Swastyadarpan Pratishthan’s Shantiniketan College of Pharmacy, Dhotre (BK) Ahmednagar, Maharashtra -414304
A major limiting factor for the treatment of central nervous system (CNS) related diseases is the incapability for medicine substances to cross the blood- brain hedge. Some specifics may retain cure- limiting systemic side goods that hamper their capability to reach maximum effective attention in the CNS. Over the last several decades, scientists have studied the capability for medicines to be transported from the nose directly to the brain, and compared to intravenous injections, numerous studies have reported advanced brain attention from phrasings administered intranasally. The primary focus of this paper is to review the expression and device approaches that have been reported to increase medicine delivery into the CNS through the nose- to- brain delivery pathway.
Neurological diseases are the leading cause of disability worldwide, adding the burden on healthcare(1). Brain medicine delivery is challenging due to the Blood Brain hedge (BBB), the complexity of the brain, and safety and toxin enterprises. Nose- to- brain medicine delivery has surfaced as a novel,non-invasive route with advantages over systemic medicine administration similar as Elusion of systemic toxin, better side effect profile,non-invasiveness, short quiescence, and increased Central Nervous System (CNS) bioavailability. Nose- to- brain medicine delivery bypasses the BBB through neural connections among the olfactory epithelium, olfactory bulb, trigeminal whim-whams, and the brain (2).
Define: Nose to brain drug delivery system is a novel invasive technique that allows direct transportation of therapeutic drugs from the nasal cavity to the brain through the olfactory and trigeminal neural pathways by passing the blood-brain barrier (3). This system enhance drug absorption in the brain, provides faster onset of action and minimizes systemic side effect (4).
Alzheimer’s Disease: Number of patients suffering from neurodegenerative diseases and other central nervous system (CNS) disorders has shown a continuous increase that is associated with the aging population during the last decade (5). Alzheimer’s disease (AD), Parkinson’s disease, schizophrenia, migraine, malignant glioma, vestibular schwannoma, meningitis, and multiple sclerosis are representative CNS-related diseases (6).
Neurofibrillary tangles and plaques containing β-amyloid is what biologically characterizes Alzheimer’s disease (AD) (7). The classic presentation of AD, a hereditary and sporadic neurodegenerative disease, is amnesty” cognitive impairment; its less prevalent variations, on the other hand, induce non-amnestic cognitive impairment (8). Although AD is a prevalent cause of cognitive impairment that develops in midlife and late life, other neurodegenerative and cerebrovascular disorders can alter its clinical impact (9). Between 60 and 70 percent of all occurrences of cognitive impairment in the senior population are caused by Alzheimer’s disease (AD), a progressive neurodegenerative illness (10).
It is typified by a slow deterioration in behavioural, cognitive, and memory abilities that eventually results in total dependence (11). It is estimated that 2.3 million persons in the US have Alzheimer's disease (with a range of 1.09 to 4.8 million. The number of cases increases every five years after age 60. While a variety of progressive and fatal neurological conditions were known at that time, including senile dementia, the early age four years later1.
SYMPTOMS:
Alzheimer’s disease causes symptoms that get worse over time, and they are different from the normal changes that happen as people get older (12).
These symptoms often start with memory problems:
CAUSES & RISK FACTORS OF AD:
Causes & Risk Factors of AD
|
Causes |
Risk Factor |
|
A build of amyloid plaques (misfolded beta-pleated protein) And tau tangles in the brain |
Poor Cardiovascular health |
|
Genetics |
DOWN Syndrome |
|
Environmental factors |
Head ingury |
|
|
Family history |
PATHOPHYSIOLOGY:

Fig: Pathophysiology Of AD
ALZHEIMER’S DISEASE (AD) PATHOGENESIS:
The pathogenesis of Alzheimer’s disease involves two major hypotheses that explain how neuronal damage and cognitive decline occur (16):
1. Amyloid Cascade Hypothesis:
This is one of the most widely accepted explanations for Alzheimer’s disease. According to this hypothesis (17):
Intracellular deposition of neurofibrillary tangles (NFT) and extracellular deposition of amyloid-beta (Aβ) plaques Lead to a series of damaging cellular events.
2.The Cholinergic Hypothesis:
According to this theory, the primary cause of Alzheimer’s disease is a lack of the neurotransmitter acetylcholine (Ach), which is essential for memory and learning (18).
It includes:
Decrease in the enzyme that breaks down acetylcholine, acetylcholinesterase (unbalanced enzyme activity impacts signalling) (19).
Acetylcholine neurotransmitter levels drop as a result, which leads to: Impairment of the transmission of nerve impulses, these abnormal protein accumulations cause, Disruption of calcium (Ca²?) Homeostasis, Overproduction of free radicals, leading to oxidative stress (20).
WHY DIAGNOSIS IS IMPORTANT.
Early Interventions: An early diagnosis gives you more time to begin treatments, seek support, and plan for future care. Excluding Other Causes: Many illnesses can cause memory and thinking issues, and a comprehensive diagnosis can help identify and cure these conditions if they exist.
TREATMENT:
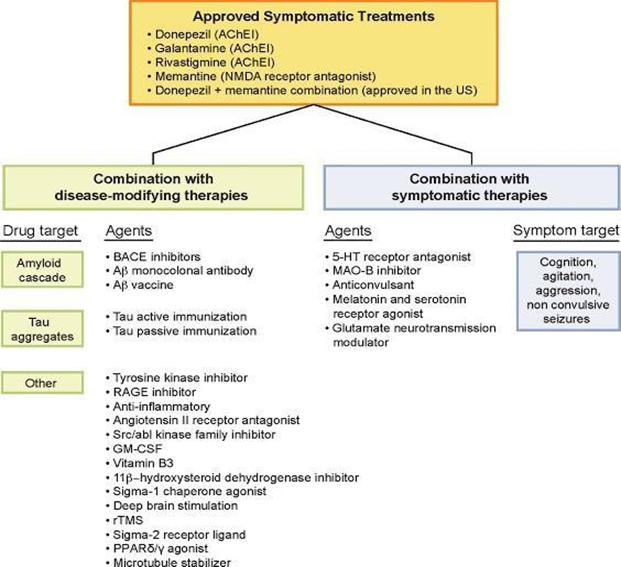
Fig. Treatment
Approved Symptomatic Treatments for Alzheimer’s Disease Current authorized symptomatic therapies include: Donepezil (Ache) Galantamine (Ache) Rivastigmine (Ache). Memantine (an NMDA receptor antagonist). Donepezil + Memantine combination
Combination with Disease Modifying Therapies Drug Targets and Agents. 1. The amyloid cascade: BACE Inhibitors A β monoclonal antibody. Aβ vaccination 2. Tau Aggregate: Tau active immunization. Tau passive immunization. 3. Other targets: Tyrosine kinase inhibitors RAGE inhibitors Anti-inflammatory agents (21). Angiotensin II receptor antagonist Sc/Abl kinase family inhibitor GM-CSF Vitamin B3 11β-hydroxysteroid dehydrogenase inhibitor. Sigma-1 chaperone agonist Deep Brain Stimulation Repetitive transcranial magnetic stimulation (rTMS). Sigma-2 receptor ligand. PPARγ agonist A microtubule stabilizer --- Combination of Symptomatic Therapies Agents: 5-HT receptor antagonist, MAO-B inhibitors, Anticonvulsant and serotonin receptor agonists (22). Glutamate Neurotransmission Modulator Symptom Targets: Cognition Agitation Aggression Non-convulsive seizures (23).
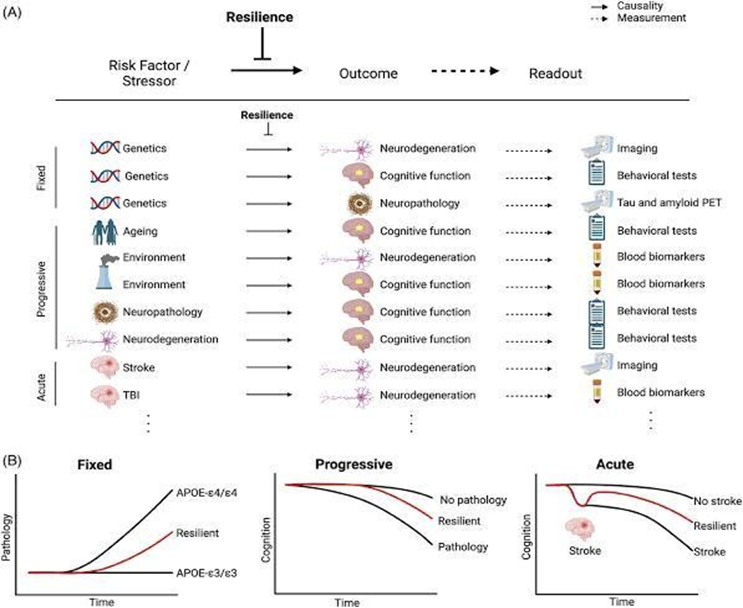
RECENT ADVICES:
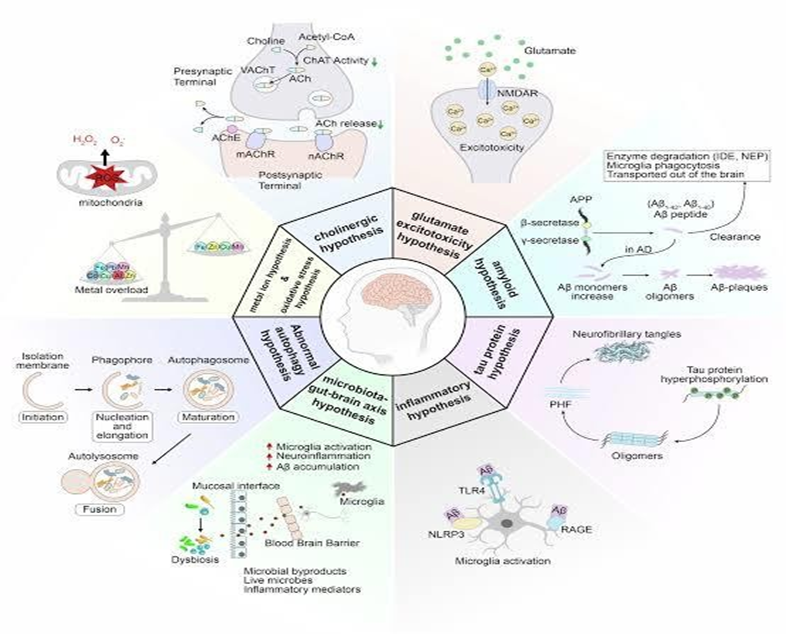
Fig: Recent Advices in Alzheimer’s Disease
Disease-modifying Therapies Monoclonal Antibodies: FDA-approved medications such as lecanemab and aducanumab target and eliminate amyloid-beta in the brain, halting disease development . Future Targets: Other antibodies targeting amyloid-beta and the tau protein, both of which are associated with Alzheimer’s disease, are being studied (24).
CHALLENGES AND FUTURE DIRECTION:
Challenges and Future Directions. Blood-Brain Barrier (BBB) Penetration: One key problem is effectively getting medications over the BBB to the brain. Amyloid-Associated Imaging Abnormalities (ARIAs) (25) Monoclonal antibody therapies have been linked to adverse effects such as cerebral edema and microhaemorrhages. need for a cure: Current disease-modifying medications assist control the condition, but they do not cure Alzheimer’s or repair damaged neurons (26).
NEW DIRECTION OF ALZHEIMER’S DISEASE:
FUTURE STRATEGY:
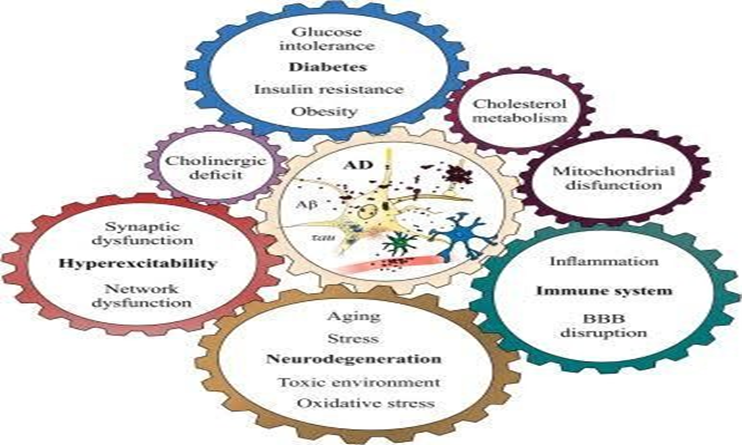
Fig: Future Strategies of Alzheimer’s Disease
REFERENCE



Umesh Jaybhaye, Shradhha Kayande, Ashwini Waybhase, Review on Nose-To-Brain Drug Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4859-4865. https://doi.org/10.5281/zenodo.17762345
 10.5281/zenodo.17762345
10.5281/zenodo.17762345
