Krishna Foundation`s Jaywant Institute of Pharmacy, Wathar, Karad, Maharashtra 415539
One of the main causes of death, cancer is becoming more common worldwide. Gradually, There are numerous medications on the market to treat different forms of cancer, but none is discovered to be completely safe and effective. The main issue with cancer chemotherapy is the toxicity of the recognized drugs. Nonetheless, the treatment and management of plants and plant-derived products has proven to be both safe and effective of cancers. Nowadays, the majority of cancer medication research focuses on plants and plant-derived natural goods. Natural products have shown promise as anti-cancer agents due to their diverse chemical structures and bioactivity. This review investigates their central role in cancer treatment, focusing on the mechanisms of action and therapeutic benefits. Plants contain bioactive compounds such as flavonoids, alkaloids, terpenoids, and polyphenols, which exhibit various anticancer properties, characteristics. These substances cause apoptosis, prevent cell division and cell cycle progression, and disrupt microtubule formation, affect topoisomerase targets, prevent angiogenesis, alter important signaling pathways, enhance the tumor microenvironment, reverse drug resistance and stimulate immune cells. More research is necessary to fully understand the therapeutic advantages and promising anticancer effects of natural products and growth.
Each of the millions of tiny cells that make up our body is a self-contained living unit. The body's normal cells develop and divide for a while before ceasing to do so. After that, they only procreate when needed to replace damaged or dying cells [1]. Cancer is a disorder of abnormal cell development that causes aberrant cells to invade and destroy healthy tissues. Although cancer has affected humans from the dawn of time, until the nineteenth century, it was an uncommon disease. heart disease is the leading cause of death, with cancer coming in second [2]. The complexity of treating this widespread illness is highlighted by its multifaceted nature, which encompasses a wide range of diseases with unique etiologies, manifestations, and treatment responses [3]. Over 7.8 million people die from the illness each year, making up roughly 13% of all fatalities in 2019. According to the World Health Organization, there were more than 10 million cancer-related deaths worldwide in 2020. At 1.8 million, lung cancer was the leading cause of death, followed by colorectal cancer (916,000), liver cancer (830,000), stomach cancer (769,000), and breast cancer (685,000) [4, 5]. Over 2 million new cases of cancer are expected to occur in the US in 2024, according to an article published by the American Cancer Society. Despite improvements in treatment, cancer remains a serious health concern because it is the second most common cause of death for people under 85 in the United States alone [6]. The United States reported 2041,110 cancer cases and 618,120 cancer-related deaths in 2025. Digestive system cancers accounted for the greatest number of deaths, with 174,520 cases reported [7]. One of the main causes of death and illness in the world, cancer is predicted to affect 21 million people by 2030 due to its steadily rising incidence [8]. Cancer is a genetic disease. The oncogenesis manifestation is one important event in the early stages of tumor formation [9]. Each year, four common cancer types—breast, lung, prostate, and rectum/colon cancer with an unknown etiology—kill millions of people. The current tenet highlights a clear distinction between chemoprevention and cancer chemotherapy. While cancer chemoprevention is the phenomenon of a carcinogenesis intervention by blocking the agents that induce the neoplastic process or preventing the processing of transformed cells to the malignant phenotype using suppressing agents, cancer chemotherapy is the control of the developed disease. Reversing the growth of cancer cells may also be a component of cancer chemoprevention [10]. The complexity of cancer research has always made it difficult. The genetic changes, organs affected, prognosis, and treatment modalities of various cancer types can differ greatly [11]. The type and stage of the disease determine the effectiveness of the various treatment options [12].
1.1 TYPES OF CANCER
It begins with the skin or tissue that envelops the internal organs and glands. The tumor solidifies. prostate carcinoma. cancer of the breast, colon, and lungs [13].
It starts with the body's supporting and binding tissues. It may develop in blood vessels, bone, muscles, cartilage, joints, tendons, nerves, or lymph vessels [14].
Leukemia is one form of blood cancer. It starts when healthy blood cells undergo abnormal changes and uncontrollably multiply. Acute myeloid leukemia, acute lymphocytic leukemia, chronic myeloid leukemia, and chronic lymphocytic leukemia are its four subtypes [15].
The lymphatic system, a network of glands and tubes that aids in the body's defense against infection, is the source of lymphamic cancer. lymphomas that are Hodgkin and those that are not [15].
Plasma cells are another type of immune cell that can develop into multiple myelomas. Bone malignancies are caused by the accumulation of myeloma cells, also called plasma cells, in the bone marrow. Plasma cell myeloma and Kahler disease are the names given to it [16].
It begins in the progenitor cells of melanocytes. Melanin, the pigment that gives skin its color, is produced by these specialized cells. Melanomas can develop in other pigmented tissues, like the eye, even though they typically appear on the skin [17].
2. PATHOPHYSIOLOGY
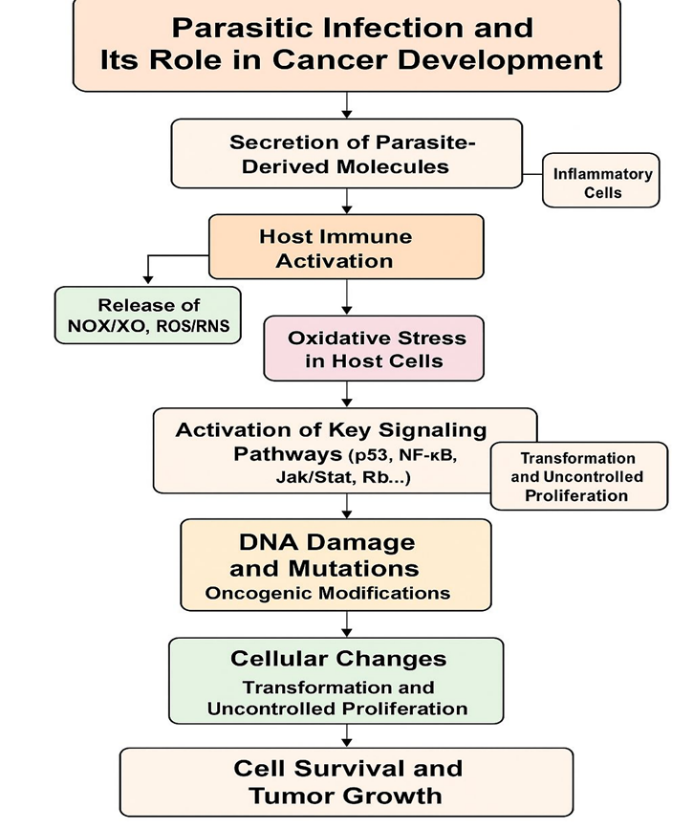
FIG 3.1. Diagramatic Representation of Pathophysiology of Cancer [20].
Cancer frequently affects several organs due to unchecked cell invasion, migration, and division. Understanding its pathophysiology is crucial given the rising number of cases and the drawbacks of traditional treatment options, which result in low overall and disease-free survival rates for many patients. The most widely accepted explanation at the moment is the multistep theory, which explains the genetic and epigenetic processes that transform a single cell into multiple cancerous cells with the capacity to spread [21]. There are several stages in the pathogenesis of cancer. A mutation in a cell's DNA causes oncogenes—genes that promote cell growth—to become active or tumor suppressor genes—genes that restrict cell growth—to become inactive during the first stage, known as initiation. In the second stage, called promotion, the mutant cells are stimulated to divide and proliferate rapidly, resulting in the formation of a small cluster of aberrant cells. In the third stage, known as progression, the aberrant cells keep growing and dividing until they develop into a tumor that can penetrate nearby tissues and travel to other areas of the body via the lymphatic or circulatory systems [22]. Hearth lesions are developing immunological responses with established cellular, cytokine, and vascular reactions that promote cellular proliferation and the inflammatory process for effective tissue regeneration. Resuming antitumor immunity, or more precisely, causing CD8+ cells to build up at the site of injury after healing, protects the organism from malignantly altered cells, which almost always appear in the inflammatory area [23]. The temporary local decrease in antitumor immunity serves a physiological function in the successful restoration of damaged tissue. Growing tumor cells and tissue cells have similar characteristics and structures, according to a study. Thus, eliminating proliferating cells would stop active anti-tumor immunity from healing damaged tissue. Therefore, the outcome of tissue healing depends on both the activation of immune responses that promote healing and a localized, transient reduction of anti-tumor immunity [24].
2.1 ETIOLOGY AND RISK FACTORS OF CANCER :
The genetic material of the original cells is harmed by a sequence of events that eventually result in unchecked cell growth, tumor formation, and finally carcinogenic tissue. Anything that has the potential to cause or raise the risk of cancer is a risk factor. The majority of cancer types are linked to exposure to a variety of factors, including behavioral, lifestyle, and environmental factors [25]. For example, skin cancer is highly likely to result from skin exposure to intense sunlight. There are two categories of cancer risk factors: those that can be changed, like smoking, being overweight, and drinking alcohol, and those that cannot be changed, like age, inherited genetic mutations, and gender. Additionally, there are a number of factors that have been shown in studies to play a significant role in either promoting the growth and spread of cancer or raising the likelihood of developing it [26]. Age and cancer risk [27], smoking and tobacco use [28], heavy alcohol consumption [29], diet and physical activity, viruses and other infections [30] are the primary risk factors for cancer as well as the sun and other forms radiation [31].

FIG3.2. Schematic Representation of Cancer [32].
3. TREATMENTS
Radiation, chemotherapy, immunotherapy, and surgical excision of malignant tissue or tumors are common treatments. Chemotherapy and targeted therapy have a systemic impact, whereas surgery and radiation have a local one. Whether these treatments are used alone or in conjunction with other therapies, like chemotherapy and radiation, depends on the type and stage of the cancer [33]. Chemotherapy and targeted therapy using small molecules are two approaches to using chemicals to treat cancer. Chemotherapeutic drugs typically disrupt various stages of the cell cycle by acting as cytotoxic agents. They are used because cancer cells typically divide more quickly than healthy cells, making them more vulnerable to chemotherapeutic drugs [34]. Based on their biochemical characteristics, these medications can be broadly classified into five groups: alkylating agents (like cisplatin), antimetabolites (like 5-fluorouracil), antitumor antibiotics (like doxorubicin), topoisomerase inhibitors (like topotecan), and tubulin-binding medications (like paclitaxel) [35]. Chemotherapeutic drugs are useful, but they can also have negative effects on healthy cells, including myelosuppression, nausea, vomiting, mucositis, alopecia, and neuropathy. Furthermore, over 90% of cancer patients die during chemotherapy due to multidrug resistance (MDR), which is linked to these medications [36]. Some cancer patients will only receive one kind of treatment, such as surgery or chemotherapy [37]. However, the majority of them receive a combination of treatments, including radiation therapy, chemotherapy, and/or surgery. The type, location, stage, and progression of the cancer in the body, as well as the patient's overall health, are all important considerations when it comes to cancer treatment [38].
Theoretically, all cancers aside from leukemia can be cured if they are totally eradicated by surgery, though this is rarely the case [39]. In situations where cancer spreads to other parts of the body prior to surgery, total surgical removal is typically not feasible. Therefore, the goal of surgery is to either completely eradicate cancer or remove as much of it as possible (Figure 4.1) [40]. Surgery is required not only to remove the primary tumor but also to assess the tumor's stage (size, location, and spread to nearby lymph nodes). The primary objective of the diagnosis is to ascertain the tumor's stage and whether adjuvant treatments are necessary [41]. In what is referred to as a palliative treatment, surgery may occasionally be necessary to manage symptoms, such as in cases where the tumor increases pressure on the spinal cord or obstructs the bowel [42, 43, 44, 45].

FIG 4.1. Breast Cancer Surgery [40].
Radiation treatment Also referred to as radiation exposure, X-ray therapy, or radiotherapy The use of high doses of ionizing radiation to eradicate cancer cells and shrink tumors is known as radiation therapy [46]. High-energy molecules or waves, such as protons, gamma rays, X-rays, and electronic beams, are frequently used in radiation therapy to destroy cancer cells (Figure 4.2) [47]. External beam radiation therapy (EBRT) is an external form of radiotherapy; local radiotherapy is an internal form. Radiation therapy has the effect of concentrating on the intended treatment area. Through the destruction of genetic material (DNA), radiation therapy eliminates cells in the targeted tissue [48, 49, 50, 51].
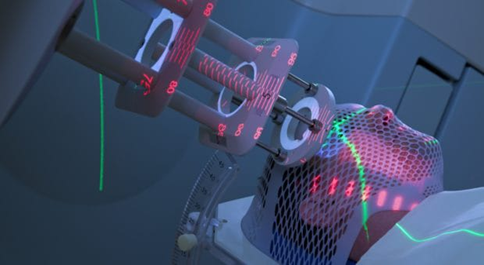
FIG 4.2. Radiation therapy uses high-energy rays are applied from outside the body focusing on the tumor [47].
Chemotherapy is a drug treatment approach that uses potent chemicals to eradicate cancer cells, halt their growth, or stop them from spreading to nearby regions or other parts of the body [52, 53]. Chemotherapy is one of the main treatments for cancer, but not every cancer patient receives it. Regarding its uses, chemotherapy could be used extensively as a primary therapeutic strategy to eradicate cancer cells. Additionally, it could be used in conjunction with another treatment to eliminate any remaining cancer cells, before another treatment to shrink the tumor, or to alleviate the symptoms of advanced cancer [54]. Chemotherapy is used to eradicate cancer cells, but it typically damages healthy cells that divide rapidly, like those in the digestive system and hair follicles [55].
Immunotherapy, also referred to as biological therapy, is a type of treatment that employs the body's immune system to eradicate cancer [56]. To strengthen or reestablish the immune system's functionality, it makes use of chemicals that the body manufactures or those created in a lab Many cancer treatments are still in clinical trials, and immunotherapy is a relatively new method of cancer control. The body's immune system is a sophisticated network of organs and cells that cooperate to protect the body from foreign substances known as anti-gens, like bacteria, viruses, and cancer cells (Figure 3.3) [57]. The immune response is a specific action carried out by various cell types when the body detects the presence of such foreign substances. The body's immune system includes the following cell types: lymphocytes, dendritic cells, B cells, T cells, natural killer cells (NK), and macrophages [58, 59].
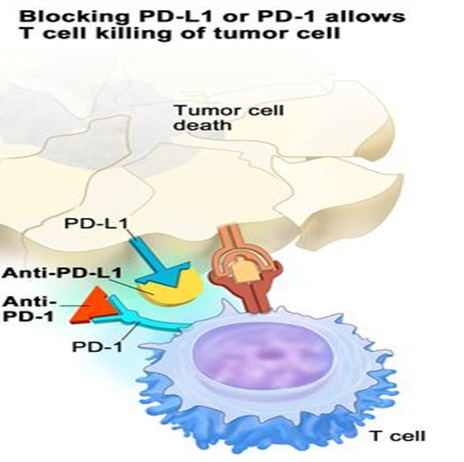
FIG 4.4. Immunotherapy check point inhibitor [57].
The body's immune system uses white blood cells, which are produced in the bone marrow [60]. Bone marrow is destroyed by cancer because chemotherapy and radiation therapy can also destroy it. When the cancer is inactive, the same person's stem cells can be used, or cells from a compatible donor can be transplanted after a chemotherapy dose to eliminate the cancerous cells and replace them with healthy ones. Currently, the goal of stem cell therapy is to give the patient a robust immune system that will be able to carry out its function in the future by shielding the patient from bacteria, viruses, and other infections (Figure 4.5) [61]. One form of cancer treatment that is currently accessible is stem cell therapy, also known as stem cell transplantation [62]. Leukemia, lymphoma, and melanoma are among the cancers that can be cured using this method [63].
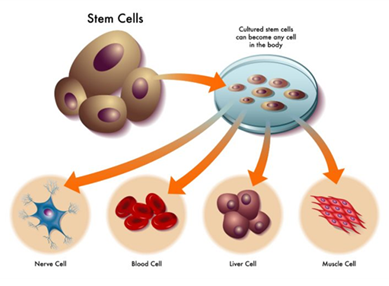
FIG 4.5. Stem cell function in body [61].
In order to treat cancer, gene therapy involves introducing healthy genes into cancerous cells to correct the function of ineffective genes. The idea behind this option is to load the genes into a carrier in order to introduce a functionally effective gene into cancerous cells [64]. After antagonizing the target cells, the carrier introduces the gene into the cancer cells, causing the missing protein to replicate and perform its function [65, 66].
4. PHYTOCHEMICALS WITH ANTICANCER PROPERTIES
Cell cycle regulation, apoptosis, angiogenesis, and metastasis are just a few of the pathways that phytochemicals influence in the development of cancer [67,68,69]. As a result, their multimodal actions provide synergy with traditional therapeutic modalities, which may enhance therapeutic results and lessen side effects. For instance, curcumin, which comes from turmeric, increases lung cancer cells' susceptibility to chemotherapy, which lowers drug resistance [70].
Through a variety of molecular pathways, phytochemicals exhibit anticancer properties that cause cancer cells to stop proliferating, induce apoptosis, inhibit metastasis, and stop angiogenesis. The mechanisms covered here support their integration into cancer treatment and offer a scientific foundation for their therapeutic potential [71,72,73,74,75,76].
Turmeric, or Curcuma longa Linn. (C. longa), is a member of the Zingiberaceae family and has a long history of being used to treat a wide range of illnesses. With its anti-inflammatory, antiproliferative, and immunomodulatory qualities in a variety of cancers, curcumin, a polyphenolic molecule derived from Curcuma longa, has become a promising adjuvant and therapeutic agent in cancer treatment [77,78,79,80,81]. Because curcumin can interact with numerous molecular targets and cellular signaling pathways that are crucial to tumor biology, including those that regulate cell growth, death, blood vessel growth, invasion, and metastasis, it is a major focus of cancer research. Preclinical research has demonstrated that curcumin can induce apoptosis in a variety of cancer types, including brain, breast, lung, head and neck, and prostate cancers. In order to cause programmed cell death, it suppresses antiapoptotic proteins like Bcl-2 and Bcl-xL and increases the expression of death receptors DR4 and DR5 on tumor cells.
Through complex interactions with and modulation of numerous cell signaling pathways necessary for tumor initiation, development, and metastasis, curcumin demonstrates anticancer properties. These pathways regulate angiogenesis, the development of new blood vessels that supply tumors, cell growth, programmed cell death (apoptosis), and the spread of cancer to other areas of the body.
Curcumin keeps cells alive, inflammatory, and resistant to apoptosis by blocking nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) signaling, which is usually elevated in cancers. Curcumin reduces inflammatory responses that support cancer cell survival and encourages tumor cell apoptosis by blocking NF-κB activation [82,83,84].
By interfering with the Janus kinase (JAK)/signal transducer and activator of transcription (STAT) pathway, curcumin inhibits gene transcription associated with cell proliferation and immunological evasion [83,84].
Curcumin targets components of the mitogen-activated protein kinase (MAPK) cascade (including ERK, JNK, and p38) and the epidermal growth factor receptor (EGFR) to inhibit proliferative gene transcription and cause apoptosis in various cancer cells [85,86].
Curcumin has been shown to affect numerous pathways, such as JAK/STAT, Notch, Hedgehog, and p53, which increases its range of anticancer effects. By addressing multiple signaling axes simultaneously, curcumin may help circumvent tumor adaptability and resistance that frequently occur during single-target therapy.
Curcumin's therapeutic potential for liver cancer has been thoroughly studied; it has the ability to prevent tumor growth, trigger apoptosis, and control important signaling pathways linked to hepatocarcinogenesis. In hepatocellular cancer cell lines and animal models, curcumin effectively suppresses proliferation and induces programmed cell death, according to consistent results from systematic evaluations of preclinical and clinical trials [84,87].
Curcumin can reduce tumor burden, lower prostate-specific antigen (PSA) levels, and improve patient biochemical recurrence rates, according to several meta-analyses that support its use as an adjuvant drug in the treatment of prostate cancer [88].
In cancers of the mouth, head, and neck, curcumin exhibits anti-cancer effects at the molecular level. Curcumin increases the efficacy of chemotherapeutic medications like cisplatin and 5-fluorouracil while suppressing the expression of genes linked to tumor growth and metastasis, such as COX-2, MMP-9, and cyclin D1, according to experimental studies [89,90]. Clinical evaluations show that curcumin reduces the severity of oral mucositis in cancer patients, indicating its therapeutic and preventive benefits [91,92,93].
Through a variety of mechanisms, such as anti-inflammatory effects, inhibition of tumor promoting cytokines, and modification of gut microbiota composition, dietary supplementation with curcumin is linked to a lower incidence and development of colorectal cancer [94,95,96].
The black seed, or Nigella sativa L. (Family: Ranunculacea), is one of the naturally occurring plant-based products used to prevent and treat a variety of diseases. Panacea, habbat al-barakah, karayal, black cumin, fennel-flower kalonji, Nigella, black caraway, nutmeg-flower, and Roman-coriander are some of the names given to N. sativa [97]. According to botany, the black seed belongs to the Kingdom: Plantae; Division: Magnoliophyta; Order: Ranunculales; Family: Ranunculaceae; Sub-family: Ranunculoideae; Genus: Nigella; Species: sativa [98,99].
It is unclear how black seed's anti-cancer properties work at the molecular level. According to certain research, TQ strengthens the body's defenses and acts as an antioxidant. According to other research, black seed oil causes apoptosis, which enables the body to methodically get rid of old, unnecessary, and unhealthy cells—like cancer cells—without releasing toxins into the body. Additionally, it has been discovered to regulate Akt signaling pathways, which implies that it regulates the mechanisms governing the survival of both healthy and malignant cells. According to Gali-Muhtasib et al. [100,101], TQ causes the production of ROS. The p53, NF-kB, PPARy, STAT3, MAPK, and P13/AKT pathways are some of the most important pathways mediating the anti-cancer activity of black seed (TQ), according to our review of the mechanisms of action [102]. The therapeutic potential of N. sativa and its component thymoquinone was emphasized in the article by Arshad Rahmani et al., which also described how these compounds prevent cancer by either activating or inactivating a number of molecular pathways [103]. Lei Peng et al. showed that TQ successfully inhibits tumor growth and angiogenesis both in vitro and in vivo when working with osteosarcoma. They hypothesized that one potential mechanism of TQ's antitumor and anti-angiogenic activity is the inhibition of NF-KB and downstream effector molecules [104]. The anti-cancer effects of TQ are mediated through various modes of action, such as antiproliferation, apoptosis induction, cell cycle arrest, ROS generation, and antimetastasis/anti-angiogenesis [105], according to the Woo et al. article from 2012 (102).
El-Mahdy et al. (2005) investigated TQ's impact on human leukemia HL-60 cell lines and found that it had an antiproliferative effect [106]. Analysis of terpene-terminated 6-alkyl residues from TQ revealed that they were effective against HL-60 and 518A2 melanoma [107]. The time and dose-dependent apoptotic effect of α-hederin against murine leukemia P388 cells has also been reported by Swamy and Huat (2003) [108].
Women are frequently diagnosed with breast cancer, which frequently results in death. The effects of N. sativa's alcoholic and aqueous extracts on breast cancer cells (MCF-7) were investigated, and it was found that the extracts, either by themselves or in combination, significantly reduced the cells' ability to proliferate, indicating that they are an effective treatment for breast cancer. Rat mammary cancer was reduced when N. sativa seeds were combined with melatonin and retinoic acid [109,110]. Rat mammary carcinoma was reduced when sativa seeds were combined with retinoic acid and melatonin [111].
Ferric nitrilotriacetate (FeNTA) was used to induce renal carcinogenesis in Wistar rats. N. sativa (50 mg and 100 mg/kg body weight) demonstrated a remarkable effect in restoring normalcy in metabolic pathways and preventing the carcinogenic effect of Fe-NTA [112]. Human renal cancer cells have been significantly inhibited by N. sativa hydroalcoholic extracts [113].
There have been some encouraging findings from research on N. sativa's ability to prevent lung cancer. N. sativa has anticancer properties against Lewis lung carcinoma (LL/2) that were implanted in BDF1 mice, according to Kumara and Huat (2001) [114]. Additionally, Swamy and Huat (2003) reported that α-hederin is the cause of LL/2's anticancer effect [108]. At a concentration of 100 μM, TQ, the primary component of black seed oil, has been shown to have an anticancer effect against lung cancer with an approximately 90% antiproliferative property [115].
Chemotherapy is a key component of cancer treatment, but problems like non-specific drug distribution, quick circulation clearance, and systemic toxicity limit its effectiveness [116,117]. At physiological temperatures, these hydrogels change from a low-viscosity injectable solution to a semi-solid gel depot, exhibiting a distinctive sol-gel transition behavior [118,119,120].
a. Apoptosis induction mechanisms
Microtubule stabilization is the main mechanism by which PTX promotes apoptosis. It disrupts the dynamic processes necessary for the formation of mitotic spindles by binding to β-tubulin and preventing microtubule depolymerization (Fig. 3.1) [121,122]. Cellular stress and the activation of apoptotic pathways result from this disruption, which causes mitotic arrest at the G2/M phase of the cell cycle [123,124]. Both intrinsic (mitochondrial) and extrinsic (death receptor-mediated) pathways are involved in the induction of apoptosis. PTX suppresses anti-apoptotic proteins like Bcl-2 and increases the expression of pro-apoptotic proteins like Bax in the intrinsic pathway [125,126]. This imbalance causes the permeabilization of the mitochondrial membrane, which releases cytochrome c and activates caspase-9 and downstream caspase-3, which coordinate programmed cell death (Fig. 3.1) [127,128]. The apoptotic response is amplified concurrently with the activation of the extrinsic pathway through the upregulation of death receptors such as Fas. These pathways frequently complement one another, increasing PTX's efficacy [129,130,131]. Reactive oxygen species (ROS) production is another important mechanism in PTX-induced apoptosis [132,133,134]. ROS damages cellular components and activates p53, a crucial tumor suppressor that encourages apoptosis, by raising oxidative stress within the cell.This oxidative damage promotes the activation of caspase cascades and further weakens the integrity of the mitochondria [135,136,137]. The execution of apoptosis is largely dependent on caspase-dependent mechanisms, whereby effector caspase-3 cleaves structural and regulatory proteins, methodically destroying the cell [138,139,140].
b. Anti-proliferative mechanism
PTX not only causes apoptosis but also enforces cell cycle arrest at the G2/M phase, which has strong anti-proliferative effects [141,142]. Microtubule stabilization disrupts the spindle assembly checkpoint, which stops cell division and mitosis [143]. Microtubule stabilization disrupts the spindle assembly checkpoint, which stops cell division and mitosis [144]. The build-up of cyclin B1 and the suppression of cyclin-dependent kinase 1 (CDK1) activity support this process [145].
PTX successfully reduces the ability of cancer cells to proliferate by interfering with the cell cycle [146]. Furthermore, it inhibits important survival pathways that cancer cells frequently use to avoid apoptosis and maintain growth, such as PI3K/AKT and NF-κB. PTX's anti-proliferative effects are further enhanced by the downregulation of these pathways, particularly in cancer types that are resistant [147]. Additionally, PTX shows a special capacity to make resistant cancer cells more receptive to therapy. It increases the retention and effectiveness of chemotherapeutic agents by modulating ATP-binding cassette (ABC) transporters, which are in charge of drug efflux [148,149,150]. Because of this characteristic, PTX is especially useful in combination treatments that target tumors that are resistant to multiple drugs [151]. Additionally, it modifies histone acetylation, which results in modifications to gene expression that promote apoptosis and prevent proliferation [152]. By targeting endothelial cells and blocking vascular endothelial growth factor (VEGF) signaling, the medication also interferes with angiogenesis, depriving tumors of essential nutrients and further inhibiting growth [153].
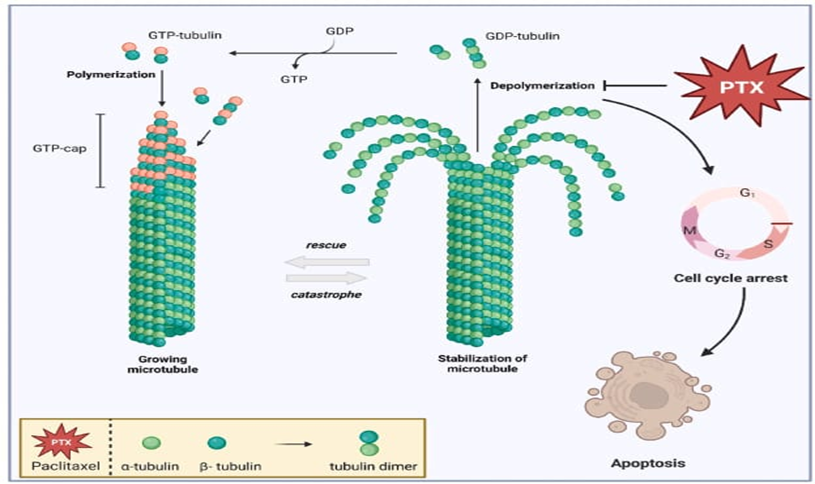
FIG 3.1 Paclitaxel stabilizes microtubules, induces cell cycle arrest, and triggers apoptosis.[127].
Paclitaxel is frequently used in chemotherapy to treat a variety of cancers, particularly as the first-line medication for lung, cervical, breast, and ovarian cancers [154].
The cotton plant (genus Gossypium) and Thespesia populnea, both belonging to the Malvaceae family, are sources of gossypol, a polyphenolic compound [155]. It is mostly embedded in the pigment glands of cotton seeds, making up 20–40% of the gland weight and 0.4–1.7% of the entire kernel. However, it can also be found in other plant parts, including the leaves, bark of roots, seed hulls, and flowers [156]. Another name for it is an oral male contraceptive used to treat gynecological conditions. Its anti-tumor, antioxidant, antiviral, anti-microbial, and immunomodulatory properties have been demonstrated in numerous studies [157].
Gossypol's anticancer action is based on the reduction of anti-apoptotic Bcl-2 family members, which causes apoptosis [158].
Gossypol's primary mode of action against cancer is to cause apoptosis by inhibiting Bcl-2 family anti-apoptotic proteins. This effect is caused by AT-101's inhibitory activity, which downregulates Bcl-2-related proteins in human cancer cells by acting as a mimetic agent to Bcl-2 Homology Domain 3 (BH3) [158].
Through oxidative stress, gossypol has also been demonstrated to cause cell death (Fig. 4.1). It has been shown that gossypol therapy causes tumor cells to produce reactive oxygen species (ROS). Apoptotic pathways, oxidative stress, and DNA damage can all be brought on by high ROS levels. When multiple myeloma cells were treated with 80 μmol/L gossypol, cellular ROS levels significantly increased, resulting in ATP depletion and mitochondrial malfunction. Apoptosis is further triggered by compromised mitochondrial activity [159].
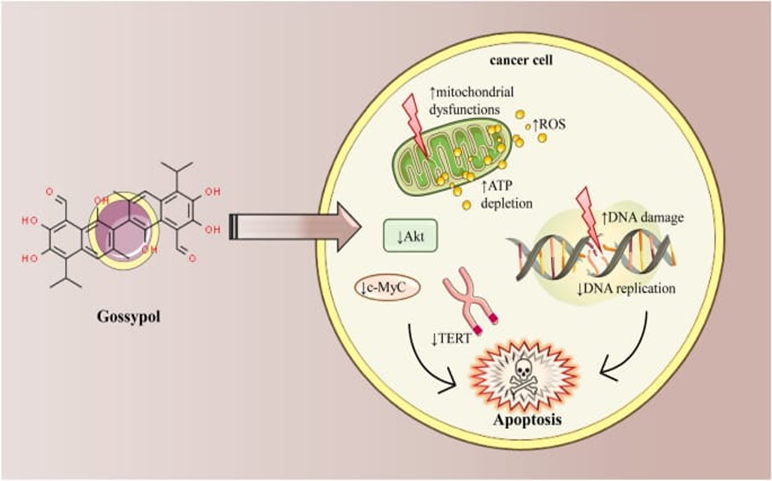
FIG 4.1 Apoptosis induction in cancer cells by gossypol[159].
Gossypol's antitumor potential was first demonstrated in an in vitro study conducted in 1984 [160].
a. Breast cancer
Gossypol has anticancer activity on a number of cancer cell lines, according to earlier in vitro research. After 24 hours, gossypol treatment at varying concentrations (up to 100 µM) considerably reduced the growth of human breast cancer cells (MCF7). After two hours of treatment, the same treatment of pancreatic cancer cells (MIA PaCA-2) demonstrated a significant reduction in cell viability [161].
b. Lung cancer
Gossypol (up to 20 µM for 24 h) inhibits cell migration and proliferation and causes caspase-dependent cell apoptosis in non-small cell lung cancer (NSCLC) cell lines (H1975), according to an in vitro study [162].
Gossypol may be used to prevent the production of androgens in prostate cancer cells, which is another potential mechanism of its anti-tumor effect. Rats' 5α-reductase 1 and 3α-hydroxysteroid dehydrogenase are considerably inhibited by gossypol acetate [163].
Gossypol dramatically decreased cell viability in a time and dose-dependent manner in a different study using human colon cancer cells (COLO 225) [164]. Additionally, the impact of gossypol treatment on 55 genes' mRNA levels was examined. High concentrations of gossypol (up to 100 µM) were found to suppress the expression of most genes [165].
Vinblastin, also known as vincristine, belongs to the group of organic compounds known as vinca alkaloids, which are made up of carbon, hydrogen, nitrogen, and oxygen. The periwinkle plant Catharanthus roseus, formerly known as Vinca rosea, is the source of these compounds [166].
As will be discussed below, vincristine's mechanism of action is characterized by a number of crucial processes that collectively impede the growth and division of cancer cells.
a. Microtubule binding:
The plus ends of microtubules, which are dynamic protein polymers made up of tubulin subunits, are where vincristine binds. Essential parts of the cytoskeleton, microtubules play crucial roles in cell division, including intracellular transport, meiosis and mitosis, and the preservation of cellular shape.
b. Inhibition of microtubule polymerization:
By attaching itself to tubulin subunits inside the microtubule lattice, vincristine prevents microtubule polymerization. Microtubule elongation is inhibited by this binding, which stops new tubulin subunits from joining the developing microtubule.
c. Disruption of mitotic spindle formation:
Microtubules create the mitotic spindle, a dynamic structure that divides chromosomes into daughter cells during the mitotic phase of cell division. The formation and operation of the mitotic spindle are disrupted by vincristine's interference with microtubule dynamics.
d. Cell cycle arrest:
Vincristine disrupts spindle formation, which prevents treated cells from completing the cell cycle. When chromosomes are unable to properly align and segregate during the metaphase stage, cell cycle arrest occurs [167].
e. Induction of apoptosis:
Extended metaphase arrest sets off a cellular reaction that eventually results in programmed cell death, or apoptosis. Microtubule disruption prevents the cell from completing mitosis, which sets off a series of events that ultimately result in cell death [168].
Vinca alkaloids are successfully used as a single agent or in combination with other medications to treat a variety of cancers, including leukemia, breast cancer, and bone marrow cancers. These medications were first used to treat childhood cancers, but they have since been used to treat adult and solid cancers [169,170]. VBL is one of the most researched VAs and is utilized as a crucial part of many chemotherapy courses. VBL is used to treat a number of cancers, including lung cancer, melanoma, brain cancer, Hodgkin's lymphoma, and testicular cancers [171]. Monomers such as vindoline and catharanthine are the most abundant. Vincristine and vinblastine are two popular anticancer medications made from this plant. While vinblastine is used for childhood leukemia, vincristine is used in the chemotherapy regimen for Hodgkin's lymphoma. Native to the Caribbean, Catharanthus roseus (apocyanaceae), commonly referred to as Vinca rosea, has long been used to treat a variety of illnesses. The plant was used by European herbalists to treat everything from headaches to diabetes. Leukemia, Hodghin's disease, malignant lymphomas, neuroblastoma, rhabdomyosarcoma, Wilms tumor, and other cancers are among the more than 400 known alkaloids found in it that have been approved as antineoplastic agents [172]. Madagascar periwinkle has long been used to treat a number of conditions, including infection, high blood pressure, and diabetes mellitus. Ninety distinct alkaloids are found in the plant's leaf portion. Monomers such as vindoline and catharanthine are the most prevalent. Vinpocetine or ethylapovincaminate are two vincamine derivatives that are commonly used in medicine. It has effects on antherosclerotic plaques, blood thinning, vasodilation, and memory [173].
Red and chili peppers are rich in capsaicin, a bioactive phytochemical. Even though the majority of the data clearly shows that capsaicin has significant anticancer benefits, more research is needed to better understand the molecular mechanisms of capsaicin's action so that we can suggest a potential therapeutic approach for its use against cancer. It has been demonstrated that capsaicin modifies the expression of a number of genes related to angiogenesis, growth arrest, metastasis, and cancer cell survival [174,175].
a. Capsaicin and Apoptosis
Loss of apoptotic signaling is strongly linked to malignancy, and apoptosis is a crucial defense against the initiation and spread of cancer [176]. Two important signaling pathways that trigger executioner/effector caspases and cause programmed cell death are the intrinsic mitochondrial death pathway and the extrinsic death receptor pathway. The mitochondrion has been referred to as the "gatekeeper" of the apoptotic mechanism because the mitochondrial pathway is specifically involved in the full execution of apoptosis, and the proteins and pathways of the mitochondrial death pathway have emerged as promising targets for new therapeutic treatments [177].
b. Capsaicin and Metastasis
When cancer cells develop the capacity to infiltrate the vasculature and move to distant organs, a complicated and multi-step process known as metastasis takes place. Eighty percent of cancer-related deaths are caused by metastatic cancer, which is resistant to treatment and continues to be a significant obstacle in cancer treatment [178]. Tumor cell-secreted proteases, such as serine proteases, plasminogen activators, and matrix metalloproteinases (MMPs), break down extracellular matrix components during tumor cell invasion and migration. By altering signaling pathways involved in cell invasion and migration, capsaicin demonstrated anti-invasive and anti-migratory activity and inhibited advanced cancer stages. In transgenic adenocarcinoma of the mouse prostate (TRAMP) mice, capsaicin treatment dramatically decreased the metastatic burden [179]. Without clearly causing cellular cytotoxicity, capsaicin dramatically reduced the migration of melanoma cells [180]. This effect was linked to a decrease in RAS-related c3 botulinum toxin substrate 1 (RAC1), a crucial kinase controlling cell motility and migration, and downregulation of the phosphoinositide 3-kinase (PI3K) signaling cascade [181].
Through the downregulation of AKT/FAK, extracellular signal-regulated kinases, and p38 MAPK signaling, as well as the subsequent downregulation of MMP9 in invasive fibrosarcoma cells, capsaicin inhibited the EGF-induced invasion and migration of human fibrosarcoma cells [182,183]. In bladder cancer, MMP9 activation and capsaicin-stimulated migration depend on TRPV1 [184]. However, colonic cancer metastasis was encouraged by a low dose of capsaicin [185].
It is used to treat cancer of the colon, lungs, bladder, stomach, and myeloma [186].
Vinorelbine can be administered orally or intravenously [187]. When taken orally, you might need to take multiple capsules at once. It is imperative that you take them according to the instructions provided. Vinorelbine capsules should be swallowed whole (not sucked or bitten), along with a glass of water and some food. The capsule should be kept in the refrigerator. Vinorelbine can also be injected into a vein in the hand or arm or administered as a brief mixture (drip) [188].
Vinblastine is the source of vinorelbine, a semisynthetic vinca alkaloid. Periwinkle leaves (Vinca rosea) are the original source of vinca alkaloids like vincristine and vinblastine [189]. By attaching itself to the tubulin of the mitotic microtubules, vinorelbine prevents the growth of cells. Vinorelbine encourages cancer cells to undergo apoptosis, just like other mitotic inhibitors. One Vinorelbine exhibits both non-multidrug and multidrug resistance in vitro [190]. Neuronal axons, mitotic spindles, and other cells all contain microtubules. While axonal microtubule inhibition seems to be associated with neurotoxicity, mitotic microtubule inhibition appears to be associated with antitumor activity. Vinorelbine is less neurotoxic than vincristine and vinblastine because it is more selective against mitotic rather than axonal microtubules in vitro [191]. One substance that sensitizes to radiation is vinorelbine. It is specific to the M phase of the cell cycle [190]. Similarly, VNR is highly noteworthy for inducing apoptosis in cancer cells using various anti-microtubule operators. Although the precise mechanism by which this process takes place is complicated, different data still need to be explained. The initiation of the cancer suppressor gene p53 and the activation or inactivity of several protein kinases involved in essential signaling pathways, including p21 WAF1/CIP1, Ras/Raf, PKC/PKA, and others, are all impacted by disarray of the microtubule structure [192]. The apoptosis inhibitor Bcl2 is rendered inactive by these atomic alterations, leading to phosphorylation. Thus, the arrangement of cell apoptosis is animated by a decrease in the formation of heterodimers between Bcl2 and the pro-apoptotic gene BAX [193].
Numerous alkaloids with anticancer properties have been found in Catharanthus roseus, including vinblastine, vincristine, vindoline, vindolidine, vindolicine, vindolinine, and vindogentianine [194]. By altering microtubular dynamics, they can prevent cell proliferation and trigger apoptosis [195]. Vinblastine sulphate has been used to treat Hodgkin's disease, choriocarcinoma, neuroblastoma, lymphosarcoma, and lung and breast cancers. On the other hand, acute juvenile leukemia, lymphocytic leukemia, Hodgkin's disease, reticulum cell sarcoma, neuroblastoma, and Wilkins's tumor can all be treated with vincristine sulfate, an oxidized form of vinblastine that prevents mitosis in the metaphase [196].
CONCLUSION
This review article offers details on herbs and natural items that may slow the spread of cancer or be used as an adjuvant to cancer treatments for individuals who now have or have previously had the disease. Medicinal herbs are known to have strong anticancer properties, and they are a major source of synthetic and/or herbal origin when discussing anticancer treatments. The use of natural materials derived from medicinal plants has been crucial in the fight against cancer. In animal models of leukemia, skin cancer, and sarcomas, they have shown anticancer efficacy. The biological activity of a few chosen plants has been investigated, and more research into the anticancer potential of the plants exhibiting promising activity has to be done. Vinblastine and vincristine, two alkaloids from Vinca rosea, are among the most effective anticancer medications now available. High death rates are linked to cancer The patient would be greatly relieved if herbs could be utilized even in palliative care or to lessen the negative symptoms of cancer.
REFERENCES




Kajal Ingavale, Pranali Jadhav, Kusum Hanbar, Sushama Garud, Dr. Bhagyesh Janugade, Phytochemicals as Promising Anticancer agents Mechanism and Therapeutic Potential, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 2095-2123. https://doi.org/10.5281/zenodo.19116289
 10.5281/zenodo.19116289
10.5281/zenodo.19116289
