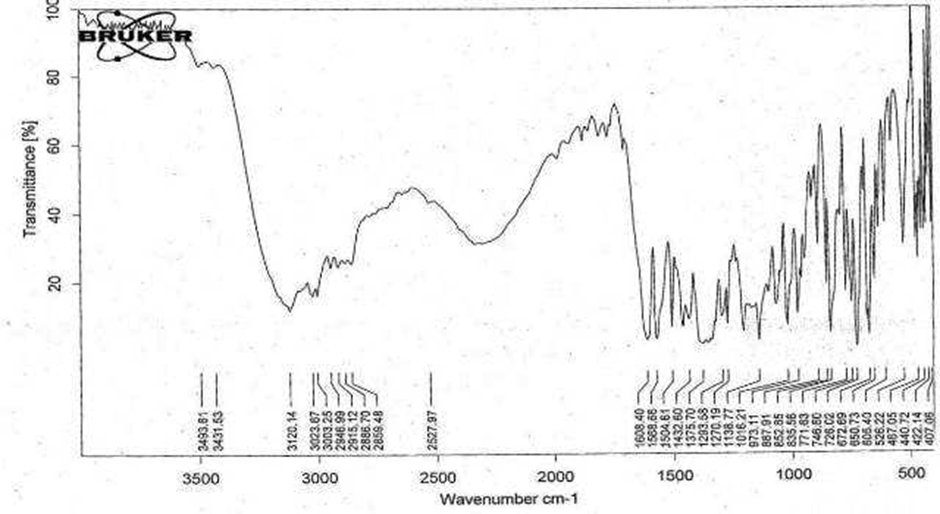
Figure 4: FTIR Spectrum of Formulated Rizatriptan benzoate transdermal patch (P1)
Formulation of Rizatriptan transdermal patch
The prepared Rizatriptan patch was successfully formulated using a polymeric base composed of HPMC K100, which provided the required viscosity and consistency. The incorporation of the drug solution into the polymer matrix was facilitated by continuous stirring, ensuring a homogeneous dispersion of active ingredients.
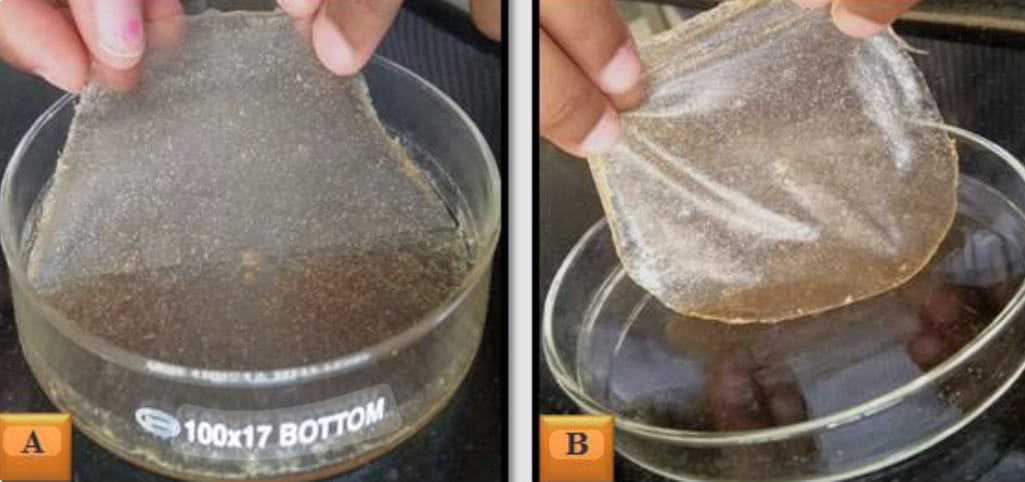
Figure 5: Formulation of Rizatriptan Transdermal Patch
Post Evaluation Studies of Transdermal Patches
The prepared transdermal patches (P1, P2, and P3) were evaluated for various physicochemical parameters, and the results are summarized in Table 4.
Physical appearance
All three formulations (P1, P2, and P3) of the transdermal films were observed to be whitish-yellow in color, smooth, and flexible. The uniform appearance across all formulations indicates proper dispersion of the drug and excipients and suggests good film-forming properties.
Film thickness
The film thickness for P1, P2, and P3 was found to be 0.132 ± 0.01 mm, 0.153 ± 0.03 mm, and 0.169 ± 0.04 mm, respectively. An increase in thickness was observed with the increasing polymer concentration from P1 to P3. Uniform thickness is crucial for consistent drug release, and the measured values show acceptable uniformity (n = 3).
Weight variation
The weight of the films varied slightly across formulations: 0.430 ± 0.02 g (P1), 0.562 ± 0.04 g (P2), and 0.567 ± 0.02 g (P3). The slight increase in weight with thicker films correlates with the polymer concentration. Minimal weight variation indicates reproducibility of the film casting process.
Folding endurance
The folding endurance of the transdermal films, which reflects their mechanical strength and flexibility, was found to be 83 ± 0.15, 79 ± 0.07, and 74 ± 0.09 for P1, P2, and P3, respectively. A gradual decrease in folding endurance was observed with increasing polymer concentration or film thickness, indicating slightly reduced flexibility in thicker films. Despite this, all formulations exhibited adequate mechanical strength to withstand handling and application, with P1 showing the highest flexibility and P3 demonstrating comparatively greater stiffness.
Drug content uniformity
The drug content uniformity for P1, P2, and P3 was 86.2 ± 0.59%, 80.3 ± 0.045%, and 78.3 ± 0.032%, respectively. A slight decrease in drug content with increasing polymer concentration was observed, possibly due to increased polymer matrix density affecting drug dispersion.
Tensile strength
The tensile strength of the transdermal films was 2.90 ± 0.23, 2.73 ± 0.27, and 1.91 ± 0.21 kg/cm² for P1, P2, and P3, respectively. P1 showed the highest strength, indicating it is the most resistant to breaking, while P3 was the weakest. All films had enough strength to handle and use without breaking, with P1 being the strongest and most durable.
Percentage moisture content
The percentage moisture content of the films was 2.97 ± 0.40% (P1), 3.35 ± 0.33% (P2), and 3.45 ± 0.51% (P3). Lower moisture content, as seen in P1, is generally preferable because it ensures better stability of the drug and prevents microbial growth, while still maintaining adequate flexibility. Therefore, P1 is the best in terms of moisture content.
Table 4: Post Evaluation Studies of Transdermal Patches
|
Evaluation parameters |
P1 |
P2 |
P3 |
|
Physical appearance |
Whitish yellow, flexible ,smooth |
Whitish yellow, flexible ,smooth |
Whitish yellow, flexible ,smooth |
|
Film thickness(mm) |
0.132±0.01 |
0.153±0.03 |
0.169±0.04 |
|
Weight variation(g) |
0.430±0.02 |
0.562±0.04 |
0.567±0.02 |
|
Folding endurance |
83 ±0.15 |
79 ±0.07 |
74 ±0.09 |
|
Drug content uniformity |
86.2 ± 0.59 |
80.3 ± 0.045 |
78.3 ± 0.032 |
|
Tensile strength(kg/cm2) |
2.90±0.23 |
2.73±0.27 |
1.91±0.21 |
|
Percentage moisture content(%) |
2.97 ±0.40 |
3.35 ±0.33 |
3.45 ±0.51 |
n±3
IN VITRO DRUG RELEASE STUDY
The in-vitro drug release from the rizatriptan transdermal patches showed that P1 released the highest amount of drug (95.45 ± 0.22% at 360 min), followed by P2 (83.43 ± 0.26%) and P3 (76.23 ± 0.32%)as shown in Table 5 and Figure 6 . P1 exhibited the fastest and most complete release because it has the lowest polymer concentration and thinnest film thickness, which reduces the diffusion barrier and allows the drug to permeate more easily through the membrane. In contrast, P2 and P3 have thicker and denser polymer matrices, which slow drug diffusion and result in more sustained release. Therefore, P1 is considered the best formulation for achieving rapid and effective drug delivery.
Table 5: In-vitro permeation studies data of rizatriptan transdermal patch P1to P3
|
Time in minutes |
% cumulative drug release |
|
|
|
|
P1 |
P2 |
P3 |
|
15 |
8.02±0.12 |
6.7±0.41 |
5.0±0.52 |
|
30 |
16.61±0.21 |
14.25±0.32 |
12.12±0.21 |
|
60 |
25.94±0.32 |
23.09±0.11 |
20.34±0.36 |
|
120 |
49.92±0.11 |
32.86±0.21 |
29.87±0.21 |
|
180 |
67.85±0.22 |
49.32±0.32 |
38.12±0.24 |
|
240 |
76.45±0.31 |
60.12±0.24 |
54.43±0.21 |
|
360 |
95.45±0.22 |
83.43±026 |
76.23±0.32 |
n±3
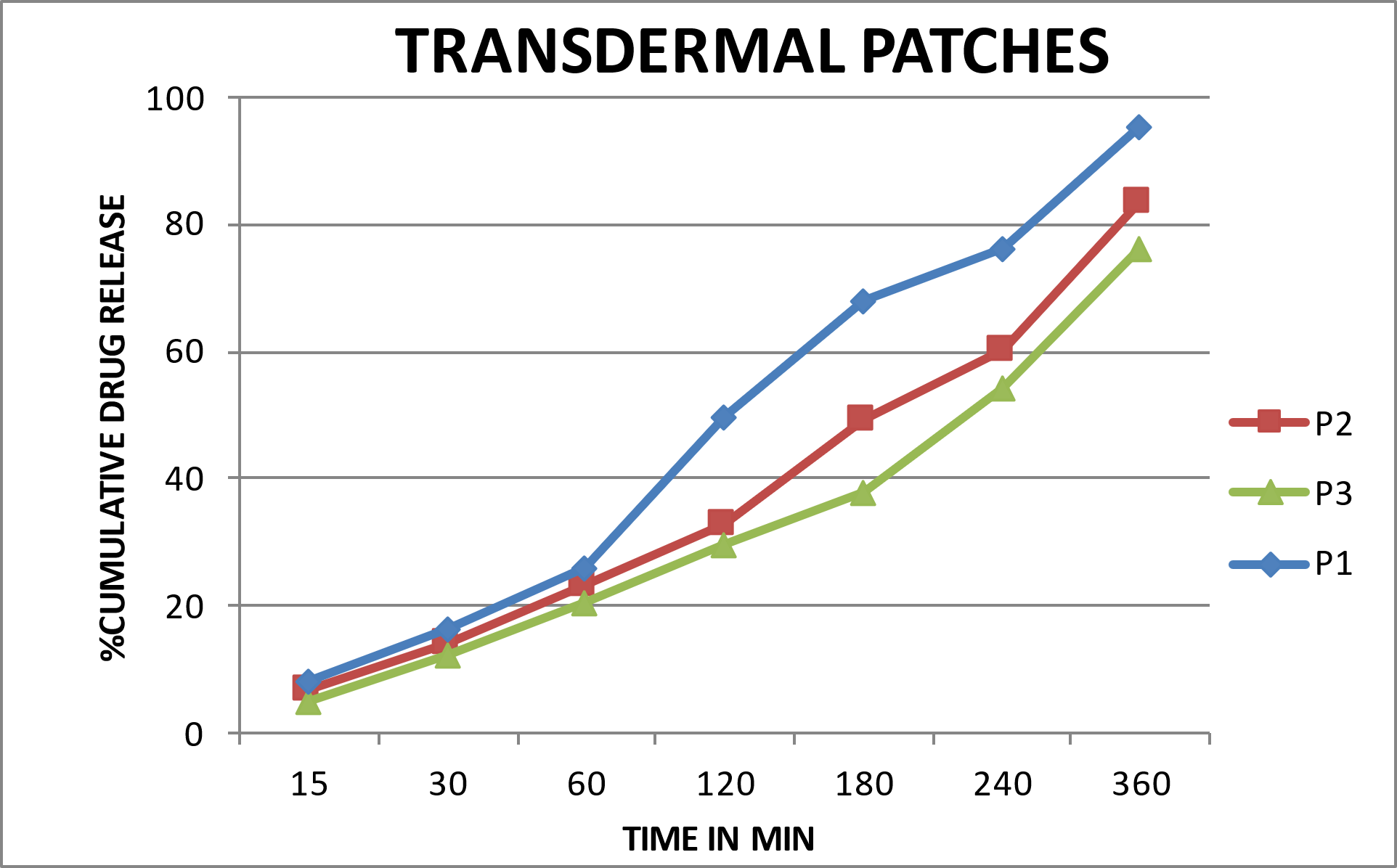
Figure 6: In-vitro permeation studies data of rizatriptan
Stability Study
The P1 transdermal patch exhibited excellent stability when stored for 3 months under accelerated conditions (40?°C ± 2?°C / 75% RH ± 5% RH). The patch remained transparent throughout the study, indicating no physical changes such as cracking, peeling, or discoloration. The in vitro drug release remained high at 93.63 ± 0.2%, and the drug content stayed well within acceptable limits at 84.01 ± 0.21%.These results demonstrate that P1 maintains its physical integrity, drug release performance, and chemical stability even under harsh conditions, highlighting the effectiveness of the optimized polymer matrix and low moisture content. Therefore, P1 is a robust and reliable formulation suitable for long-term storage and use. The results of the stability study are presented in Table 6.
Table 6: Stability studies of the Rizatriptan Transdermal Patch Formulation P1
|
Formulation code |
Days |
Appearance |
in-vitro diffusion release |
% Drug content |
|
P1 |
0 |
Transparent |
95.45±0.2 |
86.20±0.59 |
|
|
15 |
Transparent |
94.75±0.2 |
85.75±0.13 |
|
|
30 |
Transparent |
94.45±0.2 |
84.96±0.16 |
|
|
45 |
Transparent |
94.05±0.2 |
84.58±0.12 |
|
|
60 |
Transparent |
93.95±0.2 |
84.36±0.11 |
|
|
90 |
Transparent |
93.63±0.2 |
84.01±0.21 |
n±3
CONCLUSION
The present study successfully developed and evaluated rizatriptan benzoate transdermal patches using HPMC K100 as the polymer. Among the formulations, P1 emerged as the best, demonstrating optimal thickness, uniform drug content, highest tensile strength, and lowest moisture uptake, ensuring both stability and mechanical integrity. In vitro studies revealed that P1 achieved the maximum drug release (95.45%) within 360 minutes, attributed to its thinner matrix and reduced diffusion barrier.
Furthermore, stability studies under accelerated conditions confirmed the robustness of P1, with no significant changes in appearance, drug content, or release profile. Overall, the findings highlight that P1 is a stable, efficient, and patient-friendly transdermal delivery system for rizatriptan, capable of overcoming the limitations of oral therapy such as low bioavailability and short half-life, thereby offering a promising alternative for effective migraine management.
CONFLICT OF INTEREST: All authors declare that there is no conflict of interest regarding the publication of this paper.
REFERENCES


Dr. J. Gomathi, V. Dharani, A. Priyanka, M. Sowmiya, K. M. Thenmozhi, Transdermal Patch-Based Delivery of Rizatriptan Benzoate: A Novel Strategy for Migraine Treatment, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1472-1482 https://doi.org/10.5281/zenodo.19482678
 10.5281/zenodo.19482678
10.5281/zenodo.19482678
