Nootan College of Pharmacy, Kavthe-Mahankal
Recent advancements in cancer immunotherapy, including immune-checkpoint blockade, adoptive cellular therapy, and vaccines, have transformed treatment. Understanding T cell evolution is critical due to variable patient responses.1 Single-cell technologies and TCR analysis enable detailed characterization of intratumoral T cell states and antigen specificities, facilitating the tracking of T cell trajectories and phenotypic changes to elucidate effective immunotherapy mechanisms. 2This review examines T cell subsets linked to positive responses and how immunotherapies activate tumor-specific T cells to inform future strategies. T lymphocytes are central to employing the immune system against cancer, with their antigen-directed cytotoxicity being key. Advances in T cell biology have resulted in successful therapeutic modalities like checkpoint blockade, adoptive cellular therapy, and cancer vaccinology over the past 50 years.3 Natural killer (NK) cells also play a significant role by rapidly eliminating transformed cells. Ex vivo activation, expansion, and genetic modification of NK cells can improve their antitumor activity and overcome tumor resistance mechanisms. Clinical trials involving NK cell infusions for hematological malignancies and solid tumors have shown encouraging results, utilizing established clinical-grade platforms. 4Future NK cell products will be engineered for enhanced activation, proliferation, suppression of inhibitory signals, and improved tumor homing. Emerging evidence also suggests increased NK cell-mediated tumor cell killing when combined with molecularly targeted therapies, establishing NK cells as crucial components of multifaceted cancer treatment strategies.
Cancer immunotherapy represents an innovative approach to tumor treatment, offering potential advantages over traditional therapies by prolonging progression-free survival (PFS) and overall survival (OS). However, it is characterized by complexity and uncertainty, with the risk of severe adverse reactions due to overactive immune responses.5 The field is actively exploring more effective immunological checkpoints with fewer side effects. This review provides an overview of recent advancements in cancer immunotherapy, analyzing its pros and cons to project future treatment directions.
Immunotherapy functions by modulating the immune system and its microenvironment to target cancer cells. While combinations with traditional therapies or multiple immune checkpoint inhibitors (ICIs) can enhance effects, specific outcomes require further study.
Cellular immunotherapy aims to harness the body's immune cells to identify and kill tumors. 6Adoptive Cellular Immunotherapy (ACI), a key area, involves administering modified and amplified immune cells. It can be non-specific (e.g., NK cells, CIK cells) or specific (e.g., TIL therapy, TCR-T, CAR-T). Specific ACI, particularly CAR-T, shows strong specificity and is primarily used for blood tumors, while TIL therapy is mainly applied to melanoma due to collection difficulties.
Despite infiltrating the tumor microenvironment (TME), T cells often fail to eradicate cancer cells due to acquired dysfunction and immune evasion, hindering long-term remission in many patients. Restoring anti-tumor T cell functionality is a key goal of modern immunotherapies, but improving efficacy requires a deeper understanding of T cell properties and dynamics. Challenges include identifying specific T cell subsets, characterizing diverse T cell specificities, and tracking dynamic responses. 7Technological advancements, such as single-cell RNA sequencing (scRNA-seq) and single-cell TCR sequencing (scTCR-seq), coupled with TCR reconstruction, now allow for comprehensive analysis of anti-tumor T cells within the TME and their modulation by immunotherapies.
T cell :
Immune cells, particularly T cells with their specific T cell receptors (TCRs) recognizing antigens presented by human leukocyte antigen (HLA) molecules, are fundamental to cancer immunotherapy.8 Under normal conditions, antigen-triggered T cell stimulation leads to effector and memory cell generation, providing robust immune responses. However, in the tumor microenvironment (TME), T cells often fail to eradicate tumor cells despite infiltration and recognition, acquiring a dysfunctional state that facilitates tumor immune evasion. 9Restoring the functionality of tumor-specific T cells in the TME is a central aim of modern immunotherapies. Despite advancements, only a minority of patients achieve long-term remission, emphasizing the need for a deeper understanding of antitumour T cell properties and dynamics.10 Challenges in deconstructing the antitumour T cell landscape include the broad spectrum of T cell functional states, the diverse specificities of tumor-infiltrating lymphocytes (TILs) making TCR identification difficult, and the dynamic nature of T cell responses requiring meticulous longitudinal sampling. Recent technological advances, such as single-cell RNA sequencing and single-cell TCR sequencing, enable the assignment of phenotypic characteristics to T cell clonotypes at an individual cell level. 11TCRs also serve as molecular barcodes to track antigen-specific populations across time and compartments, and TCR reconstruction in reporter cell lines allows for interrogation of TCR antigen specificity and biochemical properties. The combination of these capabilities facilitates comprehensive investigation of antitumour T cells within the TME and following immunotherapeutic intervention.
T CELL Dynamics and specification
12Recent advancements in cancer immunotherapy, including immune checkpoint blockade, adoptive cellular therapy, and vaccines, have transformed cancer treatment. However, variability in patient responses necessitates a deeper understanding of T cell evolution in response to these interventions.13 Multidimensional single-cell technologies now allow for the dissection of lymphocyte states within the tumor microenvironment (TME) and the linking of intratumoral phenotypes to T cell receptor (TCR) antigen specificity. This enables the investigation of tumor-specific T cells, tracking their dynamics and phenotypic changes through TCR clonality.14 The presence and functionality of T cells within tumors (tumor-infiltrating lymphocytes or TILs) are crucial prognostic factors, with their infiltration often correlating with better clinical outcomes. TILs exist in a spectrum of phenotypic states, varying in differentiation, cytotoxicity, and proliferative potential. Despite these insights, challenges remain in precisely identifying T cell subsets responsible for effective anti-tumor responses due to the broad range of T cell functional states and specificities, and the technical demands of identifying tumor-specific TCRs at scale. 15The dynamic nature of T cell responses over time and across tissue compartments also requires meticulous longitudinal sampling. Technological advancements such as single-cell RNA sequencing and single-cell TCR sequencing have been pivotal in assigning phenotypic characteristics to T cell clonotypes and tracing antigen-specific populations.16 TCR reconstruction in reporter cell lines further allows for the interrogation of TCR antigen specificity and biochemical properties. The combination of these technologies provides a comprehensive means to study anti-tumor T cells within the TME and in response to immunotherapy, aiming to inform the development of more effective treatment strategies by elucidating factors that elicit productive anti-tumor T cell immunity.
Immune server checkpoints
Evolutionarily conserved negative regulators of T cell activation, known as checkpoint molecules, fine-tune immune responses and prevent hyperactivation. 17Cytotoxic T lymphocyte antigen 4 (CTLA4) and programmed cell death 1 (PD1) are key examples, functioning at different times and sites in the T cell lifespan, thus complementing each other. This complementary action allows T cell responses to maintain self-tolerance while effectively combating pathogens and neoplasia. 18Targeting CTLA4 and PD1 has proven successful in treating various difficult-to-treat cancers, a breakthrough recognized with the 2018 Nobel Prize in Physiology or Medicine awarded to James P. Allison and Tasuku Honjo.
Immune checkpoint treatment
Immune checkpoint therapy utilizes evolutionarily conserved molecules that act as negative regulators of T cell activation to modulate the immune response and prevent overactivation. 19Key examples include Cytotoxic T lymphocyte antigen 4 (CTLA4) and programmed cell death 1 (PD1), which function at different stages and locations within the T cell lifespan. These checkpoints work complementarily to maintain self-tolerance while enabling the body to defend against pathogens and cancer. 18The successful targeting of CTLA4 and PD1 in treating various difficult-to-treat cancers was recognized with the 2018 Nobel Prize in Physiology or Medicine awarded to James P. Allison and Tasuku Honjo.
20Immune checkpoint treatment refers to a class of therapies designed to enhance the body's immune response against cancer. These treatments work by targeting specific molecules, known as immune checkpoints, that cancer cells exploit to evade detection and destruction by the immune system. Immune checkpoints are essentially "brakes" on immune cells, preventing them from attacking healthy tissues. However, cancer cells can hijack these checkpoints to suppress anti-tumor immune responses. Immune checkpoint inhibitors (ICIs) are drugs that block these inhibitory signals, thereby "releasing the brakes" on immune cells, such as T-cells, and enabling them to recognize and attack cancer cells more effectively. 21Key examples of immune checkpoints targeted by these therapies include Programmed cell death protein 1 (PD-1), its ligand Programmed death-ligand 1 (PD-L1), and Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4). By inhibiting these pathways, ICIs can restore and amplify anti-cancer immunity, leading to durable clinical responses in a significant proportion of patients across various cancer types.
T-cell adoption treatments
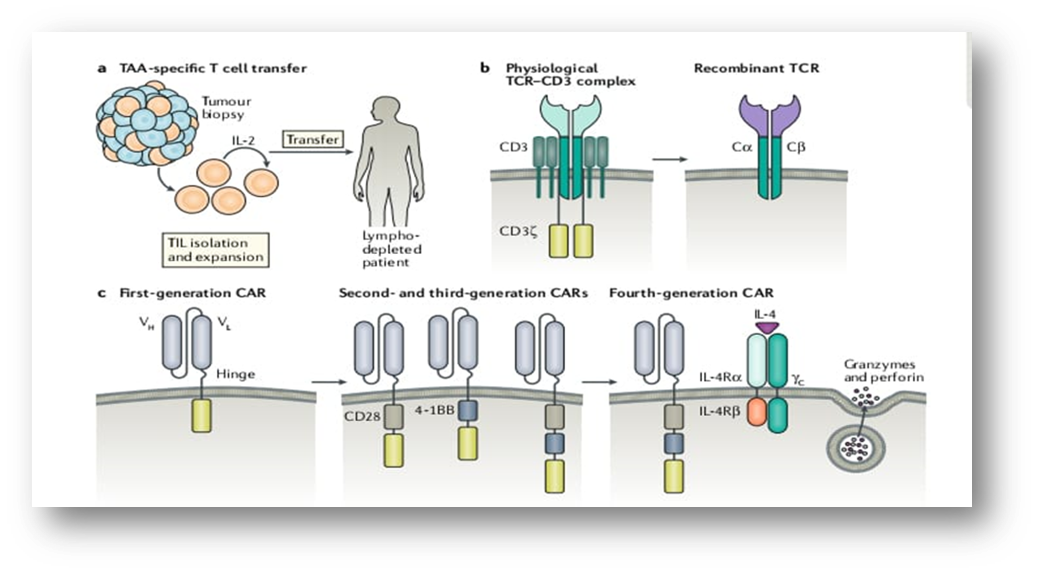
22Adoptive cell transfer (ACT) is an immunotherapeutic strategy that involves the ex vivo expansion and infusion of autologous lymphocytes possessing antitumor activity into cancer patients. This method aims to amplify antigen-specific T-cell populations, thereby augmenting the antitumor immune response through cytokine release and tumor cell lysis. ACT necessitates the isolation or generation of autologous lymphocytes with antitumor capabilities. One approach involves isolating Tumor-infiltrating lymphocytes (TILs) from patient tumor samples, followed by ex vivo culture and expansion to therapeutic numbers, although the difficulty in achieving sufficient TIL expansion has limited its application beyond melanoma. A more direct method is the production of genetically engineered autologous T cells expressing tumor antigen-specific T-cell receptors (TCRs) or chimeric antigen receptors (CARs). TCR-engineered T cells are created by transferring antigen-specific TCR genes into lymphocytes isolated from peripheral blood, with these genetically modified cells, termed designer T cells (dTcs), then expanded in vitro. 23Successful examples include TCR-based dTcs targeting melanoma antigens (MART-1, gp100) that induced tumor regression in treatment-refractory melanoma, dTcs targeting NY-ESO-1 CTA showing objective responses in synovial cell carcinoma, and dTcs targeting GD2 leading to responses in neuroblastoma. CAR-modified T cells feature an extracellular targeting domain fused to an intracellular signaling domain, recognizing antigens independently of human leukocyte antigens (HLAs), thus offering broader clinical applicability compared to TCRs. Despite positive outcomes with TCR- and CAR-based therapies, optimization is needed to mitigate toxicity and overcome the immunosuppressive tumor microenvironment. Enhancing therapeutic efficacy can be achieved through IL-2 administration and host lymphodepletion (using combinations of cyclophosphamide, fludarabine, and total body irradiation) prior to ACT. Lymphodepletion is thought to work by eliminating immunosuppressive regulatory T cells (Treg) from the tumor microenvironment.24 Preliminary data indicate response rates of 50-70% in metastatic melanoma patients treated with TILs, IL-2, and intensive lymphodepletion. An ongoing trial is assessing HPV E6- and E7-reactive TILs (HPV-TILs) for metastatic HPV-positive cancers, with an interim analysis of cervical cancer patients showing complete responses in 2 of 9 treated individuals. Allogeneic stem cell transplantation (AlloSCT) can also be considered a form of unselected ACT, wherein donor-derived lymphocytes stimulate a graft-versus-tumor (GVT) effect, resulting in long-term cancer control.
Adoptive T cell (ATC) therapy, which involves infusing autologous or allogenic T cells into cancer patients, has emerged as a promising treatment modality. 25Early evidence for its viability dates back to 1966, with Southam et al. observing tumor regression in patients with advanced cancer following co-transplantation with patient-derived leukocytes and autologous tumor cells. Clinically, allogeneic hematopoietic stem cell transplants for leukemia represented an initial effective application of adoptive transfer, with T cell graft-versus-tumor response identified as the mechanism for clinical improvement.
26A significant advancement in ATC therapy was the pioneering use of tumor-infiltrating lymphocytes (TILs) for metastatic melanoma in the late 1980s, which involved isolating, expanding with IL-2, and reinfusing these lymphocytes.27 This early approach achieved an objective response rate of 34%, though the median duration of response was limited to four months. Later studies integrated lymphodepletion before ATC therapy, leading to more favorable outcomes in metastatic melanoma patients, with complete tumor regression observed in 22% of cases, and sustained complete remission in 19 of those patients after three years. Recent innovations include the application of high-throughput technologies to identify and enrich for neoantigen-specific TILs, demonstrating potential in metastatic breast cancer. Additionally, the knockdown of the gene for cytokine-inducible SH2-containing protein (Cish), a negative regulator of TCR signaling, has shown potential to augment the antitumoral response of ATC therapy in experimental models. 28A key challenge for TIL-based ATC therapy remains the requirement for effector T cells with antitumoral activity to be present within the tumor, which is not universal across all cancer types. Future advancements in modulating T cell activity and proliferation are anticipated to expand the therapeutic landscape.
CD4+ T cell help in cancer immunotherapy
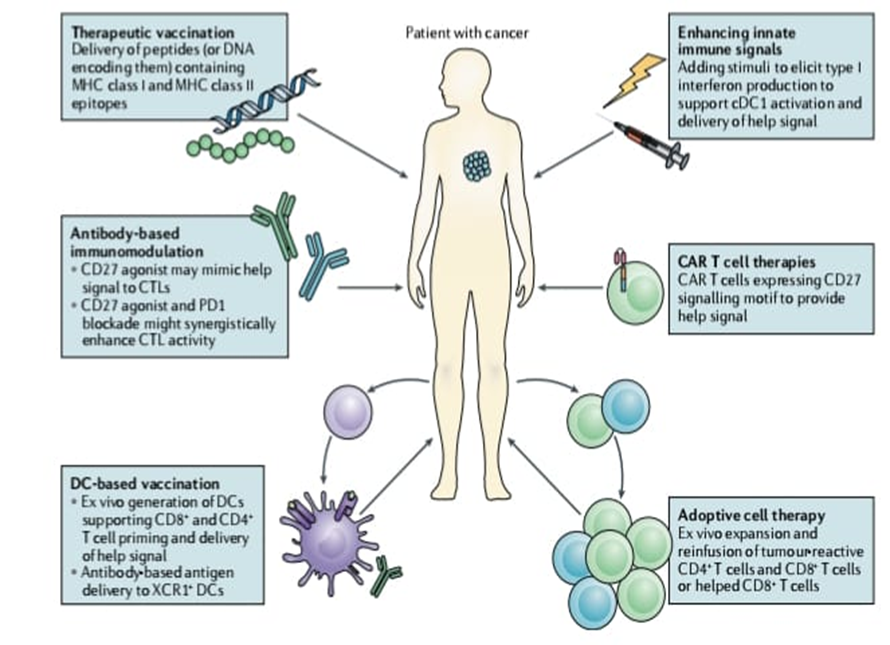
Enhancing CD4+ T cell assistance can improve cytotoxic T lymphocyte (CTL) responses for cancer immunotherapy. Strategies for improving cancer immunotherapy can involve enhancing CD4+ T cell activation or its effector functions. 29Therapeutic vaccines, whether peptide-, DNA-, or mRNA-based, should include both MHC class I and class II epitopes to stimulate CD4+ T cells. Alternatively, CD4+ T cell help can be mimicked by agonistic CD27 antibodies, potentially augmenting PD1 blockade in treating tumor-induced immune suppression. 30For DC-based vaccination, it is crucial to utilize DC subsets that prime CD4+ T cells and convey help signals to CTLs, or to direct antigens and activation signals to XCR1+ DCs via antibody conjugates. Adoptive cell therapy can be improved by including CD4+ T cells for tumor site assistance or by using pre-programmed CD8+ T cells that have received help signals during expansion. CAR T cell therapies could incorporate motifs that mimic help delivery through co-stimulatory receptor signaling. Treatments that induce a type I interferon response, such as STING agonists or radiation, may promote cDC1 activation and their engagement with CD4+ T cells. Cancer immunotherapy, a growing treatment modality alongside surgery, radiotherapy, and chemotherapy, aims to enhance tumor-specific T cell responses. Tumors are often poorly immunogenic, and the tumor microenvironment (TME) suppresses T cell activity. 31While CD8+ cytotoxic T lymphocytes (CTLs) are primary effectors, CD4+ T cells are also vital for effective anti-tumor immunity, aiding in T cell priming, effector function, and memory. Immunotherapies, such as immune checkpoint inhibitors targeting CTLA4 and PD1, promote anti-tumor CTL responses by overcoming negative regulation, though they can also trigger autoimmunity.32 CD4+ T cells play a critical role in optimizing anti-tumor immunity by assisting dendritic cells in antigen presentation and providing necessary co-stimulatory signals to CD8+ T cells, thereby promoting their expansion and differentiation into effective effector or memory cells.
33Immune checkpoint drugs targeting CTLA4 and PD1 enhance anti-tumor T cell responses through distinct, not fully elucidated, mechanisms. While these therapies can overcome T cell regulation, they risk inducing autoimmunity by activating self-antigen-specific T cells. CD4+ helper T cells play a crucial role in bolstering T cell priming, effector, and memory functions, offering a pathway to augment anti-tumor immunity while mitigating adverse autoimmune effects.
The goals of cancer immunotherapy are to prime tumor-specific CTLs in lymphoid organs, increase cytotoxic T lymphocyte (CTL) activity within tumors, and create long-lasting anti-tumor immunity. 34To maximize the size and caliber of the CTL response, CD4+ T cells use certain dendritic cells to send vital "help" signals to CD8+ T cells during the priming phase. The cellular dynamics, membrane receptors that aid CD4+ T cells, and the molecular processes that enhance CTL anti-tumor activity are the main topics of this review. 35It talks about how CTL responses are reduced by inadequate CD4+ T cell assistance and how optimizing this assistance can enhance the results of cancer immunotherapy.
NK CELL :
Natural killer (NK) cells are vital for tumor immunosurveillance, capable of rapidly recognizing and lysing malignant cells via cytotoxic granules and modulating adaptive immunity through cytokine production.36 NK cell-based immunotherapies have been investigated for decades with established safety, leading to the development of "off-the-shelf" therapies. Challenges such as limited ex vivo expansion, in vivo persistence, tumor infiltration, and immune evasion are being addressed through strategies like cytokine pre-conditioning and CAR-NK engineering, driving a significant increase in NK-based cancer immunotherapy research and clinical trials.37 Natural Killer (NK) cells, critical cytotoxic lymphocytes, defend against virus-infected and transformed cells. Their activity, regulated by surface receptors interacting with target cell ligands, can be enhanced by cytokines (IL-15, IL-2) and antibodies that block inhibitory receptors (KIR, NKG2A, TIGIT) or activate receptors (CD137, NKG2D, CD16). These methods boost NK-cell mediated antibody-dependent cellular cytotoxicity (ADCC) against antibody-coated tumor cells, supporting combinatorial immunotherapy in cancer.
Numerous clinical trials are investigating NK cell-based immunotherapies for solid tumors. These include trials evaluating human HLA-haploidentical hematopoietic cell transplantation followed by donor NK cell infusion for high-risk solid tumors like Ewing Sarcoma and Neuroblastoma.38 Other trials focus on tumor-targeting CAR-NK cells, such as HER2-specific CAR-NK cells for HER2-expressing solid tumors, ROBO1-specific CAR-NK cells for various solid tumors, and MUC1-specific CAR-pNK cells for MUC1-positive solid tumors, which have shown a good safety profile and preliminary efficacy. Additionally, trials are exploring NK cell combinations with other treatments, such as nimotuzumab for late-stage malignancies and NK cell infusion following multi-line therapies for advanced malignant tumors.
An outline of the biology of NK cells: classification, growth, and memory.
Natural Killer (NK) cells are part of the innate lymphoid cell family, identifiable in human peripheral blood, bone marrow, and tissues by the absence of TCR and CD3 molecules, and the presence of CD56.39 Natural cytotoxicity triggering receptor 1 (NCR1, also known as NKp46 or CD335) specifically identifies NK cells. These cells originate from CD34+ hematopoietic progenitors in the bone marrow, maturing in lymphoid organs without thymic involvement. NK cells exhibit homeostatic maintenance in the periphery and have a turnover of approximately two weeks, with a doubling time of about 13.5 days. In vitro, adult peripheral blood NK cells undergo senescence after around 16 population doublings, a limit reducible by telomerase reverse transcriptase (TERT) overexpression, indicating telomere shortening as a lifespan determinant.
40Historically, NK cell responses were considered non-amplifying. However, evidence suggests NK cells can develop "memory-like" features, leading to enhanced functional activity and recall responses upon repeated exposure to targets, as observed in responses to cytomegalovirus (CMV) in mice, macaques, and humans. CMV infection in humans can increase NK cells expressing NKG2C, an activating receptor capable of recognizing polymorphic CMV peptides.
NK cells in cancer immunosurveillance
Natural Killer (NK) cells are innate lymphocytes vital for early defense against virus-infected and transformed cells.41 Their activation is mediated by germ-line encoded surface receptors that recognize ligands, leading to the secretion of cytotoxic mediators like granzyme B and perforin, as well as pro-inflammatory cytokines such as IFNg and TNFa. Mature NK cells possess inhibitory receptors for self-HLA class I molecules to prevent attacks on healthy cells. These cells also interact with dendritic cells, macrophages, and T cells, contributing to anti-tumor adaptive immune responses. 42NK cell immunosurveillance has been documented in tumor models and epidemiologic studies, with low NK cell activity linked to increased cancer risk. Despite challenges with homing and immunosuppressive microenvironments in established solid tumors, increased intra-tumoral NK cell numbers often correlate with good prognosis and anti-metastatic effects in various carcinomas, underscoring their role in immunosurveillance. 43Natural killer (NK) cells play a crucial role in cancer immunosurveillance by identifying and eliminating cancerous cells. Their ability to detect cells lacking major histocompatibility complex (MHC) class I molecules, a common evasion strategy used by tumors, positions them as critical effectors in the early detection and control of cancer. 44NK cells employ various mechanisms, including the release of cytotoxic granules (perforin and granzymes) and the induction of apoptosis, to directly kill malignant cells. Furthermore, NK cells contribute to anti-tumor immunity through the secretion of cytokines, such as interferon-gamma (IFN-γ), which can modulate the activity of other immune cells and enhance anti-tumor responses.
Infusions of NK cells in the clinical
45Clinical trials evaluating NK cell infusions in patients with hematological malignancies and solid tumors. An early study by Miller et al. demonstrated that haploidentical peripheral blood mononuclear cells (PBMCs) enriched in NK cells, following T cell depletion and a short culture with IL-2, achieved complete remission in 5 of 19 patients with poor-prognosis Acute Myeloid Leukemia (AML). This response was linked to in vivo NK cell expansion, and no graft-versus-host disease (GVHD) was observed. 46A subsequent report from the same group indicated responses in 17 out of 57 patients. Those who received Flu/Cy combined with IL-2–diphtheria toxin fusion protein (to deplete regulatory T cells, Treg cells) exhibited more frequent NK cell expansion and elevated IL-15 serum levels compared to patients treated with Flu/Cy alone. 47This resulted in complete remission rates of 53% versus 21% and 6-month disease-free survival of 33% versus 5%. The interpretation of these findings is tempered by the fact that the Treg cell-depleted group received a higher number of NK cells. The promising early outcomes by Miller et al.48 spurred the application of allogeneic NK cells in AML or myelodysplastic syndrome, administered either unactivated or activated with cytokines such as IL-2, IL-12, IL-15, and IL-18. Some studies reported therapeutic responses in approximately one-third to one-half of patients, whereas other investigations yielded unclear results regarding NK cell efficacy. Beyond potential differences in cell product potency, patient factors like characteristics and disease status significantly influence response. For instance, two AML patients treated upon molecular relapse achieved remissions lasting 4 and 9 months, contrasting with only one response among five patients treated at the stage of overt disease.
49Administration of anti-GD2 antibodies, in conjunction with Natural Killer (NK) cells to augment Antibody-Dependent Cell-mediated Cytotoxicity (ADCC), has resulted in partial or complete responses in approximately 40% of neuroblastoma patients. No correlation between patient response and KIR/HLA genotype or FCGR3A polymorphisms was observed. In a separate trial, haploidentical NK cells were administered to enhance rituximab-mediated ADCC in patients with refractory Non-Hodgkin Lymphoma (NHL), yielding four objective responses in 14 evaluable patients, including two complete responses that persisted for 3 and 9 months.
CONCLUSION
The field of NK cell-based cancer immunotherapy is advancing rapidly, with methods employing cytokines and surface receptors to enhance NK cell anti-tumor responses showing promise. However, discrepancies between human and mouse NK cell biology, along with emerging clinical trial data, necessitate further research into the impact of various molecular tools on human NK cells. Cancer immunotherapy, building on decades of research, has become a significant modality, with T cell-focused treatments leading the way. Further enhancements may arise from research into T cells, antigen-presenting cells (APCs), and natural killer (NK) cells. Immunotherapies such as checkpoint blockade, adoptive T cell transfer, and cancer vaccines have demonstrated superior efficacy over chemotherapy in difficult tumors, generally with better tolerability, despite common immune-related adverse effects. The expansion of indications and the identification of new drug targets highlight the crucial connection between basic research and clinical application in cancer treatment.
REFERENCES

Pramod Chikkodi, Suhani Jadhav, Aniket Pawar, T Cell and NK Cell Immune-Checkpoints from Clinical Practices for Cancer Immunotherapy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1407-1418. https://doi.org/10.5281/zenodo.17112735
 10.5281/zenodo.17112735
10.5281/zenodo.17112735
