1Pune District Education Association College of Pharmacy Hadapsar Pune
2Department Of Pharmaceutical Chemistry, Sinhgad Technical Education society,Sinhgad Institute of pharmacy ,Narhe Pune 41
Artificial intelligence (AI) has become a game-changer in healthcare, showing great promise in improving the control of hospital-acquired infections. This review delves into how AI is being used to enhance infection control in healthcare environments. It looks at the latest research on AI-based prediction models, real-time monitoring systems, and decision support tools that help prevent and manage healthcare-associated infections (HAIs). By utilizing machine learning and data analytics, AI has proven effective in forecasting outbreaks, refining antibiotic use, and enhancing the accuracy of infection surveillance. This review aims to give healthcare professionals and researchers a thorough understanding of the advantages, challenges, and future possibilities of using AI in infection control.
Artificial Intelligence
John McCarthy, the father of artificial intelligence who coined the term in 1956, said that "it is the combination of science and engineering to make intelligent devices for human welfare." Artificial intelligence is an intellect that is much smarter than the best human brain in practically every field, including computer science and linguistic logic.[1] It is a modern method of creating machines that can perform muscle work and solve complex questions in an "intellectual" manner. AI is concerned with the fundamental aspects of our lives, including philosophy, computer science, mathematics, linguistics, biology, neuroscience, and sociology. AI plays a very important role in exhibiting intelligent behavior, learning, demonstrating, and providing advice to the user. [2] Artificial General Intelligence (AGI) refers to systems capable of performing intellectual tasks at the level of human intelligence, capable of handling multiple processes simultaneously. AGI encompasses learning, perception, problem-solving, and adapting new solutions. It also involves linguistic logic and reasoning. [1,2]
Artificial intelligence can be categorized into two types:
Weak AI:
Weak AI systems are designed to behave as if they are intelligent. These systems can perform tasks like thinking, talking, and moving if programmed accordingly. For example, in a chess game, a computer can play and make moves automatically. While the computer does not truly think, it is programmed to make optimal moves. [4]
Strong AI:
Strong AI systems possess genuine intelligence and can perform calculations, think independently, and make predictions about the future. An example is IBM's artificial intelligence supercomputer, Watson. In the future, there may be machines or humanoids capable of performing tasks and thinking more powerfully than human beings. [4]
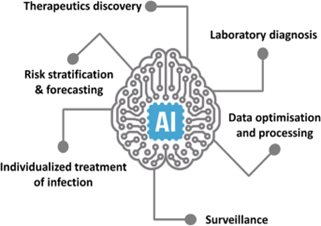
FIG 1
NASOCOMICAL INFECTION
Nosocomial infections, also known as hospital-acquired infections, have a history that goes back to the very beginning of hospitals. [5] The World Health Organization (WHO) describes these infections as those that occur in a patient during their stay in a hospital or other healthcare facilities and were not present at the time of admission. [6]
These infections often become noticeable either during the hospital stay or after the patient has been discharged. The pathogens responsible for these infections are referred to as nosocomial pathogens. In addition, infections that affect hospital staff or visitors can also be classified as nosocomial. [7]When harmful microorganisms are detected in body fluids or areas of the body that are typically sterile, such as the cerebrospinal fluid or blood of patients without symptoms, this can indicate an infection. [8] However, an infection that is present upon admission is not considered nosocomial. It is only labeled as such if there is a change in symptoms or if a new pathogen is detected, suggesting a new infection has been acquired. [9,10] Nejad and colleagues noted that patient care occurs in a variety of facilities, ranging from basic front-line units to advanced university teaching hospitals. [11] These facilities are linked to various nosocomial infections, from mild skin infections to severe, life-threatening conditions. [12] Such infections not only increase healthcare costs but also prolong hospital stays and significantly raise mortality rates. [13] Studies indicate that nosocomial infections are becoming increasingly problematic in the 21st century. This rise is partly due to the increased reliance on outpatient treatments, leaving hospitalized patients generally more severely ill. Hospitals also admit a large number of patients with compromised immune systems. Reports from the WHO and other sources have pointed out that the frequent use of antibiotics in hospitals has led to the emergence of antibiotic-resistant microorganisms. This issue is further aggravated by medical procedures that bypass the body’s natural defenses and by cross-contamination between medical staff and patients. Additionally, inadequate cleaning practices, such as improper washing, sterilization of equipment, and insufficient hygiene measures, contribute to the spread of pathogens in healthcare environments. [15]
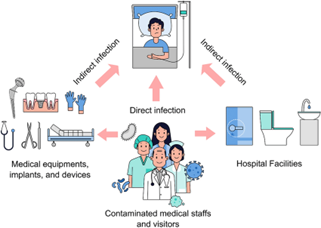
FIG. 2
Transmission of Infections in Healthcare Facilities
Infections are transmitted to individuals in healthcare settings through various routes, including:
Droplet transmission –
Droplet Transmission Droplets larger than five microns in diameter are spread through coughing, sneezing, talking, or during procedures like suctioning or bronchoscopy. [16] Because of their relatively large size, these droplets travel only short distances, usually two meters or less. Common organisms spread via droplet transmission include: [17]
Neisseria meningitidis, which is associated with a severe form of bacterial meningitis
Airborne transmission –
Airborne Transmission Tiny pathogens, smaller than five microns in diameter, are spread through coughing or sneezing. These particles can travel greater distances and remain airborne for longer periods. They are more likely to reach the alveoli, increasing their pathogenic potential. Common organisms spread via airborne transmission include: [18]
Contact Transmission (Direct or Indirect)
Direct contact transmission occurs when microorganisms are transferred from one person to another through direct physical contact. Doctors and nurses are at high risk during their physical examinations of patients. [20]
Indirect contact transmission involves the transfer of microorganisms to objects or surfaces within healthcare facilities, which are then touched by other patients or healthcare workers. Common objects associated with this type of infection include bed linen, furniture, bedpans, urinals, and medical examination equipment like thermometers, blood pressure cuffs, and stethoscopes. [21] In the age of antibiotic-resistant microbes, organisms of particular concern in this form of transmission include:
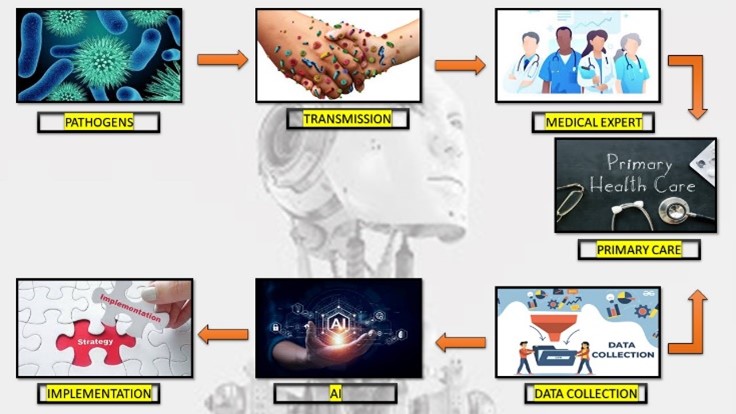
FIG 3
Prevention of Nosocomial Infections
Preventing nosocomial infections requires a multifaceted approach, focusing on hygiene practices, proper use of antibiotics, and effective infection control protocols. Here are some key strategies:
1. Hand Hygiene
Regular Hand Washing: Healthcare workers must wash their hands thoroughly with soap and water or use alcohol-based hand sanitizers before and after patient contact, after touching potentially contaminated surfaces, and before performing medical procedures.
Challenge FG:
WHO Guidelines on Hand Hygiene in Health Care: a Summary. World Health Organization, Geneva, Switzerland 2009. [22]
2. Use of Personal Protective Equipment (PPE)
Appropriate Use of PPE: Gloves, gowns, masks, and eye protection should be worn when there is a risk of exposure to infectious agents. Proper use and disposal of PPE are crucial to prevent the spread of infections. [22]
3. Sterilization and Disinfection
Sterilizing Medical Equipment: Instruments and equipment must be properly sterilized using autoclaves or chemical disinfectants. Single-use items should be disposed of immediately after use. Environmental Cleaning: Regular and thorough cleaning of hospital environments, including patient rooms, operating theaters, and common areas, is essential. This includes disinfection of high-touch surfaces like doorknobs, bed rails, and medical equipment[23]
4. Antibiotic Stewardship
Rational Use of Antibiotics: Antibiotics should be prescribed only when necessary and in the correct dosages to reduce the development of antibiotic-resistant bacteria. Monitoring antibiotic use and resistance patterns helps in guiding appropriate therapy. [24]
5. Isolation of Infected Patients
Isolation Protocols: Patients with contagious infections should be isolated to prevent the spread of pathogens. Negative pressure rooms can be used for airborne infections to contain and filter the air. [25]
6. Education and Training
Staff Training: Continuous education and training programs for healthcare workers on infection prevention and control practices are vital. This includes proper hand hygiene, use of PPE, and updated protocols for managing infections. [25]
7. Monitoring and Surveillance
Infection Control Teams: Establishing dedicated infection control teams to monitor infection rates, investigate outbreaks, and implement control measures. Regular Audits: Conducting regular audits of infection control practices and adherence to protocols to identify areas for improvement. [26]
8. Safe Injection Practices
Use of Sterile Needles and Syringes: Ensuring that needles and syringes are sterile and used only once to prevent the transmission of bloodborne pathogens. Proper Disposal: Safe disposal of sharps in designated containers to prevent needlestick injuries and subsequent infections. [27]
9. Patient Education
Informing Patients: Educating patients about the importance of hygiene, the correct way to use antibiotics, and how to recognize signs of infection. Encouraging patients and visitors to follow hygiene protocols to minimize infection risks. [27]
10. Environmental and Engineering Controls
Air Filtration Systems: Utilizing high-efficiency particulate air (HEPA) filters in areas like operating rooms and isolation units to reduce airborne pathogens. Ventilation: Ensuring proper ventilation systems are in place to reduce the concentration of airborne infectious agents. [28,29]
Role of Artificial Intelligence in Preventing Nosocomial Infections[29]
Role of Artificial Intelligence in Preventing Nosocomial Infections as follows :
Predictive Analytics
Early Detection of Outbreaks: AI uses large amounts of data, such as electronic health records and infection reports, to spot patterns and predict potential outbreaks of hospital-acquired infections. By identifying trends and unusual occurrences, AI helps in taking early action to prevent the spread of infections[29]
Risk Assessment
AI models evaluate individual patient factors, such as their medical history and recent treatments, to estimate their risk of developing nosocomial infections. This allows for focused prevention efforts [30]
Surveillance and Monitoring
Real-Time Monitoring: AI systems can continuously check patient data and hospital environments for signs of infections. These systems alert healthcare workers about possible infections based on real-time analysis of various data sources, like lab results and patient symptoms [31]
Automated Surveillance
AI automates the tracking of infection rates and adherence to infection control practices. This reduces the manual work for healthcare staff and improves the accuracy of monitoring efforts [31,32]
Diagnostic Support
Enhanced Diagnostics:
AI algorithms help in diagnosing infections by analyzing medical images, lab results, and patient data. For instance, AI can review chest X-rays to detect pneumonia or other infections more accurately and quickly [33]
Pathogen Identification: AI systems aid in identifying the pathogens causing infections by analyzing genetic material from samples. This leads to faster and more precise identification of the infectious agents [34]
Antibiotic Stewardship
Optimizing Antibiotic Use:
AI analyzes patient data and infection patterns to suggest the most effective antibiotics. This helps to reduce antibiotic resistance by tailoring antibiotic treatments to individual needs [35]
Resistance Prediction:
AI models predict potential antibiotic resistance by analyzing historical data and current infection trends. This helps in anticipating resistance patterns and adjusting treatment protocols accordingly [36]
Infection Control Practices
Compliance Monitoring:
AI tools monitor and evaluate how well infection control protocols, such as hand hygiene and equipment sterilization, are followed. These systems provide feedback and reminders to healthcare staff to ensure adherence to best practices [37]
Environmental Monitoring:
AI-driven sensors and systems check environmental factors like air quality and surface contamination in healthcare settings. This helps maintain a clean and safe environment by identifying potential contamination sources [38]
Personalized Prevention Strategies
Tailored Interventions:
AI uses patient-specific data, including their medical history and current health status, to create personalized prevention strategies for nosocomial infections. This involves recommending specific precautions and monitoring plans for patients at high risk [36,38]
Data Integration and Management
Integrating Diverse Data Sources
AI integrates and analyzes data from various sources, such as electronic health records, lab results, and environmental sensors. This helps in understanding the factors contributing to nosocomial infections and developing effective prevention strategies [39]
Improving Research Efficiency:
AI speeds up research by automating data analysis, finding relevant studies, and generating insights from large datasets. This accelerates the discovery of new infection control measures and treatments [40]
Patient Engagement and Education
Interactive Tools:
AI-powered apps provide patients with information about preventing and managing infections. These tools offer personalized advice, answer questions, and encourage adherence to infection control practices [41]
Virtual Assistants:
AI-driven virtual assistants support both healthcare workers and patients by providing information, answering queries, and guiding them through infection prevention protocols[39,41]
Early Detection and Diagnosis
AI systems can analyze vast amounts of data from electronic health records (EHRs) to identify patterns and predict the likelihood of infections. By using machine learning algorithms, AI can detect early signs of infections before they become apparent to healthcare providers.
Example:
An AI system might flag a patient with a rising white blood cell count and other symptoms that suggest an infection, prompting early intervention. [42]
Infection Control and Surveillance
AI can enhance infection control by continuously monitoring hospital environments and patient data to identify potential outbreaks. This real-time surveillance allows for immediate response to infection threats, reducing the spread within healthcare facilities.
Example:
AI-powered systems can monitor hand hygiene compliance among healthcare workers by analyzing video footage. [43]
Antimicrobial Stewardship
AI can assist in optimizing the use of antibiotics, ensuring they are used appropriately to prevent the development of antibiotic-resistant bacteria. AI systems can recommend the best antibiotic treatments based on the specific characteristics of the infection and the patient's medical history.
Example:
An AI system can analyze a patient’s infection type and suggest the most effective antibiotic, reducing the likelihood of resistance. [44]
Workflow Optimization
AI can streamline hospital workflows by predicting patient needs and optimizing resource allocation. This can lead to more efficient care delivery and reduced opportunities for infection transmission.
Example: AI can predict when a patient will need specific medical equipment, ensuring it is sanitized and ready for use, thereby reducing infection risks. [45]
Personalized Patient Care
AI can provide personalized care plans by analyzing patient data and predicting individual risks for infections. Tailored care plans can improve patient outcomes and minimize infection risks.
Example:
AI might develop a personalized hygiene protocol for a patient with a weakened immune system, reducing their infection risk. [46]
CONCLUSION
Integrating artificial intelligence into the control of hospital-acquired infections offers many benefits, including better prediction, real-time monitoring, optimized use of antibiotics, and improved surveillance. AI's capability to analyze and interpret large, complex datasets provides a significant advantage in preventing and managing healthcare-associated infections. However, challenges such as concerns about data privacy, the need for standardized protocols, and the integration of AI into current healthcare systems must be addressed. Future research should aim to overcome these obstacles and explore new AI applications to further enhance infection control practices. The promising results highlight AI's potential to transform nosocomial infection control and improve patient outcomes in healthcare settings.
REFERENCE


Ganesh Anil Vitukade, Ashwini A. Bhosale, Monika N. Pawar, Nishigandha S. Chopde , The Impact Of Artificial Intelligence On Nosocomial Infection Control: A Comprehensive Review, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 10, 1772-1781. https://doi.org/10.5281/zenodo.14013842
 10.5281/zenodo.14013842
10.5281/zenodo.14013842
