Shri Sambhaji College of Pharmacy Nanded.
Malaria continues to be a problem for children returning or immigrating to industrialized countries from tropical regions. Proper diagnosis begins with clinical suspicion. In nonimmune children, malaria typically presents with a high fever that might be accompanied by chills and headache. Symptoms and signs may be more subtle in partially immune children, and anemia and hepatosplenomegaly may also be present [10]. The number of people traveling to malaria-endemic countries continues to increase, and malaria remains the commonest cause of serious imported infection in non-endemic areas. Severe malaria, mostly caused by Plasmodium falciparum, often requires intensive care unit (ICU) admission and can be complicated by cerebral malaria, respiratory distress, acute kidney injury, bleeding complications, and co-infection. The mortality from imported malaria remains significant. This article reviews the manifestations, complications, and principles of management of severe malaria as relevant to critical care clinicians, incorporating recent studies of anti-malarial and adjunctive treatment. Effective management of severe malaria includes prompt diagnosis and early institution of effective anti-malarial therapy, recognition of complications, and appropriate supportive management in an ICU. All cases should be discussed with a specialist unit and the transfer of the patient considered [9]. Children may present with respiratory distress and/or rapidly progressing cerebral malaria that manifests as altered sensorium and, sometimes, seizures. Thick blood smears help to determine when infection is present, but a single smear without parasites is not sufficient to rule out malaria. Thin blood smears aid in identifying the species of parasite [10].
Severe malaria is most commonly caused by infection with Plasmodium falciparum, although P. vivax and P. knowlesi2,3 can also cause severe disease. The risk is increased if treatment of an uncomplicated attack of malaria caused by these parasites is delayed [1]. Once an Anopheles mosquito with the infection bites a human, the parasites multiply in the host’s liver before causing infection and destroying red blood cells. Early symptoms include a fever, and over time, it can affect the internal organs, leading to death [6].

Image 1-
In the past, chloroquine was effective for treating nearly all cases of malaria. In recent studies, chloroquine-resistant P. falciparum malaria has been observed with increasing frequency across the country. The continued treatment of such cases with chloroquine is probably one of the factors responsible for increased proportion of P. falciparum relative to P. vivax. A revised National Drug Policy on Malaria has been adopted by the Ministry of Health and Family Welfare in 2008 and these guidelines have therefore been prepared for clinicians involved in the treatment of malaria [3]. Severe malaria is important. It is a major cause of preventable childhood death in tropical countries. Tis large number of avoidable deaths justifes the substantial global investments in malaria control and elimination. But severe malaria is increasingly overlooked by the international agencies, donors and policy makers who determine the direction and support for global malaria initiatives [4]. Malaria remains a devastating global health problem. Worldwide, an estimated 300–500 million people contract malaria each year, resulting in 1.5–2.7 million deaths annually. Because of the increase in global travel to and immigration of people from areas endemic for malaria, the incidence of imported cases of malaria in developed countries has risen. Approximately 10 000–30 000 travellers from industrialized countries are expected to contract malaria each year. In addition, drug-resistant Plasmodium falciparum malaria continues to spread and at present involves almost all areas of the world. An increasing number of travellers are exposed to drug-resistant plasmodia [2].
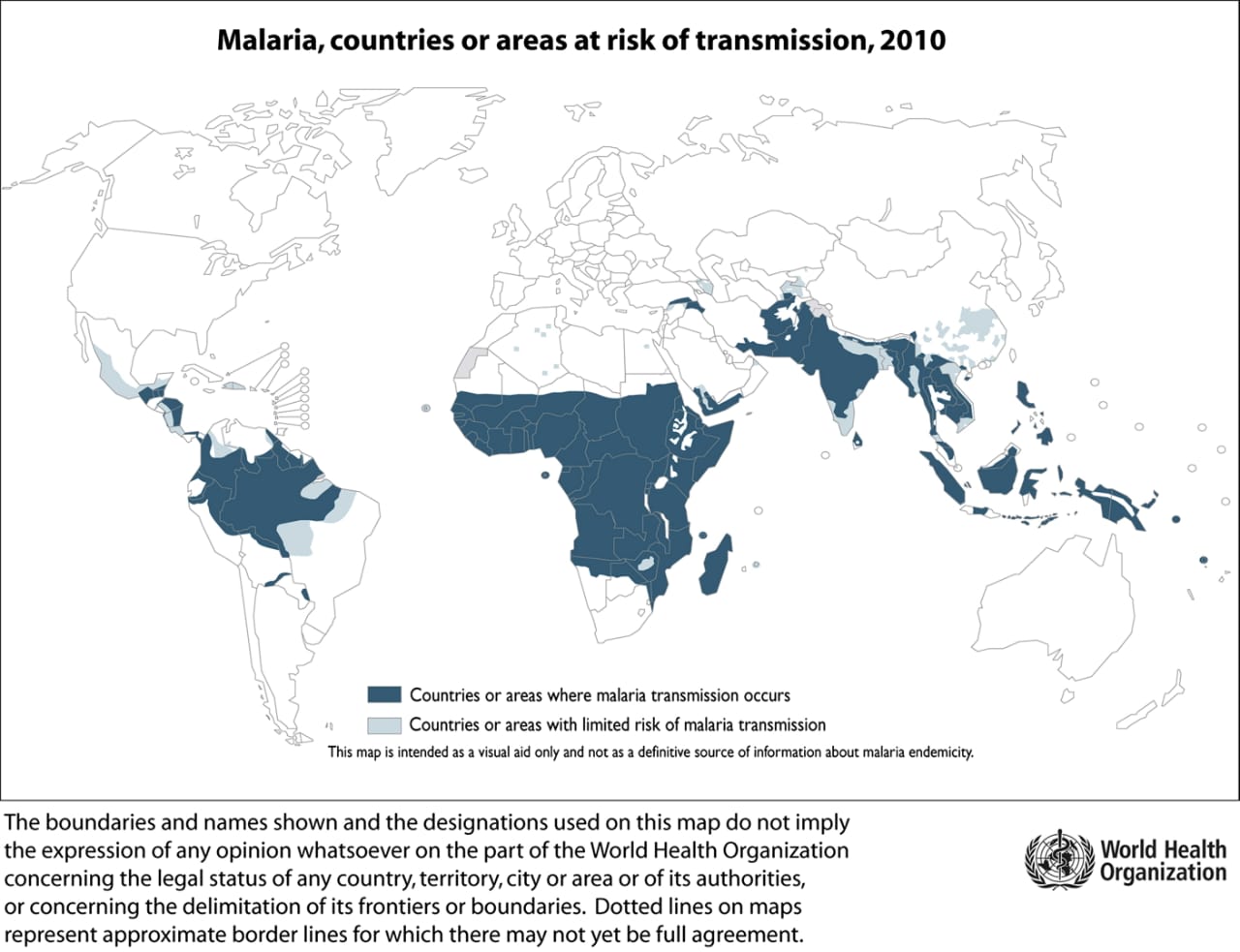
Figure- Countries and areas with risk of malaria transmission. Map from WHO International Travel and Health Programme [ 9].
Causes –
A person can develop malaria if they receive a bite from an infected mosquito. To cause an infection in a person, the insect must carry a parasite known as Plasmodium. There are many types of this parasite, but only five –
Five species of Plasmodium (single-celled parasites) can infect humans and cause illness:
Falciparum malaria is potentially life-threatening, can cause malaria in humans. Moreover, only a bite from a female Anopheles mosquito can transmit malaria to humans. [6].
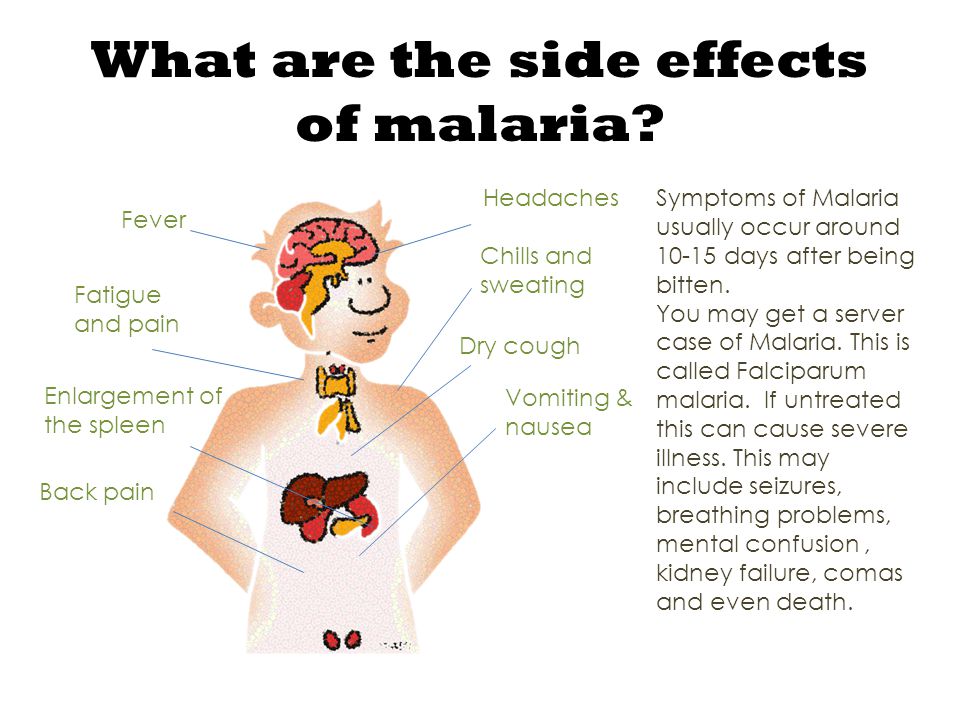
In some cases, malaria can progress and affect vital body organs. At this point, malaria parasites have affected over 5% of the red blood cells.
Symptoms Include:
Severe malaria is a life threatening medical emergency [6].
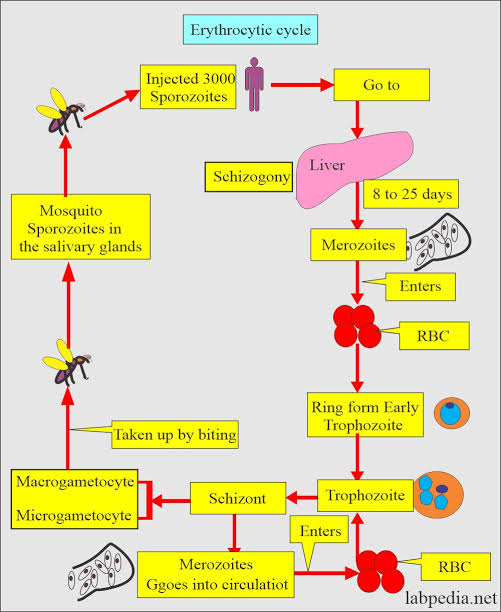
Image-2 Life Cycle of Malaria.
The mosquito vector transmits the Plasmodium spp. parasite in the sporozoite stage to the host during a blood meal. Within 30–60 minutes, sporozoites invade liver cells, where they replicate and divide as merozoites. The infected liver cell ruptures, releasing the merozoites into the bloodstream, where they invade red blood cells and begin the asexual reproductive stage, which is the symptomatic stage of the disease. Symptoms develop 4–8 days after the initial red blood cell invasion. The replication cycle of the merozoites within the red blood cells lasts 36–72 hours (from red blood cell invasion to haemolysis). Thus, in synchronous infections (infections that originate from a single infectious bite), fever occurs every 36–72 hours, when the infected red blood cells lyse and release endotoxins en masse. Plasmodium vivax and Plasmodium ovale can also enter a dormant state in the liver, the hypnozoite. Merozoites released from red blood cells can invade other red blood cells and continue to replicate, or in some cases, they differentiate into male or female gametocytes. The transcription factor AP2-G (not shown) has been shown to regulate the commitment to gametocytogenesis. Gametocytes concentrate in skin capillaries and are then taken up by the mosquito vector in another blood meal. In the gut of the mosquito, each male gametocyte produces eight microgametes after three rounds of mitosis; the female gametocyte matures into a macrogamete. Male microgametes are motile forms with flagellae and seek the female macrogamete. The male and female gametocytes fuse, forming a diploid zygote, which elongates into an ookinete; this motile form exits from the lumen of the gut across the epithelium as an oocyst. Oocysts undergo cycles of replication and form sporozoites, which move from the abdomen of the mosquito to the salivary glands. Thus, 7–10 days after the mosquito feeds on blood containing gametocytes, it may be ‘armed’ and able to infect another human with Plasmodium spp. with her bite. Drugs that prevent Plasmodium spp. invasion or proliferation in the liver have prophylactic activity, drugs that block the red blood cell stage are required for the treatment of the symptomatic phase of the disease, and compounds that inhibit the formation of gametocytes or their development in the mosquito (including drugs that kill mosquitoes feeding on blood) are transmission-blocking agents. *Merozoite invasion of red blood cells can be delayed by months or years in case of hypnozoites. The number of days until symptoms are evident. The duration of gametogenesis differs by species [8].
Effects –
Malaria affecting skeletal muscles the detrimental effects of the causing malaria agents on skeletal muscles in animals and humans are well known. The main pathogenic mechanism in severe malaria is microvascular sequestration of parasitized red blood cells, decreasing oxygen delivery, leading to obstructed blood flow and tissue hypoxia. The skeletal muscle microvascular function and its oxygen consumption is significantly impaired in malaria in the proportion of the disease severity and oxygen consumption in severe malaria reduces similarly as in sepsis patients.[7]. Effects of malaria on cardiac muscle Few studies have been focused on cardiac effect in severe malaria despite serious symptoms of coronary complications have been observed in severe malaria patients. Although, few electrocardiographic reports of malaria patients have been published, their results have shown even some cases of deaths related to cardiac arrhythmias in severe malaria [7]
Diagnosis –
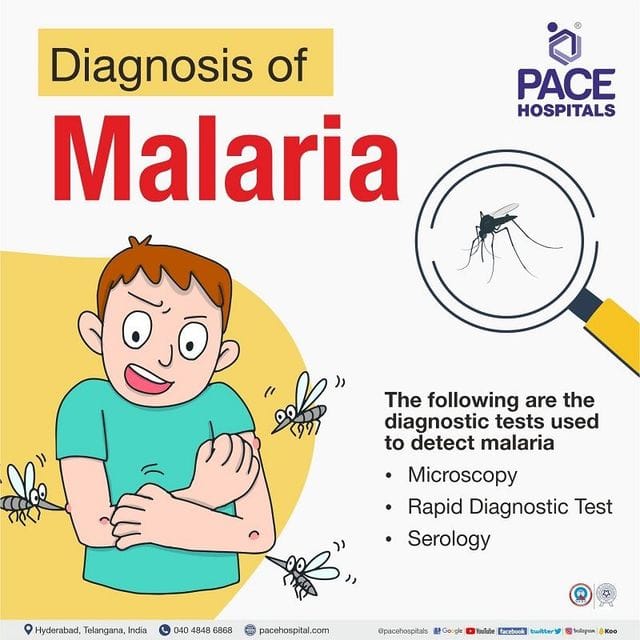
Early diagnosis is critical for recovery from malaria. People can acquire an infection even after taking antimalarial drugs. In this case, symptoms can show up to a year after infection. Anyone with symptoms that may indicate malaria should speak with a doctor as soon as possible. They should tell the healthcare professional if they have been in an area where malaria has been present in the past 12 months. A doctor will ask the person about their symptoms and travel history. If they suspect malaria, they will order some blood tests.
These Include:
Treatment –
Treatment of P. falciparum
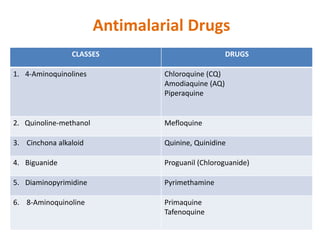
cases the treatment of P. falciparum malaria is based on areas identified as chloroquine resistant/ sensitive as listed in annexure. Artemisinin Combination Therapy (ACT) should be given in resistant areas whereas chloroquine can be used in sensitive areas. ACT should be given only to confirmed P. falciparum cases found positive by microscopy or RDT. ACT consists of an artemisinin derivative combined with a long acting antimalarial (amodiaquine, lumefantrine, mefloquine or sulfadoxine-pyrimethamine). The ACT used in the national programme in India is artesunate + sulfadoxine-pyrimethamine (SP). Presently, Artemether + Lumefantrine fixed dose combination and blister pack of artesunate + mefloquine are also available in the country. Other ACTs which will be registered and authorized for marketing in India may be used as alternatives. According to current WHO guidelines, ACTs can be given in the second and third trimester of pregnancy. The recommended treatment in the first trimester of pregnancy is quinine. Artemisinin derivatives must never be administered as monotherapy for uncomplicated malaria. These rapidly acting drugs, if used alone, can lead to development of parasite resistance.[3]. Mixed infections with P. falciparum should be treated as falciparum malaria.
Vaccination:
A vaccine is now available for preventing malaria, but it is not for use by travelers. It has approve for children who live in moderate-to-high risk areas in Sub-Saharan Africa, where infection with Plasmodium falconium is common. So far, health experts have administered over 2.3 million doses, and it has a good safety profile. While the vaccine will save lives, it is not 100% effective. Currently, in children under the age of 5 years, it:
Strategies For Preventing Malaria Include:
Antimalarial drugs are around 90% effective in preventing malaria. If a person uses these drugs, they should still take measures to prevent bites when spending time in an area where the disease is likely. Anyone planning to travel to an area where malaria is common should enquire about malaria tablets in good time. In most cases, people need to start taking the drugs days before traveling. They may also need to take tests before using some drugs, and it can take time to organize these screenings.[6].
Aim & Objective:
Aim:
To provide insights that inform better policies, enhance treatment strategies, and improve efforts towards malaria control and eventual eradication.
Objective:
CONCLUSION –
Rates of international travel continue to increase and the ‘febrile returned traveller’ is an increasingly common clinical problem. Malaria remains the most important cause of imported fever and cases requiring ICU admission continue to be associated with a high mortality. While there have been significant advances in our understanding of the management of malaria in the last decade, high-quality data to guide management of imported malaria remain scarce, with most derived from endemic settings or retrospective series. The emergence of artemisinin-based therapy has translated into a significant improvement in outcomes in endemic countries and is likely to improve outcomes in imported malaria in the future.
REFERENCES








Sontakke Pradip*, Waghmare Vyankatesh, Farande Rushikesh, Swami Bhujayya, Shinde Devanand, Shaikh Shirin Fatema, Wangawar Pallavi, Suryawanshi Yogita, Severe Health Effect of Malaria and its Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 925-933 https://doi.org/10.5281/zenodo.15176296
 10.5281/zenodo.15176296
10.5281/zenodo.15176296
