Womens College of Pharmacy, Peth Vadgaon
The Nipah virus (NiV) infects both humans & animals; causes serious neurological and respiratory disorders. Coming from the natural reservoir of fruit bats (Pteropus spp.). It was first identified 20 years ago in Malaysia and has since caused outbreaks in other parts of South and Southeast Asia. It causes severe neurological and respiratory disease which is highly lethal. It is highly infectious and spreads in the community through infected animals or other infected people. Diseased animals, tainted food, or human-to-human transmission are the three ways the virus spreads. With a high fatality rate, NiV infection causes symptoms that range from fever and headache to severe encephalitis and respiratory difficulties.There aren't any licensed vaccines or antiviral medications for the Nipah virus at this time. Since there is currently no specific therapy or vaccination, early discovery, supportive care, and stringent biosecurity measures are the only ways to prevent outbreaks. Nipah virus is still a major worldwide health issue because of its potential to spread like a pandemic. There are currently no effective therapeutics, and supportive care and prevention are the mainstays of management.
In 1998, the Nipah virus (NiV) emerged in Malaysia. Predominantly affecting the Indo-Bangladesh regions.It has caused numerous encephalitis outbreaks with high mortality rates (1). Fruit bats (Genus Pteropus) are widely acknowledged as the natural hosts and reservoirs of NiV (2).This is a study to characterize some of the epidemiological aspects of the disease. In particular, the aims of this study was to determine the relationship of the disease to pig farming, the possible modes of transmission, the Nipah virus infection rate and the rate of asymptomatic infection (3).It leads to severe respiratory and neurological conditions, often resulting in fatalities. The virus is highly contagious and spreads within populations through contact with infected humans or animals (4). The fear of disease like: fever, encephalitis, pulmonary involvement, leukopenia, transaminitis, and/or thrombocytopenia that could have been a sign of bioterrorism (5).The foundation of effective infection prevention and control lies in hygiene, serving as essential components of a comprehensive infection prevention and control strategy (6). However, in order to create treatment alternatives and vaccinations, it is vital to comprehend the pathophysiology and disease dynamics(7).
Epidemiology
After further investigation, it was found that the first Nipah virus outbreak in Malaysia and Singapore (1998–1999) was indeed Nipah virus, rather than Japanese encephalitis (JE) (1-2). Fever, headache, and diminished awareness were reported in many cases in the Malaysian state of Perak in September 1998 (1). A patient from the town of Sungai Nipah tested positive for a new virus (NiV) in their cerebrospinal fluid (CSF) in March 1999 . Males who worked with pigs made up the bulk of the patients, and there weren't many young children. in (4). In 2001, a second, geographically unconnected outbreak of the disease occurred in the Meherpur district of Bangladesh and Siliguri, West Bengal, India (2). The Nipah virus is thought to be stored by Pteropus bats. Close contact with pigs was identified as a substantial risk factor for outbreaks (1), even though the majority of patients in Bangladesh reported contact with pigs. A total of 209 cases of NiV were reported between 2001 and 2012, with 161 (or 77% of the total) resulting in fatalities (4). The worst case of person-to-person transmission occurred in Faridpur in 2004. Patient saliva has tested positive for NiV RNA, suggesting that droplet infection is a factor in the transmission of this virus (1). Nipah virus emerged in the districts of Kozhikode and Malappuram in May 2018 in the southwest coast Indian state of Kerala, which is geographically far from where the virus had previously broken out. Date palm sap isn't often drunk in this area, unlike in other parts of the world. Over 90% of those infected died during this epidemic, and at least 17 people were killed (4). There have been only three outbreaks of NiV in India, thus there isn't enough data to draw any firm conclusions, even if the epidemiological pattern is similar to Bangladesh (2).
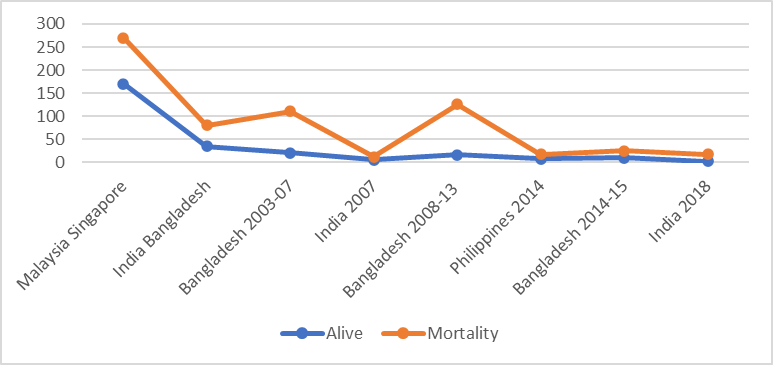
Chart No.01
The Nipah Virus
This newly-discovered virus can infect humans and cause severe respiratory infections and potentially deadly encephalitis (6). Pathogens such as parainfluenza, measles, mumps, Newcastle disease, and Hendra virus (HEV) are also members of this family of viruses (7). The illness can be found in Pteropus bats, which are found all over the world (1). NiV is a paramyxovirus that features an enveloped structure. Its genome is composed of helical nucleocapsids that have a negative stranded orientation, and it is not segmented (8). Although ribavirin was the first antiviral medication to be used to treat NiV, it was only effective in reducing death by 36%. Further, clinical trials have utilised the purine analogue favipiravir (T-705) to treat Ebola and several influenza viruses through the inhibition of RNA-dependent RNA polymerase (9).
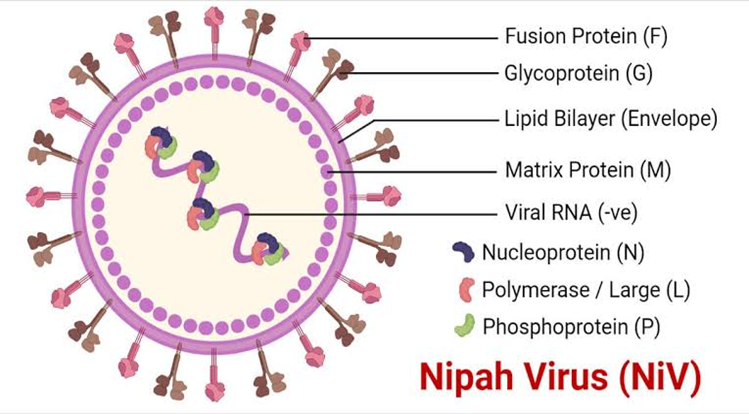
Fig No.01 Structure of Nipah Virus
Pathogenesis
This newly-discovered virus can infect humans and cause severe respiratory infections and potentially deadly encephalitis (6). Pathogens such as parainfluenza, measles, mumps, Newcastle disease, and Hendra virus (HEV) are also members of this family of viruses (7). The illness can be found in Pteropus bats, which are found all over the world (1). NiV is a paramyxovirus that features an enveloped structure. Its genome is composed of helical nucleocapsids that have a negative stranded orientation, and it is not segmented (8). Although ribavirin was the first antiviral medication to be used to treat NiV, it was only effective in reducing death by 36%. Further, clinical trials have utilised the purine analogue favipiravir (T-705) to treat Ebola and several influenza viruses through the inhibition of RNA-dependent RNA polymerase (9).
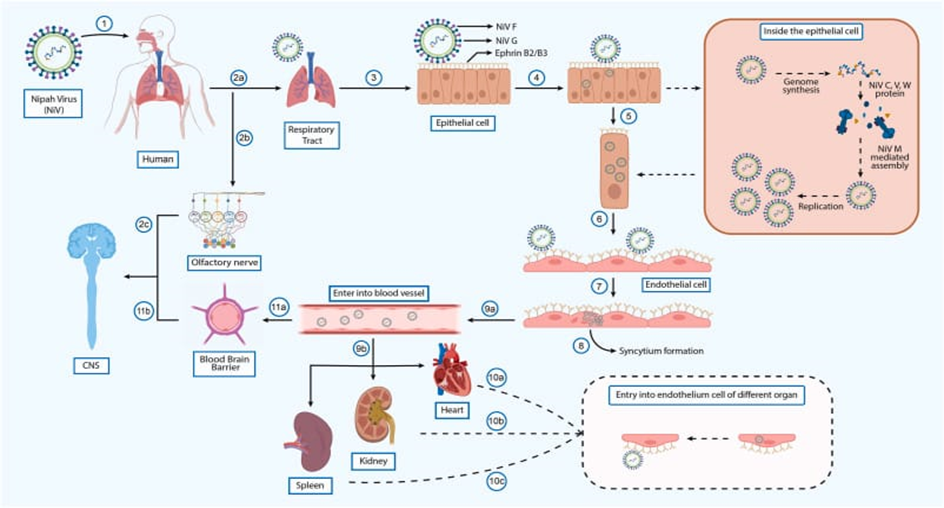
Fig No.02 Pathogenesis of Nipah
Mode of Transmission
One example of a zoonotic virus is the Nipah virus (NiV), which can infect both humans and other animals. Those who came into touch with infected pigs became very sick in the first recorded case of the Nipah virus (12). Researchers tracked the virus's origin back to bats after it infected pigs (6). There are mostly Pteropus fruit bats that spread the Nipah virus. The virus can infect humans if they come into touch with infected pigs or their fluids (12). Raw date palm sap or fruits tainted with bat saliva, urine, faeces, blood, or saliva are examples of foods that can be contaminated with animal fluids and thus pose a significant risk of infection. When someone gets infected, they can transmit the virus to others through their own fluids. Without proper PPE, healthcare personnel and carers providing care to patients also put themselves at danger of infection (6)
Sign and Symptoms
The major site of infection for the Nipah virus (NiV) in humans is the oronasal region, and the incubation period for this virus is 4 to 45 days. The neurological system, cardiovascular system, kidneys, spleen, and lungs are all susceptible to infection with the NiV virus (4). Symptoms of a NiV infection include a high temperature, headache, confusion, and vomiting, which are similar to those of the flu (1). Serious respiratory problems are common among people infected with NiV, in addition to neurological problems. Depending on the severity of the infection, a NiV-M infection can progress to a later stage and cause CNS encephalopathy. Diminutive mental status, changes in cerebellar function, and convulsions are also possible neurological signs (15). Encephalitis, in its most severe forms, can cause lethargy, disorientation, and, within 48 hours, seizures and coma. A few days is all it takes for death to happen (14).
Initial Symptoms (Flu-like)
Encephalitis:
Diagnosis
Patients who exhibit symptoms may provide specimens for viral detection. It is best to gather specimens for serological testing 10–14 days following the commencement of the infection (1).Early detection of NiV infection is essential for both containing an epidemic and enabling appropriate patient care because its symptoms are similar to those of other infectious disorders(14). Samples must be gathered securely and packed in triplicate containers between 2 and 8 °C. It is advised to store at -20°C after 48 hours of collection (5).Strict operational protocols, personal protective equipment, and physical infrastructure are necessary for the safe handling of specimens in both clinical and research operations (1). Healthcare providers can confirm a Nipah virus (NiV) infection using a real-time polymerase chain reaction (RT-PCR) test (14). Immunohistochemistry is performed on tissues obtained from autopsy to detect the virus. Viral RNA can also be identified in an infected person's saliva through extraction and analysis (16).
1. Molecular Biology
Specimens such as tissue samples, swabs, cerebrospinal fluid (CSF), and urine can be used for diagnosing Nipah virus (NiV). However, due to the low sensitivity of virus detection, direct diagnosis in animals can be difficult (1). RT-PCR is capable of detecting NiV RNA in respiratory secretions, urine, or brain fluid (20). It is particularly useful during outbreaks for confirming diagnoses as it specifically identifies NiV RNA (5).
2. Immunohistochemistry
Immunohistochemistry can be conducted on formalin-fixed tissue samples (17). Various organs used for this process since viral replication occurs primarily in the vascular endothelium (1). In pregnant animals, the uterus, placenta, and fetal tissues are also examined. Previously, immunohistochemistry was performed using human convalescent serum. However, rabbit serum against NiV is now commonly used for this purpose (17).
3. Virus Isolation
Within three days, cytotoxic effects can be seen (5).After the cells produce syncytia, the syncytia lift off the surface, causing punctate holes to appear in the monolayer (19-20). PCR or immunohistochemistry can be used to definitively identify the virus from cell culture (1). Electron microscopy and sequencing, which is used to characterize viruses, are other procedures that could be employed. They are not suitable for initial diagnosis, though, and are rarely accessible (9).
4. Antibody detection
Detection of antibodies Serum or CSF containing IgM antibodies is used for diagnosis (20).IgG antibody detection is a useful technique for human surveillance and identification in reservoir animals during epidemiological studies. During outbreaks, it has also been used to diagnose people(5).
5. ELISA
ELISA Because of its high sensitivity, speed, convenience of use, and safety, it is the most widely used test for serological diagnosis(20). Inv ELISAs for IgG and IgM detection were utilized to confirm the diagnosis(18). The highly conserved N antigen has been used to construct further recombinant protein-based testing (6).It has been discovered that 50% of patients have detectable IgM antibodies on the first day of sickness, whereas 100% of patients have IgG positive after day 18. For several months, IgG positive lasts (1).
6. Serum Neutralisation Test
Test of Serum Neutralization This test involves allowing test sera to infect Vero cells after they have been cultured with the virus(21). Test results can be read three days after a positive serum test prevents the onset of cytopathic consequences. Here, the viral-serum mixture is extracted following an adsorption period, and the virus is detected by immunostaining. It is possible to conduct a surrogate neutralization test using pseudotyped viruses(20). A virus that has envelopes and one or more foreign envelope proteins is called a pseudo typed virus. (4, 20).
Management and control
Patients must be segregated, and strict infection control procedures must be followed (1). Nipah virus infection requires supportive treatment, such as mechanical breathing and intensive care, as the major management method (26).
1. Antiviral chemotherapy
Since then, ribavirin has been shown to be ineffective in animal models (6, 23).Although acyclovir was used in Singapore, its effectiveness is unknown Although chloroquine was found to be beneficial in cell culture, neither alone nor in conjunction with ribavirin was able to stop death in a hamster model (1).A hamster model has demonstrated the effectiveness of favipiravir, a medication licensed treatment of influenza (4). As a result, This includes isolating suspected or confirmed cases, using personal protection equipment (PPE), hand hygiene, disinfecting contaminated surfaces, and providing supportive care & also recommended that patients who are discharged stay in isolation (3).Antiviral drugs and vaccines are the subject of ongoing trials (14-16).
2. Surveillance
Regular disease surveillance is conducted in Bangladesh's Nipah belt. Surveillance activities include two main types: sentinel surveillance and event-based surveillance. Monitoring print and electronic media is a key aspect, involving ten national newspapers, eight national news channels, and hotlines for medical professionals to report outbreaks. These methods facilitate the rapid detection of suspected epidemics and deaths from unknown causes (9, 13). Surveillance is an essential component of disease control and should be applied in regions like India and other affected areas (4). During epidemics, active case finding and improved laboratory diagnostic capabilities contribute to the early detection of human cases (15).
3. Vaccine
NiV vaccines have been developed in a variety of ways, some of which have been evaluated in animal models (1, 4).Equivac, manufactured by Zoetis, Inc., is the only vaccine that has received formal approval and registration from the Australian Pesticides and Veterinary Medicines Authority (APVMA)(5).A subunit vaccination based on the G glycoprotein (sG) of HeV and NiV has been the most researched strategy (22-24).It was demonstrated that the developed vaccination was non-toxic and non-allergic (4).Additionally, a vaccine containing virus-like particles grown from mammalian cells has been developed(23).In numerous animal models, these methods have all resulted in complete protection against oro-nasal NiV exposure following a single dosage (5).These two strategies are appealing for potential use in humans due to the efficacy of the sG vaccination in horses and the VSV vectored Ebola vaccine (rVSV-ZEBOV) (22).An essential component of the fight against theepidemic is vaccination. The first vaccine licensed and commercially deployed against a BSL-4 agent (23).These results suggest that these particles have vaccination potential and will serve as the foundation for upcoming protective effectiveness research in NiV illness animal models(24).
Prevention
A significant concern is the morbidity and mortality of medical personnel who care for patients with NiV (2). Although there are uncertainties regarding the transmission and spread of this paramyxovirus, guidelines for healthcare worker protection should be developed based on current evidence and available resources (2, 6). Personal protective equipment (PPE), hand hygiene, isolation, and standard precautions remain essential elements of a comprehensive infection prevention and control strategy (1). Hospitals should adhere to standard infection control protocols for all patient care activities, particularly during procedures that generate aerosols (5). In the case of a confirmed NiV infection, additional precautions including droplet, contact, and airborne measures should be implemented within healthcare settings (13).In order to reduce the danger of exposure, hospitals in high-risk locations should generally be ready to handle Nipah cases through hospital screening, admission processes, and triage. Additionally, visitor access and movement should be managed (1). This international partnership between governments and pharmaceutical companies seeks to create vaccines for diseases like NiV that are safe, efficacious, and accessible(25).,
Future prospect
Extensive research on Nipah virus pathogenesis and transmission has highlighted the need for a vaccine and effective risk reduction strategies. Strengthening surveillance and response networks, especially after outbreaks in Bangladesh and India, is crucial. Improved communication between veterinary and medical services is essential, along with raising awareness, early detection about food and public hygiene to prevent infections(13, 26).
CONCLUSION
Nipah Virus (NiV) first appeared 20 years ago, it had a devastating effect on Malaysia's pig farming sector by causing serious sickness and animal and human deaths. With its bat reservoir host widely dispersed, NiV continues to pose a threat to outbreaks worldwide, with outbreaks continuing in Bangladesh and India(25).Given these difficulties, it is critical to keep funding research and development initiatives to fight NiV while highlighting the significance of preventative public health measures, risk education, and community involvement (26).
REFERENCES








Patil Yogita*, Nandrekar A. N., Palake G. J., Nalavade P. A., Patil S. K., Jadhav V. S., Patil M. S., Dr. Jadge D. R., The Nipah Virus: A Review OF Epidemiology, Pathogenesis and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2438-2445. https://doi.org/10.5281/zenodo.15258014
 10.5281/zenodo.15258014
10.5281/zenodo.15258014
