Gajanan Maharaj College of Pharmacy, Chh. Sambhajinagar.
Hyperacidity, is refers to as the excessive stomach acid, occurs when the stomach produces an abnormal amount of acid, often leading to symptoms such as heartburn, indigestion, and gastric discomfort. Common causes include diet, stress, smoking, and certain medications. Chronic hyperacidity can result in complications like gastro-esophageal reflux disease (GERD) and peptic ulcers. Management typically involves lifestyle modifications, dietary changes, and medications like antacids, proton pump inhibitors, or H2 blockers to reduce acid production and develop symptoms. Understanding hyperacidity is crucial for effective prevention and treatment. The excessive gastric acid production leads to symptoms such as heartburn, indigestion, and discomfort.
The term hyperacidity refers to the excess secretion of hydrochloric acid in the stomach. Hyperacidity simply means an increased level of acid in the stomach. The stomach secretes hydrochloric acid, a digestive juice that breaks down food particles into their smallest form to aid digestion. When there is an increase in the secretion of hydrochloric acid by the cells in the lining of our stomach, it is known as hyperacidity.
Hyperacidity also known as acid reflux or gastroesophageal reflux disease (GERD) occurs when stomach acid frequently flows back to the oesophagus. This backflow of acid in stomach can irritate the lining of the oesophagus, causing discomfort and potentially leading to more serious health issues if left untreated. Untreated hyperacidity may lead to gastroesophageal reflux disease (GERD). Hyperacidity is also called Acid Dyspepsia which is one of the most common problems. Hyperacidity is a medical condition in which the stomach secretes a lot of acids. The excessive production of acid by the stomach, leads to the back flow into the food pipe and causes pain or sensation in the lower chest area. Unhealthy lifestyle is responsible for acidity in individuals. This condition can be uncomfortable and may lead to more serious health problems if left untreated.
Causes: As the food particles moves down into the stomach through food pipe or oesophagus, the stomach gastric glands produces the acid necessary to digest the food. In some conditions the gastric glands produce a large amount of acid, than usual to complete the digestion process, this results in the excess acid production and the burning sensation and leads to cidity.
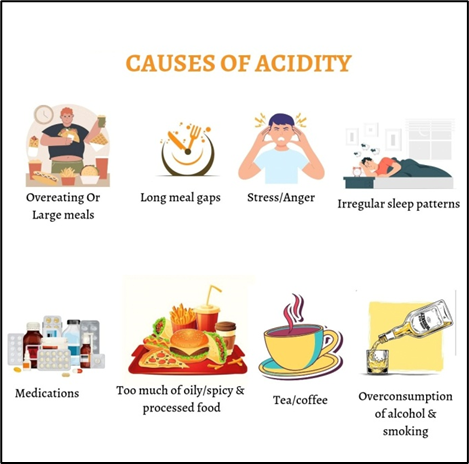
The main causes of the acidity are:
Symptoms: - These are the common acidity symptoms, and they may also vary according to the diet followed by an individual. Acidity can be easily cured by taking certain medicines to reduce the excessive production of acid in the stomach.
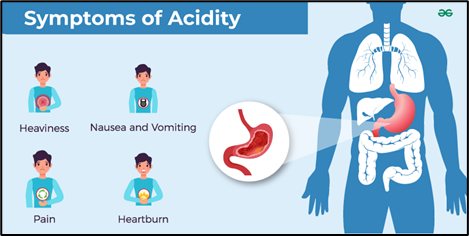
The main symptoms of acidity:
Mechanism of acid secretion:

Gastric acid is colorless, watery, acidic, digestive fluid produced in the stomach. The gastric secretions is produced by the epithelium cells of the gastric glands. A typical adult human stomach will secrete about 1.5 liters of gastric juice daily. Gastric juice is the combination of gastric gland secretions which includes the main components such as hydrochloric acid (gastric acid), gastric lipase and pepsinogen. Gastric juice consists of (HCl, Electrolytes, mucus, bicarbonates, pepsins, lipases, ghrelin). The hydrochloric acid is among the digestive juices which help in the digestion of food. Hcl or hydrochloric acid is produced by the parietal cells of the stomach. The process of HCl production starts with water (H2O) and carbon dioxide (CO2) combine within the parietal cell cytoplasm to produce carbonic acid (H2CO3) which is catalysed by carbonic anhydrase. Carbonic acid then dissociates into a hydrogen ion (H+) and bicarbonate ion (HCO3-). The hydrogen ion that is formed is transported into the stomach lumen via the H+ - K+ ATPase ion pump. This pump uses ATP as an energy source to exchange potassium ions into the parietal cells of the stomach with H+ ions. The bicarbonate ion is transported out of the cells into the blood via a transporter protein called anion exchanger which transports the bicarbonate ion out the cell in exchange for a chloride ion (Cl-). This chloride ion is then transported into the stomach lumen via a chloride channel. This results in both hydrogen and chloride ions are present within the stomach lumen. Their opposite charges leads to them associating with each other to form hydrochloric acid (HCl).
Phases of gastric secretion: Namely there are three interrelated phases: cephalic, gastric, and intestinal.
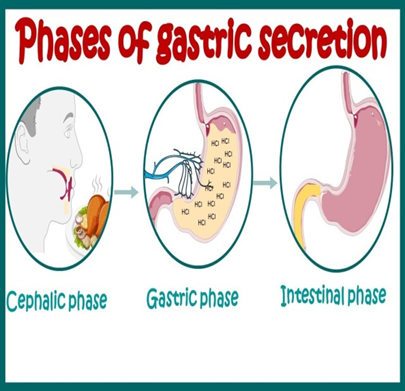
Cephalic phase (30%): This phase is responsible for 20-30% of the total acid secretion. Gastric phase (60%): This phase is triggered by the arrival of food in the stomach. This phase is responsible for 50-60% of the total acid secretion. Intestinal phase (10%): Intestinal phase is a small proportion phase which secretes small amount of acid secretory response to a meal.
Physiology of acid secretion:
Gastric secretion: the secretion of gastric juices arises from the glands in the wall of the stomach, and drain into its lumen. Surface cells – secrets mostly mucus & bicarbonate. Mucous and HCO3 protects stomach mucosa. Two different cells: Parietal cells: HCL, intrinsic factor. Chief cells, pepsinogen + gastric lipase. The epithelium cells also produce important hormones gastrin a peptide that is important in control of acid secretion and gastric motility and somatostatin. G cells: Gastrin (hormone) – HCl secretion. D cell: somatostatin (antrum). Enterochromaffin-like cell: Histamine.
Composition of and function of gastric secretions:
HCL:
Mucus
Pepsinogen
Intrinsic factor: Combines with vitamin B12 to make it absorbable.
Risk factor for hyperacidity:
Lifestyle: Smoking, excessive alcohol consumption, and high stress levels can increase stomach acid production.
Diet: Eating large meals, eating late at night, eating spicy, fatty, or acidic foods can trigger acid reflux.
Medication: Taking certain drugs, like aspirin or ibuprofen, can irritate the stomach acid production can also lead to rebound high stomach acid.
Other conditions: Genetics
Hiatal hernia, pylori infection, and pregnancy can also cause acid reflux.
Natural ways to cure acidity:
Banana: Bananas are extremely beneficial for gut and stomach health due to their high fiber content, which improves the digestive process. A ripe banana is a perfect antidote to sever heartburn.
Cold milk: That calcium is also one of the main ingredients in your over-the counter antacids Calcium helps to maintain the Ph balance and aids in proper digestion.
Fennel seeds: Fennel seeds function as an effective natural remedy for indigestion, acidity, and acid reflux.
Tulsi: Basil leaves or tulsi, as we them better, stimulate our stomach to produce more mucus which in turn helps to relieve heartburn and nausea that often occurs with acidity.
Drugs used in the treatment of acidity: Drugs such as (Omeprazole, Pantoprazole, Rabeprazole, Lansoprazole) are PPIs which are acts as proton pump inhibitors. Inhibit the H+/K+-ATPase gastric pump. H2 antagonist such as (Cimetidine, Ranitidine, Famotidine).
Proton pump inhibitors: The classes of drugs used in the treatment of acidity are PPIs proton pump inhibitor are widely used. they are effective in the treatment of acidity. They relieve the symptoms of acidity and also reduces the risk factor associated with it.These drugs inhibit the secretion of acid by inhibiting the H+/K+ proton pump which exchanges the ions and leads to formation of HCl.

Figure: 1
Adverse drug reactions:
Hypomagnesaemia, Infection, Vitamin Deficiency.
Contraindications: PPI contraindications include patients with known hypersensitivity to that class of drugs, and their use requires caution in patients with severe hepatic disease.
CONCLUSION:
Hyperacidity, or excessive stomach acid, can lead to various digestive issues, including heartburn, indigestion, and gastric ulcers. Effective management often involves lifestyle changes, dietary adjustments, and medications such as antacids or proton pump inhibitors. Long-term hyperacidity can increase the risk of more serious conditions, such as gastro-esophageal diseases, gastrointestinal disorders. So it’s important to seek medical advice if symptoms persist. Maintaining a balanced diet, managing stress, and avoiding trigger foods can help alleviate symptoms and promote digestive health. Regular check-ups with a healthcare provider are advisable for ongoing issues.
REFERENCES



Komal Chavan, Dr. Kavita Kulkarni, Madhavi Kakphale*, Review Article On Hyperacidity, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 10, 1192-1197. https://doi.org/10.5281/zenodo.13960963
 10.5281/zenodo.13960963
10.5281/zenodo.13960963
