Shivajirao S. Jondhle college of pharmacy, Asangoan, Taluka- Shahapur, District- Thane, State- Maharashtra, Pin code -421601
Cardiovascular diseases (CVDs) constitute the leading cause of morbidity and mortality in India and represent a growing public health concern among the geriatric population. India is undergoing a rapid demographic transition, with a steadily increasing proportion of individuals aged 60 years and above. This ageing population is characterized by a high prevalence of multiple chronic conditions, including hypertension, diabetes mellitus, dyslipidaemia, coronary artery disease, heart failure, and arrhythmias. The coexistence of these conditions necessitates long-term pharmacotherapy with multiple medications, resulting in widespread polypharmacy. While polypharmacy is often clinically justified in cardiovascular care, it significantly increases the risk of adverse drug reactions (ADRs), drug–drug interactions (DDIs), medication non-adherence, functional decline, hospitalizations, and mortality in older adults. Cardiovascular drugs are among the most frequently implicated agents in serious and preventable ADRs due to their narrow therapeutic indices, complex pharmacokinetics, and altered pharmacodynamics in the elderly. Pharmacovigilance plays a critical role in identifying, assessing, understanding, and preventing medication-related harm, particularly in vulnerable geriatric populations. In India, the Pharmacovigilance Programme of India (PvPI) has strengthened national drug safety surveillance; however, under-reporting of ADRs, limited geriatric-specific data, lack of interdisciplinary collaboration, and fragmented healthcare delivery remain major challenges. This review comprehensively examines the burden of cardiovascular diseases and polypharmacy among geriatric patients in India, explores the mechanisms underlying increased ADR risk, highlights commonly implicated cardiovascular drug classes and interactions, and discusses clinical, organizational, and digital strategies—including artificial intelligence—to strengthen pharmacovigilance and improve drug safety outcomes
Cardiovascular diseases (CVDs) are the foremost cause of death globally and have emerged as the dominant contributor to morbidity and mortality in India over the past few decades. According to national and global estimates, CVDs account for nearly one-third of all deaths in India and contribute substantially to disability-adjusted life years lost [1–3]. The epidemiological transition in India—driven by urbanization, sedentary lifestyles, dietary changes, tobacco use, and increased life expectancy—has resulted in a sharp rise in non-communicable diseases, particularly among older adults [4].India is experiencing rapid population ageing, with the number of individuals aged 60 years and above projected to double by 2050. Ageing is associated with physiological decline, increased vulnerability to chronic diseases, and a high prevalence of multimorbidity [5]. Multimorbidity, defined as the coexistence of two or more chronic conditions, is now considered the norm rather than the exception among geriatric patients [6]. Cardiovascular diseases frequently coexist with diabetes mellitus, chronic kidney disease, chronic obstructive pulmonary disease, and musculoskeletal disorders, leading to complex therapeutic regimens.Polypharmacy, commonly defined as the use of five or more medications, is highly prevalent among geriatric cardiovascular patients [7]. In many cases, polypharmacy is appropriate and guideline-directed; however, excessive or inappropriate polypharmacy significantly increases the risk of adverse outcomes [8]. Older adults are particularly susceptible to ADRs due to age-related changes in drug absorption, distribution, metabolism, and excretion, as well as altered pharmacodynamic responses [9].Cardiovascular drugs contribute disproportionately to ADR-related hospitalizations in the elderly. Anticoagulants, antiplatelet agents, diuretics, antiarrhythmics, and antihypertensives are frequently implicated due to their narrow therapeutic windows and high potential for interactions [10–12]. Pharmacovigilance is therefore essential to ensure the safe use of cardiovascular medications in geriatric populations.The Pharmacovigilance Programme of India (PvPI), launched in 2010, aims to monitor and improve drug safety nationwide [13]. Despite its achievements, challenges such as under-reporting of ADRs, limited awareness among healthcare professionals, inadequate geriatric-focused surveillance, and poor integration of pharmacovigilance into routine clinical practice persist [14,15]. Addressing these gaps is critical to improving cardiovascular drug safety in India’s ageing population.
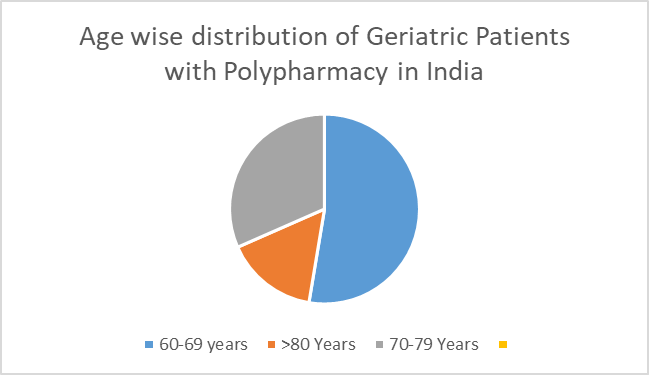
Pie chart depicting the age-wise distribution of geriatric cardiovascular patients experiencing polypharmacy in India. Approximately 55% belong to the 60–69-year age group, 30% to 70–79 years, and 15% to ≥80 years. Although the oldest-old represent a smaller proportion, they exhibit the highest vulnerability to adverse drug reactions and drug-related hospitalizations.
4. Cardiovascular Diseases in the Geriatric Population
4.1 Hypertension
Hypertension is the most prevalent cardiovascular condition among older adults in India, affecting more than 60% of individuals aged 60 years and above [16]. Age-related arterial stiffness, endothelial dysfunction, and reduced baroreceptor sensitivity contribute to isolated systolic hypertension, which is common in geriatric patients. Management often requires combination therapy involving multiple antihypertensive classes, thereby increasing medication burden and interaction risk.
4.2 Coronary Artery Disease
Coronary artery disease (CAD) remains a leading cause of morbidity and mortality among elderly Indians. Older adults frequently present with atypical symptoms, leading to delayed diagnosis and prolonged pharmacotherapy. Secondary prevention strategies typically involve antiplatelet agents, statins, beta-blockers, and renin–angiotensin system inhibitors, contributing significantly to polypharmacy [17–19].
4.3 Heart Failure
Heart failure prevalence increases exponentially with age and represents a major cause of hospitalization in the geriatric population. Management involves multidrug regimens, including diuretics, ACE inhibitors or ARBs, beta-blockers, mineralocorticoid receptor antagonists, and newer agents such as SGLT2 inhibitors. These complex regimens increase the risk of ADRs and DDIs, particularly in patients with renal impairment [20–22].
4.4 Arrhythmias
Atrial fibrillation is the most common arrhythmia in older adults and is strongly associated with stroke and systemic embolism. Long-term anticoagulation therapy is often required, frequently in combination with antiplatelet agents, significantly increasing bleeding risk [23,24].
4.5 Dyslipidaemia
Dyslipidaemia commonly coexists with other cardiovascular conditions and requires long-term statin therapy. Statins are frequently involved in clinically significant DDIs, particularly with macrolide antibiotics and azole antifungals [25].
4.6 Age-Related Physiological Changes
Age-related declines in renal and hepatic function, changes in body composition, and altered receptor sensitivity significantly affect drug pharmacokinetics and pharmacodynamics, increasing susceptibility to ADRs [26].
5. Polypharmacy in Geriatric Cardiovascular Patients
5.1 Definition and Types of Polypharmacy
Polypharmacy is commonly defined as the concurrent use of five or more medications, while hyperpolypharmacy refers to the use of ten or more drugs. Types include appropriate polypharmacy, inappropriate polypharmacy, therapeutic duplication, and prescribing cascades [27].
Types of Polypharmacy
Polypharmacy can be categorized into different forms based on the clinical justification and pattern of medication use. Understanding these categories is essential for identifying rational prescribing practices and minimizing medication-related risks, particularly among older adults with multiple chronic conditions [27].
Appropriate polypharmacy describes the use of several medications where each drug is prescribed for a well-defined clinical indication and supported by current evidence. In patients with complex disease profiles, such as elderly individuals with cardiovascular and metabolic disorders, the simultaneous use of multiple drugs may be necessary to achieve therapeutic goals. When medications are carefully selected, regularly reviewed, and appropriately monitored, the benefits of this approach can outweigh potential risks [27].
Inappropriate polypharmacy refers to the continued use of medications that offer limited clinical benefit, lack clear indications, or pose an increased risk of adverse outcomes. This form often results from inadequate medication review, age-related physiological changes affecting drug handling, or failure to discontinue drugs that are no longer required. Inappropriate polypharmacy significantly increases the likelihood of adverse drug reactions and harmful drug–drug interactions [27].
Therapeutic duplication occurs when two or more medications with similar pharmacological actions are prescribed concurrently without a valid therapeutic purpose. This situation frequently arises due to fragmented healthcare delivery or poor communication between multiple prescribers, leading to unnecessary medication exposure and an elevated risk of toxicity without additional clinical benefit [27].
Prescribing cascades develop when the side effects of a medication are mistakenly identified as a new health problem, prompting the addition of further drugs instead of modifying or discontinuing the original agent. Over time, this cycle increases medication burden and compounds the risk of adverse events, especially in older patients who are more susceptible to drug-related complications [27].
5.2 Causes of Polypharmacy in India
Key causes include multimorbidity, involvement of multiple specialists, self-medication, widespread OTC drug availability, and fragmented healthcare delivery systems [28–30].
5.3 Common Cardiovascular Polypharmacy Combinations
ACE inhibitor/ARB + calcium channel blocker + diuretic
Antiplatelet agents + anticoagulants
Statins + antihypertensives
Beta-blockers + antiarrhythmic drugs
6. Cardiovascular Drugs Causing Polypharmacy in Geriatric Patients
Table 1. Cardiovascular Drugs and Reasons for Polypharmacy
|
Drug Class |
Reason for Polypharmacy |
|
Antihypertensives |
Combination therapy for BP control |
|
Antiplatelets |
Secondary prevention |
|
Anticoagulants |
Stroke prevention |
|
Statins |
Long-term lipid control |
|
Diuretics |
Symptom relief in heart failure |
|
Antiarrhythmics |
Rhythm control |
6.1 Drug–Drug Interactions in Polypharmacy
Table 2. Major DDIs and Clinical Consequences
|
Drug Combination |
Consequence |
|
Anticoagulants + antiplatelets |
Increased bleeding risk |
|
ACE inhibitors + potassium-sparing diuretics |
Hyperkalaemia |
|
Beta-blockers + non-dihydropyridine CCBs |
Bradycardia, heart block |
|
Statins + macrolides |
Myopathy, rhabdomyolysis |
|
Digoxin + diuretics |
Digoxin toxicity |
Table 3. Cardiovascular Drugs: Class, Adverse Effects & Contraindications
|
Drug |
Pharmacological Class |
Common Adverse Effects |
Contraindications |
|
Propranolol |
Non-selective beta-adrenergic blocker |
Slow heart rate, worsening heart failure, tiredness, cold hands/ feet, breathing difficulty in susceptible patients, sexual problems |
Asthma, chronic lung disease, heart block, severe bradycardia |
|
Atenolol |
Selective β1-blocker |
Fatigue, reduced heart rate, dizziness |
Severe bradycardia, conduction defects |
|
Metoprolol |
Cardio-selective β1-blocker |
Hypotension, bradycardia, weakness |
Advanced heart block, acute heart failure |
|
Bisoprolol |
Highly selective β1-blocker |
Slow pulse, dizziness, fatigue |
Cardiogenic shock, heart block |
|
Nebivolol |
β1-blocker with vasodilatory action |
Headache, fatigue, bradycardia |
Severe liver disease, conduction disorders |
|
Chlorthalidone |
Thiazide-like diuretic |
Low potassium levels, increased uric acid, raised blood sugar |
Gout, severe kidney impairment |
|
Hydrochlorothiazide |
Thiazide diuretic |
Dehydration, low potassium, hearing disturbance (high dose) |
Anuria, severe electrolyte loss |
|
Spironolactone |
Potassium-sparing diuretic |
High potassium, breast enlargement in males, menstrual irregularities |
Hyperkalaemia, renal failure |
|
Enalapril |
ACE inhibitor |
Persistent dry cough, dizziness, high potassium, rare facial swelling |
Pregnancy, bilateral renal artery stenosis |
|
Lisinopril |
ACE inhibitor |
Hypotension, cough, impaired kidney function |
Pregnancy, bilateral renal artery stenosis |
|
Losartan |
Angiotensin receptor blocker (ARB) |
Dizziness, raised potassium (cough uncommon) |
Pregnancy |
|
Furosemide |
Loop diuretic |
Dehydration, Low potassium, hearing disturbance (high dose) |
Anuria, severe electrolyte loss |
|
Amlodipine |
Dihydropyridine calcium channel blocker |
Swelling of ankles, headache, flushing |
Severe low blood pressure |
|
Verapamil |
Non-dihydropyridine calcium channel blocker |
Constipation, slow heart rate, heart block |
Heart block, heart failure |
|
Diltiazem |
Non-dihydropyridine calcium channel blocker |
Bradycardia, hypotension |
Conduction abnormalities |
|
Guanethidine |
Adrenergic neuron blocker |
Severe postural hypotension, diarrhea, Sexual dysfunction |
Rarely used now due to toxicity |
7. Tools and Strategies to Improve Pharmacovigilance
7.1 Clinical Tools
Beers Criteria, STOPP/START criteria, Medication Appropriateness Index, and electronic DDI databases are widely used to identify potentially inappropriate medications in older adults [31–34].
7.2 Pharmacovigilance Interventions
Medication reconciliation, deprescribing protocols, involvement of clinical pharmacists, mobile ADR reporting, and patient education significantly improve drug safety outcomes [35–38].
7.3 AI and Digital Health
Figure 2: Flowchart of AI-Enabled Pharmacovigilance
Flowchart: AI-enabled pharmacovigilance in geriatric cardiovascular care Polypharmacy in geriatric cardiovascular patients
↓
Increased risk of adverse drug reactions (ADRs)
↓
Electronic health record (EHR) and pharmacy data integration
↓
AI-based signal detection and risk prediction
↓
Clinical decision support alerts to clinicians
↓
Deprescribing and therapy optimization
↓
Improved patient safety and outcomes
Flowchart illustrating AI-enabled pharmacovigilance in geriatric cardiovascular care: polypharmacy → increased ADR risk → electronic health record data integration → AI-based signal detection → clinical decision support → deprescribing and therapy optimization → improved patient safety.
CONCLUSION
Polypharmacy among geriatric cardiovascular patients in India is a complex but unavoidable consequence of multimorbidity and evidence-based therapy. Strengthening pharmacovigilance through clinical tools, interdisciplinary collaboration, and digital innovations is essential to minimize ADRs and improve cardiovascular outcomes in India’s ageing population.
REFERENCES
doi:10.1016/S0140-6736(21)00508-3
doi:10.1093/ageing/afz193
doi:10.1186/s12877-021-02359-1
doi:10.1016/j.phrs.2020.104973
doi:10.1007/s40264-020-00938-7
doi:10.1007/s40264-021-01127-4
doi:10.1177/20420986211009633
doi:10.1093/eurheartj/ehab507
doi:10.1161/CIR.0000000000000678
doi:10.1016/j.jacc.2021.03.317
doi:10.1093/eurheartj/ehaa612
doi:10.1007/s40266-020-00756-6
doi:10.1016/j.atherosclerosis.2021.07.013
doi:10.1111/jgs.16766
doi:10.1093/ageing/afz043
doi:10.1016/S0140-6736(20)30041-2
doi:10.1002/14651858.CD008165.pub5
doi:10.1007/s40266-020-00747-7
doi:10.1038/s41746-021-00423-1
doi:10.1002/cpt.1655
doi:10.1038/s41591-018-0300-7
doi:10.1161/HYPERTENSIONAHA.120.15026
doi:10.1007/s10741-020-09974-3
doi:10.1136/bmjopen-2020-043123
doi:10.1016/j.jamda.2021.09.022
doi:10.1007/s11096-021-01263-8
doi:10.1007/s40264-021-01074-0
doi:10.1016/S0140-6736(21)00508-3
doi:10.1093/ageing/afz193
doi:10.1186/s12877-021-02359-1
doi:10.1016/j.phrs.2020.104973
doi:10.1007/s40264-020-00938-7
doi:10.1007/s40264-021-01127-4
doi:10.1177/20420986211009633
doi:10.1093/eurheartj/ehab507
doi:10.1161/CIR.0000000000000678
doi:10.1016/j.jacc.2021.03.317
doi:10.1093/eurheartj/ehaa612
doi:10.1007/s40266-020-00756-6
doi:10.1016/j.atherosclerosis.2021.07.013
doi:10.1111/jgs.16766
doi:10.1093/ageing/afz043
doi:10.1016/S0140-6736(20)30041-2
doi:10.1002/14651858.CD008165.pub5
doi:10.1007/s40266-020-00747-7
doi:10.1038/s41746-021-00423-1
doi:10.1002/cpt.1655
doi:10.1038/s41591-018-0300-7
doi:10.1161/HYPERTENSIONAHA.120.15026
doi:10.1007/s10741-020-09974-3
doi:10.1136/bmjopen-2020-043123
doi:10.1016/j.jamda.2021.09.022
doi:10.1007/s11096-021-01263-8
doi:10.1007/s40264-021-01074-0




Harsh Tapal, Chetana Mayekar, Sanket Gabhale, Ashwini Taware, Pranali Vekhande, Manas Suryarao, Pharmacovigilance of cardiovascular drugs polypharmacy in the geriatric population in India., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1419-1427. https://doi.org/10.5281/zenodo.19001055
 10.5281/zenodo.19001055
10.5281/zenodo.19001055
