P. R. Pote Patil College of Pharmacy, Amravati, Maharashtra, 444604
Dermatology is the branch of medicine that focuses on the care of the skin, hair, nails, and mucous membranes. Its roots trace back to ancient civilizations, where natural remedies and traditional practices were used to treat various skin conditions. Over time, dermatology has evolved into a modern medical specialty, shaped by pioneers such as Robert Willan, known as the Father of Dermatology, and Prof. B.N. Banerjee, regarded as the Father of Modern Dermatology in India. Today, dermatology is not only important for maintaining appearance but also plays a critical role in detecting serious conditions like skin cancer and systemic diseases. The integration of modern technologies, including advanced imaging tools, artificial intelligence, lasers, and teledermatology, has made skin care more effective, precise, and accessible. Overall, dermatology significantly contributes to improving health, confidence, and quality of life worldwide.
Dermatology is the branch of medicine dealing with the skin. It is a specialty with both medical and surgical aspects. A dermatologist is a specialist medical doctor who has undergone advanced training (typically 4 years beyond medical school) and manages diseases related to skin. Dermatological conditions, including inflammatory diseases, infections, cancers, hair loss, and cosmetic issues are common in the population, and sometimes difficult to diagnose or treat, requiring the services of a dermatologist. Dermatological interventions include systemic and topical medications, surgery, radiation, and physical modalities such as cryosurgery or laser therapy. Dermatology is the medical discipline that is concerned with the diagnosis and treatment of diseases of the skin, hair, and nails in both children and adults. Specialists in dermatology are called dermatologists. Dermatology involves but is not limited to study, research, and diagnosis of normal and disorders, diseases, cancers, cosmetic and ageing conditions of the skin, fat, hair, nails and oral and genital membranes, and the management of these by different investigations and therapies, including but not limited to dermato histopathology, topical and systemic medications, dermatologic surgery and dermatologic cosmetic surgery, immunotherapy, phototherapy, laser therapy, radiotherapy and photodynamic therapy.”[1][2][6]
Dermatology provides a unique clinical perspective on the practice of skin toxicology and, in this role, is primarily concerned with the pathological consequences of cutaneous or systemic exposures to xenobiotics acquired under a wide variety of circumstances. Empirically, the dermatologist is responsible for identifying cutaneous manifestations of toxicity (diagnosis) and formulating an effective treatment strategy (including recommendations for preventative measures to avoid re-exposure).[3][5]
Dermatology is the branch of medicine concerned with the diagnosis and treatment of skin disorders. At least 2000 different cutaneous disorders are known to the dermatologist. Skin conditions show diversity in appearance and severity, ranging from cosmetic problems like dry skin and wrinkles to life-threatening conditions like toxic epidermal necrolysis. The practice of dermatology varies throughout the world. In the United Kingdom patients are normally seen by a primary care physician. If the primary care physician is unable to deal with the problem the patient is referred on to a hospital consultant. Around one in seven primary care consultations relate to a dermatological problem. About 12.5 per 1000 of the population are referred to a hospital dermatology department annually, which places dermatology among the highest volume specialties in terms of patient numbers. The integument is a multifunctional interface between the human body and the environment. A wide variety of environmental hazards like chemicals, plants, animals, parasites, microorganisms, radiation and climatic conditions can adversely affect the skin.[7][8]
History of Dermatology-
Dermatology, the branch of medicine focused on skin, hair and nails, has a rich history dating back to ancient civilizations. The history of Dermatology concerns the development of the practice of researching , defining and treating skin diseases, from ancient times to the present. The field has its origin in the earliest forms of medicine, later becoming a distinct field with its own specialized practitioners and researchers.[1]
The Father of dermatology is generally considered to Robert Willian. He is recognized for his systematic classification and description of skin diseases, laying the groundwork of the field as it is known today. Professor B. N. Banerjee is considered the "Father of modern dermatology in India". He was the first president of the Indian Association of Dermatologists, Venereologists and Leprologists (IADVL).[2]
The study of skin, the science of dermatology, has undergone significant transformations throughout the centuries. From the first descriptions of skin diseases in Egyptian papyri and in Hippocratic writings to the first treatises on dermatology, important individuals and discoveries have marked the specialty. In the 18th and 19th centuries, the specialty consolidated itself as a field of medical study based on the first classifications of dermatoses, diagnostic methods, and drug treatments. In the 20th century, the scientific and technological revolution transformed dermatological practice, incorporating new therapeutic resources, as well as surgical and aesthetic procedures. In the face of such a vigorous process, it is important to provide a historical synthesis for the medical community to recognize and understand the origins that supported one of the most relevant specialties in the current medical scenario.[5]
Skin diseases have been known to mankind since its origin, considering that the essentially visual component of these conditions allowed their early recognition. The first records of cutaneous nosology date back to ancient history, when they were described by the great civilizations that shaped Western medicine.From the Egyptian papyrus emerges the first skin hygiene measures, the handling of wounds, and the use of medicinal plants. From the postulates of Hippocrates, the father of medicine, physical inspection and clinical reasoning are established as pillars of medical diagnosis. Romans, Arabs, and Byzantines protected and contributed to the development of medicine for centuries, with marked advances in the light of the Renaissance and the Illuminism.[2][5]
Early History and Ancient Civilization: -
Ancient Egypt –
Western medicine had its origins marked by two great ancient civilizations: Egyptian and Greek. Medical practice in Egypt was closely related to religion; priests provided medical care in religious temples, and diseases were attributed to the will of the gods. The manifestations of diseases and medical treatments were recorded on papyrus, a precursor of paper, in which clinical signs, diagnoses, plants, and therapeutic formulations were described.[9]
Skin diseases are mentioned in several texts, especially in the Edwin Smith (1600 BC) and Ebers (1550 BC) papyri . The Edwin Smith papyrus, also known as Book of Wounds, has been recognized as one of the main medical texts of ancient Egypt, consisting of 48 cases of cutaneous injuries and wounds, many of which occurred during battles and accidents in Egyptian construction sites. This papyrus also addressed other medical fields such as general practice, gynaecology, paediatrics, and even cometary, mentioning rejuvenating prescriptions for skin.[10]
The Egyptians are credited with the rudimentary use of phototherapy, from the ingestion of the Ammi majus L. plant, found in the Nile delta, composed of methoxalene, a substance in the group of psoralens that acted as a natural photosensitizer. The use of this plant followed by sun exposure was included in the prescriptions of the Ebers papyrus, being recommended for repigmentation.[9][10]
Ancient India-
Dermatology, the science of the skin and its appendages, is one of the many specialties that evolved from general internal medicine during the course of the nineteenth century. Till this time, physicians with few exceptions, were little concerned with the skin, apart from the exanthematic eruptions of acute fevers. During the last decades of that century, contributions of some, such as Heberden, Cullen, and Hebra, laid the foundations on which the pioneer specialist dermatologists of the following century were able to build. In India, dermatology as a specialty came into prominence only in the twentieth century, although skin diseases like leprosy, viral fevers like measles and chicken pox (amma), psoriasis, and vitiligo (ven kushtam or white leprosy) were recognized long back. Major strides in the etiology, pathogenesis, and treatment of skin disorders took place during the twenty first century. Today, dermatology is a well-developed specialty with established departments in various medical colleges and hospitals. Growing numbers of dermatologist render their services to the general population throughout the country and many have specialized into various subspecialties like paediatric dermatology, dermatosurgery and cosmetic dermatology, and dermatopathology. Contributions to the world dermatology by many Indian doctors are applaudable, although some lacunae still remain.[11][12]
In India, therapeutics of dermatoses were known and practiced by our ancient physicians for centuries, Charaka Samhita contains one chapter on the subject. This is a famous ancient medical treatise dealing with basic principles of Ayurveda, one of the four vedas dealing with the knowledge of health. In this ancient book, worshipful Atreya Punarvasu has described eighteen dermatoses and attributed them to the preponderance of morbid humours (vata, pitta, and Kapha) causing disturbance of body elements resulting in diseases. Knowledge of infections and allergens, etc. did not exist in those days. In the absence of specific remedies, therapies used were mostly empherical and often unsatisfactory.[11][12]
Ayurvedic dermatology was later influenced by the Unani system imported into the country with the invasion by Muslims. Concoctions, Karhars, and blood purifiers were chiefly resorted to. Both the Ayurvedic and the Unani systems were practiced side-by-side, along with the barbers (Jarahs, in local language). While the former two relied mainly on purification of blood, the barbers mainly laid emphasis on cauterization of skin lesions and burning out the disease with its root. Their cheapness and easy accessibility attracted the ignorant and the illiterate, but less so the educated.[13]
Modern dermatology was introduced in India by the British, so the growth of Indian dermatology took place much earlier when compared to the rest of the Asian countries. And since then, many great contributions have been made by Indian doctors in the field of dermatology.[14]
The Vedic period: Historical material about skin and its diseases are available in the Rigveda, the earliest texts of Indo-Iranian Aryans. The various Ayurvedic texts detailed not only about diseases but also about the daily care of the normal skin such as oil massage, trimming and care of hair, beards and nails, as well as the use of perfumes and toiletries. In Charaka Samhita, the concept of anatomical structure including various layers of the skin has been mentioned, which says that the skin formed the outer boundary of the body, is composed of six layers, and is also the reside of touch sensation. Among the various diseases of the skin, dialogues on leprosy, vitiligo, cellulitis, smallpox, acne, melasma, fungal infections, etc., are quite fascinating.
In Sushruta Samhita, which deals with the surgical aspect of disease management, approximately 121 surgical instruments and more than 300 procedures are mentioned, which included different types of incision and drainage procedures of abscesses and infected wounds, various types of cauterization, and dermabrasion. The term Kustha was probably used to represent a number of skin ailments along with leprosy of the modern sense. The classification of Kustha into seven types in the Charaka Samhita and 18 types (seven Mahakustha and 11 Kshudrakustha) in the Sushruta Samhita represents the astute observation of the ancient Indian physicians.
Later on, the Siddha system came and skin diseases were grouped under the term Kuttam. There are ample discussion on various skin ailments such as thinvup-pun (urticaria), paru (acne), and sarumap-pun (dermatitis).
Coming to modern dermatology, the major contributions from India can be discussed under dermatology, venereology, and leprology.[14]
Ancient Greece-
In ancient Greece, Medicine and the art of healing were also attributed to divine entities. According to Greek mythology, Aesculapius was the god of medicine, and there were many temples dedicated to his worship on several Greek islands. In these temples, groups of priests called asclepiads treated diseases using medicinal plants, and even dog licking was used for the treatment of wounds.[15]
From the Greek island of Cos emerged one of the greatest exponents of Greek and Western medicine, the physician and professor Hippocrates (460–370 BC). Moving away from the metaphysical understanding of the health-disease process, Hippocrates contributed immensely to the rationalization of the clinical method, emphasizing clinical observation as an important resource for the diagnosis of diseases, thus becoming known worldwide as the father of modern medicine. In dermatology, a specialty in which observation is an essential attribute, the hippocratic contributions are also noteworthy. Hippocrates proposed the first classification of skin diseases, dividing dermatoses into two classes: idiopathic diseases, which originate primarily from the skin, and exanthematic diseases (rashes), cutaneous manifestations of systemic diseases caused by imbalances in body humors.[15][16]
Ancient Roman Empire-
In ancient Rome, hygiene and skin care occupied a relevant space in social life. Roman baths or public baths were intended for social gatherings and health care, in which the Romans bathed in pools of warm and cold waters, which were believed to have medicinal properties; they also cleaned the skin using instruments such as the strigil, a curved blade used for scraping. During bathing sessions, in addition to skin cleansing, body oils were applied in order to mitigate itchy disorders and moisturize the skin.
Like the Egyptians, Romans believed that organs and diseases were associated with their gods, assigning each god a specific pathology. Under this logic, they attributed each disease to a specific doctor; therefore, some dedicated themselves to the treatment of hernias, eyes, ears, and skin, and the latter were responsible for the prescription of medicinal baths.
Despite the medical-religious approach, the process of applying science to Roman medicine began at the height of the Roman Empire. In this context, the contributions of Aurelius Cornelius Celsus (25 BC–50 AD) stand out. In his work De Medicina, a medical encyclopedia, Celsus dedicated an entire chapter to skin diseases, describing approximately 40 treatments for dermatological conditions. The first descriptions of various skin lesions are attributed to Celsus, among them acrochordons, molluscum contagiosum, and kerion celsi, crusts on the scalp of children similar to honeycombs. In Greek, kerion means honeycomb, equivalent to the Latin term favus.
Mesopotamia-
Readily visible alterations of the skin surface have been recognised since the dawn of history. Among the first to take an interest in skin diseases were the Mesopotamian peoples, who sought to understand the reasons for these problems, often resorting to explanations rooted in religion, astrology and divination, and were the first to observe and define various dermatopathies. Skin conditions were considered a sign of divine punishment, the actions of demons and spirits, or as the result of black magic. One of the most influential sources of understanding views on skin conditions in Mesopotamia comes from the Babylonian chief scholar Esagil-kin-aplim, who wrote a diagnostic manual called Sakikk?. One passage describes a complex skin condition which is associated with a sexual encounter. Another work, Alandimmû, observes the human physical appearance, with a section dedicated to dermal marks, such as moles, and spots. While matching the descriptions of diseases in the few surviving cuneiform medical texts to specific ailments is challenging, it appears likely that Babylonians and Assyrians were the first to define and describe warts, pustules and scabies in writing. It is also possible to draw some conclusions about their attitude to skin conditions. Doctors of the era clearly sought to define disease according to certain criteria, using observations such as such as heat, smell, breath and bodily fluids, to help draw a diagnostic conclusion.[25][26]
Significance of Dermatology-
Dermatology is the branch of medicine focused on the study, diagnosis and treatment of conditions related to the skin, hair, nails and mucous membranes. It plays a crucial role in identifying underlying health conditions through the observation of skin changes and works collaboratively with other healthcare professionals for comprehensive treatment.[1]
In India, dermatology began to gain importance as a medical specialty only in the 20th century, even though skin conditions such as leprosy, measles, chickenpox (locally known as amma), psoriasis, and vitiligo (referred to as ven kushtam or white leprosy) were known to people since ancient times. It was during the 21st century that significant progress was made in understanding the causes, development, and treatment of skin diseases. Today, dermatology is a well-established field, with dedicated departments in many medical colleges and hospitals. A growing number of dermatologists are actively serving communities across the country, and many have gone on to specialize in areas like pediatric dermatology, dermatosurgery, cosmetic dermatology, and dermatopathology. Indian dermatologists have made noteworthy contributions to global dermatology, though some gaps and challenges still remain.[2]
Comprehensive dermatology services are crucial for diagnosing and treating skin conditions and promoting overall health. They address various issues like acne, eczema, skin cancer, etc, while also detecting underlying health conditions. With a wide range of treatments and procedures, they play a vital role in enhancing skin health and well-being.[1]
A Holistic Approach to Skin Health.
A holistic approach to skin health considers internal and external factors. Skin specialists address underlying health conditions, stress, and lack of sleep, offering treatments that promote healthy and glowing skin.
Early Detection and Prevention of Skin Cancer.
Yearly skin screenings aid in the early detection of melanoma, improving prognosis. Complete skin screenings annually for those above 40 and every three years for individuals aged 20-39 to help diagnose and prevent skin cancer.[28]
Individualised Treatment Options.
Individualised treatment is crucial for each skin condition. By identifying the root cause, determining the appropriate medication dosage, and tailoring the treatment to the patient's needs, effective management of their skin condition can be achieved.
Expertise and Specialized Knowledge.
Dermatology specialisations include dermatopathology, paediatric dermatology, Mohs surgery for skin cancer, and cosmetic dermatology. These areas of expertise enable skin specialist doctors to study skin diseases in adults and children, understand their causes and effects, and provide suitable treatments.[28]
Ancient Practices in Dermatology-
In Charaka Samhita, the concept of anatomical structure including various layers of the skin has been mentioned, which says that the skin formed the outer boundary of the body, is composed of six layers, and is also the residence of touch sensation. Among the various diseases of the skin, dialogues on leprosy, vitiligo, cellulitis, smallpox, acne, melasma, fungal infections, etc., are quite fascinating.[14]
In Sushruta Samhita, which deals with the surgical aspect of disease management, approximately 121 surgical instruments and more than 300 procedures are mentioned, which included different types of incision and drainage procedures of abscesses and infected wounds, various types of cauterization, and dermabrasion.
The term Kustha was probably used to represent a number of skin ailments along with leprosy of the modern sense. The classification of Kustha into seven types in the Charaka Samhita and 18 types (seven Mahakustha and 11 Kshudrakustha) in the Sushruta Samhita represents the astute observation of the ancient Indian physicians. Later on, the Siddha system came and skin diseases were grouped under the term Kuttam. There are ample discussion on various skin ailments such as thinvup-pun (urticaria), paru (acne), and sarumap-pun (dermatitis).
In ancient India, skin diseases (dermatoses) were treated by traditional doctors for many centuries. A well-known Ayurvedic text called the Charaka Samhita has an entire chapter on skin problems. Ayurveda, one of India’s oldest systems of medicine, explains that skin diseases happen when the body’s natural elements (called vata, pitta, and kapha) go out of balance. These ancient doctors did not know about infections or allergies, so their treatments were based on observation and experience, and often didn’t work very well.
Later, when Muslims came to India, they brought the Unani system of medicine, which also influenced Ayurvedic skin treatments. Both systems used herbal mixtures, drinks (called karhars), and blood-purifying methods to treat skin issues. Along with them, local barbers (called jarahs) also treated skin conditions. They mainly used methods like burning or cauterizing skin problems to try to remove them from the root. Because barber treatments were cheap and easy to access, uneducated or poor people often went to them, while educated people preferred the more formal Ayurvedic or Unani. [13][14]
Significance of Dermatology in United States-
In addition to improving quality of life, the skills to diagnose and treat skin disease can also allow critical early recognition and treatment of life-threatening systemic diseases such as HIV. Because dermatology is less prioritized for allocation of resources, there is a smaller amount of funding available to support clinical care, education, research, and development of the field globally. Important questions in dermatology globally remain unanswered, and important work goes unrecognized because of barriers for publishing in major journals. In this issue of Dermatologic Clinics, we have taken the opportunity to highlight a number of important issues in global health dermatology from a range of author groups representing diverse regions across the globe. We feature key topics in global dermatology that are lacking in the literature as well as notable examples of programs that will provide many key learning points. These topics include regional skin disease, telemedicine, dermatology education, tools for dermatologic care, and neglected populations. Skin diseases can have significant regional variation due to infectious diseases, genetics, culture, environmental considerations, and many other factors.
Dermatology holds a vital place within the healthcare system of the United States, addressing not only aesthetic concerns but also playing a critical role in diagnosing, managing, and treating a wide range of medical conditions that affect the skin, hair, and nails. As the largest organ of the body, the skin serves as a window to overall health, and dermatologists are often the first to detect signs of systemic diseases, infections, and malignancies.[32]
1. High Prevalence of Skin Disorders.
Skin conditions are among the most common health problems in the U.S., affecting nearly one in three Americans annually. Common disorders such as acne, eczema, psoriasis, rosacea, fungal infections, and dermatitis lead to significant physical discomfort, emotional distress, and diminished quality of life. The Global Burden of Disease Study has consistently ranked skin diseases among the top causes of nonfatal disease burden in the United States.
2. Early Detection of Life-Threatening Diseases.
Dermatologists play a crucial role in the early diagnosis of skin cancer, especially melanoma, which is one of the most aggressive forms of cancer. In the U.S., skin cancer is the most common form of cancer, with over 5 million cases diagnosed each year. Regular skin screenings and biopsies conducted by dermatologists are essential for early intervention and improving survival rates.
Additionally, many internal diseases manifest on the skin before showing signs elsewhere. Dermatologists often detect conditions such as lupus, diabetes, liver disease, and HIV/AIDS based on skin symptoms, enabling early management and referral to appropriate specialties.
3. Advancement in Medical Technology and Research.
The U.S. is a global leader in dermatological research and innovation. American dermatologists contribute significantly to clinical trials, drug development, and technological advances, including laser therapies, biologics, phototherapy, and artificial intelligence (AI)-based diagnostics. The integration of teledermatology has also expanded access to dermatologic care, especially in rural and underserved areas.
4. Role in Preventive Care and Education.
Dermatologists actively engage in preventive healthcare, particularly by educating the public on sun safety, skin cancer prevention, and the risks of tanning beds. Public health campaigns led by organizations like the American Academy of Dermatology (AAD) have helped raise awareness and reduce the incidence of preventable skin damage and malignancies.
5. Contribution to Global and Public Health.
Beyond individual patient care, dermatologists in the U.S. contribute to global health by participating in initiatives targeting neglected tropical diseases like leprosy, scabies, and cutaneous leishmaniasis. Domestically, dermatology supports public health through screening programs, community clinics, and outreach in underserved populations.[32]
Significance of Dermatology in Thailand-
A. Addressing Unique Skin Care Needs.
One of the key factors contributing to the popularity of dermatological care in Thailand among Middle Eastern tourists is the ability to provide personalized solutions for different skin types. Thai dermatologists are well-versed in addressing the specific skin care needs of individuals from various ethnic backgrounds, including Middle Easterners.
a. Specialized Care for Middle Eastern Skin.
Middle Eastern skin often requires specialized care due to its unique characteristics, such as higher melanin levels and increased susceptibility to conditions like melasma. Thai dermatologists are skilled in customizing treatment plans that address these concerns effectively.
B. The Role of Advanced Technology:
a. Cutting-Edge Technology and Treatments.
Another compelling reason Middle Eastern tourists flock to Thailand for skincare is the access to cutting-edge technology and treatments. Thai skincare clinics and hospitals invest in state-of-the-art equipment and techniques, ensuring that patients receive the latest and most advanced skincare procedures available.
b. Innovative Procedures Available.
For example, laser therapies, fractional rejuvenation, and non-surgical facelifts using radiofrequency are among the innovative treatments that are readily available. These advanced procedures provide Middle Eastern patients with non-invasive options to achieve the flawless skin they desire, often with minimal downtime.
C. Cultural Understanding and Communication:
a. Cultural Sensitivity in Dermatological Care.
Cultural sensitivity plays a significant role in attracting Middle Easterners to Thailand for skincare treatments. Dermatologists and skin care professionals in Thailand are trained to understand and respect the cultural norms and values of their patients, which creates a more comfortable and welcoming environment.
b. Effective Language Communication.
Language is rarely a barrier in Thailand, as many healthcare professionals are proficient in English and often other languages, making communication smooth and effective. This factor contributes to the overall positive experience of Middle Eastern tourists seeking skincare services in the country.[33]
Key Technologies and Their Applications in Dermatology-
Dermascopy :-
Dermoscopic imaging is commonly used for a wide range of conditions, with the most frequent application being identification of skin cancers. Dermoscopy has a high sensitivity for skin cancer, leading to improved biopsy efficiency.
Furthermore, clinicians can identify thinner melanomas with dermoscopy than with clinical examination alone.25 Multiple algorithms, such as the 2-step algorithm, ABCD rule, 7-point checklist, Menzies’ method, CASH algorithm, chaos and clues algorithm, and triage amalgamated dermoscopy algorithm, aid in the identification of common dermoscopic lesions.25-29 Wohlner et al provides a comprehensive review of dermoscopic features of skin cancer.[35][36]
Reflectance Confocal Microscopy (RCM) :-
RCM can improve diagnosis of basal cell carcinomas (BCCs), which appear as bright tumor islands with elongated cord-like structures and dark cleft-like spaces on RCM. Furthermore, validated BCC features distinguishable by RCM have been proposed to differentiate BCC tumor subtypes. Keratinocyte malignancies (actinic keratoses, squamous cell carcinoma [SCC] in situ, and SCC) can be challenging to differentiate from each other by RCM, with wide ranges in sensitivities and specificities for these conditions. Classic features of SCC include irregular epidermal honeycomb pattern with round bright nuclei in the epidermis (pagetoid spread) and looping vessels in the papillary dermis.[36][37]
RCM imaging of melanoma can be performed in vivo and ex vivo. In vivo, classic features include disorganized pattern, focal loss of dermal-epidermal junction, bright round or dendritic cells (pagetoid spread), and irregularly shaped dermal nests. RCM has a much higher sensitivity than dermoscopy (84% and 39%, respectively), particularlywhen examining hypopigmented or amelanotic melanoma. RCM imaging ex vivo involves using melanin as the chromophore. Clinicians can use RCM, typically either handheld or mosaic RCM, to diagnose lentigo maligna and lentigo maligna melanoma. RCM can be used to determine pre-operative tumor margins for melanocytic and nonmelanoma tumors. RCM visualizes invasion and superficial recurrence and monitors therapeutic interventions for skin cancers. [36][37][38]
Optical Coherence Tomography(OTC):-
OCT has been widely applied to dermatologic conditions. OCT can be used to visualize melanomas and NMSCs for diagnosis and tumor margin delineation. In addition to assessing benignity, OCT can monitor disease progression for inflammatory, infectious, blistering, and vascular lesions; wound healing; and chronologic photoaging. Skin photo scatter permits a penetration depth of ~1.5 mm (level of reticular dermis). OCT cannot be used to distinguish individual cells, which limits its diagnostic capabilities. Anatomic structures, such as scars, can impede visualization of underlying or adjacent features. Advanced training is needed for image interpretation, which remains subjective. OCT devices are expensive.[40][41]
Of all the technologies discussed, OCT appears to be the one most frequently combined with other techniques. The combination multiphoton tomography (MPT)-OCT device allows visualization of cellular details with MPT and morphology with OCT. Because MPT provides a microscopic image and OCT the macroscopic context, it can be challenging to accurately correlate images. OCT has also been combined with RCM to identify NMSC borders (Fig 1). This handheld device provides a 3D image by obtaining cross-sectional OCT and en face RCM images.[42][43]
Teledermatology can be carried out in three technological modalities: store and forward method, real-time videoconferencing and a hybrid of the above. The store and forward method is the most widely used one. It involves taking pictures and making videos which are then assessed by a dermatologist in a different time and place. No interaction between the patient and the physician is needed, what makes this method relatively inexpensive. It is particularly suited for patients with poor access to health care as there is no need for coordinating scheduled visits. It might be used across different time zones and it interferes less with daily workflow. The method does not depend on Internet connection speed but requires a very high resolution of images. The store and forward method might however require a repeat consultation if clinical data and history are incomplete. Real-time teledermatology is a technology of videoconferencing used for interaction between the patient and the physician. It enables verifying medical history and giving immediate advice. Videoconferencing is also convenient for both the patient and the physician to exchange information and clarify aspects of concern. It may potentially save time due to no need of repeating the same consultation. The method might be expensive because of technical issues and it highly depends on the Internet connection. It requires both the patient and the physician to be available at the same time which is less convenient particularly for practice across time zones and might interfere with physicians’ daily schedules. The hybrid method merges advantages of the aforementioned two: time saving aspects of real-time videoconferencing and quality of digital images . Teledermatology examined from the perspective of health care delivery identifies four practice models: consultative (most commonly used), triage, direct care and follow up. Development in communications technology creates possibilities for the patients to communicate directly with their dermatologists and means that teledermatology has to be structured in a broader spectrum.[45][46][47]
The role of light-based technologies in dermatology has expanded dramatically in recent years. Lasers and intense pulsed light have been used to safely and effectively treat a diverse array of cutaneous conditions, including vascular and pigmented lesions, tattoos, scars, and undesired hair, while also providing extensive therapeutic options for cosmetic rejuvenation and other dermatologic conditions. Dermatologic laser procedures are becoming increasingly popular worldwide, and demand for them has fueled new innovations and clinical applications. These systems continue to evolve and provide enhanced therapeutic outcomes with improved safety profiles.[50]
This review highlights the important roles and varied clinical applications that lasers and intense pulsed light play in the dermat Laser is an acronym, which represents light amplification by the stimulated emission of radiation. An understanding of the fundamental properties of laser light is essential to appreciate its clinical effects on the skin.1,2 First, laser light is monochromatic, meaning that the emitted light is composed of a single wavelength. This is determined by the medium of the laser system through which the light passes. Second, laser light is coherent – traveling in phase spatially and temporally. Third, laser light is collimated – emitted in a parallel manner with minimal divergence.[50]
Laser light may be absorbed, reflected, transmitted, or scattered when applied to the skin. In order for a clinical effect to occur, light must be absorbed by tissue. Absorption of laser light is determined by chromophores – the target molecules found in the skin, which have specific wavelength absorption profiles. The three primary endogenous cutaneous chromophores are water, melanin, and haemoglobin; whereas tattoo ink represents an exogenous chromophore. Upon absorption of laser energy by the skin, photothermal, photochemical, or photomechanical effects may occur. The cutaneous depth of penetration of laser energy is dependent upon absorption and scattering. In the epidermis, there is minimal light scattering, whereas in the dermis there is significant scatter due to the high concentration of collagen fibres. The amount of scattering of laser energy is inversely proportional to the wavelength of light. The depth of laser energy increases with wavelength until the mid-infrared region of the electromagnetic spectrum, at which point dermal penetration becomes more superficial due to increased absorption within tissue water. [51]
The skin, as the largest organ of the human body, serves a fundamental role in forming a protective barrier against environmental threats and safeguarding internal organs . The human skin is home to an extensive and diverse microbiota, comprising not only bacteria but also fungi, viruses, protozoa and mites. Approximately 1000 bacterial species inhabit the skin, with different body regions creating unique ecosystems that support distinct microbial communities. Once thought of primarily as ‘commensal’, recent research has underscored the ‘symbiotic’ role of the skin microbiome in maintaining skin health alterations in the skin microbiome, known as dysbiosis, are implicated in several common skin diseases, including atopic dermatitis, psoriasis and acne. Dysbiosis has not only been observed consistently across various skin disorders but is increasingly recognised as a contributing factor to their pathophysiology . Furthermore, research into the gut–skin axis reveals that dysbiosis in the gut microbiome may also contribute to skin disorders, highlighting a complex interplay between internal and external microbial environments . Therapeutic approaches that aim to restore microbial balance, such as the administration of autologous or allogeneic probiotic bacteria via topical or oral routes, show promise as effective treatments for these conditions . This review examines the role of the skin microbiome and microbiome-based therapies (MBTs) in managing prevalent skin disorders and offers insights into potential directions for future research in this emerging field.[47][48][49]
The skin microbiome is a highly specialised ecosystem that varies significantly across different skin surfaces, influenced by factors such as temperature, pH, humidity, lipid content and other environmental conditions. Actinobacteria represent a substantial portion of the skin microbiota, comprising 51.8% of the microbial population on human skin. Other dominant phyla include Firmicutes, Proteobacteria and Bacteroidetes . Specific bacterial communities are associated with distinct skin regions; for instance, moist areas like the cubital fossa and interdigital spaces on the feet are typically dominated by Corynebacterium and Staphylococcus species, which thrive in humid microenvironments. In contrast, sebaceous regions favour the growth of Propionibacterium due to their ability to flourish in lipid-rich settings . Fungal communities also inhabit the skin, with Malassezia as the predominant fungal genus across most regions, while feet harbour a more diverse array of fungi, including Aspergillus spp., Rhodotorula spp., Cryptococcus spp. and Epicoccum spp., alongside Malassezia species .[47][48]
Factors contributing to Skin Diseases:-
Infectious agents such as bacteria, fungi, and viruses are among the most common causes of skin diseases.
Bacterial Infections (e.g., impetigo, cellulitis) may lead to redness, swelling, pus, and discomfort. They often affect areas with cuts or weakened skin barriers.
Fungal Infections (e.g., tinea, candidiasis) thrive in moist environments, like skin folds, and cause itchiness, redness, and scaling.
Viral Infections (e.g., herpes, warts, molluscum contagiosum) can result in blisters, lumps, or chronic skin lesions.
These infections can occur independently or worsen pre-existing skin conditions, especially in people with weakened immunity or poor hygiene.[52][53][54]
2. Immune System Dysfunction-
A malfunctioning immune system can trigger autoimmune and inflammatory skin diseases.
Autoimmune skin disorders, such as lupus, pemphigus, or scleroderma, happen when the immune system mistakenly attacks healthy skin cells.
Chronic inflammatory conditions like psoriasis and eczema are linked to overactive immune responses that lead to persistent redness, scaling, and itching.
In such cases, the skin becomes a site of immune conflict, leading to visible and sometimes painful symptoms.[55][56][57]
3. Genetic Factors-
Your genes play a significant role in determining your skin’s susceptibility to certain diseases.
Skin disorders like psoriasis, eczema (atopic dermatitis), vitiligo, and alopecia areata often run in families.
Inherited traits can affect how the skin reacts to triggers, how it heals, and how well it functions as a protective barrier.
If one or both parents have a chronic skin condition, the likelihood of developing similar issues increases significantly.[58][59]
4. Environmental Factors-
External elements from our surroundings can act as triggers or aggravators of skin conditions.
Sun exposure: Prolonged UV exposure can damage skin cells, leading to sunburn, premature aging, or skin cancers.
Allergens and irritants: Contact with substances like pollen, chemicals, dust, or harsh soaps can cause reactions like dermatitis or hives.
Pollution and climate: Extreme weather, humidity, and air pollution can compromise skin health and worsen existing problems.
Protecting the skin from harmful environmental exposures is crucial in preventing flare-ups.[60][61]
5. Lifestyle Factors-
Daily habits and routines significantly affect skin health.
Diet: Nutrient deficiencies, excessive sugar or processed foods can promote inflammation and lead to acne, eczema, or dull skin.
Stress: Emotional stress can trigger or worsen conditions like psoriasis, eczema, and acne through hormonal changes.
Hygiene: Poor personal hygiene may allow the build-up of oils, dirt, and microbes, increasing the risk of infections and breakouts. On the other hand, over-washing or using harsh products can damage the skin barrier.
Maintaining a balanced lifestyle with good nutrition, stress management, and proper skincare can go a long way in maintaining healthy skin.[62][63]
Various skin diseases in Dermatology:-
Skin disorders are a significant portion of the global total of diseases, affecting millions of people worldwide. Dermatology is the medical specialty responsible for the study of more than 4,000 diseases of skin and cutaneous adnexae, accounting for 15% to 30% of outpatient medical care in health systems, incorporating a wide arsenal of diagnostic, therapeutic, and aesthetic resources.
Skin diseases have been known to mankind since its origin, considering that the essentially visual component of these conditions allowed their early recognition. The first records of cutaneous nosologies date back to ancient history, when they were described by the great civilizations that shaped Western medicine. From the Egyptian papyrus emerges the first skin hygiene measures, the handling of wounds, and the use of medicinal plants. From the postulates of Hippocrates, the father of medicine, physical inspection and clinical reasoning are established as pillars of medical diagnosis. Romans, Arabs, and Byzantines protected and contributed to the development of medicine for centuries, with marked advances in the light of the Renaissance and the Illuminism.[65][66]
1. Infections (When germs cause skin trouble)-
Infectious dermatoses are among the most common and present across all age groups and geographies. They can be caused by bacteria, fungi, viruses, or parasites/arthropods (e.g., mites).
1.1 Bacterial Skin Infections-
Common examples: Impetigo, cellulitis, folliculitis, ecthyma, erysipelas, furuncle, carbuncle, pyoderma.
Pathogenesis & microbiology-
Most are caused by Staphylococcus aureus, Streptococcus pyogenes (group A streptococcus), or mixed flora. In some cases, Gram-negative organisms may play a role (e.g. in immunocompromised). Infection can be superficial (epidermis) or deeper (dermis, subcutis). Bacteria gain entry via breaks in the skin barrier (trauma, insect bite, fissures).
Once inside, bacterial toxins, enzymes (e.g. hyaluronidases, streptokinase), and host immune response lead to inflammation, abscess formation, spread.
Clinical features-
Diagnosis-
Usually clinical. In atypical or recurrent cases: swab for Gram stain, culture & sensitivity; imaging if deep involvement or abscess suspected.
Management principles-
Complications & special issues-
Recurrent infections, antibiotic resistance, superinfection, post-streptococcal glomerulonephritis (rare), necrotizing fasciitis in severe cases.[66][67]
1.2 Fungal (Mycotic) Skin Infections-
Common examples: Tinea (ringworm) of scalp (tinea capitis), body (tinea corporis), groin (tinea cruris), foot (tinea pedis), onychomycosis; candidiasis (cutaneous or intertriginous).
Pathogenesis & microbiology-
Dermatophytes (e.g. Trichophyton, Microsporum, Epidermophyton) degrade keratin, invade stratum corneum, hair, nails.
Candida spp. (e.g. C. albicans) may overgrow in moist, occluded areas, especially in immunocompromised or diabetics.
Clinical features-
Diagnosis-
KOH mount microscopy, fungal culture, sometimes PCR or histopathology (less common).
Management principles-
Challenges/complications-
Relapses, resistance, poor penetration into nail plate, compliance issues.[68][69]
1.3 Viral Skin Infections-
Common examples: Herpes simplex, varicella-zoster, molluscum contagiosum, human papillomavirus (warts), viral exanthems.
Pathogenesis & virology-
Viruses infect keratinocytes or adnexal cells; some cause latent infection (e.g. herpes), reactivation under stress or immunocompromise.
Warts (HPV) cause proliferation of epidermal cells.
Clinical features-
Diagnosis-
Primarily clinical; can do Tzanck smear, PCR, viral culture, histopathology.
Management principles-
1.4 Parasitic / Arthropod & Mite Infestations-
Though you did not list this initially, for completeness it’s often included in “infections”: scabies, cutaneous leishmaniasis, etc.
Scabies: intense pruritus, especially at night, often burrows, papules in webs of fingers; caused by Sarcoptes scabiei
Diagnosis by skin scraping, microscopy
Treatment: permethrin cream, ivermectin, treat contacts, environmental decontamination.
2. Inflammatory Skin Diseases (When skin gets irritated or inflamed)-
These are disorders in which dysregulated inflammation (driven by immune cells, cytokines, environmental triggers) causes chronic or relapsing skin changes.
2.1 Eczema / Dermatitis-
Examples: Atopic dermatitis, contact dermatitis (allergic or irritant), nummular eczema, seborrhoeic dermatitis.
Pathogenesis-
Multifactorial: skin barrier defects (e.g. filaggrin mutations), immune dysregulation (Th2, Th22, Th17 axes), microbiome alterations, environmental triggers.
Chronic scratching → lichenification, secondary infection.
Clinical features-
Pruritus is hallmark. Redness, scaling, vesiculation in acute; lichenification, hyperpigmentation in chronic. Distribution often flexural in atopic dermatitis.
Diagnosis-
Primarily clinical; patch testing in suspected allergic contact dermatitis, biopsy rarely needed.
Management principles-
Clinical challenges-
Flare–remission course, poor adherence, comorbidities (e.g. asthma, allergic rhinitis), side effects of long-term therapy.
2.2 Psoriasis-
Pathogenesis
Auto-inflammatory/immune mediated rather than “simple inflammation.” Key contributors: IL-23/Th17 axis, dendritic cells, keratinocyte hyperproliferation, genetic predisposition (e.g. HLA-C*06:02).
Triggers: trauma (Koebner phenomenon), infections, drugs, stress.
Clinical features-
Well-demarcated plaques with silvery scale, typically on extensor surfaces (elbows, knees), scalp, sacrum. Variants include guttate, pustular, erythrodermic, inverse.
Diagnosis-
Clinical; if uncertain, biopsy showing acanthosis, parakeratosis, elongation of rete ridges, neutrophils in stratum corneum (Munro microabscesses).
Management principles-
2.3 Acne Vulgaris-
Pathogenesis-
Multifactorial: follicular hyperkeratinization, sebaceous gland hyperactivity, Propionibacterium acnes (now Cutibacterium acnes) colonization, inflammation, androgen effect.
Clinical features-
Open and closed comedones, inflammatory papules, pustules, nodules; often face, back, chest.
Diagnosis-
Clinical; severity grading (mild, moderate, severe). Occasionally cultures in resistant cases.
Management principles-
2.4 Rosacea-
Pathogenesis-
Unknown but involves vascular dysregulation, neurovascular changes, innate immune activation (LL-37, cathelicidins), demodex mites may play a role.
Clinical features-
Flushing, persistent erythema, papulopustular lesions in central face, telangiectasia, phymatous changes (e.g. rhinophyma). Ocular involvement also common.
Diagnosis-
Clinical. Subtypes (erythematotelangiectatic, papulopustular, phymatous, ocular) guide therapy.
Management principles-
3. Skin Cancer (When skin cells grow abnormally)-
Skin cancers arise when mutations trigger unchecked proliferation of skin cells. They are broadly divided into melanoma and non-melanoma skin cancers (NMSC: basal cell carcinoma, squamous cell carcinoma) as the most common.
3.1 Basal Cell Carcinoma (BCC)-
Pathogenesis-
Frequent association with UV radiation–induced DNA damage (e.g. p53 mutations), sometimes PTCH1 / hedgehog pathway alterations.
Slow-growing, locally invasive but rarely metastasizes.
Clinical features-
Pearly, translucent papules with telangiectasias; may ulcerate (“rodent ulcer”). Frequently on sun-exposed areas (face, neck). Various histologic subtypes: nodular, superficial, morpheaform, pigmented.
Diagnosis-
Dermatoscopy, biopsy (excisional or punch), histopathology.
Management-
Surgical excision (e.g. Mohs micrographic surgery), curettage with electrodessication, cryotherapy, topical therapies (e.g. imiquimod), photodynamic therapy, hedgehog pathway inhibitors in inoperable cases. through the bloodstream, leading to sepsis (life-threatening infection). Symptoms include fever, chills, rapid heartbeat, and confusion.
Severe Burns,Deep burns damaging multiple skin layers or tissues from fire, chemicals, electricity, or hot liquids. Need specialized care, skin grafts, and long recovery.
Skin Cancer:
Uncontrolled growth of abnormal skin cells, often due to sun exposure.
Types: basal cell carcinoma, squamous cell carcinoma, and melanoma (most dangerous). Early detection is vital.[70]
Skin Diseases can be classified as Acute, Chronic and Severe: -
|
Category |
Condition |
Description |
|
1. Acute Skin Conditions. |
Cellulitis |
Bacterial infection of deeper skin layers and tissue. Red, swollen, warm, painful skin (often on legs). Spreads quickly and requires antibiotics |
|
|
Shingles (Herpes Zoster) |
Reactivation of chickenpox virus. Painful rash with blisters, typically on one side of the body. May cause lasting nerve pain if untreated. |
|
|
Impetigo |
Highly contagious bacterial infection, common in children. Red sores/blisters that ooze and crust, especially around nose and mouth. |
|
2. Chronic Skin Conditions. |
Eczema (Atopic Dermatitis) |
Dry, itchy, inflamed skin. Triggered by allergens, stress, or irritants. Often starts in childhood and may improve over time. |
|
|
Psoriasis |
Chronic autoimmune condition. Thick red patches with silvery-white scales, especially on scalp, elbows, and knees. Due to rapid skin cell turnover. |
|
|
Rosacea |
Persistent facial redness, visible blood vessels, bumps. Triggered by spicy foods, alcohol, or sun. |
|
|
Vitiligo |
Autoimmune destruction of pigment cells, causing white skin patches. Not painful or contagious, but may affect self-esteem. |
|
|
Alopecia Areata |
Autoimmune disorder causing sudden, round patches of hair loss on the scalp, face, or body. |
|
3. Severe Skin Conditions |
Necrotizing Fasciitis |
Rare, life-threatening bacterial infection that destroys skin, fat, and muscle. Severe pain, swelling, fever. Needs emergency surgery and antibiotics. |
|
|
Severe Skin Infections |
Deep infections that may cause sepsis. Symptoms include fever, chills, rapid heart rate, and confusion. Requires urgent medical attention. |
|
|
Severe Burns |
Deep tissue damage from fire, chemicals, electricity, or hot liquids. Requires specialized treatment and often skin grafts. |
|
|
Skin Cancer |
Uncontrolled skin cell growth. Caused by sun exposure. Types: Basal cell carcinoma, squamous cell carcinoma, melanoma (most dangerous). Early detection is crucial.[72] |
Common Dermatological Diseases on the basis of Diagnosis, Prevention and Treatment:-
|
Disease |
Diagnosis |
Prevention |
Treatment |
|
1. Acne Vulgaris |
Clinical examination of comedones, papules, pustules |
Proper hygiene, avoid oily cosmetics |
Topical retinoids, antibiotics, oral isotretinoin in severe cases |
|
2.Eczema (Atopic Dermatitis) |
Clinical history and skin appearance |
Avoid allergens, maintain skin moisture |
Topical corticosteroids, moisturizers, antihistamines |
|
3.Psoriasis |
Clinical features, biopsy if needed |
Avoid stress, maintain healthy lifestyle |
Topical steroids, vitamin D analogs, phototherapy |
|
4.Tinea (Fungal Infection) |
KOH examination, fungal culture |
Keep skin dry, avoid sharing towels |
Topical antifungals, oral antifungals if severe |
|
5.Impetigo |
Clinical diagnosis, bacterial culture |
Maintain hygiene, avoid contact with infected people |
Topical or oral antibiotics |
|
6.Vitiligo |
Clinical diagnosis, Wood’s lamp examination |
Sun protection |
Topical corticosteroids, phototherapy |
|
7.Urticaria (Hives) |
Clinical observation |
Avoid triggers, allergens |
Antihistamines, corticosteroids if severe |
|
8.Scabies |
Microscopic exam of skin scrapings |
Avoid close contact, wash bedding and clothes |
Permethrin cream, ivermectin (oral) |
|
9.Alopecia Areata |
Clinical features, scalp examination |
Reduce stress, healthy diet |
Topical steroids, minoxidil |
|
10.Contact Dermatitis |
Patch testing, history of exposure |
Avoid irritants/allergens |
Topical steroids, emollients |
|
11.Herpes Simplex |
Tzanck smear, PCR |
Avoid direct contact during outbreaks |
Acyclovir or valacyclovir |
|
12.Warts (Verruca) |
Clinical examination |
Avoid direct contact with infected surfaces |
Cryotherapy, salicylic acid |
|
13.Melasma |
Clinical diagnosis, Wood’s lamp |
Sun protection |
Hydroquinone, retinoids, sunscreen |
|
14.Cellulitis |
Clinical evaluation, CBC, blood cultures |
Proper wound care, hygiene |
Oral/IV antibiotics |
|
15.Rosacea |
Clinical features |
Avoid alcohol, spicy foods, sun exposure |
Topical metronidazole, oral doxycycline. [73][74] |
Tools of Dermatology:A historical Perspective.
Introduction.
Dermatology, as one of the oldest branches of medicine, has long relied on the power of observation. For centuries, dermatologists have used their eyes—and later, their hands and basic tools—to diagnose and treat skin conditions. While visual inspection remains central to the specialty, a wide array of instruments has emerged over time to improve accuracy, efficiency, and patient outcomes. From ancient cleansing tools to modern digital imaging and artificial intelligence, the evolution of dermatologic tools reflects broader advances in medical science. Exploring this history offers valuable insight into how traditional practices laid the foundation for today’s cutting-edge dermatological care.[75]
Old Techniques use in Dermatology:-
1. Visual Inspection & Palpation.
For centuries, visual examination was the cornerstone of dermatologic diagnosis.
Physicians evaluated color, shape, texture, distribution, and evolution of skin lesions.
Palpation (touching the skin) helped assess consistency, tenderness, temperature, and depth of skin involvement.
This method is still fundamental in modern dermatology, though now complemented by advanced tools.
2. Use of Natural Remedies.
Traditional systems like Ayurveda, Unani, and Chinese medicine relied heavily on natural substances.
Common ingredients:
3. Cautery and Scarification.
Cautery involved burning the skin using heated instruments or chemicals.
Scarification meant deliberately scratching or cutting the skin.
These methods were used to remove warts, ulcers, or tumors, or to stimulate healing by removing “bad blood” or toxins.
Practiced across Egyptian, Indian, African, and Islamic cultures.
4. Leech Therapy & Bloodletting.
Based on the humoral theory, where skin diseases were thought to arise from imbalanced body fluids (blood, phlegm, black bile, yellow bile).
Leeches were applied to draw out "impure" blood and reduce inflammation.
Phlebotomy (manual bloodletting) was also used for chronic skin issues such as boils or acne.
These methods were widely used until the 19th century.
5. Use of Strigils (Roman Era).
Strigils were curved metal tools used by ancient Greeks and Romans.
Applied after oiling the body to scrape off dirt, sweat, and dead skin during bathing rituals.
Believed to promote hygiene, blood circulation, and treat itchy, scaly skin.
6. Poultices and Bandaging.
Poultices were soft, moist preparations made from herbs, plant extracts, clays, or grains.
Applied warm to the skin to reduce inflammation, draw out pus, and soothe irritated skin.
Commonly used with linen or cotton bandages to keep the mixture in place and encourage absorption.
7. Ancient Classifications of Skin Diseases.
Ayurvedic texts (like Charaka Samhita and Sushruta Samhita) classified skin diseases under "Kushta," which included leprosy, eczema, vitiligo, and more.
The Greek physician Hippocrates described skin conditions based on visible symptoms like dryness, pustules, or scaling.
8. Early Microscopy (17th Century Onward).
Microscopes were first used in the 1600s, revolutionizing the study of skin diseases.
Enabled the identification of microscopic organisms, such as:
This marked the transition from speculative to evidence-based dermatology.
9. Wood’s Lamp (Early 1900s).
Invented by physicist Robert W. Wood, this UV light became a diagnostic tool in dermatology.
Helps detect:
Mechanism of Instruments :-
Dermatology uses a wide range of diagnostic, surgical, and therapeutic instruments, each working through a specific mechanism.
Diagnostic tools include the Dermatoscope, which employs magnification and polarized or non-polarized light to reduce surface reflection, allowing doctors to view subsurface skin structures such as pigment networks and blood vessels for early cancer detection. [77]
Biopsy punches use a sharp circular blade to cut through the epidermis and dermis, extracting cylindrical tissue samples for laboratory analysis. [78]
The Wood’s lamp emits ultraviolet light at about 365 nm, making fungal infections, bacterial growth, and pigment disorders fluoresce in characteristic colors. Meanwhile, skin analyzer machines utilize multispectral imaging, including visible, polarized, ultraviolet, and infrared light, to assess wrinkles, pores, melanin, and sebum levels, often generating cosmetic or preventive reports.[78]
Surgical instruments rely on mechanical precision. A scalpel consists of a stainless steel blade designed to cut tissues cleanly.
Forceps and skin hooks provide grip and retraction, helping to manipulate delicate tissues during surgery. Scissors cut by the shearing action of two sharp blades, while needle holders use a ratcheted clamp to secure needles for accurate suturing.[78]
Curettes are spoon-shaped tools with a sharp edge that scrape away superficial skin lesions such as warts or keratoses, and comedone extractors use a hollow loop to apply pressure around pores, forcing out trapped sebum and keratin responsible for blackheads and whiteheads.[78]
Therapeutic devices employ advanced energy-based mechanisms. Electrocautery or diathermy units deliver electric current through a resistive electrode, producing localized heat that cuts, coagulates, or destroys abnormal tissue like warts or skin tags.
Cryoprobes work through rapid cooling: compressed gases like liquid nitrogen or nitrous oxide expand at the probe tip, dropping temperatures to as low as −196 °C, which freezes tissue, forming ice crystals inside cells and leading to their destruction.[79]
Laser machines generate concentrated light beams of specific wavelengths—such as diode, Nd:YAG, or CO? lasers—which are selectively absorbed by target chromophores like melanin, hemoglobin, or water, a process called selective photothermolysis that destroys diseased tissue without damaging nearby skin.[80]
Dermapens and dermarollers use tiny microneedles to puncture the skin at controlled depths, creating micro-injuries that trigger the body’s wound healing response, stimulating collagen and elastin production.[81]
Microdermabrasion machines exfoliate the outermost skin layer using crystals or diamond-tipped probes combined with suction, removing dead cells and encouraging regeneration for smoother, healthier skin.[82]
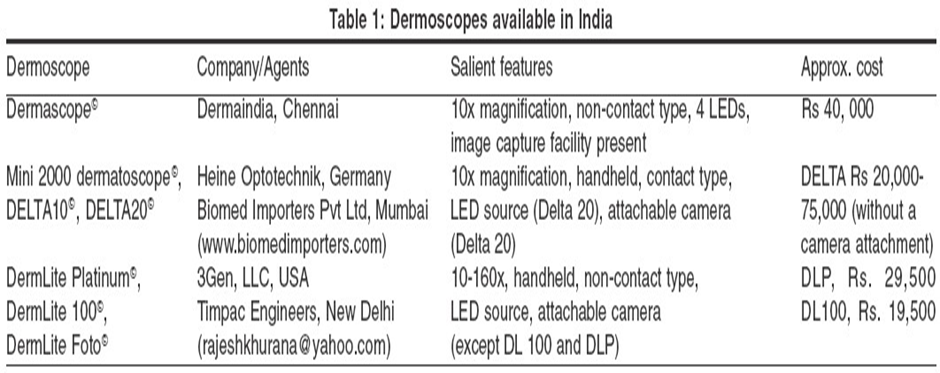
Make of Dermascope :-[83]
Make of Skin Analysis Machine :-
Case study:- Dermatoscope.
Patient Details:
Clinical Examination:
Histopathology → Superficial spreading melanoma, Breslow thickness 0.7 mm.
Treatment & Outcome:
Discussion:
Conclusion:
Dermatoscope (magnification + polarized light) gives a clearer view of subsurface structures. In this case, it enabled early diagnosis and timely treatment, improving prognosis.[84]
Case study:- Derma pen:-
Patient Details:
Clinical Examination:
Procedure:
Patient Response & Outcome:
After 2 sessions: Noticeable improvement in skin texture, mild redness post-procedure but resolved in 24 hours.
After 4 sessions.
Discussion:
Dermapen stimulates collagen and elastin production through controlled micro-injuries. More effective and precise than traditional dermarollers Minimal downtime compared to laser treatments.
Conclusion:
Dermapen proved to be a safe, effective, and minimally invasive solution for acne scars. Patient satisfaction was high due to visible scar reduction and quick recovery time.[85]
Case study :- Skin Analyzer Machine .
Patient Details:
Clinical Examination (Naked Eye):
Use of Skin Analyzer Machine (e.g., OBSERV 520x / VISIA):
Procedure: Patient’s face scanned under multiple light modes (UV, polarized, cross-polarized).
Findings:
Diagnosis & Plan:
Outcome (After 3 months):
Discussion:
Skin analyzer provided objective, data-based insights that were not visible with the naked eye. Helped in personalized treatment planning and in motivating the patient with visible before–after comparisons.
Conclusion:
Skin Analyzer Machine is a valuable tool for preventive dermatology and cosmetic planning. It enhances patient trust by showing measurable results and improves long-term treatment compliance.[86]
Integration of AI in tools of Dermatology:-
Dermatoscops with AI :-
AI-powered image analysis for mole and lesion classification.
Helps in early detection of melanoma and other skin cancers.
Digital Imaging & Teledermatology:-
AI assists in remote diagnosis by analyzing high-resolution images.
Supports virtual consultations and triage of cases.
Histopathology Tools:-
AI algorithms analyze biopsy slides for malignancy.
Enhances accuracy in differentiating benign vs malignant conditions.
Convolutional Neural Networks (CNNs):-
Integrated into apps and devices for automated skin lesion recognition.
Supports dermatologists in faster and more accurate decision-making.
Predictive & Precision Medicine Models:-
AI integrates patient data (genetics, history, lifestyle).
Suggests personalized treatment strategies for conditions like psoriasis, acne, and dermatitis.
Wearable Devices & Mobile Apps:-
AI tracks skin changes over time.
Monitors chronic skin diseases (eczema, vitiligo) and treatment response.
Robotics & Imaging Systems:-
AI-driven robots assist in phototherapy and laser-based treatments.
Improves precision and safety during procedures.[87][88][89]
Recent Advancements on Dermatological Diseases:-
Recent years have seen remarkable progress in preventive dermatology, with innovations focusing on early detection, minimizing disease recurrence, and improving patient outcomes.
Artificial Intelligence (AI):
AI-based technologies are playing a transformative role in dermatology by identifying skin cancers such as melanoma at their earliest stages. Machine learning algorithms can analyze dermoscopic images with high precision, often matching or surpassing dermatologist-level accuracy. This early identification significantly helps prevent disease progression and enhances survival rates.
Light Therapy (Narrowband UV-B):
Narrowband UV-B phototherapy has emerged as a safe and effective preventive treatment for conditions such as vitiligo and psoriasis. It helps halt disease worsening, promotes repigmentation in vitiligo, and reduces inflammation in psoriasis. Its safety profile and non-invasive nature make it particularly suitable for children and sensitive skin types.
Personalized Medicine:
Advances in genomics and immunology have led to personalized preventive strategies. By analyzing genetic, molecular, and environmental factors, clinicians can now predict and prevent relapses in chronic inflammatory skin diseases such as eczema and psoriasis. This approach ensures targeted care and long-term disease control.
2. Diagnosis
Accurate and early diagnosis remains the cornerstone of effective dermatological management. Modern technologies have revolutionized how dermatologists visualize and interpret skin conditions.
AI Diagnostic Tools:
AI-powered pattern recognition systems assist clinicians in differentiating between benign and malignant lesions. These tools analyze lesion morphology, color distribution, and border irregularities from high-resolution dermoscopic images, providing rapid and accurate assessments that support clinical decision-making.
Advanced Imaging Technologies:
Cutting-edge imaging modalities now allow real-time, non-invasive visualization of skin structures at cellular or subcellular levels.
Confocal Microscopy and Optical Coherence Tomography (OCT) provide detailed 3D images of skin layers, improving diagnostic precision for skin cancers and inflammatory conditions. High-Frequency Ultrasound is useful for assessing skin thickness and tumor depth. Raman Spectroscopy and Fluorescence Imaging aid in identifying molecular changes, enhancing diagnostic specificity and reducing the need for unnecessary biopsies.
These technologies collectively enhance diagnostic accuracy, facilitate early intervention, and support ongoing monitoring of treatment response.
3. Treatment
Therapeutic advancements in dermatology have evolved towards precision medicine, targeting the underlying mechanisms of disease rather than just symptoms.
Biologic Therapies:
Biologic agents have transformed the treatment landscape of chronic inflammatory diseases such as psoriasis, atopic dermatitis, and hidradenitis suppurativa. By targeting specific immune pathways—such as interleukin (IL)-17, IL-23, and TNF-α—these therapies provide sustained control, fewer side effects, and better quality of life for patients.
Personalized Treatment Approaches:
With a deeper molecular understanding of skin diseases, dermatologists can now design individualized treatment plans. Genetic profiling, biomarker analysis, and pharmacogenomic data enable the selection of the most effective therapy for each patient, minimizing adverse reactions and maximizing clinical success.
Topical and Drug Innovations:
Modern topical formulations and small-molecule drugs continue to expand therapeutic options. Agents such as gentian violet, tacrolimus, pimecrolimus, imiquimod, tazarotene, adapalene, and calcipotriol have shown significant efficacy against a range of dermatological conditions, including atopic dermatitis, cutaneous lymphomas, genital warts, acne, and psoriasis. These innovations offer improved absorption, enhanced safety, and more targeted mechanisms of action.[90]
Best Dermatology Hospital in India:-
CONCLUSION :
Dermatology has evolved from ancient observational practices to a technologically advanced, evidence-based medical science. The integration of smart solutions such as artificial intelligence, advanced imaging systems, tele dermatology, and personalized diagnostic tools has transformed the assessment and management of skin health. These innovations not only enhance diagnostic precision but also enable preventive, patient-centred, and accessible dermatologic care. As digital technologies continue to advance, dermatology stands at the forefront of medical innovation—bridging traditional expertise with modern intelligence to improve skin health, early disease detection, and overall quality of life. The future of dermatology lies in continuous collaboration between clinicians, researchers, and technologists to ensure safe, ethical, and equitable access to smart skin health solutions worldwide.
REFERENCE


Abhijeet Welankiwar, Samiksha Nimbokar, Smart Solutions for Skin Health: Evolving Assessment System in Dermatology, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4021-4053. https://doi.org/10.5281/zenodo.17712898
 10.5281/zenodo.17712898
10.5281/zenodo.17712898
