Chhatrapati Shivaji ColleSchool of Pharmacy and Emerging Sciences, Baddi University of Emerging Sciences and Technology, Baddi, Solan - 173205, Himachal Pradesh, Indiage of Pharmacy, Deori (441901)
Pharmacovigilance (PV) is the monitoring, detection, evaluation, and prevention of adverse drug reactions (ADRs), which is essential to guaranteeing the safety and effectiveness of pharmaceuticals. Since they are the most approachable medical practitioners, community pharmacists are in a prime position to make a substantial contribution to pharmacovigilance initiatives. However, several obstacles prevent their participation from being at its best. The purpose of this Knowledge, Attitude, and Practice (KAP) study is to assess community pharmacists' attitudes on pharmacovigilance and pinpoint tactical solutions to current problems. Using a structured questionnaire, a cross-sectional study was carried out among registered community pharmacists to evaluate their practical involvement in ADR reporting, their attitude toward the importance and responsibility of pharmacovigilance, and their understanding of its definitions, goals, and procedures. The survey found that although the majority of pharmacists had a favourable attitude toward pharmacovigilance, there was a large discrepancy between their knowledge and behavior. Lack of training, ignorance of reporting procedures, time restraints, and feared legal ramifications were major obstacles. The study suggests focused educational efforts, pharmacovigilance issues being incorporated into pharmacy curriculum, ongoing professional development initiatives, and the creation of an intuitive digital ADR reporting platform as ways to close these gaps. Furthermore, active pharmacist participation should be recognized and encouraged by national regulatory bodies. Building a strong pharmacovigilance culture at the community level requires cooperation between academic institutions, regulatory agencies, and healthcare facilities. In order to improve therapeutic outcomes and safeguard the public's health, this study emphasizes the critical necessity to increase pharmacists' participation in pharmacovigilance through strategic policy and practice-oriented methods.
Drug Safety
The use of medicines is an important aspect of many PHPs that are designed to improve the health of a target population. Their cost to the health budget is between 6% in developed countries and 45% in some developing countries, but there are huge variations between both developed countries and developing countries. Medicines are important not only because of their capacity to treat and prevent disease and to support PHPs, but also because the confidence of the public in the health policies of their countries is inextricably linked to their confidence in the availability of medicines that are safe and effective. All medicines carry some risk of harm and it is important to monitor their effects, both intended and unwanted, so that good evidence is available upon which to base an assessment of risk versus effectiveness or risk versus benefit. Furthermore, particularly with new medicines, the early identification of unexpected adverse reactions and their risk factors is essential, so that the medicines can be used in an informed manner with the least chance of harm. This is the role of pharmacovigilance. Information gathered during pharmacovigilance may also assist in selecting the most appropriate medicine for future use. Despite the progress that has been made in pharmacovigilance, the burden on public health of adverse reactions to medicines (traditionally referred to as ADRs) remains significant. Pharmacoeconomic studies on the costs of ADRs suggest that governments pay considerable amounts from their health budgets towards covering the costs associated with them. In a meta-analysis of 39 prospective studies from hospitals in the United States, it was shown that ADRs ranked from the fourth to sixth leading cause of death [1]. Extrapolation of data, from a more recent prospective study in England to the whole National Health Service bed base, suggests that for patients aged > 16 years, at any one time the equivalent of up to seven 800-bed hospitals may be occupied by patients admitted with ADRs. There are also costs associated with ADRs in primary health care, but these are more difficult to assess. To the direct costs should be added the indirect costs of adverse reactions, such as loss of productivity. There are now sufficient data available to indicate that the provision of adequate strategies to detect and prevent adverse reactions is a cost- effective commitment of resources. Health requirements and the use of medicines in different countries vary considerably for many reasons, including different burdens of disease, economic, ethnic, cultural and dietary factors, and the level of development of a system for the regulation of medicines. Vigilance regarding both safety and effectiveness of medicines must become a priority area within public health. WHO has produced guidelines for setting up a national pharmacovigilance canter and many WHO PHPs have developed their own guidelines. The vaccines example is included in Annex 1. This document offers a critical examination of the strengths and weaknesses of both pharmacovigilance systems and public health systems. It describes the roles and responsibilities of all parties involved and anticipates the developments that will be necessary to enable both pharmacovigilance and PHPs to meet the challenges of the coming years. The increasing public expectation of safety is one of the major elements of the need for improving the safe use of medicinal products. As effective medicines become more widely available, there is an increasing demand for their use by the public and it is imperative that these medicines are monitored for safety. National pharmacovigilance centers cannot address this issue alone. They need to work together with other parties including the local regulatory authority, managers of PHPs, health professionals, academia, governments, the pharmaceutical industry, patients and consumers, and the media [2,3].
Public Health Programmes Using Medicines:
Public health is defined as the organized efforts of society to protect, promote and restore people health. The programs, services and institutions involved focus on the prevention of disease and the health needs of the population as a whole. Public health activities change in response to variations in technology and social values, but the goals remain the same: to promote health and to reduce the amount of disease, premature death and disease- related discomfort and disability in the population [4]. Health promotion strategies contribute to the improvement of health and the prevention of diseases in developing and developed countries alike. Public health strategy is determined in each country according to the epidemiology of prevalent diseases and the local circumstances. Developing countries are facing a major challenge in tackling the communicable diseases that are responsible for high rates of morbidity and mortality. Infectious diseases for which effective treatment have existed for a long time, such as some diarrheal and respiratory diseases in children, continue to take their toll. Communicable diseases such as tuberculosis, human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), sexually transmitted diseases (STDs), malaria, schistosomiasis, amoebiasis, leprosy, trachoma, lymphatic filariasis, intestinal helminthiasis, onchocerciasis, leishmaniosis and trypanosomiasis add to the disease burden [5]. Health authorities include in their basic health package PHPs aimed at reducing morbidity and mortality associated with the major common diseases. The important components of a PHP are education, environmental modifications, nutrition intervention, lifestyle and behavioral changes, preventive measures such as immunization, screening for hypertension and breast cancer and, in addition, pharmacotherapy [6]. The pharmaceutical industry is increasingly involved in either donating, or providing at reduced cost, medicines for direct administration to large populations and communities through a number of public health or disease control programs. Consumers and patients of affected communities are not usually involved directly in the decision-making process of the PHP. However, they influence the success of the desired outcome by accepting or rejecting the program. The success of PHPs depends on the active participation of the population and on multisectoral involvement [7].
The Public Health Environment:
Without good guidance and training programs for healthcare working developing countries, patients could be at an increased risk of medication error and/or preventable ADRs.
Disease
Treatment is often initiated in the absence of an adequate diagnosis and there may be insufficient The diseases managed by the PHPs are not always well-diagnosed clinically. follow-up of patients. For example, because of inadequate diagnostic facilities, it is common clinical practice for patients to be given presumptive treatment for malaria although many of the patients treated will not have the disease [8].
Population
Public health programs may treat a large population over a short period. To meet the specific needs of a particular program, the community could be treated in one of three different ways: i.e. masse, case-contact or individual treatment. Under these conditions, some of the patients treated may not have the disease, or treatment could be given to patients in whom there are contraindications to the use of the medicine (e.g., pregnant, or breastfeeding women, young children or elderly people) [9].
Medicine
Huge quantities of medicines are used each year; for example, more than US$ 316 billion was spent on medicines in 2000. However, patterns of consumption differ between high- and low-income countries. In high-income countries, “originator” (patented) pharmaceuticals account for two thirds of sales of all medicines. The total sale of medicines grew substantially between 1990 and 2000. In low-income countries such pharmaceuticals account for only about one third of total sales. Medicines can be generic with low commercial value (for example mebendazole), new medicines with which there is limited clinical experience (e.g, new antiretroviral) or still be undergoing clinical trials.
Health-care provider
In response to the increasing recognition of deficiencies in the provision of health care by existing health services, the concept of delivery of primary health-care by trained non- medical, village workers and involvement of the community has emerged. This has resulted in better implementation of national PHPs. However, there is frequently an inadequate understanding of adverse reactions even among highly trained personnel and more attention needs to be given to pharmacovigilance training in the curricula for medical and nursing undergraduates. This training in turn needs to be passed on to the non-medical health-care workers. The public health staffs responsible for the dispensing of medicines and the monitoring of responses are most often paramedics with educational levels that range from primary school to university graduate. Their training involves education in public health issues such as sanitation, nutrition, hygiene, family planning and on their role in the implementation of various programs. They lack training in the early detection and reporting of ADRs. When adverse events were reported at follow-up visits, the volunteers had difficulty in distinguishing patients with persistent or potentially more serious events from those in whom symptoms had abated or were abating [10].
Post Marketing surveillance
Pre-marketing study phase I, II, III trials necessary takes place in control situation selected groups of people. Though a new drug appears to be safe in this studies, unseen adverse effects can occur. When a drug is released for use in general population [11].
Public Health Programmes for Disease Control:
WHO plays an important role in the initiation, conduct and evaluation of PHPs and much effort is made to select, procure and distribute medicines, train staff and to educate the community to enlist their participation. [12,13] Decisions to start programs for public health are taken after considerable deliberation at the international and national levels. These PHPs are considered crucial for reducing mortality and morbidity. A significant part of the program budget is allocated to the procurement of medicines. WHO plays an important role in the initiation, conduct and evaluation of PHPs. Numerous guidelines are produced by WHO or by Member States describing procedures for implementation and monitoring of PHPs and much effort is made to select, procure and distribute medicines, train staff and to educate the community to enlist their participation. Detailed manuals are available on the practical procedures for the handling and use of the medicines or vaccines, particularly storage, administration, and contraindications. Each program has a standard therapeutic protocol following WHO technical guidance. Guidelines and training programs facilitate the proper conduct of thePHPs [14-16]. It is usual for a PHP to have a vertical organization and to be operated by a program manager. Program managers in charge of different programs do not necessarily collaborate. At the community level however, health professionals or community agents may be involved in several PHPs.

Pharmacovigilance:
Pharmacovigilance is the science and activity relating to the detection, assessment, understanding and prevention of adverse effects or any other possible medicine-related problem [17]. Some important definition requires to understand pharmacovigilance: -
Periodic Safety Update Reports (Psur)
The periodic safety update report for marketed drugs (PSUR) is intended to provide competent authorities with an update on periodic but comprehensive assessment of the worldwide safety data or biological product at defined times, post-authorization.
Pharmacoeconomics
Economic evaluation which is concerned with identifying, measuring and valuing inputs ti.e. estimating cost) and outputs (benefits) of a drug therapy or health care program as compared to alternative course of action or, if realistic, "doing nothing'. An assessment is made as to the collective improvement in the welfare of individuals relative to status quo, i.e. current normal practice [18].
Regulatory Authority
The legal authority in any country with the responsibility of regulating all matters relating to drugs. Examples: Drug Controller General of India (DCGI) for India, Food and Drug Administration (FDA) for USA, Medicines and Health care Products Regulatory Agency (MHRA) for UK. [19]
Effectiveness/Risk
The balance between the rate of effectiveness of medicine versus the risk or harm is a quantitative assessment of the merit of a medicine used in routine clinical practice. Comparative information between therapies is most useful. This is more useful than the efficacy and hazard predictions from pre-marketing information that is limited and based on selected subjects [20].
Drug
A drug or medicine is a pharmaceutical product, used in or on the human body for the prevention, diagnosis, or treatment of discase, or for the modification of physiological functions'
Data Safety Monitoring Board (Dsmb)
DSMB is used as a general term for a body that reviews interim trial data and which has the potential to influence the future conduct of a trial.
Development Safety Updatereport (Dsur)
As proposed by the COMS VIT Working Grip, DSUR is an internationally harmonized document modelled after the Periodic Safety Update Report PSUR) for marketed products. It is prepared by conducting an overall appraisal of safety din I regular intervals that allows recognition of rank, after thoughtful assessment and is approach communicated to all interested stakeholder, to support the safety of clinical trial subjects.
Epidemiology
The wince concerned with the study of the factor determining and influencing the frequency distribution of discase, injury and other health. plated events and their causes in a defined sum population for the purpose of establishing programs to prevent and control their development and spread (Dorland's Illustrated Medical Dictionary).
Origins of Pharmacovigilance
The history of pharmacovigilance goes back more than 40 years. In 1965 the eighteenth World Health Assembly, WHA 18.42, drew attention to the problem of adverse drug reaction monitoring and following further resolutions (see Annex 3) in 1966, 1967 and 1970 the International Drug Monitoring Program came into being. In 2005, 78 member countries are participating in this Program and the last decade has seen the participation of numerous developing countries. Pharmacovigilance Department of WHO, Geneva. Recently, the concerns of pharmacovigilance have been widened to include herbal, traditional and complementary medicines, blood products, biologicals, medical devices, and vaccines. Many other issues are also of relevance to the science of pharmacovigilance. These include substandard medicines, medication errors, lack of efficacy, use of medicines for indications that are not approved and for which there is inadequate scientific basis, case reports of acute and chronic poisoning, assessment of medicine-related mortality, abuse and misuse of medicines, and adverse interactions of medicines with chemicals, other medicines and foods and drinks. [21-22]
The cost advantages
A medicines monitoring system is an essential and cost-efficient means of detecting and minimizing injury to patients and averting potential disaster. Pharmacovigilance can help to better access and communicate information on the effectiveness and risks of medicines and to educate and inform patients. It is also an insurance against the undetected use of ineffective, substandard or counterfeit medicines, thus minimizing the possibility of wastage of resources. The cost of a pharmacovigilance system, compared with the cost of ADRs to a nation and to the total national expenditure on medicines, is small (see Introduction). The idea that pharmacovigilance is a luxury, affordable only in the developed world, should be replaced by the realization that a reliable system of pharmacovigilance is essential for the rational, safe and cost-effective use of medicines in all countries and consequently for public health, and should produce clear advantages in relation to cost. Pharmacovigilance has developed and will continue to develop in response to the special needs and according to the strengths of members of the WHO Pharmacovigilance Program. The ultimate benefit is the safe, rational, and effective use of medicines by patients. [23]
Effectiveness and Risk Assessment of Therapies:
Effectiveness and risk: benefit and harm:
Estimating the risk and benefit of medicines among the populations exposed to them is essential to promote their rational and safe use and will enhance the tolerability and acceptability of mass-treatment programs. The effectiveness and risk profiles of many of the medicines used in PHPs in the past have been established by long experience rather than based on epidemiological evidence. The modern approach to public health requires that advice be given on the best general ways of approaching the management of diseases, notwithstanding the necessity for considerable freedom to modify therapy according to individual needs. The Council for International Organizations of Medical Sciences has produced a monograph that gives much helpful practical advice on how to assemble information on both effectiveness and risk, and points out some of the potential pitfalls in evaluation. It proposes that the context of the evaluation should be quite clear and that any value judgements must be transparent. Nevertheless, the likely imbalance between the effectiveness data and risk data in terms of quantity, quality and the sources, remains a difficulty that is rarely addressed explicitly in comparative studies of therapies, whether pharmaceutical or other (such as surgery). Therefore, as medicine development progresses at a rapid pace, and WHO proactively, in partnership with industry, promotes the use of new medicines for the control of diseases in developing countries, there will be a paradigm shift in approach to ADR monitoring of medicines used in national programs. Estimating the risk and benefit of medicines for the populations exposed to them is essential to promote their rational and safe use and will enhance the acceptability and tolerability of mass- treatment programs. This estimation requires the monitoring of programs to detect, evaluate and prevent adverse reactions, including effects on pregnant women, the elderly and children. [24]
Crisis management in Pharmacovigilance:
Any event that comes to public notice and threatens the health or safety of individuals or groups, or the reputation or stability of an organization. Crises usually erupt suddenly and dramatically; they require rapid and effective response and communications. [25]
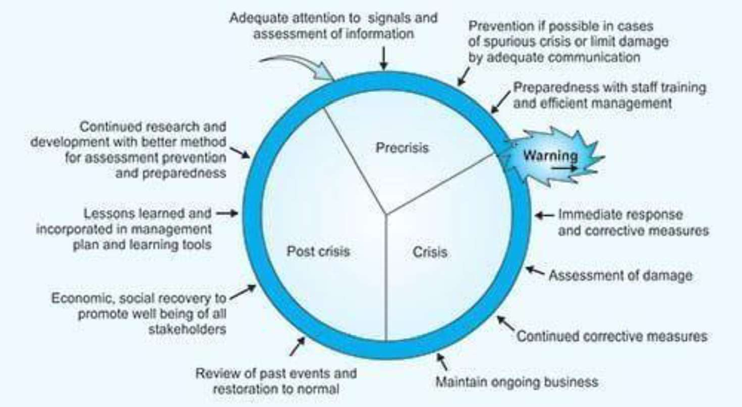
Management of a crisis requires not only resolution of the crisis event, but also very skilled management of the often-intense emotions and outrage that the public may feel. Any event that comes to public notice and threatens the health or safety of individuals or groups, or the reputation or stability of an organization. Crises usually erupt suddenly and dramatically; they require rapid and effective response and communications.
Pharmacovigilance and Public Health Programmes: Current Situation:
There can be better health outcomes as a consequence of good information on safety, which allows the early identification and prevention of adverse reactions, resulting in the more rational use of medicines, and better adherence within the target population.
1. Strengths:
Recently there have been some initiatives within countries, or under the leadership of WHO, to create and develop subsystems for pharmacovigilance to monitor the specific products used in their PHPs (e.g., vaccines, antiretroviral therapy, antimalarial programs and anthelminthic programs). On the other hand, some developing countries already have established pharmacovigilance centers that function independently. This situation provides all the ingredients for developing a unique and efficient pharmacovigilance system within PHPs and to integrate both systems. Although there are fundamental limitations and weaknesses in both PHPs and pharmacovigilance systems, PHPs have some distinct advantages for undertaking pharmacovigilance, and pharmacovigilance systems can benefit from the experience of PHPs.
Although PHPs are well-established and are considered as crucial and essential for the health of any nation, pharmacovigilance often remains incorrectly perceived as a luxury. Discipline that governmental authorities cannot support and hence that only developed nations can afford. In most developing countries, there are insufficient resources within the public health system to undertake training and capacity building and to invest in systems for monitoring drug efficacy and safety. The major resources are often concentrated on developing PHPs to reduce disease morbidity and mortality and very few of these countries have a well- established pharmacovigilance system. In most cases, PHP managers are neither aware of nor trained in the need to detect and report adverse reactions to the medicines that are used in their programs and that have been on the market for a long time. In general, pharmacovigilance is not seen as a component of public health. The reasons for this include a misunderstanding of the meaning and the objectives of the discipline; the absence of facilities for receipt, management and analysis of reports; and lack of a reporting culture. It is hoped that this document will encourage clinical program managers to develop a comprehensive understanding of the importance of pharmacovigilance. [26]
Integration of Pharmacovigilance into Public Health Programmes:
Introduction
It is important to emphasize that the survival of a PHP may depend on good pharmacovigilance. The specific needs of countries and program managers in public health for their pharmacovigilance programs will differ as new initiatives are undertaken, and the efforts required will depend on the existing systems and infrastructure. It is important to emphasize that survival of a PHP may depend on good pharmacovigilance. Some countries have well-developed, functioning, national pharmacovigilance centers, which are backed by an MRA. In such countries there is also a strong public health department with separate staff dealing with each vertical disease-related program. In other countries, the public health department may employ the same staff to handle different disease programs and pharmacovigilance centers may be rudimentary or absent. National pharmacovigilance centers may be centralized or decentralized. In different countries public health departments may function at different levels such as the primary, district, state and/or country levels. The pharmacovigilance in public health model needs to be robust and flexible if it is to be implementable not only in countries with pre-existing public health and pharmacovigilance systems, but also in countries with weak or deficient public health and pharmacovigilance programs. The model should emphasize sharing of human resources and the expansion of knowledge on effectiveness/risk, collaboration, effective communication, integration, training and capacity building. [27]
Justification:
Adverse reactions are a significant cause of morbidity and mortality and can affect adherence to treatment schedules and increase the risk of resistance and relapse of the disease. The use of pharmaceutical preparations is one of the fastest-growing components of health care expenditure throughout the world. It accounts for 30% of the total health budget in many countries. At the same time, adverse reactions are a significant cause of morbidity and mortality. In some countries there are now high public expectations for the safe delivery of health care, but the public rarely recognizes that pre-approval studies are not sufficient to truly characterize the effectiveness and risks of pharmaceutical products. Good pharmacovigilance practice can generate the evidence that will inspire public confidence and trust.
Requirements for pharmacovigilance in public health:
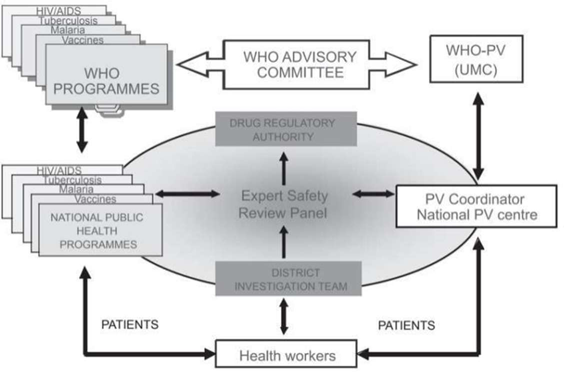
The pharmacovigilance in public health plan for a country should address these functional requirements, give details of the flow of data including feedback, and produce clear organigrams specifying roles and responsibilities. The actual designations of staff, physical locations, exact levels of responsibilities (e.g., national, state, district, primary health Centre, village) will vary between countries and will depend on existing health care and regulatory structures in the country. [28]
Exposure during pregnancy:
New medicines become available with little or no information on safety when used by pregnant women. To assess the safety of a medicine during pregnancy, it is essential that all women of child-bearing age are followed up to see if they were pregnant at the time of exposure to the medicine in question. Before administration of the medicine to a woman of childbearing age, questions should be asked about the possibility that the woman is pregnant, but because many women, particularly in rural areas, may not be aware of their pregnancy in the early months, it is necessary to check later to see if they were pregnant at the time. [,29]
Deaths:
It is important that all unexpected deaths following administration of the program medicine are investigated. In many areas, and in the absence of routine follow- up, problems will arise in identifying these deaths, but a system of notification appropriate to the area should be established. In each case, the cause of death will need to be established as accurately as possible.
Spontaneous reporting:
Spontaneous reporting is a system whereby case reports of adverse drug events are voluntarily submitted by health professionals, pharmaceutical companies or consumers to the national pharmacovigilance Centre. The type of reporting described in this document so far should be considered spontaneous. However, in PHPs, reporting should be more focused and intensive. Such reporting is sometimes referred to as intensified spontaneous reporting, or ideally, prospective monitoring should be undertaken as described below. [29]
Cohort event monitoring:
All adverse events are recorded in the study, not only suspect adverse reactions. This makes the method particularly effective at identifying previously unrecognized and unsuspected adverse reactions. This requires a record of patients to whom the medicine is administered. The means of recording this information will be best established when planning the PHP and may vary depending on the country (and perhaps the region), the program and the medicine being monitored [30,31]
Roles and responsibilities:
Where established, the national pharmacovigilance center will be responsible for the development of pharmacovigilance in the public health system, will promote pharmacovigilance in the PHPs and sensitize professionals and public health staff to the reporting of adverse reactions and irrational use of medicines.
Patients and the public
Public awareness about adverse reactions, early reporting and management are essential for ensuring patient confidence, in and adherence to, pharmacotherapy. In some countries patient reporting is accepted and can add value, but this needs to be separate from reporting by health professionals. In some programs (e.g. AIDS), the input and involvement of patient interest groups can be sought while formulating the program and should be part of the feedback communication link.
Primary health-care workers
It is the responsibility of the primary health-care provider to detect, investigate, manage and report ADRs. These staff will need training on the importance of adverse reactions, diagnosis, the basic principles of causality assessment and the important elements of the adverse reactions reporting form [32].
Other health-care workers:
Health-care workers outside the government system should also report adverse reactions. These would include, among others, nongovernmental organizations and charitable health facilities.
4.National medicines regulatory authority:
The regulatory authority will receive reports and recommendations from the ESRP. It will perform risk assessment and consider options for regulatory action which may involve requiring the manufacturers to make changes in the labelling of their product or may be a restriction in the use of the product, a temporary suspension or complete withdrawal. The regulatory authority may liaise with other national MRAs and it should always pass on the information on any action taken to WHO.
5. The national public health and pharmacovigilance programs:
The national pharmacovigilance center will be responsible for the development of pharmacovigilance in the public health system. The center, jointly with the PHP, should decide, on a continuous basis, priorities in pharmacovigilance for the PHP, whether all or only a few priority medicines will be monitored, when to review adverse reactions, the duration of monitoring and the time frames for reporting and action, and should evaluate the safety of the program. The national pharmacovigilance center will link with WHO for technical and policy advice. It should also assist the national pharmacovigilance coordinator in training activities. The center will promote pharmacovigilance in the PHPs and sensitize professionals and public health staff to the reporting of adverse reactions and irrational use of medicines.
6. The media:
The media have an important role in creating awareness in the community and among professionals. The price declaration (Annex 4) urges all players, including the media, to strive towards the highest ethical, professional, and scientific standards in promoting the safe use of medicines. WHO has made considerable efforts to train medicine regulators and national immunization staff in communicating information to the media on adverse events following immunization It is useful to assess the impact of media communications on public awareness and attitudes as this will assist the development of future communication strategies [33].
Training and capacity building:
Public health staff will not have received the training or have the expertise necessary to deal with serious medicine-induced disease, unexpected adverse reactions, adverse reactions to new medicines or adverse reactions in vulnerable groups such as pregnant women, the very young or the very old. Training and capacity building in pharmacovigilance are required for staff working at peripheral health facilities because adverse reactions are not well understood and, in many countries are seldom detected and reported. Monitoring is often neglected or absent, and staff therefore need to be made aware that ADR monitoring is a part of good professional practice In most disease-endemic countries, public health-care providers and professionals have now been exposed to modern concepts of disease management. Most of those who have used standard medicines are familiar with some of the common medicine-related problems such as nausea following treatment with chloroquine. However, none of them will have the training and expertise to deal with serious medicine- induced disease, unexpected adverse reactions, adverse reactions to new medicines, or adverse reactions in vulnerable groups such as pregnant women, the very young and the very old. Training and capacity building are required to ensure that staff understand new prescribing practices for new medicines, the correct dosage regimens and how treatment failures are defined. In conjunction, they need to be taught the reaction profile of the medicines they are to use, how to identify ADRs, how to manage them, when to refer patients, the basic data elements required in an ADR report, how to report, to whom and when Training should be given to the entire team involved in the initial identification, investigation, management, and reporting. Training and update programs should involve the experts who are members of the ESRP. [32,33]
CONCLUSION:
Pharmacovigilance can strengthen dedicated national programs such as those for the control and treatment of tuberculosis, malaria, HIV/AIDS, schistosomiasis, human African trypanosomiasis, and immunization coverage. It is important that the traditional division between medicine safety on the one hand and PHPs on the other should be removed. It is nearly 40 years since the World Health Assembly and WHO committed themselves to developing the necessary scientific and clinical infrastructure to provide for surveillance and monitoring of the safety of medicines in general use. Much has been achieved since then. Pharmacovigilance, as the discipline has come to be known, is supported by the WHO Collaborating Centre for International Drug Monitoring, based in Uppsala, Sweden (the Uppsala Monitoring Centre), and a network of 78 countries that are now affiliated as contributing centers. The MRAs have come to depend increasingly on their national pharmacovigilance centers for the continuous review of the safety of medicines that they approve after licensing for general use, and for support of rational use of medicines particularly those in use in the public sector. Pharmacovigilance provides invaluable underpinning, or has the potential to do so, to dedicated national programs such as those for the control and treatment of tuberculosis, malaria, HIV/AIDS, schistosomiasis, human African trypanosomiasis and immunization coverage. It is also essential in providing the necessary infrastructure for essential drugs programs. Health ministries, health professionals and the public can all be reassured by knowing that there is a competent and functional system in place that focuses on the safety of medicines used in the prevention and treatment of disease, including vaccines and pharmaceuticals for family planning. It is all the more important that there should be dependable monitoring of the safety of medicines as they become increasingly potent and more widely available. Experience has shown that for a country to be able to rely on its own pharmacovigilance program a number of elements need to be in place.
REFERENCES



Saroj Kumari*, Priya Sharma, Rizul Kumar, Pharmacovigilance Challenges in Community Pharmacy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2309-2322. https://doi.org/10.5281/zenodo.15645641
 10.5281/zenodo.15645641
10.5281/zenodo.15645641
