Institute of Pharmacy and research, Badnera, Amravati
Tuberculosis (TB) is a major global health concern, particularly in low- and middle-income countries like India, where it remains a leading cause of morbidity and mortality. Although the Indian government provides free TB treatment through public health programs, a significant proportion of patients still rely on private healthcare services, leading to considerable out-of-pocket expenses. This review focuses on the cost variation among anti-tuberculosis (anti-TB) drugs and its impact on treatment accessibility. It covers the epidemiology, types, diagnosis, and standard treatment regimens for both drug-susceptible and drug-resistant TB. The study reveals significant price disparities across different brands of the same drug, with cost variation percentages ranging from 10% to over 400%. Fixed-dose combinations also showed substantial cost differences. The review further discusses the direct and indirect costs borne by patients—including medication, diagnostics, hospitalization, travel, and wage loss—with total annual costs per patient ranging from ?155,200 to ?411,000. These financial burdens often hinder treatment adherence, contributing to the emergence of multidrug-resistant TB (MDR-TB). The paper emphasizes the need for strict pricing regulations, better awareness of free government services, and stronger public-private coordination. Addressing these disparities is crucial for improving treatment outcomes and reducing the overall TB burden.
Tuberculosis (TB) is an infectious disease primarily caused by the bacterium Mycobacterium tuberculosis. It most commonly affects the lungs (pulmonary TB) but can also impact other parts of the body, including the kidneys, spine, and brain (extra-pulmonary TB). Tuberculosis (TB) continues to be a significant global health issue, with around 10.6 million new cases reported in 2021, as noted in the 2022 WHO Global TB Report. The incidence of multidrug-resistant and rifampicin-resistant TB (MDR/RR-TB) is rising, with approximately 450,000 new cases that year. Although existing treatments for both drug-susceptible (DS) and drug-resistant (DR) TB have saved countless lives, TB remains a leading infectious cause of death, accounting for 1.6 million fatalities in 2021, including 187,000 individuals with HIV. If trends continue, it could soon surpass COVID-19 as the leading cause of death from a single infectious agent.[1]
In the last decade, the infection rate has continued to rise. According to the Global Tuberculosis Report published by the WHO, TB infections have affected around 1% of the global population annually from 1997 to 2023. A pictograph illustrates the global distribution of TB cases in 2022, showing that eight countries accounted for more than two-thirds of all TB cases. These countries are India (27%), Indonesia (10%), China (7.1%), the Philippines (7%), Pakistan (5.7%), Nigeria (4.7%), Bangladesh (3.6%), and the Democratic Republic of Congo (3.0%). This information is based on the Global Tuberculosis Report published by the WHO in 2023.[2]
TYPES OF TUBERCULOSIS:
? Tubercular Lymphadenitis: Jones and Campbell classify peripheral tuberculosis of the lymph nodes into five stages:
Stage I: Enlarged, firm, mobile, and discrete lymph nodes.
Stage II: Large, rubbery nodes fixed to surrounding tissue.
Stage III: Central softening due to abscess formation.
Stage IV: Formation of a collar stud abscess.
Stage V: Formation of sinus tracts.[3]
?Pleural TB: Pleural tuberculosis accounts for up to 30% of all extrapulmonary tuberculosis (EPTB) cases in countries with a high burden of the disease. Patients typically present with an acute febrile illness, non-productive cough, pleuritic chest pain, and symptoms such as night sweats, chills, weakness, dyspnoea, and weight loss. The pathogenesis of pleural TB is believed to result from delayed hypersensitivity rather than direct infection of the pleural space. This space becomes infected through initial lung parenchymal lesions, triggering an immune response dominated by neutrophils in the first 24 hours. This is followed by a lymphocyte-driven response, leading to the formation of pleural granulomas and the release of Adenosine Deaminase (ADA). Neutrophils act as the first line of defence for the first 24 hours, followed by macrophages peaking at 96 hours, and then by lymphocytes. The delayed hypersensitivity reaction to mycobacterial antigens affects the pleura, increasing capillary permeability and leading to fluid accumulation in the pleural cavity. This fluid is drained through openings in the parietal pleura called stomata. However, when the parietal pleura is diffusely involved and stomata are damaged or obstructed, pleural fluid builds up. Chronic TB empyema can leave the pleura thickened, scarred, and calcified, causing long-term chest pain, dyspnoea, and reduced lung function. Pleural fibrosis, a well-known complication, is reported in 5-55% of pleural TB cases. [4,5]
? Abdominal TB: Abdominal tuberculosis is diagnosed in 11% of patients with extrapulmonary tuberculosis (EPTB), a significant reduction from the 55-90% seen before the advent of effective antitubercular treatment (ATT). The ileocecal region is the most commonly affected site in the gastrointestinal tract due to several factors:
- Higher concentration of lymphoid tissue (Peyer’s patches)
- Increased physiological stasis
- Greater fluid and electrolyte absorption
- Lower digestive activity
Other affected sites, in descending order of frequency, include the ascending colon, jejunum, appendix, duodenum, stomach, oesophagus, sigmoid colon, and rectum. Hepatobiliary, splenic, and pancreatic tuberculosis are rare and usually associated with miliary tuberculosis, particularly in immunocompromised patients. Mycobacterium tuberculosis (MTB) bacilli reach the abdominal organs through two main pathways, leading to disease reactivation from dormant foci:
?Central Nervous System (CNS) TB: TB meningitis, accounting for 0.5-1% of all CNS tuberculosis is a serious and often fatal form of extrapulmonary TB, primarily affecting young children and posing significant diagnostic challenges. It manifests in two main forms:
1. TB meningitis, accounting for 0.5-1% of all tuberculosis cases.
2. Intracranial tuberculoma, which makes up as much as 40% of brain tumours.
Mycobacterium tuberculosis (MTB) bacilli reach the central nervous system during the dissemination process that occurs in active pulmonary TB. These bacilli cross the blood-brain barrier (BBB) via infected monocytes or neutrophils, leading to the formation of caseating lesion, or "Rich focus," in the brain parenchyma or meninges. When these foci rupture into the subarachnoid space, they trigger an inflammatory T-cell response, resulting in elevated levels of interferon-gamma (IFN-y) and tumour necrosis factor-alpha (TNF-³) in the cerebrospinal fluid (CSF). This inflammation produces infiltrates that obstruct CSF outflow, causing hydrocephalus, and vasculitis, which can lead to infarction and potentially irreversible neurological damage.[8]
?Bone And Joint TB: Osteoarticular tuberculosis accounts for 10-15% of all extrapulmonary TB cases. It typically results from the reactivation of dormant Mycobacterium tuberculosis (MTB)bacilli that become lodged in bones (such as the spine or large joints) during the bacteremia phase of primary lung infection. These bacilli are drawn to the spine and large joints due to their rich blood supply. When the initial infection spreads from the bone to the joint, it leads to tuberculous arthritis. In rare cases, MTB bacilli can reach the spine directly from the lungs via the Batson paravertebral venous plexus or through lymphatic drainage to the para-aortic lymph nodes. Additionally, non-tuberculous mycobacteria (NTM) have been linked to osteoarticular TB, particularly following trauma or surgical procedures like joint arthroplasty. In patients with AIDS or transplant recipients, NTM bone infections occur through hematogenous spread. More recently, skeletal infections caused by M. bovis have been observed in individuals undergoing intravesical Bacillus Calmette Guérin (BCG) vaccine therapy.[9]
?Genito-Urinary TB (GUTB):
Following the hematogenous spread of bacilli from an active infection site, typically the lungs, the bacilli become lodged in the kidneys (the most common site for GUTB) and form metastatic lesions known as tubercles. These infection sites may heal on their own or with treatment, enlarge and rupture into nephrons, or remain dormant for many years. The infection typically spreads in a descending manner from the kidneys to other genitourinary organs. GUTB usually develops between the 2nd and 4th decades of life, often after 5-25 years of dormancy following a primary lung infection.[10]
?Miliary TB:
Miliary tuberculosis accounts for less than 2% of all tuberculosis cases and up to 20% of extrapulmonary tuberculosis cases among immunocompetent adults. However, autopsy studies have indicated that the prevalence of miliary TB can range from 0.3% to 13.3%. The TH2 immune response plays a crucial role in the immunopathogenesis of miliary TB, as it inhibits protective mechanisms like granuloma formation, which helps contain disease activity at the infection site. During the TH2 response, the production of interleukin 4 (IL-4) downregulates nitric oxide synthase (NOS), toll-like receptor 2, and macrophage activation, effectively undermining the protective functions of TH1 cells. This process promotes the
dissemination of Mycobacterium tuberculosis (MTB).[11]
PATHOGENESIS:
Macrophages as a Model for M. tuberculosis Studies
Mycobacterium tuberculosis primarily infects macrophages, making these cells crucial for studying the pathogen's virulence. Ex vivo studies using mouse or human macrophage models help analyse early infection stages, although human alveolar macrophages are difficult to obtain.
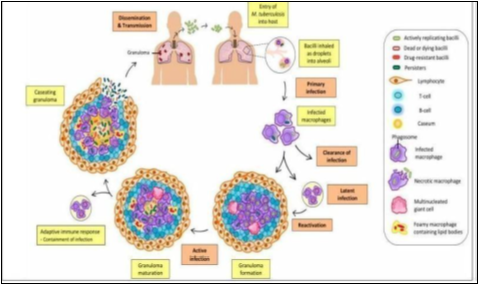
Figure 1: Pathogenesis in HUMAN
Mouse- macrophages can be sourced from bone marrow, lung alveoli, or peritoneal exudates, with primary cells providing more representative data, albeit with variability. Mouse macrophage cell lines, such as J774 and MH-S, are also widely used due to the availability of reagents and genetic modification options. Activation of macrophages for studying M. tuberculosis involves adding interferon-gamma and lipopolysaccharide to induce nitric oxide production. Human macrophages, derived from peripheral blood monocytes or bronchoalveolar lavage, are useful for understanding human disease stages, though they often do not effectively kill M. tuberculosis. However, there are limitations in using macrophages for virulence studies. Some M. tuberculosis mutants may not show an attenuated phenotype in macrophages but could still exhibit defects in growth in mice. Additionally, macrophages from different organs can respond variably to infection, as demonstrated by differences observed in lung and peritoneal macrophages from sensitive versus resistant mouse strains. This variability highlights the need for caution when relying solely on macrophage studies for virulence assessment.[12]
TREATMENT OF TUBERCULOSIS (Drug Susceptible -TB):
For nearly 50 years, the standard treatment for drug-susceptible tuberculosis (DS-TB) has been a six-month short-course chemotherapy regimen developed from extensive clinical trials. This regimen includes an intensive two-month phase with rifampicin, isoniazid, and pyrazinamide, followed by a four-month continuation phase. While effective, this treatment duration can be challenging for patients and health programs, prompting interest in shorter alternatives.
Initial studies suggested that adding fluoroquinolones might reduce treatment duration, but later trials showed that four-month regimens with these drugs did not meet efficacy benchmarks. Nevertheless, higher doses of rifampicin and the use of rifapentine have shown promise in shortening treatment to four months, leading to a conditional WHO recommendation for eligible patients.
Innovative drug combinations, including the new agent pretomanid, have also been explored, with some trials indicating faster bacterial clearance but potential safety concerns. Certain studies have demonstrated that subsets of patients, particularly those with less severe TB, can be effectively treated in shorter durations, such as 16 weeks for children or eight weeks for adults.
The ongoing need for shorter, safe regimens for both DS-TB and drug-resistant tuberculosis (DR-TB) is emphasized, as well as the potential for long-acting injectable treatments. Research into biomarkers for relapse-free cures, individualized treatment strategies, and adjunctive host-directed therapies is essential. Implementing these strategies in real-world settings remains crucial, alongside overcoming barriers to accessing new treatments and ensuring appropriate diagnostic tests are available.[13]
Classification of Anti-tubercular drugs:

Figure 1: Classification of Anti-TB drugs
VARIATION OF COST AMONG ANTI-TUBERCULOSIS DRUGS:
Tuberculosis (TB), a communicable disease, can affect individuals of any age, caste, or class but predominantly impacts the poorer segments of society. India contributes to1/4th of global incidence of TB. The economic burden of TB in India is substantial, amounting to Rs 12,000 crore annually. For patients, the cost of diagnosis and successful treatment ranges between US $100 to $1,000. In India, TB treatment is provided by the government under the Revised National TB Control Programme (RNTCP) as well as through private healthcare providers. However, not all TB cases are accurately diagnosed or reported on time, with an estimated notification rate of only 58%. Around one-third of TB cases go undiagnosed, are diagnosed but not treated, or are treated but not reported to the RNTCP. In May 2012, India declared TB a notifiable disease, but the World Health Organization estimated that nearly 1 million cases were still not reported. A study by Satyanarayana S et al further suggests that nearly 46% of TB patients may not be reported to the RNTCP.
Many people in India are unaware that the government provides all TB medications free of charge, leading them to seek treatment in the private sector. However, private healthcare providers may mismanage TB treatment, contributing to the rise of drug-resistant strains of TB. Factors such as improper use of diagnostic services, incorrect treatment protocols, and lack of supervision during TB therapy can lead to drug-resistant forms like MDR-TB and XDR-TB. Poor patients, lacking the financial means to complete treatment with private practitioners, may exacerbate the situation. Therefore, the current study was conducted to assess the cost variation of anti-TB drugs in India.
The prices of various anti-TB drugs were gathered from the latest editions of CIMS and the Indian Drug Review. The highest and lowest prices of these drugs, produced by different pharmaceutical companies but in the same dosage and formulation, were recorded. The cost for a set of 10 tablets or capsules was determined. The cost ratio, which is the comparison between the most expensive and least expensive brand of the same generic anti-TB drug, was calculated.[14] This ratio shows how many times more expensive the priciest brand is compared to the cheapest one within the same generic drug group. The percentage cost variation was computed using the formula:
% Cost Variation = (Maximum Cost 3 Minimum Cost) x 100
Minimum Cost
Additionally, fixed-dose combinations of anti-TB drugs were included in the study.
Table 1: Cost variation of various anti-TB drugs in India
|
Sr. no |
Drug |
Dose |
Maximum cost (INR) |
Minimum cost (INR) |
Cost difference |
% cost variation |
|
1.
|
Isoniazid
|
100 mg |
--- |
8.40 |
--- |
0 |
|
300 mg |
86 |
27.60 |
58.4 |
211.59 |
||
|
2.
|
Rifampin capsules |
100 mg |
--- |
15.61 |
--- |
0 |
|
150 mg |
21.78 |
17.74 |
4.04 |
22.78 |
||
|
300 mg |
47.03 |
30.13 |
16.9 |
56.09 |
||
|
450 mg |
68.93 |
19.23 |
49.7 |
258.45 |
||
|
600 mg |
92.5 |
54.27 |
38.23 |
70.44 |
||
|
Rifampin tablet |
300 mg |
--- |
47.43 |
--- |
0 |
|
|
450 mg |
68.93 |
47.65 |
21.31 |
44.66 |
||
|
600 mg |
--- |
92.50 |
--- |
0 |
||
|
3. |
Pyrazinamide tablet |
250 mg |
29.60 |
26.90 |
2.7 |
10.04 |
|
300 mg |
--- |
32.56 |
--- |
0 |
||
|
500 mg |
52.54 |
35.30 |
17.24 |
48.84 |
||
|
750 mg |
86.87 |
26.76 |
60.11 |
224.63 |
||
|
1000 mg |
105.50 |
35.42 |
70.80 |
197.85 |
||
|
1200 mg |
--- |
115 |
--- |
0 |
||
|
1500 mg |
--- |
113.40 |
--- |
0 |
||
|
4. |
Ethambutol tablet |
200 mg |
11.11 |
3.92 |
7.19 |
183.42 |
|
400 mg |
41.25 |
7.18 |
34.07 |
474.51 |
||
|
600 mg |
39.84 |
20.25 |
19.59 |
96.74 |
||
|
800 mg |
57.75 |
13.69 |
44.06 |
321.84 |
||
|
1000 mg |
66.16 |
55.68 |
10.48 |
18.82 |
||
|
5. |
Ethionamide tablet |
250 mg |
138.50 |
107 |
31.5 |
29.44 |
|
6. |
Prothionamide tablet |
250 mg |
--- |
149 |
--- |
0 |
|
7. |
Cycloserine capsule |
250 mg |
485 |
100.08 |
384.92 |
384.61 |
|
|
Tablet |
250 mg |
416.25 |
416.25 |
0 |
--- |
Table 2: Cost variation of various anti- TB fixed dose combination in India
|
Sr. no. |
Fixed dose combination |
Dose |
Maximum cost (INR) |
Minimum cost (INR) |
Cost Difference |
% cost variation |
|
1. |
Isoniazid |
300mg+800mg |
69.87 |
30.7 |
39.17 |
127.59 |
|
2. |
Isoniazid + Rifampin |
30mg + 60mg |
--- |
9.62 |
--- |
0 |
|
50mg+ 100mg |
15.43 |
12.97 |
2.46 |
18.97 |
||
|
75mg+ 150mg |
19.20 |
18.53 |
0.67 |
3.62 |
||
|
100mg+100mg |
15.31 |
12.12 |
3.19 |
26.32 |
||
|
100mg+ 150mg |
--- |
19.17 |
--- |
0 |
||
|
150mg+ 300mg |
49.50 |
34.18 |
15.35 |
44.82 |
||
|
225mg+450mg |
69.50 |
51.23 |
13.27 |
35.66 |
||
|
300mg+450mg |
67.74 |
37 |
30.74 |
83.08 |
||
|
300mg+ 600mg |
77.17 |
56.8 |
20.37 |
35.36 |
||
|
3. |
Rifampin+ Isoniazid+ Ethambutol |
150mg+75mg+275mg |
39.90 |
28.73 |
11.17 |
38.88 |
|
150mg+100mg+275mg |
--- |
34.75 |
--- |
0 |
||
|
150mg+275mg+275mg |
--- |
30.78 |
--- |
0 |
||
|
150mg+300mg+550mg |
74.50 |
57.64 |
16.84 |
29.25 |
||
|
450mg+225mg+550mg |
--- |
86.43 |
--- |
0 |
||
|
450mg+225mg+825mg |
--- |
102 |
--- |
0 |
||
|
450mg+300mg+800mg |
95.75 |
43.35 |
52.4 |
120.88 |
||
|
4. |
Rifampin+ Isoniazid+ Pyrazinamide |
60mg+30mg+150mg |
--- |
13.72 |
--- |
0 |
|
100mg+50mg+300mg |
--- |
24.60 |
--- |
0 |
||
|
120mg+80mg+250mg |
30.09 |
29.90 |
0.19 |
0.64 |
||
|
150mg+100mg+375mg |
--- |
42.25 |
--- |
0 |
||
|
150mg+75mg+400mg |
30.58 |
30.53 |
0.05 |
0.16 |
||
|
150mg+100mg+500mg |
53.60 |
34.17 |
19.49 |
58.86 |
||
|
225mg+150mg+750mg |
51.76 |
49.40 |
2.36 |
4.78 |
||
|
450mg+300mg+750mg |
--- |
161.10 |
--- |
0 |
||
|
450mg+300mg+1500mg |
162.70 |
149.50 |
13.2 |
8.83 |
||
|
5. |
Rifampin+ Isoniazid+ Pyrazinamide + Ethambutol
|
150mg+75mg+400mg+275mg |
47 |
29.23 |
17.77 |
61.07 |
|
150mg+100mg+500mg+275mg |
51 |
48.07 |
2.93 |
6.10 |
||
|
225mg+150mg+750mg+400mg |
71 |
62.23 |
1.14 |
14.09 |
||
|
450mg+300mg+750mg+400mg |
147.90 |
44.45 |
3.33 |
232.73 |
||
|
450mg+300mg+1500mg+ 1800 mg |
185.40 |
77.32 |
107.80 |
71.99 |
||
|
600mg+300mg+800mg+1100 mg |
--- |
--- |
164.80 |
0 |
||
|
450mg+225mg+1200mg+825mg |
--- |
--- |
37.26 |
0 |
Cost Breakdown
Direct Costs:
?Medication:
First-line anti-TB drugs: 5,000 - 10,000 (approximately $65-$130 USD) per patient per year.
Second-line anti-TB drugs: 50,000 - 100,000 (approximately $650-$1,300 USD) per patient per year
?Diagnostic tests:
Chest X-ray: 500 - 1,000 (approximately $6.50-$13 USD)
Sputum smear microscopy: 200 - 500 (approximately $2.60-$6.50 USD)
GeneXpert MTB/RIF: 2,000 - 5,000 (approximately $26-$65 USD) [15]
? Hospitalization:
Average cost per hospitalization: 20,000 - 50,000 (approximately $260-$650
USD)
? Outpatient visits:
Average cost per visit: 500 - 1,000 (approximately $6.50-$13 USD)
Indirect Costs:
?Lost productivity:
Average daily wage loss: 200- 500 (approximately $2.60-$6.50 USD)
Total lost productivity: 72,000- 180,000 (approximately $930-$2,340 USD) per patient per year
?Travel expenses: Average travel cost per visit: 500- 1,000 (approximately $6.50-$13 USD)
?Total travel expenses: 10,000- 20,000 (approximately $130-$260 USD) per patient per year
?Total indirect costs: 82,000- 200,000 (approximately $1,060-$2,600 USD) per patient per year.
Total Costs:
Direct costs: 73,200 - 211,000 (approximately $950-$2,700 USD) per patient per year Indirect costs: 82,000 - 200,000 (approximately $1,060-$2,600 USD) per patient per year Total costs: 155,200 - 411,000 (approximately $2,010-$5,300 USD) per patient per year.[16]
Factors Contributing to Cost Variations:
Healthcare System Structure: The structure of a country's healthcare system, including the role of private and public providers, can significantly impact treatment costs.
Medication Costs: The cost of TB medications varies across countries, with some countries facing challenges in accessing affordable medicines.
Diagnostic and Hospitalization Costs: Diagnostic tests and hospitalization costs can also contribute to overall treatment costs.
Examples of Country-Specific Costs: India: The cost of TB treatment in India ranges from 5,000 to 10,000 (approximately $65-$130 USD) per patient per year for medication, and 20,000 to 50,000 (approximately $260-$650 USD) per patient for hospitalization.
Other Countries: Similar cost variations exist in other low- and middle-income countries, such as South Africa and Indonesia.
It's essential to consider these cost variations when developing policies and programs to address TB treatment in low- and middle-income countries. By understanding the local healthcare context and cost structures, policymakers can create more effective and affordable treatment strategies.[17]
Cost Comparison of standard 6-month regimen and newer 4-month regimen:
Comparing the costs of standard 6-month regimens and newer 4-month regimens for tuberculosis treatment in India is crucial for understanding the financial implications of these treatments.
The estimated direct costs of treating pulmonary tuberculosis with the 4-month and 6month regimens in the United States are similar, around $23,000 per person. However, this data may not be directly applicable to India.
In India, the costs would likely be lower due to differences in healthcare systems and medication prices. A study published in the Emerging Infectious Disease journal estimated that the cost of TB treatment in India ranges from 5,000 to 10,000 (approximately $65-$130 USD) per patient per year for medication, and 20,000 to 50,000 (approximately $260-$650 USD) per patient for hospitalization.
?Differences in Drug Prices:
The 4-month regimen uses rifapentine and moxifloxacin, which are more expensive than the drugs used in the 6-month regimen. However, the 4-month regimen requires fewer doses, which could offset the higher drug costs.
?Treatment Outcomes:
Research shows that the 4-month regimen has similar success and safety rates as the 6-month regimen in producing favourable TB outcomes. The shorter treatment duration may reduce healthcare engagement and societal costs associated with lost productivity.[18]
CONCLUSION:
The review on the variation of costs among anti-tuberculosis drugs highlights significant disparities influenced by factors such as production methods, market competition, and regulatory environments. It concludes that addressing these cost variations is crucial for improving access to effective treatment, particularly in low-income regions. Additionally, the review emphasizes the need for policy interventions to standardize pricing and encourage equitable distribution of these essential medications. Overall, a multifaceted approach is necessary to ensure affordability and accessibility for all patients requiring anti-tuberculosis therapy.
REFERENCES


Riya Batra*, S. J. Dighade, Review On Variation of Cost Among Anti-Tuberculosis Drugs, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5254-5263. https://doi.org/10.5281/zenodo.15754556
 10.5281/zenodo.15754556
10.5281/zenodo.15754556
