1 Department of Pharmacology, Late Laxmibai Phadtare College of Pharmacy, Kalamb, Pune
2 Faculty of Medical Science and Research, Sai Nath University, Ranchi, Jharkhand-835219, India.
3 Department of Pharmacy, Regional Institute of Pharmaceutical Science and Technology, Agartala, Tripura, India
4 Department of Radiology, Mahatma Gandhi Medical College, Jaipur, India.
5 Department of Pharmacy, Channabasweshwar Pharmacy College, Latur, Maharashtra-413512, India.
6 Department of Regulatory Affairs, TI Medical Private Limited, Khasra No. 1051/1&2, Twin Industrial Estate, Selaqui, Dehradun, Uttarakhand-248197, India.
The problem of diabetic wounds is a large and increasing health burden in the world, which is associated with poor healing caused by persistent inflammation, oxidative stress and infection vulnerability. Independent therapeutic properties that are applicable to wound healing have also been found in Berberine, a natural alkaloid and chalcones, a flavonoid family of compounds. Berberine is the antioxidant, anti-inflammatory and antimicrobial agent, and recent studies have shown that it prevents ferroptosis in diabetic keratinocytes via NRF2 activation. Chalcones enhance endothelial wound healing by stimulating the production of nitric oxide and heme oxygenase-1 besides having anti-diabetic and anti-inflammatory effects. This review examines the scientific basis of the synergistic effect of herbal methodology involving berberine and chalcones in the treatment of diabetic wounds. Complementary actions of these compounds, such as protection of keratinocytes, endothelial activity, inflammation, oxidative stress, and infection, indicate possible superior therapeutic outcomes of combination treatment. We review the existing evidence regarding the preclinical studies, and explain the idea of mechanistic convergence, and the suggestions to conduct the future research to authenticate this synergistic strategy.
The occurrence rate of diabetes in the world keeps increasing alarmedly, with a growth trend that is projected to reach 1.31 billion affected persons by 2050 and this is among the major issues of public health that the twenty first century is grappling with. Diabetic foot ulcers are among the most debilitating diabetes complications, with the number of patients with this condition reaching 18.6 million each year all over the world, and causing enormous physical, emotional and financial disabilities to both patients and the healthcare systems [1]. Pathophysiology of diabetic wounds is also multifactorial and complex, which entails continuous hyperglycemia leading to the formation and accumulation of advanced glycation end-products (AGEs) in the extracellular matrix of the skin, impaired angiogenesis that causes blood supply to healing tissues, dysfunctional immune responses that do not clear pathogens and eliminate inflammation, and increased oxidative stress that damages tissue-forming components and creates an unfavorable environment in which the wound is repairing. All these interdependent pathophysiological processes disrupt every stage of normal wound healing, including hemostasis and inflammation, through proliferation and remodelling to cause chronic non-healing wounds that are prone to infection and portals to systemic complications [2]. The traditional methods of treatment, such as standard wound care, debridement, infection management, revascularization surgery, and advanced dressing, are not always effective in ensuring a fast and full healing process, which leads to a gaping and unrelenting necessity of novel and creative treatment measures that may contribute to the multifactorial nature of diabetic wound pathology. The growing interest in herbal medicines has been on their multi-targeted action and the good safety profile they have compared to single-target pharmaceutical interventions in the complex disease states. One of these natural products, the isoquinoline alkaloid berberine of (Coptis chinensis, Berberis aristata), which has long been used in classical Chinese and Ayurvedic medicine due to its variety of pharmacological effects and recent mechanistic understanding, has proven especially promising as a diabetic wound manager [3]. Correspondingly, chalcones, the precursors of flavonoids that are highly abundant in plants such as Angelica keiskei (also known as ashitaba) and are found in many edible and medicinal organisms, also have a wide range of pharmacological effects, such as anti-inflammatory, antioxidant, anti-diabetic, and anti-microbial effects that have direct application in wound healing. This review discusses the scientific rationale of combining berberine and chalcones in a synergistic herbal intervention in diabetic wound healing based on mechanistic knowledge of the current preclinical studies that have supported the existence of complementary and even cooperative pathways by which these compounds may stimulate tissue repair in the diabetic microclimate [4].
Recently, the discoveries of the radioactive findings demonstrated that the presence of berberine can prevent the ferroptosis of diabetic keratinocytes under the influence of AGEs by stimulating nuclear factor E2-related factor 2 (NRF2), which is an innovative process with profound clinical potential in wound healing. Ferroptosis is a controlled form of non-apoptotic cell death, involving iron-dependent lipid peroxidation, which has been recognized as a major pathogenesis of impaired wound healing in diabetes, and has been shown to be accompanied by reduced expression of glutathione peroxidase 4 (GPX4) and ferritin light chain (FTL) which are key regulators of ferroptosis in the epidermis of diabetic mice and increased lipid peroxidation [5]. Berberine pretreatment maintained the cell viability and decreased malondialdehyde production, iron accumulation and reactive oxygen species in the cell interior, and increased the expression of GPX4 and FTL in human HaCaT keratinocytes exposed to AGEs. These antioxidative effects were eliminated when NRF2 was knocked off, which indicates the core nature of this transcription factor in the cytoprotective activity of berberine. These findings were supported by in vivo studies which revealed that lipid peroxidation accumulation in skin tissue and the restoration of GPX4, FTL, ferritin heavy chain, and NRF2 levels that were reduced in diabetic controls were all rescued by five weeks of oral administration of berberine at 100 mg/kg/day in diabetic mice with the db/db mice. The work makes berberine an anti-ferroptic agent in the diabetic skin setting, a phenomenon that has not been previously identified and puts the compound in the position to protect the population of keratinocytes needed to facilitate the appropriate wound re-epithelialization and wound closure [6].
In addition to its cytoprotective properties against the keratinocytes, berberine has antimicrobial activity, which is of high interest to infected diabetic wounds, and recent reviews have emphasized berberine nanoparticles as a viable intervention that takes advantage of the anti-inflammatory, antioxidant, and context-dependent angiogenic properties of the compound [7]. Nano-drug delivery systems containing berberine and epigallocatechin gallate coated with manganese dioxide nanoshells and glucose oxidase have been designed that utilize endogenous glucose at diabetic wound sites to induce cascade reactions to generate oxygen and improve the photodynamic antibacterial effect of berberine against multidrug-resistant bacteria. Berberine can also regulate the response of inflammatory reaction in numerous signaling pathways such as AKT, AMPK, and glucose transporter regulation, which deals with the chronic inflammatory process that non-healing diabetic wounds have to endure. These anti-inflammatory properties are added to its antioxidant and antimicrobial ones, forming a complex therapeutic profile targeting a variety of pathological processes at the same time [8].
The occurrence rate of diabetes in the world keeps increasing alarmedly, with a growth trend that is projected to reach 1.31 billion affected persons by 2050 and this is among the major issues of public health that the twenty first century is grappling with. Diabetic foot ulcers are among the most debilitating diabetes complications, with the number of patients with this condition reaching 18.6 million each year all over the world, and causing enormous physical, emotional and financial disabilities to both patients and the healthcare systems [9]. Pathophysiology of diabetic wounds is also multifactorial and complex, which entails continuous hyperglycemia leading to the formation and accumulation of advanced glycation end-products (AGEs) in the extracellular matrix of the skin, impaired angiogenesis that causes blood supply to healing tissues, dysfunctional immune responses that do not clear pathogens and eliminate inflammation, and increased oxidative stress that damages tissue-forming components and creates an unfavorable environment in which the wound is repairing. All these interdependent pathophysiological processes disrupt every stage of normal wound healing, including hemostasis and inflammation, through proliferation and remodelling to cause chronic non-healing wounds that are prone to infection and portals to systemic complications. The traditional methods of treatment, such as standard wound care, debridement, infection management, revascularization surgery, and advanced dressing, are not always effective in ensuring a fast and full healing process, which leads to a gaping and unrelenting necessity of novel and creative treatment measures that may contribute to the multifactorial nature of diabetic wound pathology [10]. The growing interest in herbal medicines has been on their multi-targeted action and the good safety profile they have compared to single-target pharmaceutical interventions in the complex disease states. One of these natural products, the isoquinoline alkaloid berberine of (Coptis chinensis, Berberis aristata), which has long been used in classical Chinese and Ayurvedic medicine due to its variety of pharmacological effects and recent mechanistic understanding, has proven especially promising as a diabetic wound manager. Correspondingly, chalcones, the precursors of flavonoids that are highly abundant in plants such as Angelica keiskei (also known as ashitaba) and are found in many edible and medicinal organisms, also have a wide range of pharmacological effects, such as anti-inflammatory, antioxidant, anti-diabetic, and anti-microbial effects that have direct application in wound healing. This review discusses the scientific rationale of combining berberine and chalcones in a synergistic herbal intervention in diabetic wound healing based on mechanistic knowledge of the current preclinical studies that have supported the existence of complementary and even cooperative pathways by which these compounds may stimulate tissue repair in the diabetic microclimate [11-13].
A large group of bioactive flavonoids, which have demonstrated wound healing properties, is represented by chalcones, which have an 1,3-diphenyl-2-propen-1-one structure with an a,b-unsaturated carbonyl system that is the reactive centre to their biological activities. Studies investigating the implications of two chalcones namely 4-hydroxyderricin and xanthoangelol, which were derived out of the edible plant Angelica keiskei, on endothelial wound healing showed that both chalcones had significant effect in enhancing wound healing in cultured porcine vascular endothelial cells, which were injured [14]. It was also shown through mechanistic studies that these chalcones triggered the production of nitric oxide and an elevation of heme oxygenase-1, and led to an improved phosphorylation of endothelial nitric oxide synthase. The pretreatment of the nitric oxide synthase inhibitor L-NMMA and the heme oxygenase-1 inhibitor ZnPPIX inhibited the wound healing promotion, which proved the presence of these pathways. In addition, hemoglobin, which is a carbon monoxide absorbent, inhibited chalcone-dependent wound healing whereas a carbon monoxide-releasing molecule promoted the healing process, indicating that carbon monoxide generated via heme oxygenase-1 activity is involved in the activation of endothelial nitric oxide synthase. These results put chalcones as promoters of re-endothelialization, which is a key process to angiogenesis and wound vascularization, which is frequently impaired in diabetic patients because of endothelial dysfunction and the inability to generate nitric oxide bioavailability [15-17].
Notable metabolic disruptions, including hyperglycemia and dyslipidemia are major contributors of acute and chronic inflammatory reactions especially in metabolic diseases like diabetes, and cardiovascular disease. Continued hyperglycemia positively favors the development of advanced glycation end products that react with their receptor on endothelial cells, macrophages, and other immune cells. Such an interaction produces intracellular signaling that: (i) results in the increased transcription of pro-inflammatory cytokines including tumor necrosis factor-a, interleukin-6, and interleukin-1b; (ii) in nuclear factor kappa B activation. Meanwhile, hyperglycemia increases the oxidative stress by overproduction of reactive oxygen species in the mitochondria, which increases further the inflammatory signal and endothelial dysfunction. Dyslipidemia, which is the increase of the level of low-density lipoprotein, triglycerides, and the decrease of the level of the high-density lipoprotein is also involved in the process of inflammatory activity. Macrophages absorb the oxidized LDL using scavenger receptors and this encourages the formation of foam cells and the liberation of inflammatory mediators in the vascular tissues. This causes the activation of the toll-like receptors and inflammasome complexes like NLRP3, which exert additional stimulatory effects on cytokine synthesis and the recruitment of immune cells. Further, lipotoxicity, mitochondrial dysfunction, and stress-related pathways such as c-Jun N-terminal kinase and protein kinase C are induced by abnormal lipid accumulation in metabolic tissues liver, adipose tissue and vascular endothelium. These pathways scramble the insulin signaling and also make the inflammatory responses worse. Oxidative stress that hyperglycemia induces and lipid toxicity that dyslipidemia causes coexist to form a chronic low-grade inflammatory condition commonly known as metabolic inflammation or metaflammation. This ongoing inflammatory condition helps to promote endothelial injury, atherosclerotic plaque formation and further cardiovascular complication progression, which is often seen in metabolic diseases. Consequently, a detailed elucidation of the interactive molecular mechanisms between hyperglycemia and dyslipidemia and inflammatory signaling can be advantageous in devising treatment plans that can be used to mitigate the effects of inflammation to avert the metabolic and cardiovascular problems Fig.1.
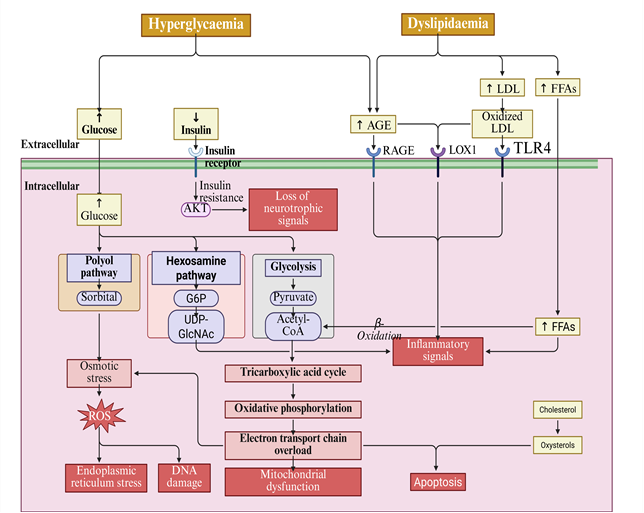
Fig.1: Pathways linking Hyperglycemia and Dyslipidemia to inflammatory responses
These extended pharmacological properties of chalcones are not limited to endothelial protection and extensive reviews have listed extensive preclinical and clinical data on the use of these compounds as antidiabetic, anticancer, antimicrobial, antioxidant, and neuroprotective agents by regulating the effects of various signaling molecules and cascades. They have been studied especially regarding their anti-inflammatory properties, including inhibition of nuclear factor-kappa B and p38 mitogen-activated protein kinase pathways, inhibition of cyclooxygenase-2 and microsomal prostaglandin E synthase-1 [18]. Clinical trials have demonstrated the use of chalcones in chronic venous insufficiency, skin disorders and cancer whereby the safety and efficacy was generally good and the bioavailability was decent. The a,b-unsaturated carbonyl system which is highly reactive and is found in chalcones is termed as the key structure of chalcones which induce their pharmacological activity, allowing them to interact with a variety of cellular targets. Chalcones are also shown to have direct antioxidant action through free radical scavenging and indirect action via increase in endogenous antioxidant defenses with heme oxygenase-1 induction being a cytoprotective mechanism that produces biliverdin and bilirubin as antioxidants and carbon monoxide as a vasoactive and anti-apoptotic molecule. This reduction of oxidative stress is specifically applicable to diabetic wounds, where oxidative stress is the main cause of tissue destruction and hampered repair by a variety of pathways such as lipid peroxidation, protein oxidation, and DNA damage [19].
The treatment with a combination of berberine and chalcones has theoretical benefits due to the complementary and possibly synergistic effects on various factors of diabetic wound pathology. The use of Berberine as a ferroptosis inhibitor will counter the process of keratinocyte death that undermine re-epithelialization of diabetic wounds and conserve the population of cells that will resurface the wound bed. At the same time, chalcones can facilitate the endothelial repair and angiogenesis to maintain sufficient vascular supply to provide oxygen, nutrients, and immune cells to the healing tissue [20]. Both compounds counter oxidative stress by inducing different but complementary mechanisms, with berberine majorly acting via NRF2 activation resulting in the upregulation of several antioxidant enzymes, including GPX4 and ferritin, and chalcones by causing heme oxygenase-1 induction and direct radical activity-reduction, forming a multidimensional antioxidant defense that is possibly more effective than either strategy alone. The overlap of the active site of a berberine and chalcone on separate yet adjacent signaling pathways is one that suggests an additive or synergistic effect, and combined treatment may produce a greater response in the expression of antioxidant enzymes than either agent alone. The two compounds are able to engage cytoprotective enzymes using different transcription factors: berberine activates NRF2, and chalcones activate heme oxygenase-1 (an NRF2 target gene), via mechanisms that may also involve other regulatory factors, suggesting possible cooperative supplementation effects of the antioxidant response of the cell. Additional evidence supporting combination therapy is the antimicrobial properties of the two compounds, especially since diabetic wounds are highly susceptible to infection with biofilms with multidrug-resistant microorganisms having a tendency to complicate their treatment. The ability of Berberine to interact with photodynamic methods and the broad-spectrum antimicrobial properties of chalcones would provide better results in terms of infection control due to various mechanisms of action that are likely to decrease the chance of resistance formation [21-23].
The failure of diabetic wound healing is caused by a combination of several pathological processes at once, which implies that one-agent interventions will hardly be associated with the best results. The berberine and chalcones combination meets this challenge by all three targeting of keratinocyte survival by blocking ferroptosis, endothelial functionality and angiogenesis via nitric oxide and heme oxygenase-1, oxidative stress by complementary antioxidant activities, inflammation by regulating NF-kB and other inflammatory activation cascades and infection by direct antimicrobial effects [24]. This complex poly-target approach is consistent with the postulates of herbal medicine, in which complex combinations usually yield therapeutic effects not achievable with isolated compounds, and with the current pharmacological insights that such combination therapies against multiple disease mechanisms tend to have better effects on complex chronic diseases. Although no actual evidence of the berberine-chalcone combinations in diabetic wound healing is yet to be produced, the mechanistic explanation is convincing and is backed by a wealth of preclinical data of each of the individual compounds. The future studies should focus on preclinical combination studies in the right in vitro and in vivo models, formulation development in order to get the best out of both compounds delivery to the wound tissues, and finally the studies can be translated to the clinical level using specially designed studies to find out whether this synergistic approach of using herbs can be effective in helping to cure the increasing number of patients with diabetic wounds. The good safety profiles of both compounds, their historical as well as traditional medicine use, and the acute need to find safer, more accessible and effective treatments to one of the most debilitating complications of diabetes give a solid motivation to move forward with this line of research that has the potential to bring safer, more accessible and effective treatments that may be used in the treatment of diabetic wounds [25].
Diabetic wound pathophysiology: multiple targets for therapeutic intervention
The pathological condition of diabetic wound healing is disrupted at various levels of the normal wound healing and is a multifactorial and complex condition that has been resistant to standard therapeutic methods of treatment. Normal wound healing cascade, followed by the overlapping phases of hemostasis, inflammation, proliferation and remodeling necessitates a close interplay between a large number of cell types, signaling molecules, and extracellular matrix components to be successfully accomplished in restoring tissue integrity. This is a beautiful and tightly controlled mechanism that is derailed in the diabetic patient at every single step leading to chronic wound that do not heal and cause immense suffering and is a significant healthcare burden in the world [26]. The complex pathophysiology of diabetic wounds requires knowledge of its underlying mechanisms in order to devise effective therapeutic approaches, and the recent growth in the field of molecular biology has provided insights into previously unknown processes that drive healing failure such as the recently described role of ferroptosis in diabetic keratinocyte death. The causative metabolic abnormality in diabetes mellitus is chronic hyperglycemia, which triggers the development and deposition of non-enzymatic products of the additional of reducing sugars to proteins, lipids, or even nucleic acids. Such AGEs accumulate gradually in diabetic tissues and have cytotoxic effects using a variety of mechanisms, including direct modification of extracellular matrix proteins to alter their structure and activity, binding the receptor of AGEs (RAGE) on cell surfaces which triggers pro-inflammatory signaling pathways and generating reactive oxygen species which induces oxidative stress [27]. All three cell types essential to normal wound re-epithelialization and wound re-closure, i.e. keratinocytes, fibroblasts and endothelial cells, are cytotoxically impacted by AGEs; necessary to up-regulate wound re-epithelialization and wound re-closure by means of proliferation and migration of keratinocytes across the wound bed to convert the wound into a new tissue; production and remodelling of the extracellular matrix by fibroblasts and contractile forces required to draw the wound edges back together respectively This cumulative impact of AGE-mediated cytotoxicity in these cellular populations is a significant wound healing impairment that is then reflected in clinical terms by sluggish or absent wound healing [28].
Recent findings have revealed that ferroptosis, a controlled non-apoptotic cell death, which involves iron-dependent lipid peroxidation, is a major and underestimated contributor to impaired wound healing in diabetes. The initial definition of ferroptosis was 2012 as a unique cell death modality, which is different, and morphologically, biochemically, and genetically different than apoptosis, necrosis and autophagy. The distinctive characteristics of ferroptosis are the presence of lipid peroxidation products, especially in polyunsaturated fatty acids in cellular membranes, free iron necessity leading to Fenton chemistry where overly reactive hydroxyl radicals are formed, and the loss of ferroperoxidase 4 (GPX4), which is the most important enzyme in the reducing and detoxifying of lipid hydroperoxides in cellular membranes [29]. The high concentration of glucose in diabetic skin ensures the encouragement of iron overload in various ways, such as increased iron uptake, altered iron transportation protein expression, and the release of iron in the damaged cells that, combined, provide conditions conducive to Fenton chemistry. The Fenton reaction whereby ferrous iron (Fe2+) combines with hydrogen peroxide to form highly reactive hydroxyl radicals, produces too much reactive oxygen species that trigger and amplify lipid peroxidation chain reactions in the cellular membranes. These reactions overwhelm the cellular antioxidant defense mechanisms that control oxidative harm when oxidative damage causes cell death, resulting in membrane damage and ferroptotic cell death. It has been shown that glutathione peroxidase 4 (GPX4) and ferritin light chain (FTL) as major ferroptosis regulators are the ones reduced in the epidermis of diabetic mice, with lipid peroxidation increased as measured by malondialdehyde and 4-hydroxynonenal [30]. The role of GPX4 in ferroptosis prevention cannot be overestimated since this is the sole enzyme that can decrease complex lipid hydroperoxides, embedded into biological membranes, and use glutathione as a cofactor. In the case of a decrease in the activity of the GPX4 enzyme (by decreasing its expression or depleting glutathione), the lipid peroxides remain unchecked, and ultimately lead to a break in membrane integrity, causing cell death. Along with ferritin heavy chain, ferritin light chain constitutes the ferritin complex that removes the intracellular iron in an inactive, harmless form and lower levels of FTL expression signify a failure of iron storage capacity, which permits additional free iron to engage in Fenton chemistry. This interaction of greater iron supply and reduced protective steps gives a perfect storm of ferroptosis in diabetic keratinocytes which directly impairs the population of these cells that is required to re-epithelialize the wound. The clinical findings that diabetic wounds tend to have bad epithelialization despite other components of the healing process seem to be developing, and the proposal that keratinocytes might be guarded against this type of cell death would imply a new treatment approach [31].
Endothelial dysfunction is another barrier to diabetic wound healing that exists together with keratinocyte impairment to inhibit timely tissue repair. The vascular endothelium- the inner lining of all blood vessels- is beautifully sensitive to the metabolic abnormalities of diabetes, and dysfunction of endothelium is one of the first and most common complications of diabetes. Endothelial cells are required to undergo angiogenesis to proliferate, migrate, and form new capillary networks in the context of wound healing, whereby the growing endothelial cells fill the wound defect with vascularized connective tissue, the granulation tissue. The angiogenic response in diabetes is grossly impaired by the interplay of various mechanisms [32]. The principal characteristic of diabetic endothelial dysfunction is impaired bioavailability of nitric oxide (NO), caused by a decrease in endothelial nitric oxide synthase (eNOS) expression and activity, an increase in the generation of reactive oxygen species capable of scavenging nitric oxide to form harmful peroxynitrite, and uncoupling of eNOS to cause production of superoxide instead of nitric oxide. Nitric oxide plays a crucial role in wound angiogenesis in numerous ways, such as vasodilation that enhances the blood flow to the wound tissue, direct induction of endothelial cell growth and motility, and endothelial cell survival by suppressing cell apoptosis. In case of loss of NO bioavailability, such angiogenic signals are lost and new vascular growth is no longer able to match the requirements of growing tissue. The angiogenesis that is diminished and the endothelial cell migration that is impaired inhibit sufficient angiogenic tissue formation and wound vascularization leading to a hypoxic wound condition that subsequently impairs cellular metabolism and function [33]. The resulting granulation tissue in diabetic wounds is frequently poorly vascularized and structurally imbalanced, and collagen deposition is not orderly and the mechanical strength is limited to promote wound breakdown and reoccurrence. More than that, endothelial dysfunction is not only angiogenic but also involves the microcirculation of the diabetic foot, decreasing baseline perfusion and restricting the hyperemic response to injury that increases blood flow to injured tissues. This impaired angiogenesis and decreased perfusion result in a chronic hypoxic wound condition incapable of supplying the high metabolic rates of healing tissue, which is one of the reasons as to why non-healing ulcers persist [34].
Wound infection susceptibility among diabetic wounds is another and more often devastating complication that complicates the whole situation and postpones the healing process. The healthy skin barrier is effective against microbial invasion by several factors such as the physical barrier of keratinocytes stratum corneum, the production of antimicrobial peptides by the keratinocytes and the activity of the resident immune cells. A myriad of failures in host defense in a diabetic patient that result in the violation of this barrier will come together to produce a highly permissive environment to microbial colonization and invasion. Neutrophil malfunctioning in diabetes encompasses a diminished chemotaxis that postpones recruitment to infection site, low phagocytic actions that cannot eliminate invading organisms and low oxidative burst ability that restricts intracellular murder. Macrophage dysfunction also inhibits the early inflammatory reaction to infection and the ensuing shift to the proliferative stage of wound healing which involves macrophage-mediated debridement and growth factor release. Hypoxia, oxidative stress, high-nutrient exudate that characterizes the diabetic wound environment itself contribute to an appropriate environment to facilitate microbial growth as the compromised host response is not able to contain proliferation [35]. The formation of biofilm is one of the most problematic issues of diabetic wound infection because the bacteria that are incorporated into the extracellular polymeric substance become extremely resistant to host defense and antimicrobial treatment. These biofilms can also include several bacterial species such as Staphylococcus aureus, Pseudomonas aeruginosa and beta-hemolytic streptococci that can create chronic infection and continue to perpetuate inflammation and prevent healing. The development of diabetic wounds into multidrug-resistant organisms has also complicated the process of managing wounds because infection that could have been treated using conventional antibiotics is now requiring last-line agents, which are more toxic and less effective. Methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamase-producing Enterobacteriaceae, and multidrug-resistant Pseudomonas aeruginosa are increasingly met in the treatment of diabetic foot, thereby restricting treatment choices and risking treatment failure, osteomyelitis, and amputation. The infection in a diabetic wound causes a vicious cycle whereby the non-healing wound becomes a chronic entry point of microbial invasion, the metabolic stress of infection worsens hyperglycemia, which further reduces the immune functioning. To halt this cycle, there is a need to have proper antimicrobial practices, which are capable of bypassing biofilms, eliminating resistant organisms, and providing the environment in which healing can occur and further selection toward resistance is prevented [36].
Due to the multidimensional and intertwined nature of pathological mechanisms that disrupt healing of the diabetic wounds, the therapeutic interventions should be based on modifying a wide variety of mechanisms, instead of specifically focusing on a single pathway. Wound resurfacing requires the presence of viable and functional epithelial population, which can only be achieved by protecting the keratinocytes against cell death. Recent findings of ferroptosis as a cell death pathway of keratinocytes in diabetes have provided therapeutic opportunities since pharmacological inhibition of this particular cell death program may maintain the epithelial ability to close wounds. This protective effect should not only be in the form of a simple inhibition of cell death but also in the form of promoting the proliferation and movement of keratinocytes, since the surviving cells still have to perform the complex tasks involved in re-epithelialization [37]. Rehabilitation of endothelial activity is a second important therapeutic objective, because proper vascularization is a precondition of the oxygen and nutrient supply to the healing tissue, and waste products removal. The defined tactics to improve the bioavailability of nitric oxide, induce endothelial cell survival and migration, and facilitate angiogenesis are likely to reverse the vascular deficit symptomatic of diabetic wounds and allow the development of appropriate granulation tissue. Modifications of oxidative stress and inflammation target the unfriendly wound environment, which harms cells and becomes dysfunctional, and should be done with due caution to the multifaceted roles of the reactive oxygen species and the inflammatory mediators in wound healing [38]. Though it is apparent that too much oxidative stress and chronic inflammation are harmful to the human body, the complete absence of these signals is also harmful, since a balanced oxidative burst and tightly regulated inflammation is crucial to normal healing. Therapeutic measures should then be focused on balancing these processes but not completely doing away with these processes. The fourth therapeutic focus is microbial burden control using effective antimicrobial measures because chronic infection results in inflammatory response, which depletes resources used to treat wounds and can cause the extension of microorganisms to other parts of the body with fatal outcomes [39]. The strategies that should be adopted to tackle biofilm-resistant organisms and multidrug-resistant pathogen must also address the problem of biofilm-embedded organisms and multidrug-resistant pathogens without further encouraging resistance selection, as well as without causing excessive toxicity to healing tissues. It would be ideal to have all four of these therapeutic targets being treated simultaneously by mechanisms that are complementary and may be synergistic so that the effects that such a combination would achieve could not be achieved by any single-target interventions. This concept of the multifactorial pathophysiology of diabetic wound healing is the basis behind the rationale of combinations of strategies that can stimulate many processes at once, and the reason why single-agent wound care strategies have not succeeded in attaining sufficient healing rates in such a demanding condition [40].
The understanding that diabetic wound healing failure is caused by multicurrent pathological processes has far reaching consequences on the design of therapy implying that optimum results will be achieved through interventions that will be able to treat the entire complexity of the disorder. The use of single-agent methods (pharmaceutical agents that inhibit certain molecular pathways or advanced dressings that mitigate the unique wound state) as a monotherapy of diabetic wounds, has resulted in disappointing clinical-trial outcomes [41]. This is expected by the fact that the pathology is multifactorial in nature since only a combination of intervention can achieve simultaneous repair of the dysfunction of keratinocytes, endothelial dysfunction, oxidative stress, inflammation, and infection. The combination methods, which involve the combination of several therapeutic mechanisms, are more promising but they should be developed with specific consideration to the interactions between components and the needs of the diabetic wound environment [42]. The optimal mix would comprise of agents that prevent ferroptosis of the keratinocytes and preserve their proliferative and migratory capabilities, enhance endothelial healing and angiogenesis, decrease oxidative stress and inflammatory states to levels that favor healing, and provide beneficial antimicrobial efficacy with respect to pertinent pathogens such as biofilm-hosting and multidrug-resistant organisms. The agents are expected to possess complementary mechanisms of action that can lead to additive or synergistic effect on combining them, have good safety profiles that are not toxic to prolonged use and also should be compatible with one another as well as with standard wound care procedures such as debridement, offloading, or infection control. In this regard, natural products and herbal medicines have certain benefits, since they often contain more than one pharmacological activity in wound healing, and have a long history of safety when used in traditional medical practice [43]. The discovery of complementing natural compounds with specific mechanisms that can overcome the entire wound pathology of diabetics is a promising approach towards finding more effective treatment options. Berberine and chalcones following their proven impact on keratinocyte protection, endothelial functionality, oxidative stress, inflammation, and infection become especially appealing targets of such a combination strategy, and synergistic improvement of wound healing via various complementary mechanisms can be an option. The large preclinical data base on the individual effect of these compounds gives a good basis to study their combined activities, whereas their historical application in traditional medicine and overall good safety profiles gives credence to the possibility of clinical development[44]. Further investigation aimed at maximizing the berberine-chalcone combinations, their mechanism of action, and determining their effectiveness in the right preclinical and clinical models would undergo a major breakthrough in the management of diabetic wounds and quality-of-life in the millions of diabetic patients who experience this crippling complication. The intersection of contemporary mechanistic conceptualization of diabetic wound pathology with ancient knowledge of medicinal plants provides a possible avenue of more effective treatments that will take into account the full complexity of this complicated disease.
Berberine: mechanisms in diabetic wound healing
Anti-hyperglycemic effects of berberine are not new, and they reflect one of the most pivotal studied natural compounds in managing diabetes under a variety of complementary mechanisms that encompass improved glucose uptake and utilization along with inhibited hepatic glucose production. This known role in the regulation of glucose in the body made berberine a possible adjunctive agent in the treatment of diabetes, and many clinical trials have shown berberine to produce significant improvements in the level of fasting blood glucose, hemoglobin A1c and insulin resistance on par with certain pharmaceutical compounds. Nevertheless, more recent studies have discovered new mechanisms in wound healing that go way beyond glucose regulation to demonstrate that berberine has direct cytoprotective action on skin cells which may render it especially useful in the treatment of diabetic complications. The identification of local cell dysfunction in diabetic wound healing regardless of the overall glucose metabolism has prompted the selection of agents capable of shielding the cells in the wound bed against the harmful influence of advanced glycation end-products, oxidative stress, and other insults of diabetes has drawn interest to the possibilities of the berberine through its newly defined anti-ferroptotic action [45].
In an innovative article, Jiang et al. (2024) established that berberinedefends AGEs-induced ferroptosis in diabetic keratinocytes by activating nuclear factor E2-related factor 2 (NRF2) and is the first to demonstrate ferroptosis inhibition as a mechanism of berberine to heal wounds, providing new therapeutic opportunities to diabetic wound management [46]. Berberine pretreatment of human HaCaT keratinocytes subjected to advanced glycation end-products to recapitulate the diabetic skin environment can protect cell viability otherwise lost to ferroptotic cell death, indicating that the compound has a direct anti-cytotoxic effect in counteracting the buildup of AGEs. This protective response was eventually followed with great decreases in the production of malondialdehyde, another hallmark of lipid peroxidation indicating the oxidative damage to cell membranes that is the hallmark of ferroptosis. Another way in which berberine counteracted ferroptotic cell death was by preventing the build-up of intracellular reactive oxygen species and mitigating iron build-up in cells, tackling two severe triggers of ferroptotic cell death: oxidative stress, and iron-dependent Fenton chemistry [47]. Notably, berberine increased the levels of glutathione peroxidase 4 (GPX4) and ferritin light chain (FTL) protein- which counter ferroptotic cell death via complementary mechanisms, where GPX4 lowers lipid hydroperoxides in the cell membranes and FTL enhances safe iron sequestration. These effects were blocked with the abrogation of NRF2 knockdown with specific small interfering RNA, supporting the central position of this transcription factor in the mediation of cytoprotective effects of berberine and outlining the mechanistic pathway in which berberine can act to stimulate expression of antioxidant and iron-regulating genes. The NRF2 transcription factor is a global controller of the cellular antioxidant response, which interacts with antioxidant response elements in the promoter of many protective genes and regulate their expression in response to oxidative and electrophilic stress, and this activity of berberine as an activator of this pathway makes it an inducer of the endogenous defense response of the cell rather than a passive antioxidant [48].
The understanding that diabetic wound healing failure is caused by multicurrent pathological processes has far reaching consequences on the design of therapy implying that optimum results will be achieved through interventions that will be able to treat the entire complexity of the disorder. The use of single-agent methods (pharmaceutical agents that inhibit certain molecular pathways or advanced dressings that mitigate the unique wound state) as a monotherapy of diabetic wounds, has resulted in disappointing clinical-trial outcomes. This is expected by the fact that the pathology is multifactorial in nature since only a combination of intervention can achieve simultaneous repair of the dysfunction of keratinocytes, endothelial dysfunction, oxidative stress, inflammation, and infection. The combination methods, which involve the combination of several therapeutic mechanisms, are more promising but they should be developed with specific consideration to the interactions between components and the needs of the diabetic wound environment [49]. The optimal mix would comprise of agents that prevent ferroptosis of the keratinocytes and preserve their proliferative and migratory capabilities, enhance endothelial healing and angiogenesis, decrease oxidative stress and inflammatory states to levels that favor healing, and provide beneficial antimicrobial efficacy with respect to pertinent pathogens such as biofilm-hosting and multidrug-resistant organisms. The agents are expected to possess complementary mechanisms of action that can lead to additive or synergistic effect on combining them, have good safety profiles that are not toxic to prolonged use and also should be compatible with one another as well as with standard wound care procedures such as debridement, offloading, or infection control. In this regard, natural products and herbal medicines have certain benefits, since they often contain more than one pharmacological activity in wound healing, and have a long history of safety when used in traditional medical practice. The discovery of complementing natural compounds with specific mechanisms that can overcome the entire wound pathology of diabetics is a promising approach towards finding more effective treatment options. Berberine and chalcones following their proven impact on keratinocyte protection, endothelial functionality, oxidative stress, inflammation, and infection become especially appealing targets of such a combination strategy, and synergistic improvement of wound healing via various complementary mechanisms can be an option [50]. The large preclinical data base on the individual effect of these compounds gives a good basis to study their combined activities, whereas their historical application in traditional medicine and overall good safety profiles gives credence to the possibility of clinical development. Further investigation aimed at maximizing the berberine-chalcone combinations, their mechanism of action, and determining their effectiveness in the right preclinical and clinical models would undergo a major breakthrough in the management of diabetic wounds and quality-of-life in the millions of diabetic patients who experience this crippling complication. The intersection of contemporary mechanistic conceptualization of diabetic wound pathology with ancient knowledge of medicinal plants provides a possible avenue of more effective treatments that will take into account the full complexity of this complicated disease [51].
Ferroptosis is an iron-dependent lipid peroxidation and loss of cellular redox balance driven cell death, unlike apoptosis, necrosis, and autophagy, which is a regulated mode of cell death. Accumulation of intracellular iron and overproduction of reactive oxygen species (ROS), which facilitates the oxidation of polyunsaturated fatty acids in cell membranes, are the main events of ferroptosis. In normal cells, the antioxidant systems, especially glutathione (GSH)-glutathione peroxidase 4 (GPX4), help cells to avoid such a damage. The presence of GPX4 lowers lipid hydroperoxides to non-toxic lipid alcohols and preserves the membrane integrity. But, in cases where the glutathione is lost or when the GPX4 is suppressed, successful lipid peroxides are produced quickly, and the ferroptotic cell death takes place. Iron metabolism is another important factor since elevated intracellular Fe 2 + may be involved in Fenton reactions to produce highly reactive hydroxyl radicals which only exacerbates oxidative stress on membrane lipids. Simultaneously cytokine signaling pathways play a major role in regulating and determining the effect of ferroptosis. The pro-inflammatory cytokines (tumor necrosis factor-alpha (TNF-a), interferon-alpha (IFN-g), and interleukin 6) triggering signaling pathways such as the JAK/STAT and NF-kB pathways, which regulate the oxidative stress, iron metabolism, and cellular survival pathways. To illustrate, the release of interferon-gamma by activated immune cells may increase lipid peroxidation and cells to ferroptosis through changing the expression of antioxidant and metabolism genes. Moreover, ferroptotic cells can also produce damage-associated molecular patterns (DAMPs) and lipid mediators that further enhance cytokine production and immune cell recruiting, which increases the level of inflammatory signaling in tissues. This two-way communication between ferroptosis and cytokine communication plays a role in the development of various pathological diseases, such as neurodegenerative diseases, cancer, ischemia-reperfusion injury, and inflammatory diseases. These interdependent mechanisms offer meaningful information about possible therapeutic approaches that can be used to regulate ferroptosis and inflammatory signaling to influence the evolution of a disease Fig.2.
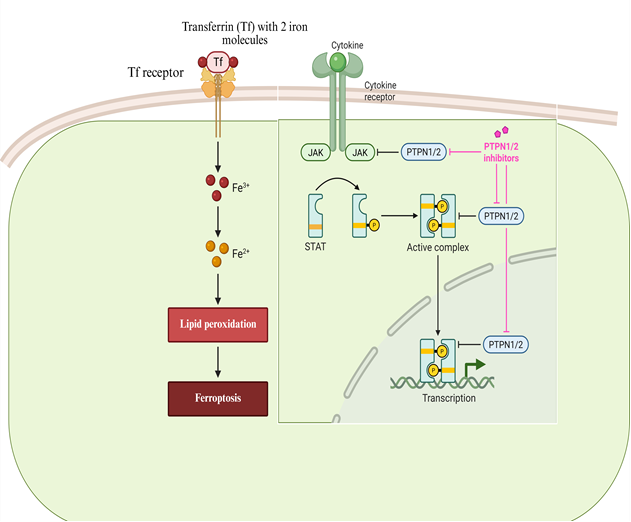
Fig.2: Mechanisms of Ferroptosis and Cytokine Signaling in Cells
These in vitro results were supported by in vivo studies in diabetic mice with the db/db mice that are a well-established type 2 diabetes model that exhibits impaired wound healing, and these studies showed the translational applicability of the ferroptosis-inhibitory effects of berberine. Oral berberine (100 mg/kg/day) treatment over 5 weeks prevented lipid peroxidation in the skin tissues as evidenced by lowering malondialdehyde and 4-hydroxynonenal (compared to untreated diabetic controls) which was indicative that orally administered berberine can reach the skin tissue in adequate levels to confer protective action [52]. The berberine therapy was also able to replace GPX4 and FTL and ferritin heavy chain (FTH) and other NRF2 protein levels that were considerably down-regulated in the diabetic control mice skin, proving that the identified mechanisms are also effective in the intact organism and that the treatment with berberine can reverse the process of damaging the protective pathways caused by diabetes. This article confirms berberine as an anti-ferroptotic agent in diabetic skin and identifies a hitherto unrecognized mechanism of impaired wound healing independent of glucose regulation and offers a justification to take berberine as part of combination therapy of diabetic wounds. Keratinocyte viability maintenance via ferroptotic inhibition augments the other reported actions of berberine on wound healing, such as antimicrobial properties against common pathogens of wounds, regulation of inflammatory response, and effects on angiogenesis which can support the development of granulation tissue. By preserving the population of keratinocytes that is critical to the healing of the wound through re-epithelialization and also preventing the risk of infection and inflammation, berberine can be regarded as a versatile tool in diabetic wound pathology, and its addition to the effect of compounds that specifically modulate other physiological processes of wound restoration, such as the activity of chalcones that stimulate endothelial activity and angiogenesis, can potentially be effective through synergy [53].
Antimicrobial and Anti-inflammatory properties
Berberine: Antimicrobial and Anti-Inflammatory mechanisms in diabetic wound healing
In addition to its cytoprotective properties against ferroptosis, berberine has strong antimicrobial effects that are of high value to the treatment of infected diabetic wounds wherein the colonization of bacteria and the development of biofilms are the primary obstacles to healing and the common outcome of therapy. The antimicrobial effects of berberine have long been known, but have been shown to be effective against a large variety of gram-positive and gram-negative bacteria, fungi, and protozoa, with various mechanisms shown, including disruption of microbial cell membranes, nucleic acid and protein synthesis inhibition and interference with bacterial quorum sensing systems which regulate the expression of virulence factors and biofilm formation. The extensive antimicrobial activity of berberine, in which case all the mentioned bacteria are sensitive, has some benefits in comparison with narrow-spectrum agents that can favor the emergence of resistant bacteria or cannot eliminate mixed-spectrum infections. Recent thorough review has identified the berberine nanoparticles as one of the most promising interventions applicable in the management of diabetic wounds because of the entire range of antimicrobial activity, anti-inflammatory, anti-oxidative, and context-specific angiogenic effects of the compound. Nanoparticle formulation strategy will address one of the conventional weakness of the berberine treatment; its limited bioavailability and low solubility in water, by improving the delivery rate to the wound tissues and extended release to sustain therapeutic levels over long periods. These nanoparticle systems may be programmed to react to particular wound environments to give acidic pH, high levels of glucose or the presence of bacterial enzymes to facilitate controlled delivery of drugs when and where they are most needed [54].
New delivery regimes have been established to increase the therapeutic efficacy of berberine even further in the demanding diabetic wound setting. Zhang et al. (2024) developed an improved nano-drug delivery system based on the combination of berberine and epigallocatechin gallate (EGCG), a polyphenol of green tea which has its own antioxidant and anti-inflammatory effects, coated with manganese dioxide nanoshells and glucose oxidase. The system is a multifunctional system that employs glucose at high concentrations available in diabetic wound sites to react to form a cascade reaction leading to the production of oxygen that in turn promotes the photodynamic antibacterial action of berberine in multidrug-resistant bacteria. The process is that glucose is oxidized to gluconic acid and hydrogen peroxide by glucose oxidase, and hydrogen peroxide is broken down to produce oxygen with the help of manganese dioxide nanoshells. This production of oxygen has two essential purposes, first, it alleviates the severe hypoxia inherent to diabetic wounds which cripples the immune cell functions and contributes to the growth of anaerobic bacteria, and second, it supplies the oxygen necessary in the photodynamic action of berberine that depends on light activation of the compound to produce reactive oxygen species that destroy bacteria. This system would produce effective antibacterial activity even in cases of multidrug-resistant strains of organisms that would otherwise be challenging to eliminate when coupled with an appropriate light irradiation proving that it is possible to incorporate berberine into more complicated therapeutic systems that would target various wound healing barriers at the same time. The glucose-receptive design should be noted to be especially glamorous in the diabetic context, with the pathological excess of glucose (a problem) being turned into a portion of the solution. Another aspect that is being dealt with by this method is the increasing issue of antibiotic resistance as this offers a non-antibiotic antimicrobial approach that eliminates bacteria by disrupting their physical membranes and damaging them with oxidative agents instead of their specific molecular targets which can alter to generate resistance [55].
The succession of coordinated cellular events restores tissue integrity after injury and wound healing is a very complicated and highly controlled biological process. There are usually four overlapping stages of this process, namely hemostasis, inflammation, proliferation, and remodeling. The hemostasis phase occurs instantly after injury and starts with the platelet aggregation and the formation of a clot which aids in the prevention of bleeding as well as gives a temporary framework in which cell migration occurs. Growth factors platelet derived growth factor and transforming growth factor-b are also released by the platelets, thereby triggering the inflammatory response. Inflammatory responses Inflammatory cells such as neutrophils and macrophages move to the wound point during the inflammation stage to eliminate pathogens, damaged cells, and debris. These cells produce cytokines and chemokines that influence immune response and attract more cells that are necessary in the process of repairing tissues. During the proliferative stage, the fibroblasts, keratinocytes, and endothelial cells are also important in the reconstruction of tissue structure. Fibroblasts produce extracellular matrix like collagen whereas endothelial cell stimulates angiogenesis to resume blood flow. Keratinocytes move across the wound bed in a bid to restore the epithelial barrier by re-epithelializing it. Lastly, collagen fibers reorganize and become stronger, and unnecessary blood vessels in the organism are regressed to normalize tissue architecture during the remodeling or maturation stage. Myofibroblasts work towards contraction of the wound, which decreases the size of the wound. The combined action of inflammatory mediators, growth factors, and cell types is involved in conducting the process of effective tissue repair and rebuilding of skin functions Fig.3.
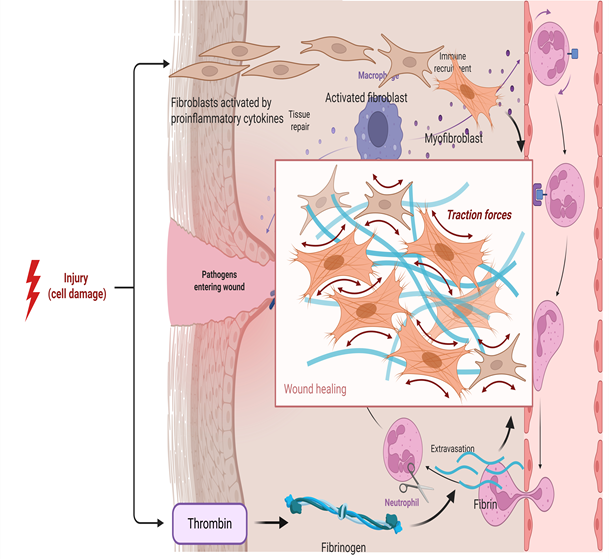
Fig.3: Cellular processes in wound healing injury
In addition to its cytoprotective properties against ferroptosis, berberine has strong antimicrobial effects that are of high value to the treatment of infected diabetic wounds wherein the colonization of bacteria and the development of biofilms are the primary obstacles to healing and the common outcome of therapy. The antimicrobial effects of berberine have long been known, but have been shown to be effective against a large variety of gram-positive and gram-negative bacteria, fungi, and protozoa, with various mechanisms shown, including disruption of microbial cell membranes, nucleic acid and protein synthesis inhibition and interference with bacterial quorum sensing systems which regulate the expression of virulence factors and biofilm formation. The extensive antimicrobial activity of berberine, in which case all the mentioned bacteria are sensitive, has some benefits in comparison with narrow-spectrum agents that can favor the emergence of resistant bacteria or cannot eliminate mixed-spectrum infections. Recent thorough review has identified the berberine nanoparticles as one of the most promising interventions applicable in the management of diabetic wounds because of the entire range of antimicrobial activity, anti-inflammatory, anti-oxidative, and context-specific angiogenic effects of the compound. Nanoparticle formulation strategy will address one of the conventional weakness of the berberine treatment; its limited bioavailability and low solubility in water, by improving the delivery rate to the wound tissues and extended release to sustain therapeutic levels over long periods. These nanoparticle systems may be programmed to react to particular wound environments to give acidic pH, high levels of glucose or the presence of bacterial enzymes to facilitate controlled delivery of drugs when and where they are most needed [56].
Inflammatory responses are also regulated by the use of Berberine using several signaling pathways to supplement antimicrobial and antioxidant effects to solve the chronic inflammation found in non-healing diabetic wounds. The inflammatory reaction to tissue damage consists of a strict time program whereby the initial pro-inflammatory cues enlisting the recruitment of immune cells to remove debris and pathogens are followed by a shift to pro-resolving cues that ensure the repair of tissue. This does not happen in diabetic wounds and instead causes chronic inflammation that is characterized by unresolved infiltration of neutrophils and macrophages, persistent elevation of pro-inflammatory cytokines such as tumor necrosis factor-alpha, interleukin-1 beta, and interleukin-6, and a loss of macrophage polarization between the pro-inflammatory M1 phenotype and the pro-reparative M2 phenotype. Berberine acts on this inflammatory environment by acting on numerous signaling pathways, such as the AKT pathway, which controls cell survival and cellular metabolism, the AMPK pathway, which monitors cellular energy status and controls inflammatory responses, and glucose transporter regulation, which regulates cellular glucose intake and glucose metabolism [57]. The activation of AMPK by berberine is of particular importance because AMPK is a metabolic master switch facilitating catabolic processes that produce ATP and inhibiting anabolic processes that consume ATP, and stimulating mitochondrial biogenesis by activating AMPK has been demonstrated to suppress inflammatory responses by inhibiting the NF-kB signaling pathway and stimulating mitochondrial biogenesis that generates cellular stress-resilience. The anti-inflammatory actions of berberine are extended to macrophage actions in which researchers have found that the administration of berberine leads to polarization on the M2 phenotype which produces anti-inflammatory cytokines and growth factors which aid in the process of tissue repair. This regulation of the inflammatory condition, together with the antimicrobial effect of berberine withdrawing the infectious stimulus of inflammation and its antioxidant action of eliminating oxidative stress-induced inflammatory signaling, provide a multi-dimensional approach towards normalizing the diabetic wound environment [58]. Berberine can be used to reverse the conditions that cause chronic inflammation by dealing with the various factors that maintain it, including chronic infection, oxidative stress, and cellular signaling imbalances, and can thus facilitate the wound healing process of passing through the stages of healing expected. Combined with the recently described ability to prevent keratinocyte ferroptosis, these multifactorial effects put berberine as a singularly broad-spectrum agent in the treatment of diabetic wound care that targets the pathophysiology of this difficult disorder in a complex, multifactorial manner [59].
Chalcones: wound healing properties and mechanisms
These results make chalcones promoters of re-endothelialization, an important step in angiogenesis and wound vascularization that is frequently damaged in diabetic patients, and that is a major cause of slow wound healing. The process where endothelial cells regenerate the denuded blood vessel surfaces or generate novel capillary sprouts in angiogenesis and involves highly coordinated endothelial cell growth, motility, and tubing is called re-endothelialization. Various factors such as decreased bioavailability of nitric oxide, oxidative stress disrupted endothelial cells, and unregulated growth factor signaling leading to inappropriate angiogenic stimulation are the cause of impaired re-endothelialization in diabetic wounds. The strength with which chalcones can undertake multiple effects of dysfunction in endothelial cells stimulates the generation of nitric oxide via activation of eNOS, stimulates the generation of the cytoprotective enzyme HO-1, and, in addition, produces carbon monoxide, which further stimulates the nitric oxide signal, indicates that the compounds may be especially active in the demanding diabetic condition. Chalcones have the potential to improve granulation tissue-forming and enhance wound vascularization and faster wound healing by restoring endothelial function and facilitating re-endothelialization. The synergistic action of chalcones, which affect endothelial activity targeting the nitric oxide and heme oxygenase pathways, and the action of berberine on the protection of keratinocytes by inhibiting ferroptosis and its antimicrobial and anti-inflammatory actions develop a strong case in favor of combination therapy that would cover several cell groups and pathological mechanisms. The research needs to be extended to investigate whether the chalcones and berberine combination exhibits additive or synergistic effects on wound healing, and whether the combinations can result in a better outcome than does the individual agent in preclinical diabetic wound models and ultimately in clinical trials. The positive safety profile of chalcones of edible sources such as Angelica keiskei, as well as the long history of its traditional use and the growing clinical interest in the use of the compounds, warrant their further development as the constituents of multi-target therapeutic agent to diabetic wounds and other diseases with compromised tissue repair [60].
Mechanistic complementarity
The combination of berberine and chalcones offers theoretical advantages through complementary and potentially synergistic mechanisms targeting different aspects of diabetic wound pathology (Table 1).
Table 1: Complementary Mechanisms of Berberine and Chalcones in Diabetic Wound Healing
|
Target |
Berberine Mechanisms |
Chalcone Mechanisms |
|
Keratinocytes |
Inhibits ferroptosis via NRF2 activation; upregulates GPX4, FTL, FTH |
Limited direct evidence; antioxidant effects may provide indirect protection |
|
Endothelial cells |
Modulates angiogenesis (context-dependent) |
Promotes migration; induces NO and HO-1; activates eNOS |
|
Oxidative stress |
Reduces ROS and lipid peroxidation; activates NRF2 |
Induces HO-1; free radical scavenging |
|
Inflammation |
Modulates NF-κB, AMPK pathways |
Inhibits NF-κB and p38 MAPK; suppresses COX-2 |
|
Infection |
Direct antimicrobial activity; enhances photodynamic therapy |
Antimicrobial properties documented |
The newly described effect of berberine in the inhibition of ferroptosis is a response to the keratinocyte death, which inhibits re-epithelialization in diabetic wounds. At the same time, chalcones induce endothelial repair, angiogenesis, and sufficient supply of vascularization of the healing tissue. The two compounds fight oxidative stress by binding to NRF2 and HO-1 respectively, respectively, and operate synergistically, forming a complex antioxidant system [61].
Failure in the healing of diabetic wounds is due to a combination of coexisting pathological processes that interact in a synergistic manner to develop an environment that is highly hostile to the process of tissue repair and that any attempt to treat these conditions using individual agents, no matter how potent or specific that agent is, is unlikely to produce optimal clinical therapy. This underlying incompatibility between the specific mechanism of action of most pharmaceutical agents and the multifactorial characteristics of the condition it aims to treat is likely the cause of the failure of many of its promising compounds in clinical testing in the treatment of diabetic wounds. Prolonged hyperglycemia pushes the generation of advanced glycation end-products that build up in the skin and cause cytotoxic effects on all cell types that are implicated in the healing process [62]. The effect on the endothelium is dysfunction, which leads to impaired angiogenesis that lacks sufficient vascularization of the granulation tissue. Chronic oxidative stress destroys cellular elements and overloads body antioxidant mechanisms. Unregulated inflammation does not cause a shift between the first stage of pro-inflammatory to the next pro-reparative phase that should take place thereafter. Infection, usually with biofilm-forming and multidrug-resistant organisms, generates a chronic inflammatory stimulus that continues tissue destruction. The recently described phenomenon of ferroptosis as a major form of keratinocyte death in diabetic skin directly undermines the epithelial population necessary to restore the skin to its former state. All these pathological processes have a contribution to the impairment of healing, and each of them interacts with each other in complex forms increasing their individual effect: oxidative stress enhances ferroptotic, inflammation stimulates further oxidative stress, infection stimulates inflammation, and endothelial dysfunction decreases oxygen delivery to enhance all the other processes. To stop this vicious cycle, an intervention is needed that can focus on a number of therapeutic processes working together to reestablish the orchestrated cellular and molecular milieu to allow normal healing [63].
This complexity is overcome with the interaction of berberine and chalcones with complementary and potentially synergetic effects on the key pathological events that undermine the healing of diabetic wounds. The survival of keratinocytes, a crucial step in re-epithelialization, is directly guarded by the recently discovered anti-ferroptotic potential of berberine in activation of NRF2 and expression of GPX4 and ferritin proteins that inhibit the process of lipid peroxidation and free iron sequestration. This process maintains the cellular population that is in charge of replacing the wounded bed thus that once the conditions conducive to migration arise, viable keratinocytes will be used to perform the complex behaviors that are needed in epithelial closure. Chalcones stimulate endothelial activity and angiogenesis, which are vital in vascularization of granulation tissue, provision of oxygen and nutrients to cells in a wound, by increasing nitric oxide, eNOS activation, and heme oxygenase-1 upregulation with subsequent carbon monoxide-mediated amplification of NO signaling. These effects respond to the endothelial dysfunction that diabetes causes and replaces the ability of the body to form new blood vessels which are critical in sustaining the tissue metabolic needs. Both compounds reduce oxidative stress, which damages membranes of cellular structures, proteins, and DNA and promotes inflammatory signaling and ferroptosis, and both compounds act complementary: berberine activates the NRF2 transcription factor that regulates the expression of various antioxidant enzymes such as GPX4, catalase, and superoxide dismutase, whereas chalcones induces heme oxygenase-1 that produces biliverdin and bilirubin with direct antioxidant properties [64]. This bilateral response to oxidative stress produces a complex antioxidant response that might be more efficient than either of the two mechanisms individually because the compounds act on both transcriptional expression of antioxidant enzymes as well as antioxidant molecule formation as small molecules. Both compounds regulate the formation of inflammation which cannot be resolved in diabetic wounds and leads to the development of a chronic pro-inflammatory condition and, as a consequence, prevents the shift of the pro-inflammatory M1 macrophages towards pro-reparative M2 macrophages and inhibits production of inflammatory cytokines that reinforce tissue damage. The antimicrobial effects of both compounds counter infection, a direct barrier to healing, and a stimulus to continuous inflammation, and berberine, in this case, is a broad-spectrum antimicrobial, inhibiting both bacteria and fungi, whereas chalcones is an added antimicrobial that may be especially useful in relation to biofilm-forming organisms. The synergistic mechanism of the two complementary processes is a comprehensive treatment method that covers almost all key areas of diabetic wound pathology simultaneously, and this provides the possibility of clinical outcomes that would not be the case with interventions of one or another mechanism [65].
This poly-target approach is quite consistent with the key principles of herbal medicine since complex combinations of compounds have been used over millennia specifically due to the fact that they exhibit therapeutic effects that cannot be achieved with single compounds. The conventional herbal formulations are usually made up of several herbs each comprising of many bioactive compounds that synergize to form a cocktail which is capable of meeting the complex demands of complex diseases. The insight of these traditional methods is becoming progressively verified by the modern pharmacological studies that interrelations of compounds with complementary action may result in additive or synergistic action, and also may potentially lessen toxicity due to the possibility of lowering the dose administered of the individual components. Applied to diabetic wound healing, this principle would propose that berberine and chalcones can synergistically produce an effect that neither of the two compounds could accomplish by itself because of their long history of safe medicinal use [66]. The combination may also potentially generate actual synergy, with the joint effect being greater than the sum of the effects of the individual components, due to some possible actions by one compound to increase the bioavailability or tissue penetration of the other compound, one compound to inhibit pathways that would otherwise hamper the efficacy of the other compound, or the compounds targeting different points of signaling pathways that are interconnected to cause exaggerated downstream effects. Additive effects due to complementary mechanisms would still be a large improvement over those using single agents even in the absence of real synergy as the combination would cover a wider array of pathological processes than a single compound. The safety and tolerance of berberine-containing plants such as Coptis chinensis, and chalcone-rich plants such as Angelica keiskei have been used in traditional medicine systems and therefore offer further assurances regarding the safety and tolerability of these classes of compounds, and the modern scientific knowledge of their mechanisms offers a rational falsehood to optimize their combination, and the type of patients that may respond most to them [67].
Preclinical combination studies
Although the use of berberine and chalcones has been studied separately in different conditions related to wound healing, no literature on the use of combinations of berberine and chalcones in diabetic wound models has been published, which is a critical gap that should be filled by systematic preclinical studies before the clinical translation is initiated. The lack of combination studies is not accidental due to the fact that the ferroptosis-inhibitory effect of berberine in diabetic keratinocytes was recently reported, and the endothelial actions of chalcones, in turn, have a longer history, yet not tried in conjunction with berberine. Critical preclinical research must involve in vitro evaluation on the model of the diabetic wound with appropriate cell culture models. The cells of the human keratinocytes HaCaT and primary human epidermal keratinocytes must be subjected to high glucose levels, and advanced glycation end-products to simulate the diabetic state, and then subjected to berberine alone, chalcones alone, and at different ratios and concentrations. Ferroptotic protection can be determined through cell viability assays, whereas cell motility on keratinocyte motility necessary to resolve the epithelialization process can be determined through migration assays with scratch wounds. The study should be done once again with parallel experiments on human endothelial cells, both macrovascular and microvascular and they should be tested to be protected against dysfunction caused by high glucose as well as to stimulate migration and tube formation that are indicative of the angiogenesis process. The checkerboard assays, where the different concentrations of each compound are used in all possible combinations, could be used to identify whether combinations have additive or synergistic effect on the main results and what ratios of concentrations of the compounds would be of interest to be considered further. Such in vitro experiments must also investigate activity on oxidative stress signatures, production of inflammatory mediators and expression of important proteins such as NRF2, GPX4, ferritin, HO-1, and eNOS to initiate a better understanding of the combination processes [68-70].
The next step to confirm the therapeutic potential of the combinations of berberine and chalcone in wound healing is the studies in vivo wound healing of a proper animal model. Diabetic mouse models, such as the genetically diabetic db/db mice and streptozotacin-induced diabetic mice, are able to offer well-characterized systems with impaired wound healing that mimic a large number of aspects of human diabetic wounds. On the back of these animals, full-thickness excisional wounds are to be made and treatments done topically (in the form of creams, gels or dressings) or systemically (by oral gavage or injection) to compare berberine alone, chalcone alone, combination treatment and control of the vehicle. Planimetry should be used to monitor the wound closure over time, and digital analysis and image analysis to measure the reduction of the wound area. Wounds are to be harvested and analyzed by histology with hematoxylin and eosin stains to assess the general morphology, masson trichrome staining to assess collagen structure, and immunohistochemistry stains of proliferation (Ki67), angiogenesis (CD31), inflammation (F4/80 of macrophages with M1 and M2 markers) and specific pathway activation (NRF2, HO-1). The expression of antioxidant defense, inflammation, and tissue repair genes and proteins can be quantified in the wound tissue with the use of molecular analysis in the form of quantitative PCR and western blotting. These experiments must use enough animals in each group to identify clinically significant differences and must be constructed to measure the initial impact on inflammation and oxidative stress and subsequent impact on wound healing and tissue properties [71].
Combinations Mechanistic dissection of combination effects needs to go beyond documenting efficacy to describing the mechanisms by which berberine and chalcones interact at a molecular level. Research must aim to establish whether or not combination treatment has more NRF2 activation, HO-1 induction, or ferroptosis inhibition than the respective compounds, and the nature of the effect (additive or synergistic). It is also significant to investigate the possibility of cross-talk between signaling pathways because the main mechanism of action of berberine is NRF2 activation and chalcones inducing HO-1 by a mechanism that may also involve NRF2 but can involve other regulatory factors. The fact that carbon monoxide-mediated eNOS activation is mediated by chalcones and the antioxidant properties of the two compounds could lead to positive feedback loops which enhance protective responses. Combination effects Scramble with genetic methods can be defined by knockout mouse models, or siRNA knockdown in cells, can determine whether that particular pathway is necessary to clarify any combination effects, or by analyzing whether that combination effects has a redundant pathway that would otherwise be needed, but when that pathway is knocked down. These mechanistic experiments will not only focus on how the combination acts but will also be able to find biomarkers which could predict response and be used to select out patients in future clinical trials [72].
Formulation and delivery optimization
The formulation of the physicochemical properties of both berberine and chalcones has a formulation challenge, which will have to be tackled to ensure the best rate of therapeutic efficacy of compounds since the most potent combination of compounds will not help, unless it can be able to deliver the compounds to the target tissues in sufficient amounts. Poor water solubility, widespread intestinal metabolism, and active efflux across the intestinal lumen via P-glycoprotein transporters, has notoriously restricted oral bioavailability of berberine, and consequently, wound healing effects of the agent when administered orally may be inadequate. Nanoparticle formulations however have proven to have significant potential of improving the delivery of berberine where a number of methods have been used that have shown enhanced bioavailability and targeted delivery such as liposomes, polymeric nanoparticles, solid lipid nanoparticles and inorganic nanoparticles. Advanced delivery systems can also be beneficial to chalcone bioavailability, since most chalcones lack solubility in water and are also subject to unreliable absorption. The use of combination formulations also requires that attention should be paid on how to deliver the two compounds together in a way that will ensure that they reach target tissues in the right proportions and at right time [73].
Topical preparations such as hydrogels, creams, ointments, and films are the closest method of wound application, whose problems of systemic absorption and first-pass metabolism are evaded and whose high concentrations are directly deposited to the wound bed. The hydrogel, especially hydrogels, is of particular interest in wound care since it is able to keep the wound moist, absorb exudate, and cool and provide pain relief as well as release drugs incorporated into it in a controlled way. During formulation development, suitable gelling agents, preservatives, and penetration enhancers incompatible with berberine or chalcones and incompatible with maintaining the stability and activity of the compounds should be found. This is the benefit of nanoparticle co-delivery systems where the simultaneous penetration of both compounds into the tissue is achieved (and nanoparticles can be programmed to release their payloads under as yet undescribable wound-specific conditions like elevated glucose, acidic pH or bacterial enzymes). The glucose-responsive system designed by Zhang et al. to deliver berberine may be potentially modified to combine delivery, with chalcones being added to the same or different nanoparticles. Formulations that are controlled to release therapeutic concentrations during the long period of healing that is characteristic of diabetic wounds would lessen the frequency of dressing changes and enhance patient compliance. Completely developed delivery systems may also include more features like wound health monitoring in real-time, on-demand delivery, or even on smart bandages that update the user on wound healing status. The delivery system will be determined finally by the clinical situation and various formulations will be tailored to the wound location, type and patient characteristics [74].
Safety and clinical translation
Both the berberine and chalcones have shown a good safety profile in various preclinical trials and in clinical practice with berberine having a history of use as an over-the-counter supplement in metabolic disorders and the chalcones being dietary constituents and having a long safety history. Nevertheless, their concomitant safety can not be guaranteed with references to the individual safety profile since there might be drug-drug interactions, which may cause a shift in metabolism, raise the toxicity, or have an unanticipated adverse outcome. Before clinical trials, thorough toxicological evaluation of the combination should be done, such as standard acute and repeated-dose toxicity tests in suitable animal models, local tolerance testing of topical formulations, and potential evaluation of genotoxicity, carcinogenicity and reproductive toxicity. Such studies need to be done based on regulatory recommendations and Good Laboratory Practice in order to facilitate subsequent Investigational New Drug submissions [75].
Clinical translation would occur in a well-organized chronology of experiments that would start with dose-ranging studies on healthy volunteers or patients with diabetic wounds in order to determine the most appropriate ratios of combination and the optimal dose regimens. These initial studies must determine pharmacokinetics of both drugs during co-administration, to identify any drug-drug interactions that may change absorption, distribution, metabolism or excretion. Evidence that the combination is impacting its intended targets at feasible dosages may be provided by biomarkers of target engagement, e.g. NRF2 activation in accessible tissues or circulating indicators of oxidative stress and inflammation. Preliminary efficacy indications in patients with chronic diabetic ulcers would then be assessed in proof-of-concept trials using standard wound assessment tools, with close attention paid to wound characteristics, wound healing rate, and other biomarkers. These trials are to be randomized, controlled, and preferably to be double-blinded to decrease bias, and the sample size should not be too big because it can be prohibitively expensive to run a trial with a large sample in the early stages of study. To prove the role of berberine-chalcone combinations in clinical practice and facilitate regulatory approval and reimbursement, comparative effectiveness studies versus standard care, including advanced dressings, growth factors, and other evidence-based interventions, would eventually be required. To make sure that the combination would not only shorten the time of wound healing, but also provide more desirable experience to the patients with this difficult condition, patient-reported outcomes such as pain, quality of life and treatment burden would have to be integrated into clinical development [76-78].
CONCLUSION
The rationale behind synergistic herbal treatment of diabetic patients using berberine and chalcones and the opportunity to offer a scientifically premised approach to managing diabetic wounds is the finding that the multifactorial nature of diabetic wounds does not inherently fit into the narrow spectrum of most conventional treatments. The recently uncovered effect of berberine in inhibiting NRF2-mediated keratinocyte ferroptosis to protect the epithelial cells required in wound resurfacing and the recently discovered chalcone-mediated enhancement of endothelial wound healing through nitric oxide and heme oxygenase-1 signatures to reestablish the angiogenic ability of the granulation tissue, provide a further avenue to keratinocyte ferroptosis. The two compounds play redundant yet complementary roles in antioxidant, anti-inflammatory and antimicrobial effects that, together, target the adverse wound environment associated with diabetes. This multi-targeted treatment has been shown to support the traditional wisdom of herbal medicine, in which complex combinations are specifically appreciated due to their capacity to treat complex diseases, as well as, with the current understanding of the pharmacology in general, in which combination therapies that target more than one disease mechanism are generally reported to be more effective in complex chronic diseases. Although direct evidence of combinations of berberine and chalcone in the wound healing of diabetics has yet to be produced, there is compelling mechanistic reasoning behind the use of every of these compounds alone and substantial preclinical evidence has been produced to this effect. The positive safety profiles of the two compounds and their long-standing use in traditional medicine systems, as well as the desperate necessity to find more effective ways of diabetic wound treatment, give a good rationale to continue with this stream of research. The preclinical combination studies should be used in future research to determine the proof-of-concept and maximize ratios, develop formulations to ensure effective delivery, conduct systematic toxicological studies to confirm the safety, and ultimately translate to clinical research using well-designed trials. The increasing worldwide presence of diabetic wounds with millions of patients having non-healing wounds that put the limb and life at risk necessitate new methods of addressing them which can result in better outcomes as compared to the present therapies. The integration of berberine and chalcones, based on traditional knowledge, and modern mechanistic knowledge has true potential to address this emergency medical necessity and warrants serious study to find out whether this synergistic form of herb can live up to its therapeutic possibilities.
REFERENCES


Megha Shitole, Shivam Kumar, Somenath Routh, Vibhu Bansal, Prathmesh Chikale, Himanshu, Targeting Diabetic Wound: A Synergistic Herbal Approach of Berberine and Chalcone Potential, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3038-3068. https://doi.org/10.5281/zenodo.19216245
 10.5281/zenodo.19216245
10.5281/zenodo.19216245
