IPS Academy College of Pharmacy, Rajendra Nagar, A.B. Road, Indore, Madhya Pradesh, India 452012
Background: Most doctors learn new things through artificial intelligence. This is owing to the fact that it contains a lot of medical data and high computing capabilities. This mixture has altered how researchers are thinking about novel concepts within the health sector. The impact of artificial intelligence on respiratory medicine is large as the diseases are so complex and the ways of diagnosing them are numerous. This review examines the current use of AI in the treatment of breathing issues, but will specifically focus on the massive transformations that have occurred since 2021. It clearly gives out what should be done in this field. The paper only explores the main developments and future innovations in AI technology that are relevant to respiratory diseases. Recent Trends: The treatment of respiratory problems is one of the sectors Artificial Intelligence is performing quite well as of now. It is a technology that aids doctors to maintain the lungs of their patients. Recent research results indicate that deep learning algorithms such as convolutional neural networks (CNNs) can identify lung nodules with relative precision as doctors. Such technologies could potentially determine the severity of an illness of a patient by examining the chest x-rays, similar to physicians. It has been established that these algorithms can determine the severity of bad lung diseases such as COVID-19 and emphysema. Tests of lung functioning are being enhanced by artificial intelligence that collects data on its own and verifies that it is accurate. It may monitor the patients through observing their cough and breathing sounds such as non-invasive diagnostic tests. Future Prospects: Artificial intelligence would be a great relief to individuals experiencing difficulty in respiration. It will assist us to create smarter and better systems that are compatible with each other. The digital twins are the simulated versions of the ailing individuals who are not real. They allow carrying out computer simulation of clinical trials and creating a highly personalized treatment plan with each patient. The AI can enhance therapies by simplifying the procedure of robotic bronchoscopy and simplifying the process of ventilating critically ill patients in real time. Individual and preventive respiratory therapy could be given to people, which could include various forms of data used, such as genetic, imaging, and real-world sensor data, which would allow us to fully comprehend diseases.
The respiratory system in human body is a complex and a significant connection between the body and the external environment. People are also seriously weak in this aspect. The exposure to different particles, viruses, and allergens is increased over a long period leading to the probability of disease acquisition which can be both chronic and debilitating and life-threatening in a short-term. Respiratory diseases are a serious issue of 21st century health problems [1]. Their power is impressive indeed. COPD is a progressive disease which is largely irreversible and chronic. It has now been identified to rank as the third largest cause of death in the world. Asthma is a long-term inflammatory illness, which is present in approximately 262 million people and causes a great deal of stress not only to children but also to adults. The worldwide cancer-related mortality is lung cancer, which is characterized by a very low five-year survival rate that is mainly because of its late diagnosis. The fact that acute infections are a constant threat worsens a continuing problem because they could be seasonal flu and bacterial pneumonia or novel viruses. The current COVID-19 pandemic is one of the best examples [2].
The modern pulmonologist has his arsenal based on the methods that have proven to be effective as there has been much need to utilize them. The subjective ones are clinical history and physical examination, which are crucial. Pulmonary function tests (PFTs) and chest imaging have traditionally been clinically applied by physicians to make fair decisions concerning patients. The spirometry examination is the most common way of pulmonary examination. It reveals much on the hindrance of airflow. This therapy group is worrying about some issues. These vital tests complicate the treatment of patients. Patients also have a considerable effect on pulmonary tests of function and any slight variations in coaching or performance can cause ambiguity. Those who interpret pulmonary function tests occasionally use inflexible and population-specific standards which are not always relevant to the intricacies of the situation experienced by an individual [3].
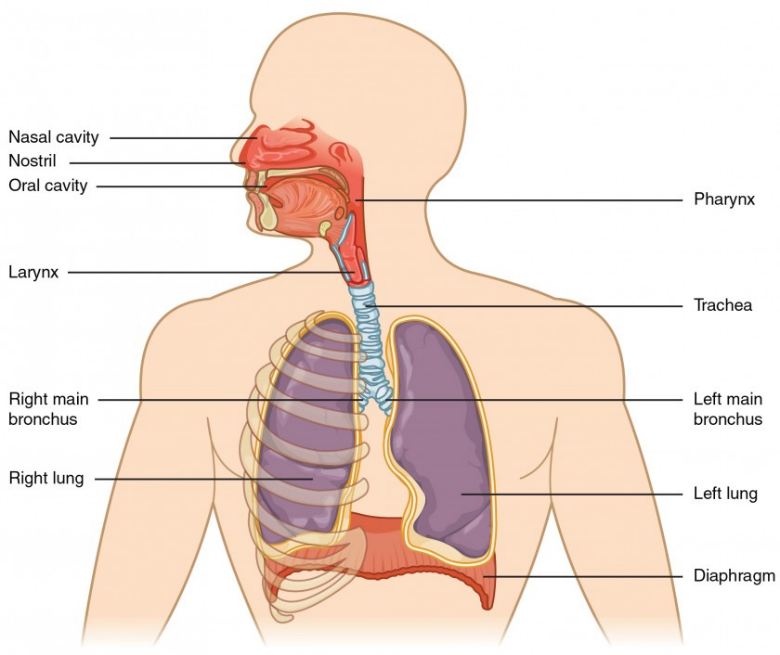
Fig. No. 1: Human Respiratory System
Thoracic imaging, especially the analysis of sophisticated HRCT images of pathology such as Interstitial Lung Disease (ILD), has been recognised to have high inter and intra-observer variability, even in the experienced radiologist. Such ambiguity goes beyond being a statistical problem; it also has serious implications on therapy causing delays in diagnosis, wrong diagnosis of a disease and inaccurate assessment of treatment effectiveness. Many people are sick in this scenario, and even the routine diagnostic is not very productive. The digital revolution has revolutionized health care in such a way that can change everything. Biological data have been greatly enhanced in the past ten years through its acquisition. People cannot examine data on their own because of the large size and complexity. There is a great power enhancement in computers. This is the best place where AI can develop [4].
AI, particularly, machine learning and deep learning, is a major change in the process of reasoning by humans to reasoning based on data. These algorithms are able to detect trends in huge volumes of data that is complicated and cannot be recognized by humans. This ability is not merely a promise of the future, but it is improving medicine. AI has been effective at detecting dermatological and ophthalmological disorders using pictures. They have in a number of occasions proven to be more accurate than experts in that field [5].
2. RECENT TRENDS: THE BROADENING SPECTRUM OF AI APPLICATIONS
Pulmonology's use of artificial intelligence has grown quickly from a small part of medicine to a big and important one. There was a clear change from simple proof-of-concept models to more advanced algorithms. A lot of places are testing these algorithms right now, and in many cases, they are already being used in hospitals. The level of maturity differs from place to place, and it is more noticeable in places where data is easy to get to, technology is advanced, and certain therapeutic needs encourage new ideas. This part gives a full picture of how things work right now, starting with the basics and then looking at how they help sick people [5].
Foundational AI Methodologies in Pulmonology
To appreciate the recent trends, one must first understand the primary AI engines driving them. While many algorithms exist, the field is overwhelmingly dominated by three core architectures of deep learning, each uniquely suited to a different type of respiratory data.
Monitored Learning: This is the predominant method wherein models are trained using labeled data sets. Models including thousands of CT images will be provided. This is referred to as a "malignant node" or "benign knot," which categorizes fresh imperceptible scans. Support Vector Machines (SVMs), Random Forests, and Convolutional Neural Networks (CNNs) are techniques employed for classification (presence/absence) and regression (e.g., forecasting lung function values) [6].
Difficult Learning: Even without data, these algorithms might be able to find patterns or structures that aren't obvious. Clustering algorithms can look at large groups of patients and use a number of factors, like imaging and clinical genetics, to find diseases like asthma and COPD. This is essential for the progress of personalized treatment [7].
Deep Learning: The "deep" MLS subgroup is made up of artificial neural networks with many layers.
Convolutional Neural Networks (CNNs): The most important part of medical image analysis. The structure of a CNN is based on the human visual cortex, and it learns from pixel input in a way that reinforces itself. The main parts, called "convolutional filters," can find many different kinds of features. These filters learn to find important things like edges and textures in the first layers. As input moves deeper into the network, it combines these basic features to find more complex structures, like the unique texture of a ground-glass opacity or the spiculated border of a malignant nodule [8]. Convolutional Neural Networks (CNNs) can find nodules, sort diseases like COVID-19 and bacterial pneumonia, and, most importantly, do "segmentation," which means separating structures like the lungs, airways, or fibrotic tissue at the pixel level [9,10]. This happens when they learn things gradually, moving from "pixel" to "concept" on their own.
Recurrent Neural Networks (RNNs) and Long Short-Term Memory (LSTM) Networks:
RNNs are better at analyzing time, while CNNs are better at analyzing space.
These models are specifically engineered to handle sequential data, featuring an integrated "memory" that allows information from previous stages in a sequence to influence the current step. In pulmonology, this makes them the best tool for understanding data over time. Recent applications of notable efficacy include the analysis of acoustic data, such as the classification of coughs and the detection of wheezing in continuous audio streams.
RNNs, along with the more advanced Long Short-Term Memory (LSTM), are also used to predict when things will get worse. By examining time-series data from a patient's digital inhaler, wearable sensor (tracking respiratory rate or oxygen levels), or daily symptom diary, a recurrent neural network (RNN) can identify the subtle, sequential patterns of physiological decline that often precede a significant exacerbation of COPD or asthma, thus facilitating proactive intervention [11].
The newest and possibly most powerful architecture, have completely changed the field of natural language processing (NLP) and are now being quickly adapted for use in medicine and vision. Their strength lies in a technique called "self-attention," which lets the model look at the importance of all parts of an input sequence (or picture) at the same time, instead of one at a time like an RNN does.
This extensive understanding facilitates the detection of complex, long-range interactions within the data. Vision Transformers (ViT) are beginning to compete with CNNs in the field of respiratory medicine. For instance, in the complex field of "radiogenomics"—the prediction of a tumor's genetic mutations from its CT image, a ViT can concurrently analyze the entire 3D tumor volume, identifying correlations between textures in one area of the nodule and its periphery in another, indicating potential superiority over traditional CNNs in forecasting EGFR mutation status [12,13].
Deep Dive into AI in Thoracic Imaging
Thoracic imaging remains the area of best AI impact.
Lung Cancer: AI`s role has multiplied beyond smooth nodule detection.
The primary issue with low-dose CT (LDCT) lung cancer screening is not the detection of nodules, but the exceedingly high false-positive rate, resulting in additional scans and increased stress for patients. This is the area where modern AI models have come the farthest.
The first models were made to be sensitive to the level of a radiologist, but the newest algorithms are made to be specific. A major multi-center validation study published in Radiology in 2025 found that a deep learning algorithm cut down on false positives by a lot compared to the PanCan model that was already being used.
The AI tool could find cancers with 100% accuracy in a year.The PanCan model only put 47.4% of benign nodules in the low-risk group, but the other model put 68.1% of them there. This led to a 40% relative drop in false positives. The change from "Can AI identify cancer?" to "Can AI reliably exclude non-cancer?" is a big step forward in making national screening systems more useful and less expensive [14, 15].
AI is now working on the more difficult task of not only finding the indeterminate pulmonary nodule (IPN) but also describing it. AI systems can now give a very accurate malignancy risk score by using 3D CNNs and models that have been trained on large, publicly available datasets like the Lung Image Database Consortium (LIDC-IDRI).
These models assess a nodule's internal and external attributes in comprehensive 3D, including density, texture, border irregularity, and temporal growth (when historical data is available), often achieving an area under the curve (AUC) exceeding 0.90 in differentiating benign from malignant nodules—a performance comparable to or surpassing that of expert thoracic radiologists [16].
Radiogenomics is the most recent trend. It uses AI to figure out the genetic traits of a tumor just by looking at pictures.
This is a way to get enough tissue for genetic testing without hurting anyone, which is a big problem. Recent research from 2023 and 2024 suggests that "fusion models," which combine deep learning elements from a CNN or Vision Transformer with manually created "radiomic" features, may effectively predict the mutation status of essential driver genes like EGFR.
A study that predicted EGFR status in 2024 had an AUC of 0.910, which was better than models that only used radiomics or deep learning. This suggests a future use where a standard diagnostic CT scan could quickly tell the doctor how likely it is that there is a targetable mutation, which could speed up patients' access to the best biologic therapies [17].
Fig. No. 2: Unveiling The Chronic Diseases
COPD and Asthma: AI is permitting quantitative assessment of structural changes withinside the lungs.
Quantitative CT (qCT): Artificial intelligence has made the complicated process of quantitative computed tomography (qCT) easier. Deep learning models, especially U-Net architectures (a type of CNN), can accurately and effectively divide the lung parenchyma into parts. It is possible to find out the LAA%, which is a good way to tell how bad emphysema is. At the same time, these models may show the bronchial tree in the lung and measure the airway wall thickness (AWT) and lumen diameter. This gives two important, objective biomarkers; one that indicates parenchymal disease (emphysema), and the other that indicates airway-based disease (chronic bronchitis), a more comprehensive patient profile as compared to an individual spirometry examination [18].
Integrating Imaging and Physiology:
The latest superior models are now integrating structure and function. The authors have been able to use 3D CNNs to regress the FEV1, a key pulmonary function test finding, of a patient based on the CT image of their chest. This is exemplified in a 2024 study that achieved a high concordance correlation coefficient (CCC) of 0.91 indicating that there is a high level of correlation between the prediction of the image and the actual test of spirometry of the patient by the AI. This can be put into practice with serious consequences: opportunistic screening of COPD by any CT of the chest that is ordered in other cases (e.g. in the emergency Department), the identification of patients with physiological abnormalities that are not detected by routine tests, and a functional estimation of patients too ill to do spirometry [19].
In this area, artificial Interstitial Lung Diseases (ILDs): Interstitial lung diseases pose serious diagnostic problem of pulmonology because of their complexity and overlapping characteristics of imaging. intelligence is becoming a relevant means of getting things more objective and repeatable.
A study published in 2025 emphasized that quantification of HRCT based on AI (AIqpHRCT) should be used in patients with ILD due to connective tissue disease. The reason is that such objective percentage-based measures provide a more realistic image of the badness of the disease as compared to subjective visual assessment. This plays a crucial role in the process of diagnosis as well as ensuring that all the patients are treated to the same standards. It is also quite significant in determining the effectiveness of new anti-fibrotic drugs in clinical trials [20].
Artificial intelligence is also used to predict what will happen in the future. AI models can now predict the risk of death or rapid progression of a patient with Idiopathic Pulmonary Fibrosis (IPF) by analyzing their baseline HRCT scan over the subsequent one to two years. Prognostic models that combine clinical data like age and pulmonary function tests with imaging characteristics could help doctors find patients who are at high risk and may need treatment sooner, more aggressively, or a referral for a lung transplant. Also, AI can use serial CT scans to accurately measure changes in fibrosis over time. This makes it a more sensitive biomarker for disease progression than the yearly drop in Forced Vital Capacity (FVC) [21].
Infectious Diseases: The COVID-19 pandemic sped up the process of coming up with new ideas. AI models were enhanced to independently evaluate a severity score or "percentage of lung involvement" from CT images. There was a strong link between this score and clinical outcomes and the need for mechanical ventilation [10,22]. This artwork is now used to make it easier to evaluate and measure bacterial pneumonia and TB, especially in places where resources are limited [23].
AI in Physiological and Functional Assessment
Enhancing Pulmonary Function Tests (PFTs): Spirometry, the most common pulmonary function test (PFT), depends a lot on the patient's effort and guidance, which leads to a lot of results that can't be repeated or are not what the patient wanted. AI models are now being added directly to spirometry systems to make sure that the quality is always good. The AI may look at the shape of the flow-volume loop while the patient is doing the maneuver and give the technician real-time feedback, such as "Increase blowing speed" or "Avoid premature cessation," to help the patient pass the test according to American Thoracic Society (ATS) standards. This simple use of AI has the potential to greatly improve the quality and dependability of PFT data around the world [24].
The Rise of Acoustic Biomarkers: The field of AI-enhanced respiratory sound analysis is growing quickly. AI systems that have been trained on large sets of recorded lung sounds can accurately tell the difference between wheezes, crackles, and rhonchi. Smartphone apps that use similar algorithms are being made to be cheap ways to screen for COPD, pneumonia, and asthma by using cough and breath sounds as digital biomarkers [25, 26].
Precision Phenotyping and Chronic Disease Management
Unsupervised Learning to Discover Novel Phenotypes:
Asthma and COPD are very different from each other. Individuals diagnosed with COPD may exhibit significantly different underlying biological conditions (e.g., emphysema-dominant versus chronic bronchitis-dominant) and may respond variably to identical therapeutic regimens. Researchers can now find new, data-driven patient subgroups by using unsupervised machine learning methods like clustering algorithms on large, high-dimensional datasets that combine clinical data, pulmonary function tests, biomarkers, and quantitative computed tomography characteristics. These "phenotypes" or "endotypes" show more biological uniformity. This methodology has enabled the identification of distinct patient cohorts in severe asthma, such as "Th2-high" and "neutrophilic," which demonstrate diverse responses to specific biologic therapies, thereby promoting a "treatable traits" paradigm in medicine [27,28].
Predictive Analytics for Exacerbations: The main goal of managing chronic respiratory conditions is to reduce acute exacerbations. Artificial intelligence is now in charge of this project through predictive models. These models work like advanced early warning systems. An RNN or LSTM model can figure out a patient's unique "baseline" and spot small changes that could mean an exacerbation is coming by putting together different real-time data streams. These streams could include daily symptom reports from a smartphone app, rescue inhaler use from a "smart" inhaler, and physiological metrics (like heart rate, sleep disturbances, and respiratory rate) from a wrist-worn device (18,44,65). A study conducted in 2025 demonstrated that data from digital inhalers can be utilized by a machine learning algorithm to accurately predict COPD exacerbations within a five-day timeframe. This is a great chance for a "push" message to the patient or a direct alert to their healthcare team. This could lead to preemptive therapy (like steroids) that could keep the patient from having to go to the hospital, which would be very expensive and dangerous [29,30].
Predicting Treatment Response: In the end, AI is helping to answer one of the hardest questions in medicine: "What is the right treatment for this patient?" Models are being made now to guess how a patient will probably respond to a certain drug. Artificial intelligence (AI) models are looking at CT scans and digital pathology slides of lung cancer patients before they start treatment to try to figure out who is most likely to benefit from expensive immunotherapy. This is a difficult task to do right now. At the same time, research is being done to make models that can predict which type of inhaler (e.g., LAMA, LABA, or a combination) would give a certain COPD patient the biggest boost in FEV1, which will help us get closer to truly personalized respiratory treatment [31,32].
3. FUTURE PROSPECTS: THE NEXT FRONTIER OF AI IN RESPIRATORY CARE
These trends are just the start. In the next five to ten years, AI will become even more integrated into clinical practice, changing the focus from managing diseases to predicting and preventing health problems.
Fig. No. 3: AI In Pulmonary
Generative AI and Large Language Models (LLMs)
A lot of things are going to change in respiratory medicine now that powerful LLMs like GPT-4 and Med-PaLM 2 are here.
Digital twins that are able to breathe
When referring to a patient's respiratory system, the term "digital twin" refers to a virtual model that is able to alter over time based on clinical data.
Personalized Simulation: A digital twin might replicate the airflow in a patient's airways in order to determine the most effective method of administering inhalation treatment drugs to the patient. It is also possible that it will demonstrate how a new medication can alter the way in which a person's lungs function before they take it [36].
In the Silico Clinical research: Researchers have the ability to conduct the earliest phases of clinical investigations totally in silico by constructing a cohort of digital twins that accurately match a patient population. In light of this, it is possible that future human studies will be constructed with more ease. In addition to this, it would make it feasible to verify the efficacy and safety of novel medications in a more expedient and cost-effective manner [37].
Interventions in Critical Care That Are Powered by Artificial Intelligence
The function of artificial intelligence will shift from diagnosing patients to deciding how they should be treated.
Bronchoscopy instruments that are robotic can be controlled by artificial intelligence. Artificial intelligence has the potential to create a "GPS" for the lungs by combining live video feeds with CT pictures that were acquired prior to surgery. It is because of this that the pulmonologist is able to locate small peripheral nodules for biopsy in a more straightforward and risk-free manner [38].
Better Management of Ventilators Artificial intelligence systems in intensive care units are able to constantly examine data from patient monitors and mechanical ventilators and make suggestions for adjusting the settings of the ventilator in real time. By doing so, individuals could reduce the amount of time they spend on mechanical ventilation and prevent ventilators from causing damage to their lungs [39].
4. ETHICAL CONSIDERATIONS, ISSUES, AND THE MEANS BY WHICH TO PURSUE THEM
AI has a lot of potential, but it is difficult to bring it from research to everyday clinical application. However, it has much potential.
Concerns Regarding Methods That Are Focused on Data
Data Scarcity and Quality: Although there is a large amount of data available, it is particularly challenging and costly to create datasets that are of high quality, well-organized, and well-annotated. These datasets are required for the training of supervised models.
Because of the variability of the data, it is difficult to develop AI models that are well-suited for use across a variety of healthcare systems. The occurrence of this phenomenon occurs when data from several institutions do not always adhere to the same standards, formats (such as diverse CT scanning methodologies), or patient demographics [40].
Bias in the algorithm: Artificial intelligence algorithms may exacerbate existing health inequities if the training data does not include all individuals. There is a possibility that a model that has been predominantly trained on data from one ethnic group will perform less than optimally when applied to data from other ethnic groups [41].
Concerns Regarding Methods of Technology and Algorithms
A problem with artificial intelligence (XAI) that can be described is referred to as the "black box" problem. The fact that doctors do not always know how deep learning models arrive at their conclusions may cause them to lack trust in these algorithms. When it comes to the emerging field of XAI, the objective is to simplify the process of comprehending the significance of model predictions. An illustration of this would be saliency maps, which display the areas of an image that the artificial intelligence (AI) focused its attention on [42].
Integration with the clinical workflow: An artificial intelligence tool is of no value if it does not be compatible with the way things are done at the clinic. In order to accomplish this, it is necessary to give careful consideration to the ways in which people and computers interact, as well as the procedures for designing user interfaces and connecting with picture archiving and communication systems (PACS) and electronic health records (EHR) [43].
The Structure of the Rules and Ethical Standards
Health Insurance Portability and Accountability Act (HIPAA) in the United States and General Data Protection Regulation (GDPR) in Europe are examples of regulations that must be adhered to in order to ensure the protection of patient privacy and data security in huge patient datasets.
The question of accountability and responsibility arises when an artificial intelligence model provides an incorrect diagnosis. Would it have been possible for the equipment to be utilized by the company, the hospital, or the physician? For the purpose of ensuring that individuals are responsible, there ought to be unambiguous moral and legal laws.
In order to comply with regulatory pathways, artificial intelligence-based medical devices must undergo extensive testing and obtain authorization from regulatory authorities such as the European Medicines Agency (EMA) and the Food and Drug Administration (FDA) of the United States. In order to determine whether or not these complex algorithms are both safe and effective, these groups are constantly revising the rules that govern how to test them [44].
Table 1: Summary Of AI Applications In Respiratory Medicine
|
Area of Application |
Recent Trends |
Future Prospects |
Key AI Techniques |
|
Thoracic Imaging |
Lung nodule detection / classification, ILD pattern recognition & quantification, COVID-19 severity assessment, qCT for COPD. |
Automated comprehensive radiology reports (Generative AI), precision guidance for biopsies (Robotic AI). |
CNNs, Radiomics, Transformers |
|
Physiological Assessment |
Automated spirometry quality control/interpretation, acoustic biomarker analysis (cough/breath sounds). |
Real-time continuous monitoring via wearables, early disease screening in community settings. |
SVMs, RNNs, Signal Processing |
|
Chronic Disease Management |
Phenotyping (asthma, COPD), exacerbation prediction, personalized treatment response prediction. |
Multimodal data integration for holistic patient assessment, "Digital Twins" for in-silico trials. |
Unsupervised Learning, RNNs, Fusion Models |
|
Critical Care & Interventions |
Ventilator parameter optimization, patient deterioration prediction (e.g., ARDS, sepsis). |
AI-guided robotic bronchoscopy, real-time closed-loop ventilator control, predictive analytics for ICU outcomes. |
Reinforcement Learning, LSTMs, Computer Vision |
|
Drug Discovery |
Identification of drug targets, lead compound optimization. |
De novo drug design, personalized drug response prediction at molecular level. |
DL (GANs), QSAR, Molecular Dynamics Simulations |
|
Clinical Decision Support |
Early warning systems for patient deterioration, differential diagnosis assistance. |
Context-aware CDSS, LLM-powered virtual assistants for clinicians and patients. |
Ensemble Models, LLMs, Knowledge Graphs |
5. CONCLUSION
In the realm of respiratory medicine, the incorporation of artificial intelligence represents a significant progress in the discipline. AI has been a great way to make education better, get important medical information from complicated datasets, and make patient care more objective and measurable from 2021 to 2025. AI is changing how doctors do their jobs by making chest scans more accurate and helping them figure out when chronic diseases are likely to get worse. Some technologies that could change how respiratory diseases are treated in a way that is both preventative and proactive are digital twins, AI, generative models, and multimodal data.
We need to make medicines again, find the best treatments for each patient, and help doctors do their jobs better. This will help people get better and deal with the many respiratory diseases that affect people all over the world. This goal will be very hard to reach. Making algorithms and using them fairly in healthcare settings will be hard. To get the most out of this life-changing technology, we need to fix data problems, make AI easier to understand, set clear ethical and legal rules, and make sure it works well in therapy settings. These steps are important, but they are also hard to do. To make sure that AI is used to keep people healthy and happy, data scientists, doctors, engineers, and policymakers all need to work together.
REFERENCES

Anuj Yadav, Dr. Akash Yadav, Dr. Dinesh Kumar Jain, Recent Advances and Future Opportunities in AI for Respiratory Care, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1583-1596. https://doi.org/10.5281/zenodo.18269303
 10.5281/zenodo.18269303
10.5281/zenodo.18269303
