We use cookies to make sure that our website works properly, as well as some ‘optional’ cookies to personalise content and advertising, provide social media features and analyse how people use our site. Further information can be found in our Cookies policy
To get around the challenges of oral medicine delivery, the transdermal drug delivery method was developed. A transdermal patch is an adhesive pharmaceutical patch applied to the skin that allows a prescribed dosage to enter the bloodstream through the skin. This frequently aids in the recovery of a damaged body part. The preparation techniques for several transdermal patch types, including matrix patches, reservoir type, membrane matrix, drug-in-adhesive patches, and micro reservoir patches, are covered in this review article. Additionally, a study of the several transdermal dosage form evaluation techniques has been conducted. Transdermal drug delivery is a very appealing and cutting-edge method of getting medications through the skin since it can have a systemic effect. Given the current situation, producing safe medications with fewer harmful side effects associated with the majority of pharmacologically active substances requires particular attention. Transdermal drug delivery is a key paradigm that offers patients convenience, avoidance of first-pass hepatic metabolism, local targeting, and a decrease in toxic effects associated with a variety of drug classes, including analgesics, anti-inflammatory, antibiotics, antivirals, anaesthetics, and anticancer medications. The highly ordered structure of the skin, which serves as the primary barrier to drug penetration via the skin, makes even this route difficult. Nowadays, transdermal patches are widely employed as topical, transdermal, and cosmetic delivery systems. These patches are a major result of the advancements in skin science, technology, and expertise that have been made possible by clinical observation, trial-and-error, and evidence-based research that goes all the way back to the first human records. This review starts with the first topical treatments and tracks topical distribution to the contemporary transdermal patches, outlining the early trials, tools, and drug delivery systems that support the active ingredients in transdermal patches today. This is followed by consideration of the evolution in the various patch designs and their limitations as well as requirements for actives to be used for transdermal delivery. The properties of and issues associated with the use of currently marketed products, such as variability, safety and regulatory aspects ,are then described. Their view concludes by examining future prospects for transdermal patches and drug delivery systems ,such as the combination of active delivery systems with patches ,minimally invasive microneedle patches and cutaneous solutions, including metered-dose systems.
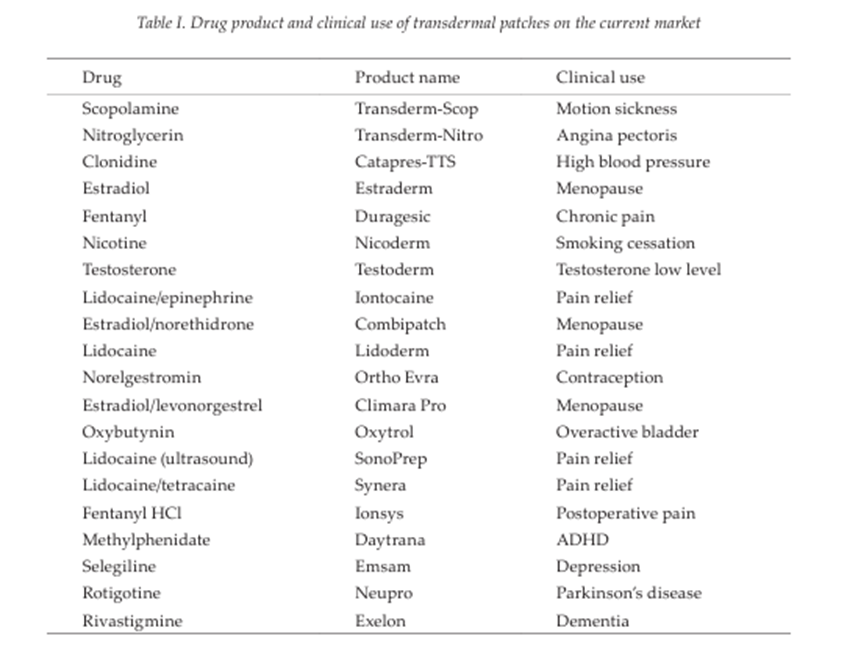
To provide a precise dosage of medication through the skin and into the bloodstream, a transdermal patch is utilised. The FDA initially authorised transdermal patches in 1981. There are currently transdermal delivery systems that contain nicotine to help people quit smoking, fentanyl for chronic pain, clonidine and nitroglycerin for cardiovascular illness, and scopolamine (hyoscine) for motion sickness. Transdermal delivery removes pulsed entry into the systemic circulation, permits continuous input of medications with brief biological half-lives, and offers controlled, continuous drug administration 1. Compared to traditional injection and oral techniques, TDDS has numerous benefits.. It lessens the strain that the oral route often puts on the liver and digestive system. It improves patient adherence and reduces negative pharmacological adverse effects brought on by transient overdose. It is particularly useful for patches that only need to be applied once a week. Patient adherence to medication therapy is facilitated by such a straightforward dose schedule2.
The main components to a transdermal patch are:
Polymer matrix–backbone of TDDS, which regulates the drug's release. The polymer should be nontoxic, chemically non-reactive, and not break down while being stored. It should also be reasonably priced. For instance, zein, gelatin, shellac, cellulose derivatives, gums, waxes, Silicon rubber, nitrile, acrylonitrile, polybutadiene, hydrin rubber, polyisobutylene, neoprene, Polyacrylate, polyamide, polyurea, polyvinyl alcohol, polyvinyl chloride, polyethylene, polypropylene, polyvinylpyrrolidone, and polymethylmethacrylate3.
Drug- For medications with the right pharmacology and physical chemistry, the transdermal route is a very alluring choice. Transdermal patches provide numerous medications that endure a lengthy first pass metabolism, medications with a limited therapeutic window, or medications with a brief half-life. such as nitroglycerine, fenatyl, etc.
Permeation enhancers- Enhance the stratum corneum's permeability to get greater medication therapeutic concentrations. These come in three varieties: surface active, lipophilic solvent, and agents as well as two separate systems. For instance, DMSO4
Adhesive-Increasing the stratum corneum's permeability will let the medication reach higher therapeutic levels.
Backing laminates-should be highly flexible or have a low modulus. such as polyethylene and vinyl.
Release liner- keeps the patch safe while being stored. Before using, the liner is taken out.
Other excipients like plasticizers and solvents 5.
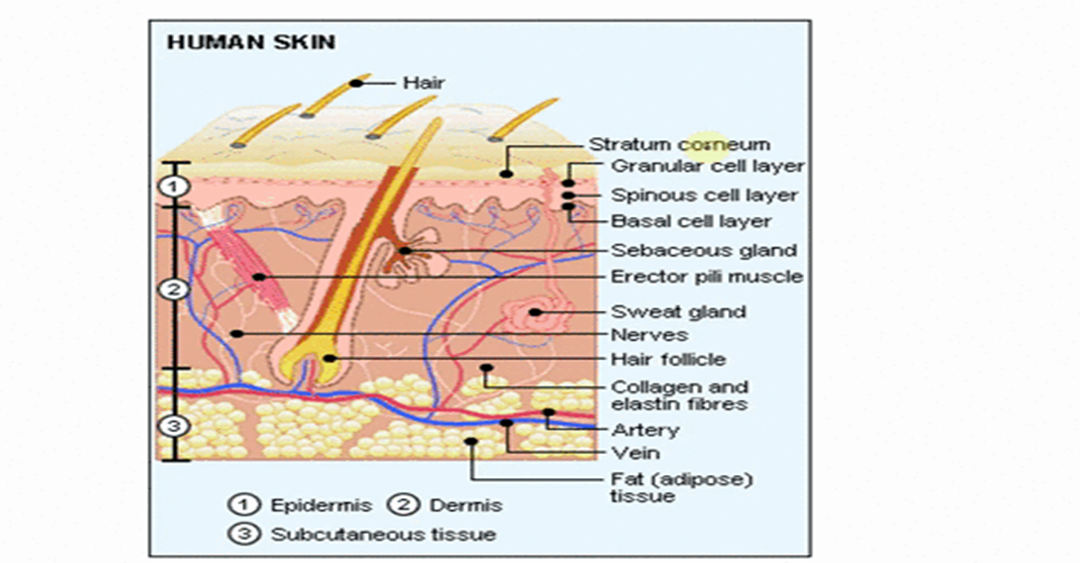
Drug Delivery Routes across Human Skin
Drug molecules can penetrate by three pathways:
Sweat ducts
Hair follicles
Sebaceous glands
or
Directly across the stratum corneum.
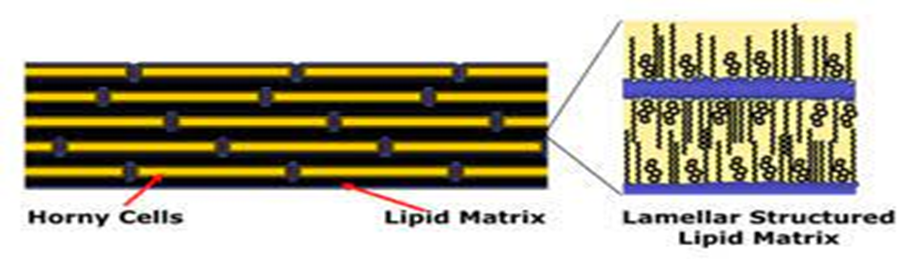
Large, flat, polyhedral, plate-like envelopes filled with keratin—a substance derived from dead cells that have moved up from the stratum granulosum—make up the stratum corneum, the outermost layer of the epidermis. Dead cells devoid of nuclei make up the majority of this skin layer. New cells from the stratum germinativum (basale) continuously replace these dead cells when they slough off on the surface in the thin, air-filled stratum disjunctum. The thickness of the stratum corneum, which is made up of 10–15 layers of corneocytes, ranges from around 10–15 μm when dry to 40 μm when hydrated. It primarily consists of a multi-layered "brick and mortar" structure.In an intercellular matrix (mortar) made up of long chain ceramides, free fatty acids, triglycerides, cholesterol, cholesterol sulphate, and sterol/wax esters, the structure of keratin-rich corneocytes (bricks) is similar. Keratinocytes in the middle to upper stratum granulosum release their lamellar contents into the intercellular space, generating the intercellular lipid matrix. The tratum corneum's first layers reorganise to create wide, intercellular lipid lamellae, which subsequently unite to form lipid bilayers. The lipid phase behaviour differs from that of other biological membranes due to the lipid content of the stratum corneum. A vital component of the stratum corneum, water serves as a plasticiser to keep it from cracking and contributes to the production of natural moisturising component that keeps the skin soft. Determining the main route of drug penetration within the stratum corneum is crucial to comprehending the physicochemical characteristics of the spreading drug and vehicle effect throughout the stratum corneum. A molecule moving across For the majority of medications, it is detrimental to diffuse into and across several hydrophilic and hydrophobic domains. As a result, it is presently thought that the intercellular route is the main mechanism that most medications pass through the stratum corneum6.
Fig. 1: Transverse section of skin showing routes of penetration 1. Through the sweat ducts; 2. Directly across the stratum corneum; 3. Via the hair follicles2
Fig. 2: Schematic structure of the stratum corneum according to the brick-and-mortar model3.
For more than ten years, transdermal medication delivery patches have been available on the market4.Over-the-counter nicotine patches that aid in quitting smoking are the most widely used transdermal drug delivery patches. The term "transdermal drug delivery patch" raises a number of queries, like what kind of material it is composed of, how it operates, and so on. Transdermal patches were initially developed to treat motion sickness in astronauts travelling into space7.However, a few drawbacks have prevented this medication delivery technology from reaching its full potential. The quantity of medications may be restricted by localised skin irritation and sensitisation. Effective transdermal medications possess molecular masses that are only a few hundred Daltons, which thus restricts the drug's dosage. Other drawbacks include delayed absorption, high prescription costs, and challenges in administering hydrophilic medications8.For both local effects and systemic therapy, transdermal drug delivery systems are sustained and controlled release devices that deliver medications or other therapeutic agents, such as peptides, nucleic acids, etc. via application on the skin's surface9. Although many transdermal systems with various medications have been developed, their practical application is restricted by the skin's penetration barriers. Many techniques have been developed and patented to aid with transdermal absorption10. These innovative technologies include, for example, electroporation, iontophoresis, microneedles, ultrasound, and above all the application of nanotechnology11. With an area of 1.5 to 2.0 m2 in adults, the skin is the biggest organ in the human body by mass. Since the beginning of human history, drugs have been administered topically to cure surface conditions, transdermally to administer therapies to treat systemic illnesses, and as cosmetics. For example, ancient Egyptian and Babylonian medicine (c. 3000 BC) already widely used salves, ointments, potions, and even patches made of plant, animal, or mineral extracts. (Geller, 2010; Magner, 2005). However, it wasn't until the latter part of the 20th century that transdermal delivery methods became widely used, thanks to advancements in delivery technology that made it possible to administer medications precisely and consistently through the skin for systemic effects. The goal of every pharmaceutical firm and researcher is to create a safe and effective medication delivery system 12. Drug administration via the transdermal method can provide both systemic and local therapeutic effects 13. Since transdermal drug delivery avoids gastrointestinal side effects and first pass metabolism, it is a desirable alternative to oral drug administration. Additionally, it can overcome the low patient compliance that is linked to other drug delivery methods 14. Self-administered transdermal drug delivery enables the medication to enter intact skin over a predetermined amount of time to produce a local or systemic effect15.
TDDS Classification Based on Their Technical Sophistication:
Rate pre-programmed drug delivery system
Activation modulated drug delivery system
Feedback regulated drug delivery system
Carrier based drug delivery system
a) Rate Pre-Programmed Drug Delivery System: Involves the creation of a system that administers medication by regulating the molecular diffusion of drug molecules within or around the delivery system across the eIt pidermal barrier16.
Polymer membrane permeation-controlled drug delivery system: Includes the system where the medication is contained inside a medication reservoir .This is taken care of by the polymer's semipermeable barrier, which controls release and has a particular Permeability17. There is some possibility development using the membrane process Microporous membranes allow for penetration. Stomach fluid resistance intestine targeted controlled release gastrointestinal device, gel diffusion-controlled medication delivery system, and permeation controlled gastrointestinal delivery device.
Polymer matrix diffusion-controlled drug delivery system : It is created by uniformly spreading drug particles within a rate-controlling carrier matrix. For instance, NitroDur. It provides a consistent transdermal infusion of nitroglycerine and is intended to be applied to intact skin for 24 hours18.
Microreservoir partitioned controlled drug delivery system : It uses high energy dispersion to distribute drug solution microparticles (which are aqueous in nature) throughout a polymer. For instance. The Syncromate implant was designed to administer Norgestomet19 subcutaneously.
b) Activation Modulated Drug Delivery System :This type of delivery system can be achieved by
Physical means:
Hydrodynamic pressure-controlled medication delivery system; osmotic pressure-activated drug delivery system.
A drug delivery device that is activated by vapour pressure.
A drug delivery mechanism that is mechanically actuated.
A drug delivery method that is magnetically actuated.
A drug delivery system that is electrically actuated.
A drug delivery device that is activated by ultrasound.
A drug delivery mechanism that is activated by hydration.
Chemical means:
pH activated drug delivery system.
Ion activated drug delivery system.
Hydrolysis activated drug delivery system.
Biochemical means:
Enzymes activated drug delivery system.
Feedback Regulated Drug Delivery System: An agent that initiates the release of the drug, such as biochemicals, facilitates the release of the drug molecules from the transdermal system. In the body and is also controlled by its concentration via a feedback mechanism20.
Bio-erosion regulated drug deliverysystem.
Bio-responsive drug delivery system.
Self regulated drug delivery system17.
Carrier Based Drug Delivery System (Colloidal particulates carrier system): Hydrogels and other vesicular systems are involved microerythrosomes, microspheres, Aquasomes, dendrimers, transferosomes, etc21.They are favoured over the oral method of medication delivery because theysystemic circulation due to a number of favourable factors;
2. ADVANTAGES OF TRANSDERMAL PATCHES:
There is an improvement and an increase in bioavailability.
Some patients have trouble swallowing pills and capsules.
In order to facilitate swallowing, patients are tempted to smash medications, which eliminates the pills' controlled release properties.
They are favoured over more uncomfortable hypodermic injections.
Provide a risk of disease transmission and produce medical waste22.
Increased patient cooperation because the procedure is easy, non-invasive, and practical, and there is more freedom in how medications are discontinued. through patch removal.
Drugs delivered through the skin under control can offer less fluctuation and lower the concentration of the medication increase seen following the medications used orally23 .
3. DISADVANTAGES OF TRANSDERMAL PATCHES:
The potential for local discomfort at the application location.
The medication, the adhesive, or additional excipients in the patch formulation may result in erythema, irritation, and local oedema.
Could result in allergic responses24.
It is necessary to have a molecular weight below 500 Da.
A log P (octanol/water) of 1 to 3 is necessary for the permeate to cross the SC and underlying aqueous layers, indicating adequate aqueous and lipid solubility.
4. TYPES OF TRANSDERMAL PATCHES :
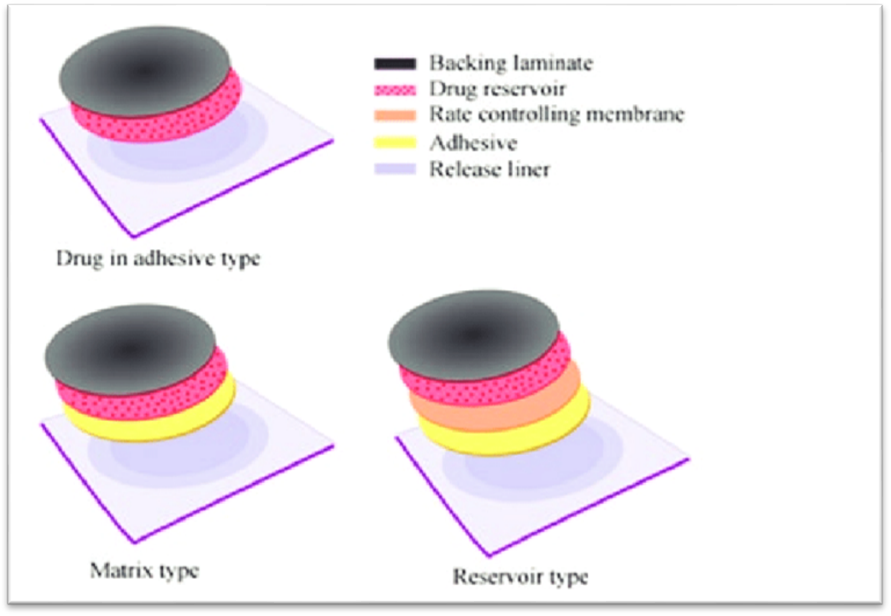
Single layer drug in adhesive patches: A single layer of an adhesive polymer serves as a drug dispersion reservoir in Figure 1. The single layer is covered with an impermeable backing laminate. The medication is released from the backing laminate layer supporting the drug reservoir after being deposited in and adhering to the single polymer layer25. One example of a single layer drug-in-adhesive transdermal patch that contains methylphenidate is the transdermal medication Daytrana®.
Multilayer drug in adhesive patches: A drug reservoir layer and an adhesive layer with regulated medication release over time make up multilayer transdermal patches26. Multilayer systems comprise both a permanent backing laminate and a temporary protective layer. Multilayer patches are used to administer hormone therapy, painkillers, and medications that promote quitting smoking; the duration of drug delivery can be up to seven days.
Vapour transdermal patches: A single layer of sticky polymer with a vapour release feature that allows vapour to be released makes up vapour transdermal patches27. There are several vapour dermal patches on the market, each with a distinct function. Nicoderm CQ®, for instance, are transdermal patches that contain nicotine vapour and essential oils that, when released, can aid in quitting smoking. In 2007, this product made its debut on the European market. Another kind of vapour patch that contains essential oils and can be used for decongestion is Altacura®. There are different kinds of vapour patches on the market that are used as sedatives or antidepressants28 (Table I).
Membrane moderated transdermal reservoir patches:A transdermal patch with a drug reservoir, an impermeable metallic plastic laminate backing layer, and a porous polymeric membrane that regulates drug release over time is seen in Fig. 1. Polymeric materials, such as ethylene vinyl acetate copolymer and hypoallergenic adhesive polymer, are used to make the membrane. The drug's molecular dispersion in a polymer matrix portion of the preparation regulates the drug's presence in the transdermal patch29. Commercial transdermal patches with modified drug release include Catapres®, which contains clonidine for seven days, Transderm-Nitro®, which contains nitroglycerin for one day, and Transderm-Scop®, which contains scopolamine for three days (Table I).
Fig. 1. Schematic diagram of various types of transdermal patches.
Microreservoir Transdermal Patches: Matrix dispersion and a drug reservoir are combined in microreservoir transdermal patches. The reservoir is made by spreading the drug suspension uniformly on a lipophilic polymer after it has been suspended in an aqueous solution of hydrophilic polymer30. Thousands of tiny, insoluble spheres are formed as a result of the strong shear mechanical stress used during dispersion. The drug level in the plasma is kept constant by the drug release profile, which adheres to a zero order rate of kinetic drug release. Since the medication dispersion must be thermodynamically stable, crosslinking polymeric agents are typically included31.
Matrix system: drug-in-adhesive:As illustrated in Fig. 1, the drug reservoir is made to disperse the medication on an adhesive polymer using single layer or multilayer transdermal patches. Either solvent casting or melting the sticky polymeric elements are used to deposit this drug-polymer matrix onto an impermeable backing layer32. There are several commercial products of this kind of transdermal patch on the market. For instance, the NicoDerm® CQ transdermal patch contains nicotine to promote quitting smoking for up to 10 weeks, and the Climara® transdermal patch contains 100 microgrammes of oestradiol for one-day application (Table I).
Matrix systems: Matrix-dispersion:A hydrophilic or lipophilic polymer matrix serves as the reservoir in a matrix transdermal patch, and the medicine is uniformly distributed throughout the matrix33 by covering the plate with an impermeable laminate backing. A continuous medication flow through undamaged skin is provided by commercial matrix dispersion patch products like Nitro-Dur®, which comprises nitroglycerin and minitran (Table I).
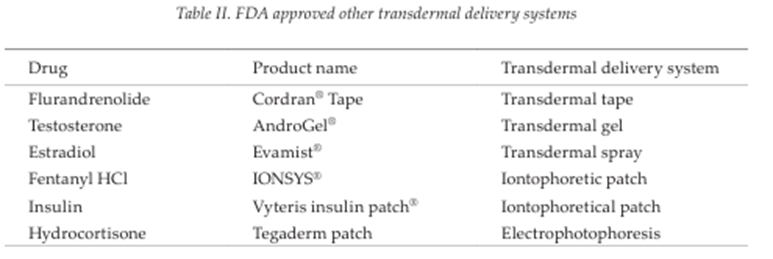
Miscellaneous transdermal patches: Transdermal patches with adhesive tapes, transdermal gel, transdermal spray, iontophoretic delivery, and photophoresis delivery are other FDA-approved transdermal matrix delivery methods, as indicated in Table II34.
5. Evaluation Parameters:
Thickness of the patch: Using a digital micrometre, the thickness of the drug-loaded patch is measured at several sites. To guarantee the thickness of the prepared patch, the average thickness and standard deviation are calculated. Transdermal film thickness is measured at several locations on the film using a micrometre, screw gauge, or travelling microscope dial gauge35.
Weight uniformity: Before testing, the created patches are dried for four hours at 60°C. A predetermined patch area needs to be chopped into several pieces and weighed using a digital balance. The individual weights must be used to get the average weight and standard deviation values36.
Folding endurance: It is necessary to cut an even strip of material and fold it repeatedly at the same spot until it breaks. The folding endurance of a film is determined by how many times it can be folded in the same spot without breaking37.
4. Percentage Moisture content: Each produced film must be weighed separately and stored for 24 hours at room temperature in a desiccator filled with fused calcium chloride. The films must be reweighed after 24 hours in order to calculate the percentage moisture content using the formula below38.
5. Content uniformity test: Ten patches are chosen, and each patch's content is established. Transdermal patches pass the content uniformity test if the content of nine of ten patches is between 85% and 115% of the prescribed value, and one patch has at least 75% to 125% of the stated value. However, 20 more patches are examined for drug content if three of them contain content between 75% and 125%. The transdermal patches pass the test if the range of these 20 patches is between 85% and 115%39.
6. Moisture Uptake: Films that have been weighed are stored for 24 hours at room temperature in desiccators. After that, they are removed and placed in desiccators with a saturated potassium chloride solution at 84% relative humidity until their weight remains constant. The percentage of moisture uptake is computed as follows:40
7. Drug content: A certain volume of a patch must be dissolved in an appropriate solvent. After that, the solution must be filtered through a filter medium, and the drug content must be examined using the appropriate technology (either the UV or HPLC method). The average of three distinct samples is shown by each value41.
8. Tensile strength: A tensile tester (Shimadzu Autograph AG-X, Japan) assessed the patches' tensile strength. The tested patches were positioned between cell grips after being trimmed to a size of 4 × 1 cm2. The film was subjected to force until it broke42. The dial reading in kilogrammes was used to calculate the patches' tensile strength. The following formula was used to determine the patches' tensile strength: 43
9. Shear Adhesion test: The purpose of this test is to determine an adhesive polymer's cohesive strength44. The molecular weight, degree of cross linking, polymer composition, kind, and quantity of tackifier used can all have an impact. A stainless steel plate is covered with adhesive-coated tape, and to make the tape pull parallel to the plate, a certain weight is suspended from it. The time it takes to remove the tape from the plate is used to calculate the shear adhesion strength. The shear strength45 increases as removal time increases.
10. Peel Adhesion test: Peel adhesion is the term used in this test to describe the force needed to remove an adhesive covering from a test substrate. The variables that influenced the peel adhesion qualities were the adhesive polymer's molecular weight and the kind and quantity of additives. The force needed to remove a single piece of tape is measured after it has been attached to a stainless steel plate or a preferred backing membrane. The tape is then lifted from the substrate at a 180º angle46.
11. Water vapor transmission studies (WVT): Weigh one gramme of calcium chloride and put it in previously dried, empty vials with the same diameter to determine WVT. Using an adhesive such as silicon adhesive grease, the polymer films are applied to the brim and left to set for five minutes. The vials are then precisely weighed and put in a humidity chamber that is kept at 68% relative humidity. The vials are measured once more at the conclusion of the first, second, and third days for a total of seven days in a row. A weight rise was regarded as a quantitative indicator of the amount of moisture that was transferred through the patch. In a different procedure that was published, vials containing 200 mL of saturated sodium bromide and saturated potassium chloride solution were placed in desiccators47.The desiccators were sealed tightly, and a hygrometer was used to measure the humidity within. The process was then repeated after the weighed vials were put in desiccators. WVT is equal to W/ST. W is the weight increase during a 24-hour period; S is the exposed film area (cm2); and T is the exposure time 48.
12. Rolling ball tack test: This test evaluates a polymer's talk-related softness. In this test, a 7/16-inch-diameter stainless steel ball is dropped upon an incline so that it rolls downward and encounters horizontal, upward-facing adhesive. Tack, which is measured in inches 17, is determined by the distance the ball goes along the adhesive49.
13. Quick Stick (peel-tack) test: In this test, the tape is dragged 12 inches per minute away from the substrate at 90 degrees Celsius. Tack value, which is measured and documented as the peel force necessary to break the adhesive-substrate bond, is given in ounces or grammes per inch width 50.
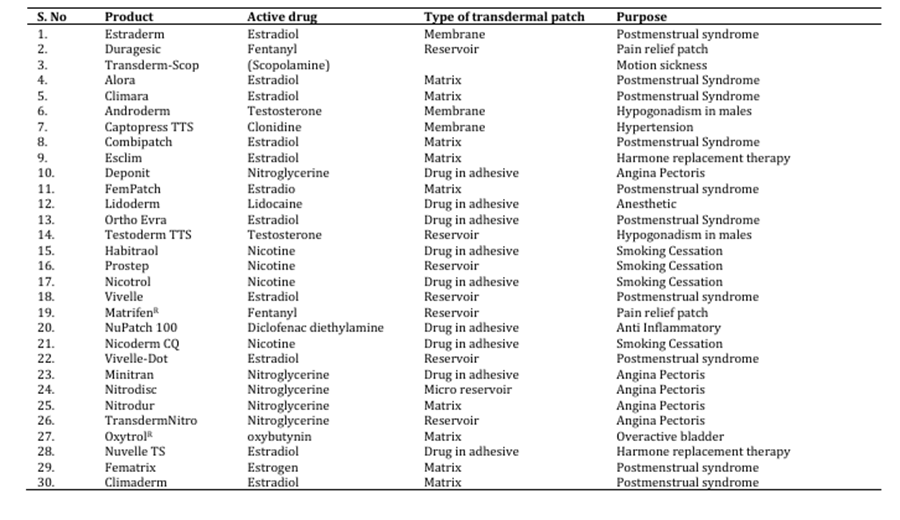
Table 3: : Marketed Products of Transdermal Drug Delivery System
CONCLUSION:
Since 1981, transdermal drug administration systems have been employed as secure and efficient medication delivery tools. In the field of transdermal patches, significant advancements have been made. Many researchers are interested in the Transdermal Drug Delivery System because of its many benefits. Nowadays, a lot of new research is being done to use this system to incorporate newer medications. Transdermal dose forms might give doctors the chance to give their patients more treatment choices so that their care is optimised. Our knowledge of the nature of the stratum corneum barrier and how chemicals interact with and affect its structure has improved recently thanks to the application of several biophysical approaches. The establishment of structure-activity connections for enhancers and a deeper comprehension of how enhancers interact with the stratum corneum will help designers create enhancers with the best properties and the least amount of toxicity. Important aspects about transdermal drug delivery systems and their evaluation procedure are covered in full in this article.
REFERENCES
Gaur PK, Mishra S, Purohit S, Dave K. Transdermal drug delivery system- A review. Asian Journal of Pharmaceutical and Clinical Research. 2009; 2:14-20.
Aggarwal G, Dhawan S. Development, Fabrication and Evaluation of Transdermal Drug Delivery System - A Review. Pharmainfo.net. 2009; 7(5).
Heather AE. Transdermal Drug Delivery: Penetration Enhancement Techniques. Current Drug Delivery. 2005; 2:23-33.
Tanner T, Marks R. Delivering drugs by the transdermal route: Review and comment. Skin Res Technol 2008;14(3):249-60
Rizwan, M.; Aqil, M.; Talegaonkar, S.; Azeem, A.; Sultana, Y.; Ali, A. Enhanced transdermal drug delivery techniques: an extensive review of patents. Recent Pat. Drug Deliv. Formul., 2009, 3, 105-124.
Barry, B.W. Novel mechanisms and devices to enable successful transdermal drug delivery. Eur. J. Pharm. Sci., 2001, 14, 101-114.
Merino, V.; Lopez, A. Transdermal Iontophoresis. In: Escobar Chávez, J. Ed.; Current Technologies to Increase the Transdermal Delivery of Drugs; Bentham Science Publishers: The Netherlands, 2010; pp.41-52.
Escobar-Chávez, J.J.; Bonilla-Martínez, D.; Villegas-González, M.A.; Revilla-Vázquez, A.L. Electroporation as an efficient physical enhancer for skin drug delivery. J. Clin. Pharmacol., 2009, 49, 1262-1283.
L. Zhang and S. Mao, Application of quality by design in the current drug development, As. J. Pharm. Sci. 12 (2017) 1–8; https://doi.org/10.1016/j.ajps.2016.07.006.
M. R. Prausnitz and R. Langer, Transdermal drug delivery, Nat. Biotechnol. 26 (2008) 1261–1268; https://doi.org/10.1038/nbt.1504.
M. J. Tsai, I. J. Lu, Y. S. Fu, Y.P. Fang, Y. B. Huang and P. C. Wu, Nanocarriers enhance the transder mal bioavailability of resveratrol: In-vitro and in-vivo study, Colloids Surf. B Biointerfaces 148 (2016) 650–656; https://doi.org/10.1016/j.colsurfb.2016.09.045.
M. Arafat, Approaches to achieve an oral controlled release drug delivery system using polymers: a recent review, Int. J. Pharm. Pharm. Sci. 7 (2015) 16–21.
Keith, AD (1983), “Polymer matrix consideration for Transdermal Devices”, Drug Dev. Ind Pharm, Vol.9, 605-625.
Karim, A (1983), “Transdermal absorption: a unique opportunity for constant delivery of nitroglycerin. Drug Dev. Ind Pharm, Vol.9, 671.
Helier, J and Trescony, PV (1979), “Controlled drug release by polymer dissolution II, Enzyme mediated delivery device, J. Pharm. Sci., Vol.68, 919.
Snigdha, B, Sharma, PK; Garg, VK; Kumar, N and Bansal, M (2011), “Recent advancement in transdermal drug delivery system”, Int. Pharma Prof. Res., Vol. 2(1), 247-254.
Williams A. Transdermal and Topical Drug Delivery. London: Pharmaceutical Press; 2003.
Glenn GM, Kenney RT. Mass vaccination: Solutions in the skin. Curr Top Microbiol Immunol 2006;304:247-68.
M. Imani, F. Lahooti-Fard, S. M. Taghizadeh and M Takrousta, Effect of adhesive layer thickness and drug loading on estradiol crystallization in a transdermal drug delivery system, AAPS Pharm. Sci. Tech. 11 (2010) 1268–1275; https://doi.org/10.1208/s12249-010-9494-9.
S. Dhiman, T. G. Singh and A. K. Rehni, Transdermal patches: A recent approach to new drug de livery system, Int. J. Pharm. Pharm. Sci. 3 (2011) 26–34.
S. Rani, K. Saroha, N. Syan and P. Mathur, Transdermal patches a successful tool in transdermal drug delivery system: An overview, Der Pharm. Sinica 2 (2011) 17–29.
B. Berner and V. A. John, Pharmacokinetic characterization of transdermal delivery system, J. Clin. Pharmacol. 26 (1994) 121–134.
S. Mutalik and N. Udupa, Pharmacological evaluation of membrane-moderated transdermal system of glipizide, Clin. Exp. Pharmacol. Physiol. 33 (2006) 17-26.
C. L. Stevenson, J. T. Jr. Santini and R. Langer, Reservoir-based drug delivery systems utilizing microtechnology, Adv. Drug Deliv. Rev. 64 (2012) 1590–1602; https://doi.org/10.1016/j.addr.2012.02.005.
P. J. Hughes, M. K. Freeman and T. M. Wensel, Appropriate use of transdermal drug delivery sys tems, J. Nurs. Edu. Pract. 3 (2013) 129–138.
S. Cherukuri, U. R. Batchu, K. Mandava, V. Cherukuri, K. R. Ganapuram, Formulation and evalua tion of transdermal drug delivery of topiramate, Int. J. Pharm. Investig. 7 (2017) 10–17; https://doi. org/10.4103/jphi.JPHI_35_16.
Keleb E, Sharma RK, Mosa EB, Aljahwi A-AZ. Transdermal Drug Delivery System – Design and Evaluation. International Journal of Advances in Pharmaceutical Sciences. 2010; 1:201-211.
Rhaghuram RK, Muttalik S, Reddy S. Once – daily sustained- release matrix tablets of nicorandil: formulation and invitro evaluation. AAPS Pharm.SciTech. 2003; 4(4):480–488.
Shaila L, Pandey S, Udupa N. Design and evaluation of matrix type membrane controlled.
Aggarwal G, Dhawan S. Development, Fabrication and Evaluation of Transdermal Drug Delivery System - A Review. Pharmainfo.net. 2009; 7(5).
Keleb E, Sharma RK, Mosa EB, Aljahwi A-AZ. Transdermal Drug Delivery System – Design and Evaluation. International Journal of Advances in Pharmaceutical Sciences. 2010; 1:201-211.
Prajapati ST, Patel CG, Patel CN. Formulation and evaluation of transdermal patch of repaglinide. ISRN Pharm 2011;2011:1-9.
Baichwal MR. Polymer films as drug delivery systems, Advances in drug delivery systems. Bombay, MSR Foundation; 1985; 136-147.
Vyas SP, Khar RK. Targetted and controlled Drug Delivery Novel carrier system. 1st ed. CBS Publishers and distributors New Delhi; 2002; 411- 447.
J. Singh, K. Tripathi and T. Sakya, Effect of penetration enhancers on the in vitro transport of ephedrine through rat skin and human epidermis from matrix based transdermal formulations, Drug Dev. Ind. Pharm. 19 (1993) 1623–1628.
N. Maftoona, H. S. Ramaswamy and M. Marcotte, Evaluation of factors affecting barrier, mechanical and optical properties of pectin-based films using response surface methodology, J. Food. Process Eng. 30 (2007) 539–563; https://doi.org/10.1111/j.1745-4530.2007.00123.x
Singh and A. Bali, Formulation and characterization of transdermal patches for controlled delivery of duloxetine hydrochloride, J. Anal. Sci. Technol. 7 (2016) 25; https://doi.org/10.1186/s40543 016-0105-6
J. Wiechers, Use of chemical penetration enhancers in transdermal drug delivery – possibilities and difficulties, Acta Pharm Nord. 4 (1992) 123.
S. Banerjee, P. Chattopadhyay, A. Ghosh, P. Datta and V. Veer, Aspect of adhesives in transdermal drug delivery systems, Int. J. Adhes. Adhes. 50 (2014) 70–84.
M. Wokovich, S. Prodduturi, W. H. Doub, A. S. Hussain and L. F. Buhse, Transdermal drug delivery system (TDDS) adhesion as a critical safety, efficacy and quality attribute, Eur. J. Pharm. Biopharm. 64 (2006) 1–8.
J. Steven-Fountain, A. G. Atkins, G. Jeronimidis, J. F. V. Vincent, D. F. Farrar and R. A. Chivers, The effect of flexible substrates on pressure-sensitive adhesive performance, Int. J. Adhes. Adhes. 22 (2002) 423–430.
G. Thakur, A. Singh and I. Singh, Formulation and evaluation of transdermal composite films of chitosan-montmorillonite for the delivery of curcumin, Int. J. Pharm. Investig. 6 (2016) 23–31; https://doi.org/10.4103/2230-973X.176468
T. Kamal, M. Sarfraz, M. Arafat, M. Mikov and N Rahman, Cross-linked guar gum and sodium borate based microspheres as colon-targeted anticancer drug delivery systems for 5-fluorouracil, Pak. J. Pharm. Sci. 30 (2017) 2329–2336.
O. A. Hanbali, R. Hamed, M. Arafat, Y. Bakkour, H. Matubsi, R. Mansour, Y. Bataineh, M. Aldhoun, M. Sarfraz and A. K. Yousef Dardas, Formulation and evaluation of diclofenac controlled release matrix tablets made of HPMC and Poloxamer 188 polymer: An assessment on mechanism of drug release, Pak. J. Pharm. Sci. 31 (2018) 345–351.
T. Z. Marques, R. Santos-Oliveira, L. B. de Siqueira, V. S. Cardoso, Z. M. de Freitas, R. C. Barros, A. L. Villa, M. S. Monteiro, E. P. Santos and E. Ricci-Junior, Development and characterization of a nanoemulsion containing propranolol for topical delivery, Int. J. Nanomedicine 13 (2018) 2827–2837; https://doi.org/10.2147/IJN.S164404
S. Cerqueira-Coutinho, V. E. De Campo, A. L. Rossi, V. F. Veiga, C. Holandino, Z. M. Freitas, E. Ricci-Junior, C. R. Mansur, E. P. Santos and R. Santos-Oliveira, Comparing in vivo biodistribution with radiolabeling and Franz cell permeation assay to validate the efficacy of both methodologies in the evaluation of nanoemulsions: a safety approach, Nanotechnology 27 (2016) 015101; https://doi.org/10.1088/0957-4484/27/1/015101
J. Wang, Y. Wei, Y. R. Fei, L. Fang, H. S. Zheng, C. F. Mu, F. Z. Li and Y. S. Zhang, Preparation of mixed monoterpenes edge activated PEGylated transfersomes to improve the in vivo transdermal delivery efficiency of sinomenine hydrochloride, Int. J. Pharm. 533 (2017) 266–274; https://doi.org/10.1016/j.ijpharm.2017.09.059
Abu Hashim, N. F. Abo El-Magd, A. R. El-Sheakh and M. F. Hamed, Pivotal role of Acitretin nanovesicular gel for effective treatment of psoriasis: ex vivo–in vivo evaluation study, Int. J. Nanomedicine 13 (2018) 1059–1079; https://doi.org/10.2147/IJN.S156412
Reference
Gaur PK, Mishra S, Purohit S, Dave K. Transdermal drug delivery system- A review. Asian Journal of Pharmaceutical and Clinical Research. 2009; 2:14-20.
Aggarwal G, Dhawan S. Development, Fabrication and Evaluation of Transdermal Drug Delivery System - A Review. Pharmainfo.net. 2009; 7(5).
Heather AE. Transdermal Drug Delivery: Penetration Enhancement Techniques. Current Drug Delivery. 2005; 2:23-33.
Tanner T, Marks R. Delivering drugs by the transdermal route: Review and comment. Skin Res Technol 2008;14(3):249-60
Rizwan, M.; Aqil, M.; Talegaonkar, S.; Azeem, A.; Sultana, Y.; Ali, A. Enhanced transdermal drug delivery techniques: an extensive review of patents. Recent Pat. Drug Deliv. Formul., 2009, 3, 105-124.
Barry, B.W. Novel mechanisms and devices to enable successful transdermal drug delivery. Eur. J. Pharm. Sci., 2001, 14, 101-114.
Merino, V.; Lopez, A. Transdermal Iontophoresis. In: Escobar Chávez, J. Ed.; Current Technologies to Increase the Transdermal Delivery of Drugs; Bentham Science Publishers: The Netherlands, 2010; pp.41-52.
Escobar-Chávez, J.J.; Bonilla-Martínez, D.; Villegas-González, M.A.; Revilla-Vázquez, A.L. Electroporation as an efficient physical enhancer for skin drug delivery. J. Clin. Pharmacol., 2009, 49, 1262-1283.
L. Zhang and S. Mao, Application of quality by design in the current drug development, As. J. Pharm. Sci. 12 (2017) 1–8; https://doi.org/10.1016/j.ajps.2016.07.006.
M. R. Prausnitz and R. Langer, Transdermal drug delivery, Nat. Biotechnol. 26 (2008) 1261–1268; https://doi.org/10.1038/nbt.1504.
M. J. Tsai, I. J. Lu, Y. S. Fu, Y.P. Fang, Y. B. Huang and P. C. Wu, Nanocarriers enhance the transder mal bioavailability of resveratrol: In-vitro and in-vivo study, Colloids Surf. B Biointerfaces 148 (2016) 650–656; https://doi.org/10.1016/j.colsurfb.2016.09.045.
M. Arafat, Approaches to achieve an oral controlled release drug delivery system using polymers: a recent review, Int. J. Pharm. Pharm. Sci. 7 (2015) 16–21.
Keith, AD (1983), “Polymer matrix consideration for Transdermal Devices”, Drug Dev. Ind Pharm, Vol.9, 605-625.
Karim, A (1983), “Transdermal absorption: a unique opportunity for constant delivery of nitroglycerin. Drug Dev. Ind Pharm, Vol.9, 671.
Helier, J and Trescony, PV (1979), “Controlled drug release by polymer dissolution II, Enzyme mediated delivery device, J. Pharm. Sci., Vol.68, 919.
Snigdha, B, Sharma, PK; Garg, VK; Kumar, N and Bansal, M (2011), “Recent advancement in transdermal drug delivery system”, Int. Pharma Prof. Res., Vol. 2(1), 247-254.
Williams A. Transdermal and Topical Drug Delivery. London: Pharmaceutical Press; 2003.
Glenn GM, Kenney RT. Mass vaccination: Solutions in the skin. Curr Top Microbiol Immunol 2006;304:247-68.
M. Imani, F. Lahooti-Fard, S. M. Taghizadeh and M Takrousta, Effect of adhesive layer thickness and drug loading on estradiol crystallization in a transdermal drug delivery system, AAPS Pharm. Sci. Tech. 11 (2010) 1268–1275; https://doi.org/10.1208/s12249-010-9494-9.
S. Dhiman, T. G. Singh and A. K. Rehni, Transdermal patches: A recent approach to new drug de livery system, Int. J. Pharm. Pharm. Sci. 3 (2011) 26–34.
S. Rani, K. Saroha, N. Syan and P. Mathur, Transdermal patches a successful tool in transdermal drug delivery system: An overview, Der Pharm. Sinica 2 (2011) 17–29.
B. Berner and V. A. John, Pharmacokinetic characterization of transdermal delivery system, J. Clin. Pharmacol. 26 (1994) 121–134.
S. Mutalik and N. Udupa, Pharmacological evaluation of membrane-moderated transdermal system of glipizide, Clin. Exp. Pharmacol. Physiol. 33 (2006) 17-26.
C. L. Stevenson, J. T. Jr. Santini and R. Langer, Reservoir-based drug delivery systems utilizing microtechnology, Adv. Drug Deliv. Rev. 64 (2012) 1590–1602; https://doi.org/10.1016/j.addr.2012.02.005.
P. J. Hughes, M. K. Freeman and T. M. Wensel, Appropriate use of transdermal drug delivery sys tems, J. Nurs. Edu. Pract. 3 (2013) 129–138.
S. Cherukuri, U. R. Batchu, K. Mandava, V. Cherukuri, K. R. Ganapuram, Formulation and evalua tion of transdermal drug delivery of topiramate, Int. J. Pharm. Investig. 7 (2017) 10–17; https://doi. org/10.4103/jphi.JPHI_35_16.
Keleb E, Sharma RK, Mosa EB, Aljahwi A-AZ. Transdermal Drug Delivery System – Design and Evaluation. International Journal of Advances in Pharmaceutical Sciences. 2010; 1:201-211.
Rhaghuram RK, Muttalik S, Reddy S. Once – daily sustained- release matrix tablets of nicorandil: formulation and invitro evaluation. AAPS Pharm.SciTech. 2003; 4(4):480–488.
Shaila L, Pandey S, Udupa N. Design and evaluation of matrix type membrane controlled.
Aggarwal G, Dhawan S. Development, Fabrication and Evaluation of Transdermal Drug Delivery System - A Review. Pharmainfo.net. 2009; 7(5).
Keleb E, Sharma RK, Mosa EB, Aljahwi A-AZ. Transdermal Drug Delivery System – Design and Evaluation. International Journal of Advances in Pharmaceutical Sciences. 2010; 1:201-211.
Prajapati ST, Patel CG, Patel CN. Formulation and evaluation of transdermal patch of repaglinide. ISRN Pharm 2011;2011:1-9.
Baichwal MR. Polymer films as drug delivery systems, Advances in drug delivery systems. Bombay, MSR Foundation; 1985; 136-147.
Vyas SP, Khar RK. Targetted and controlled Drug Delivery Novel carrier system. 1st ed. CBS Publishers and distributors New Delhi; 2002; 411- 447.
J. Singh, K. Tripathi and T. Sakya, Effect of penetration enhancers on the in vitro transport of ephedrine through rat skin and human epidermis from matrix based transdermal formulations, Drug Dev. Ind. Pharm. 19 (1993) 1623–1628.
N. Maftoona, H. S. Ramaswamy and M. Marcotte, Evaluation of factors affecting barrier, mechanical and optical properties of pectin-based films using response surface methodology, J. Food. Process Eng. 30 (2007) 539–563; https://doi.org/10.1111/j.1745-4530.2007.00123.x
Singh and A. Bali, Formulation and characterization of transdermal patches for controlled delivery of duloxetine hydrochloride, J. Anal. Sci. Technol. 7 (2016) 25; https://doi.org/10.1186/s40543 016-0105-6
J. Wiechers, Use of chemical penetration enhancers in transdermal drug delivery – possibilities and difficulties, Acta Pharm Nord. 4 (1992) 123.
S. Banerjee, P. Chattopadhyay, A. Ghosh, P. Datta and V. Veer, Aspect of adhesives in transdermal drug delivery systems, Int. J. Adhes. Adhes. 50 (2014) 70–84.
M. Wokovich, S. Prodduturi, W. H. Doub, A. S. Hussain and L. F. Buhse, Transdermal drug delivery system (TDDS) adhesion as a critical safety, efficacy and quality attribute, Eur. J. Pharm. Biopharm. 64 (2006) 1–8.
J. Steven-Fountain, A. G. Atkins, G. Jeronimidis, J. F. V. Vincent, D. F. Farrar and R. A. Chivers, The effect of flexible substrates on pressure-sensitive adhesive performance, Int. J. Adhes. Adhes. 22 (2002) 423–430.
G. Thakur, A. Singh and I. Singh, Formulation and evaluation of transdermal composite films of chitosan-montmorillonite for the delivery of curcumin, Int. J. Pharm. Investig. 6 (2016) 23–31; https://doi.org/10.4103/2230-973X.176468
T. Kamal, M. Sarfraz, M. Arafat, M. Mikov and N Rahman, Cross-linked guar gum and sodium borate based microspheres as colon-targeted anticancer drug delivery systems for 5-fluorouracil, Pak. J. Pharm. Sci. 30 (2017) 2329–2336.
O. A. Hanbali, R. Hamed, M. Arafat, Y. Bakkour, H. Matubsi, R. Mansour, Y. Bataineh, M. Aldhoun, M. Sarfraz and A. K. Yousef Dardas, Formulation and evaluation of diclofenac controlled release matrix tablets made of HPMC and Poloxamer 188 polymer: An assessment on mechanism of drug release, Pak. J. Pharm. Sci. 31 (2018) 345–351.
T. Z. Marques, R. Santos-Oliveira, L. B. de Siqueira, V. S. Cardoso, Z. M. de Freitas, R. C. Barros, A. L. Villa, M. S. Monteiro, E. P. Santos and E. Ricci-Junior, Development and characterization of a nanoemulsion containing propranolol for topical delivery, Int. J. Nanomedicine 13 (2018) 2827–2837; https://doi.org/10.2147/IJN.S164404
S. Cerqueira-Coutinho, V. E. De Campo, A. L. Rossi, V. F. Veiga, C. Holandino, Z. M. Freitas, E. Ricci-Junior, C. R. Mansur, E. P. Santos and R. Santos-Oliveira, Comparing in vivo biodistribution with radiolabeling and Franz cell permeation assay to validate the efficacy of both methodologies in the evaluation of nanoemulsions: a safety approach, Nanotechnology 27 (2016) 015101; https://doi.org/10.1088/0957-4484/27/1/015101
J. Wang, Y. Wei, Y. R. Fei, L. Fang, H. S. Zheng, C. F. Mu, F. Z. Li and Y. S. Zhang, Preparation of mixed monoterpenes edge activated PEGylated transfersomes to improve the in vivo transdermal delivery efficiency of sinomenine hydrochloride, Int. J. Pharm. 533 (2017) 266–274; https://doi.org/10.1016/j.ijpharm.2017.09.059
Abu Hashim, N. F. Abo El-Magd, A. R. El-Sheakh and M. F. Hamed, Pivotal role of Acitretin nanovesicular gel for effective treatment of psoriasis: ex vivo–in vivo evaluation study, Int. J. Nanomedicine 13 (2018) 1059–1079; https://doi.org/10.2147/IJN.S156412
Kanchan Maurya
Corresponding author
Ideal Institute of Pharmacy, Posheri, Wada, Palghar, Maharashtra, India.
Ideal Institute of Pharmacy, Posheri, Wada, Palghar, Maharashtra, India.
Kanchan Maurya, Sonali Uppalwar, Transdermal Nanoparticle Patches: A New Era in Controlled Drug Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 2508-2521. https://doi.org/10.5281/zenodo.17942500




 10.5281/zenodo.17942500
10.5281/zenodo.17942500
