1B. Pharmacy student, NRI College of Pharmacy, Pothavarappadu, Agiripalli, Eluru district,
212th Grade student, Delhi Public School, Vijayawada, Krishna district,
3Professor, Department of Pharmacology, NRI College of Pharmacy, Pothavarappadu, Agiripalli, Eluru district.
Asparagus racemosus, commonly known as Shatavari, is a prominent medicinal herb in Ayurvedic medicine, traditionally used for managing a variety of female reproductive health conditions. Among these, menorrhagia or excessive menstrual bleeding represents a significant clinical challenge due to its multifactorial etiology involving hormonal imbalance, endometrial hyperactivity, inflammation, oxidative stress, and uterine dysfunction. This review provides an in-depth analysis of the pharmacological potential of Shatavari in managing menorrhagia and related gynaecological disorders, integrating traditional knowledge with modern biomedical evidence. Phytochemically rich in steroidal saponins (e.g., Shatavarin IV), flavonoids, and polyphenols, Shatavari exhibits phytoestrogenic, anti-inflammatory, antioxidant, endometrial-stabilizing, hematopoietic, and adaptogenic activities. These properties contribute to its ability to modulate oestrogen receptors, reduce cytokine-mediated inflammation, stabilize oxidative damage to endometrial tissue, and promote hormonal balance. Additionally, evidence suggests potential uterotonic and anti-spasmodic effects that may support menstrual regularity and comfort. Preclinical toxicological assessments confirm a high safety margin, although clinical data remain limited and warrant rigorous investigation through standardized clinical trials. Modern advancements in extraction technologies, nano formulation, and omics-based pharmacology offer promising avenues for enhancing bioavailability and mechanistic understanding. This review also highlights translational gaps, including the need for dose standardization, regulatory recognition, and global integration into evidence-based gynecological care. Altogether, Shatavari presents as a compelling candidate for natural, multi-targeted intervention in menorrhagia and beyond, meriting further exploration within integrative and personalized medicine paradigms.
The increasing global interest in herbal and alternative medicine reflects a growing need for safer and more sustainable therapeutic options, especially in areas where conventional treatments are associated with side effects or limited accessibility. In the context of women's health, particularly disorders of the menstrual cycle, traditional botanicals like Asparagus racemosus commonly known as Shatavari have been extensively used in Ayurvedic medicine for centuries. Shatavari has gained recognition for its beneficial effects on reproductive health, lactation, hormonal balance, and menstrual regulation. Among its various uses, its potential role in managing menorrhagia a condition of abnormally heavy or prolonged menstrual bleeding has sparked interest due to its multifaceted pharmacological properties [1,2]. Menorrhagia affects approximately 10–30% of women of reproductive age worldwide, significantly impairing quality of life by causing anaemia, fatigue, and social discomfort. The standard therapeutic approaches include non-steroidal anti-inflammatory drugs (NSAIDs), hormonal contraceptives, tranexamic acid, and, in severe cases, surgical procedures like endometrial ablation or hysterectomy. These interventions, while effective for some, are often associated with adverse effects, contraindications, and poor adherence. Furthermore, women in low-resource settings may not have consistent access to these therapies. This creates a substantial need for alternative treatment strategies that are both effective and well-tolerated. Herbal remedies like Shatavari offer a promising solution, as they are widely accessible and culturally accepted in many parts of the world [3,4]. Shatavari is a climbing plant from the Liliaceae family, native to tropical and subtropical regions of India, Sri Lanka, and Southeast Asia. The roots of the plant are the primary source of its medicinal properties and are often dried and ground into powder or decocted for oral use. The name “Shatavari” in Sanskrit translates to “the woman with a hundred husbands,” reflecting its traditional role as a tonic for female vitality and fertility. The pharmacological potential of Shatavari is largely attributed to its rich phytochemical content, which includes steroidal saponins (shatavarins I–IV), flavonoids, alkaloids, tannins, mucilage, and polyphenols. Among these, shatavarin IV is particularly noteworthy for its estrogenic activity and hormonal modulation capabilities [5–7]. In Ayurvedic literature, Shatavari is classified as a “Rasayana,” or rejuvenative herb, often recommended for female reproductive disorders such as menorrhagia, dysmenorrhea, infertility, and menopausal symptoms. Its effects are believed to be mediated through balancing the “doshas,” especially Vata and Pitta, and nourishing the reproductive tissues (Shukra dhatu). Ayurvedic physicians have long used Shatavari to restore hormonal balance, enhance uterine tone, and reduce excessive uterine bleeding, making it a cornerstone of herbal gynaecology in traditional medicine systems [8,9]. Modern pharmacological studies have begun to validate many of these traditional uses. Research indicates that Shatavari possesses significant estrogenic activity by interacting with oestrogen receptors and influencing the hypothalamic-pituitary-ovarian (HPO) axis. Experimental studies on rodents have shown that Shatavari root extracts increase serum levels of oestradiol and modulate the secretion of gonadotropins such as LH and FSH. These hormonal shifts can contribute to the stabilization of endometrial lining and reduction in menstrual blood loss. Such mechanisms are particularly relevant in the management of menorrhagia, where hormonal imbalances often play a central role [10–12]. In addition to its hormonal effects, Shatavari exhibits strong anti-inflammatory and antioxidant properties. Its flavonoid and polyphenolic constituents inhibit the cyclooxygenase (COX) and lipoxygenase (LOX) pathways, thereby reducing the synthesis of pro-inflammatory prostaglandins. Elevated levels of prostaglandin F2α have been implicated in uterine hypercontractility and increased menstrual blood loss. By modulating these inflammatory pathways, Shatavari may help alleviate pain and bleeding associated with menorrhagia. Moreover, its antioxidant potential aids in mitigating oxidative stress within endometrial tissues, which has been linked to menstrual irregularities and chronic uterine inflammation [13–15]. Recent in vitro and in vivo findings have also demonstrated Shatavari’s mild haemostatic effect, possibly through modulation of platelet function and enhancement of coagulation profiles. Although these findings are preliminary, they suggest an added benefit in conditions like menorrhagia where excessive bleeding is a primary concern. Furthermore, its adaptogenic properties support endocrine resilience by normalizing stress-related fluctuations in cortisol and gonadal hormones, which can further impact menstrual regularity. As an immunomodulator, Shatavari enhances the function of macrophages and lymphocytes, potentially improving immune-endocrine interactions within the female reproductive tract [16–18]. Shatavari’s therapeutic value is not limited to menorrhagia. It has shown potential in treating a range of other gynaecological and systemic conditions, including polycystic ovary syndrome (PCOS), premenstrual syndrome (PMS), menopausal symptoms, and postpartum lactation failure. Its galactagogue action is attributed to prolactin-enhancing effects, while its role in mood stabilization and neuroprotection is linked to serotonergic and GABAergic modulation. These diverse actions suggest that Shatavari may offer holistic support to women throughout various phases of their reproductive life span [19–21]. Despite promising pharmacological evidence and traditional acclaim, the clinical validation of Shatavari in the management of menorrhagia remains limited. Most of the current data derive from small-scale animal studies or observational trials with limited controls. There is a pressing need for well-designed, randomized controlled clinical trials to determine optimal dosing, safety profiles, pharmacokinetics, and long-term outcomes. Additionally, standardization of Shatavari extracts based on bioactive markers like shatavarin IV is essential for ensuring consistency in therapeutic results. Only through rigorous scientific investigation can Shatavari be fully integrated into evidence-based clinical practice for managing menorrhagia and related conditions [22–24]. Given the increasing burden of menstrual disorders worldwide and the limitations of conventional treatments, exploring the full pharmacological potential of Shatavari is both timely and necessary. This review aims to consolidate the available pharmacological data supporting Shatavari’s role in managing menorrhagia, with a focus on its hormonal, anti-inflammatory, antioxidant, and haemostatic effects. Furthermore, it highlights the need for translational research to bridge the gap between traditional knowledge and modern clinical applications. In doing so, it offers a comprehensive perspective on Shatavari as a natural therapeutic agent for menstrual health and beyond. In recent years, advanced analytical methods such as high-performance liquid chromatography (HPLC), gas chromatography-mass spectrometry (GC-MS), and nuclear magnetic resonance (NMR) spectroscopy have facilitated the standardization and quality control of Shatavari extracts. These techniques are essential for quantifying key bioactive constituents, especially steroidal saponins like shatavarin IV, which are considered responsible for its estrogenic and adaptogenic effects. Standardization ensures consistency in pharmacological efficacy and minimizes the variability often associated with crude herbal preparations. Additionally, metabolomic profiling has begun to identify new potential biomarkers for Shatavari's pharmacological activity, opening avenues for targeted formulation development [25–27]. Ethnomedical records across various Indian subcultures and other South Asian regions consistently support the use of Shatavari in female health. In traditional Unani and Siddha medicine, it is similarly employed for its restorative effects on the female reproductive system. Tribal practitioners in central India use Shatavari root paste for menstrual cramps and to arrest excessive uterine bleeding. These community-level practices, passed down through generations, have largely remained undocumented in scientific literature. However, their convergence with formal pharmacological findings suggests that centuries of empirical use may align with measurable therapeutic outcomes, meriting more comprehensive ethnobotanical documentation [28,29]. Despite the widespread usage of Shatavari, global integration into mainstream medicine is still limited due to concerns related to herbal pharmacovigilance. The lack of stringent regulation and product variability across different brands raises safety and efficacy concerns. Adverse event reporting, interaction with conventional drugs (such as anticoagulants or hormonal agents), and potential contraindications in hormone-sensitive conditions must be thoroughly investigated through rigorous clinical pharmacology frameworks. It is equally important to consider patient-centred outcomes and cultural acceptability when designing such studies, especially in reproductive and menstrual health, where treatment adherence is closely tied to cultural beliefs and experiences [30–32]. Polyherbal formulations containing Shatavari are widely marketed for gynaecological indications, often in combination with herbs like Saraca indica (Ashoka), Symplocos racemosa (Lodhra), and Boerhaavia diffusa (Punarnava). These synergistic blends aim to offer a multi-targeted therapeutic approach, improving efficacy in conditions like menorrhagia, leucorrhea, and menstrual irregularities. However, while traditional formulations offer theoretical synergism, their complex compositions make it difficult to attribute specific therapeutic effects to individual herbs. This necessitates more focused pharmacodynamic studies, both on mono-herbal extracts of Shatavari and on standardized polyherbal combinations, to delineate their respective contributions and interaction profiles [33,34]. Another crucial dimension in understanding Shatavari’s clinical utility is its pharmacokinetics. Preliminary animal models suggest moderate oral bioavailability and hepatic metabolism of its steroidal saponins. However, detailed human pharmacokinetic profiles, including absorption rates, tissue distribution, and elimination pathways, remain inadequately explored. Advances in nanotechnology and drug delivery systems have also prompted interest in encapsulated or nano formulated Shatavari extracts, which may improve bioavailability and target-specific delivery to reproductive tissues. Such innovations could optimize therapeutic response while reducing required doses and side effects [35–37]. In the context of global health priorities, plant-based therapies such as Shatavari hold significant promise in addressing menstrual health inequities. Women in low- and middle-income countries (LMICs) often lack access to menstrual health products and treatments, increasing reliance on traditional remedies. Formal validation of such remedies through pharmacological and clinical studies can not only expand therapeutic options but also empower local healthcare systems and communities by integrating culturally familiar solutions into primary care. The World Health Organization (WHO) has emphasized the importance of developing evidence-based traditional medicine protocols for non-communicable diseases, including reproductive disorders a goal aligned with research on Shatavari [38–40]. In summary, Shatavari stands at the intersection of traditional wisdom and modern pharmacology. Its multifaceted pharmacological actions including hormonal modulation, anti-inflammatory and antioxidant properties, haemostatic activity, adaptogenic effects, and immunomodulation make it a compelling candidate for the management of menorrhagia and broader gynaecological conditions. However, realizing its full therapeutic potential requires more rigorous research, including standardization, pharmacokinetic profiling, toxicity studies, and large-scale randomized controlled trials. This review aims to provide a consolidated, evidence-informed analysis of the pharmacological mechanisms underlying Shatavari’s use in menorrhagia and beyond, and to lay the groundwork for its clinical integration as a safe and effective therapeutic agent in women's health.
Pathophysiology and Symptoms of Menorrhagia
Menorrhagia, defined as excessive and/or prolonged menstrual bleeding, is one of the most common gynecological complaints among women of reproductive age. Clinically, it is characterized by menstrual blood loss exceeding 80 mL per cycle or menstruation lasting longer than 7 days, occurring at regular intervals [50]. The pathophysiology of menorrhagia is multifactorial, involving disruptions in endometrial haemostasis, hormonal imbalance, uterine structural abnormalities, and local or systemic factors that interfere with coagulation and vascular integrity. At the hormonal level, dysregulation of the hypothalamic-pituitary-ovarian (HPO) axis plays a significant role in many cases of menorrhagia. Anovulatory cycles are particularly implicated, as the absence of ovulation leads to sustained unopposed oestrogen stimulation without the balancing effect of progesterone. This results in excessive endometrial proliferation, inadequate stabilization, and asynchronous shedding, leading to unpredictable and heavy menstrual bleeding [51]. In ovulatory menorrhagia, altered levels of prostaglandins, especially elevated prostaglandin E2 and F2α, contribute to enhanced vasodilation, increased vascular permeability, and dysregulated uterine contractions, exacerbating menstrual blood loss [52]. From a haemostatic perspective, disturbances in local coagulation mechanisms within the endometrium have been documented. Women with menorrhagia often exhibit altered expression of fibrinolytic enzymes, tissue plasminogen activator (tPA), plasminogen activator inhibitor-1 (PAI-1), and matrix metalloproteinases (MMPs), resulting in enhanced fibrinolysis and reduced clot stability [53]. Additionally, aberrant angiogenesis marked by increased vascular endothelial growth factor (VEGF) and dysfunctional remodelling of spiral arterioles contributes to fragile vasculature prone to excessive bleeding [54]. Structural uterine anomalies, such as fibroids (leiomyomas), endometrial polyps, adenomyosis, and intrauterine devices (IUDs), can also disrupt normal menstrual flow by distorting the endometrial cavity, increasing endometrial surface area, and inducing local inflammatory changes. Inflammatory mediators such as interleukins (IL-1β, IL-6), TNF-α, and prostaglandins are often elevated in these conditions, perpetuating local vascular dysfunction and excessive bleeding [55]. In systemic disorders, such as coagulopathies (e.g., von Willebrand disease, thrombocytopenia) or thyroid dysfunction, menorrhagia may be a prominent symptom due to impaired clot formation or altered metabolic regulation of the menstrual cycle. Moreover, certain medications like anticoagulants, hormonal therapies, and chemotherapeutic agents may induce or worsen menstrual bleeding patterns [56].
Women with menorrhagia typically present with symptoms including:
Psychosocial impacts are also significant, with affected women reporting embarrassment, social withdrawal, reduced productivity, and diminished quality of life. The burden of menorrhagia is thus not limited to physical symptoms but also extends to emotional and occupational domains. Given the diverse etiologies and symptomatology, an accurate diagnosis of menorrhagia often requires a combination of clinical evaluation, laboratory testing (e.g., complete blood count, coagulation profile, thyroid function), imaging (e.g., transvaginal ultrasound), and sometimes hysteroscopy or endometrial biopsy to rule out malignancy or structural causes. Treatment strategies are tailored according to etiology, severity, patient age, reproductive goals, and treatment response. However, when pharmacologic or surgical options are contraindicated or poorly tolerated, herbal agents like Asparagus racemosus are increasingly being explored as alternative or adjunctive therapies with promising preclinical support.
Table 1: Common Symptoms of Menorrhagia.
|
Symptom |
Description |
|
Heavy Menstrual Flow |
Soaking through ≥1 sanitary pad or tampon per hour for several consecutive hours. |
|
Prolonged Menstrual Bleeding |
Bleeding lasting more than 7 days. |
|
Large Blood Clots |
Passage of clots larger than 2.5 cm in diameter. |
|
Nocturnal Bleeding |
Waking up at night to change protection due to excessive bleeding. |
|
Double Protection Needed |
Requirement to use both pads and tampons simultaneously. |
|
Activity Restriction |
Limitation of daily work, school, or social activities due to bleeding. |
|
Fatigue and Weakness |
General tiredness due to blood loss and possible anaemia. |
|
Anaemia Symptoms |
Dizziness, pale skin, breathlessness, and palpitations. |
|
Emotional and Social Distress |
Feelings of embarrassment, anxiety, or social withdrawal. |
History of Shatavari (Asparagus racemosus)
The history of Shatavari (Asparagus racemosus) is intricately woven into the fabric of traditional South Asian medicine, where it has been cherished for over 3,000 years. Rooted in Ayurvedic philosophy, Shatavari is one of the most revered plants in the treatment of women’s health conditions. It appears in the Samhitas of Charaka and Sushruta, the foundational texts of Ayurveda, where it is described as a balya (strengthening), rasayana (rejuvenating), and stanyajanana (galactagogue) herb, used to support vitality, milk production, fertility, and hormonal regulation in women [58,59]. These early mentions were not merely symbolic; they indicated detailed therapeutic properties, dosages, and formulations, many of which are still followed today in Ayurvedic practice. In Charaka Samhita, Shatavari is recommended for disorders such as excessive menstrual bleeding, infertility, and internal heat disorders. In Sushruta Samhita, it is included in wound-healing formulations and vaginal pessaries for gynecological complaints. Shatavari was often prescribed in combination with ghee, honey, or milk to enhance its absorption and systemic effects [60]. These formulations indicate early knowledge of drug solubility and potentiation in traditional pharmacology. Beyond Ayurveda, Siddha medicine a Tamil system of medicine with roots parallel to Ayurveda has long recognized Shatavari (locally known as Tanneer vittan kizhangu) for its cooling, nourishing, and tonic effects, especially for female reproductive issues. In the Unani system, it is identified as Shaqaqul Misri and categorized as a mohallil (resolvent) and muqawwi-e-rahm (uterine tonic), traditionally used to relieve menorrhagia, leucorrhea, and uterine inflammation [61,62]. These cross-cultural applications in diverse systems of medicine highlight Shatavari’s pan-traditional reputation. The recognition of Shatavari was not confined to India alone. Ancient Sri Lankan, Nepalese, and Tibetan medical systems also documented its medicinal use. In Sri Lanka’s Deshiya Chikitsa, Shatavari has been employed for postpartum recovery and uterine toning. In Nepalese ethnomedicine, the roots are boiled into decoctions to treat vaginal infections, irregular menstruation, and even gastric ulcers, indicating the plant’s multifaceted role [63]. The botanical exploration of Shatavari began in earnest during the colonial era. British and European botanists catalogued Asparagus racemosus in several herbal compendia, such as The Flora of British India and Pharmacographia Indica, where it was noted for its galactagogue and uterotonic effects. Pharmacognostic interest in the West grew steadily, and early chemical analyses isolated saponins that mirrored the activity of endogenous oestrogens. Colonial surgeons and medical officers observed its clinical use among indigenous healers and recognized its potential, albeit with limited mechanistic understanding at the time [64]. In the 20th century, with the global resurgence of interest in complementary and alternative medicine (CAM), Shatavari found new life in integrative health paradigms. The World Health Organization has since acknowledged Asparagus racemosus in its medicinal plant monographs, encouraging further phytochemical and pharmacological investigation [65]. It now appears in modern herbal pharmacopoeias and wellness products across Europe, Australia, Southeast Asia, and the Americas, particularly in formulations aimed at hormonal balance, menopause support, and female reproductive wellness. Botanically, Shatavari is a climbing plant native to the Indian subcontinent and parts of Southeast Asia, thriving in tropical and subtropical climates. Traditionally harvested from wild forests, especially in Maharashtra, Chhattisgarh, Odisha, Madhya Pradesh, and Rajasthan, the roots are considered the primary medicinal component. However, due to overharvesting and habitat destruction, wild populations have diminished. This has prompted its classification as a “vulnerable” species in certain states by the National Medicinal Plants Board (NMPB) and the IUCN, leading to the implementation of conservation cultivation protocols under India’s National AYUSH Mission [66,67]. Traditional agricultural practices, such as intercropping with legumes, and organic farming methods are being encouraged to sustainably cultivate Shatavari while preserving its phytochemical integrity. Several cultivars have now been developed for better yield and saponin content, enabling wider commercialization through Ayurvedic pharmaceutical industries. In the contemporary herbal trade, Shatavari root is now a commercially valuable medicinal plant featured in over 200 proprietary Ayurvedic formulations, such as Shatavari Kalpa, Stree Rasayan, Ashokarishta, and modern nutraceuticals for hormonal balance and menopause support. Globally, it is incorporated into functional foods, powders, capsules, and teas, reflecting both traditional wisdom and modern innovation. The history of Shatavari is not only a testament to its long-standing medicinal use but also reflects a fascinating journey from ancient pharmacopoeias to modern clinical interest. Its cultural relevance, therapeutic breadth, and continued research interest make it a unique herb bridging tradition and evidence-based medicine in the domain of women’s health.
Drug Profile: Shatavari (Asparagus racemosus):
Table 2: Drug profile of Shatavarin.
|
Parameter |
Details |
|
Botanical Name |
Asparagus racemosus Willd. |
|
Common Names |
Shatavari (Sanskrit), Wild Asparagus (English), Shaqaqul Misri (Unani), Tanneer Vittan Kizhangu (Siddha) |
|
Family |
Asparagaceae |
|
Plant Part Used |
Tuberous roots |
|
Plant Description |
Climbing plant with needle-like leaves and small white flowers; roots are cylindrical, fleshy, and clustered. |
|
Traditional System of Medicine |
Ayurveda, Unani, Siddha, Folk Medicine |
|
Rasa (Taste) |
Madhura (Sweet), Tikta (Bitter) |
|
Guna (Quality) |
Snigdha (Unctuous), Guru (Heavy) |
|
Virya (Potency) |
Sheeta (Cooling) |
|
Vipaka (Post-digestive Effect) |
Madhura (Sweet) |
|
Pharmacological Classification |
Rasayana (Rejuvenative), Stanyajanana (Galactagogue), Balya (Tonic), Hridya (Cardioprotective) |
|
Major Bioactive Constituents |
Steroidal saponins (Shatavarins I–IV), flavonoids, alkaloids, isoflavones, mucilage, tannins, polyphenols |
|
Mechanism of Action |
Phytoestrogenic activity via ER receptor modulation; antioxidant action; anti-inflammatory cytokine inhibition; hormonal regulation |
|
Primary Pharmacological Actions |
Estrogenic, Galactagogue, Adaptogenic, Antioxidant, Anti-inflammatory, Immunomodulatory, Gastroprotective |
|
Therapeutic Uses |
- Menorrhagia- Female infertility- Dysmenorrhea- Menopausal symptoms- Lactation support- Gastric ulcers- Anaemia- PCOS- Stress and anxiety |
|
Dosage (Ayurvedic Texts) |
Powder: 3–6 g/day Decoction: 50–100 ml/day (in divided doses)Capsules: 250–500 mg twice daily (standardized extract) |
|
Available Formulations |
Churna (powder), Ghrita (medicated ghee), Kalpa (granules), Tablets, Syrup, Capsules |
|
Toxicity and Safety |
Considered safe in traditional doses; high doses may cause mild GI upset. No significant toxicity observed in sub-chronic studies. |
|
Contraindications |
None established, but use cautiously in oestrogen-sensitive conditions unless clinically justified. |
|
Pregnancy & Lactation |
Traditionally used during pregnancy and lactation under professional supervision; recent studies support galactagogue use postpartum. |
|
Regulatory Status |
Approved under Ayurvedic Pharmacopeia of India (API); listed in WHO monographs on medicinal plants |
|
Storage Conditions |
Store in a cool, dry place away from sunlight to preserve bioactivity and prevent moisture contamination. |
Pharmacological Uses of Shatavari (Asparagus racemosus)
The pharmacological utility of Asparagus racemosus (Shatavari) spans across multiple organ systems and therapeutic categories. Its actions are mediated through a rich matrix of bioactive compounds, primarily steroidal saponins (e.g., shatavarins I–IV), flavonoids, alkaloids, isoflavones, polysaccharides, and tannins. These constituents collectively contribute to its adaptogenic, endocrine-modulating, and tissue-protective actions, many of which are particularly relevant to female reproductive health, including menorrhagia, while also offering system-wide benefits.
1. Gynecological and Reproductive Health
Shatavari is arguably best known for its role in female reproductive medicine, particularly in Ayurvedic gynaecology. It exerts a normalizing effect on the menstrual cycle, alleviating heavy, irregular, or painful periods through its combined estrogenic, anti-inflammatory, and spasmolytic activities. Its use in menorrhagia is supported by studies indicating a regulatory influence on the hypothalamic-pituitary-ovarian axis, which modulates oestrogen and progesterone levels [68,79]. Furthermore, Shatavari supports ovarian follicular development, improves ovulatory rates, and enhances endometrial receptivity, making it beneficial in infertility and luteal phase defects. Studies have shown increased ovarian weight and improved follicle-stimulating hormone (FSH) and luteinizing hormone (LH) profiles in rodent models [80].
2. Support During Menopause and PMS
Shatavari plays a central role in managing menopausal syndrome, where declining oestrogen levels lead to hot flashes, mood disturbances, vaginal dryness, and cardiovascular risks. The plant’s phytoestrogenic saponins help alleviate vasomotor symptoms and prevent bone demineralization by interacting with oestrogen receptors [81]. Additionally, its mood-stabilizing and anxiolytic actions support mental health during premenstrual and perimenopausal phases.
3. Digestive and Gastrointestinal Health
Traditionally described as a pittashamaka (pitta-dosha pacifying) herb, Shatavari demonstrates gastroprotective and anti-ulcer activity. It reduces gastric acid secretion, enhances mucus secretion, and inhibits gastric wall cell damage through flavonoid-mediated antioxidant action [73,82]. It is commonly prescribed in Ayurveda for hyperacidity, gastritis, peptic ulcers, and intestinal inflammation. Moreover, it supports gut microbiota balance, and recent studies suggest prebiotic-like activity, promoting beneficial Lactobacillus and Bifidobacterium growth [83].
4. Immunomodulatory and Hematopoietic Activity
Shatavari enhances both innate and adaptive immunity. Polysaccharide fractions from its roots stimulate macrophage phagocytic activity and increase immunoglobulin production, while simultaneously regulating T-helper and T-regulatory cell activity [70,71]. These effects make it useful in chronic inflammatory, autoimmune, and post-infectious fatigue syndromes. Further, Shatavari has been shown to increase red blood cell (RBC) count, haemoglobin levels, and platelet counts in animal models, indicating its potential role in anaemia associated with menorrhagia and other bleeding disorders [84].
5. Neuroprotective and Cognitive Enhancement
Emerging studies support Shatavari’s nootropic and neuroprotective effects, where its antioxidant and anti-inflammatory properties counteract neurodegeneration, particularly in stress-induced and age-related models. Improvement in spatial memory, learning behaviour, and cholinergic activity has been observed in preclinical trials [74,85]. Its adaptogenic profile helps attenuate hypothalamic-pituitary-adrenal (HPA) axis overactivity and cortisol-induced damage.
6. Anti-diabetic and Metabolic Benefits
In streptozotocin-induced diabetic models, Shatavari root extract has been observed to lower fasting blood glucose, glycated haemoglobin (HbA1c), and oxidative markers while improving pancreatic β-cell regeneration and insulin sensitivity [86]. These metabolic effects may support women with polycystic ovary syndrome (PCOS), a condition often associated with insulin resistance and menstrual irregularities.
7. Renal Protective Effects
Renal-protective actions of Shatavari have been reported in models of drug-induced nephrotoxicity, where it reduced serum urea, creatinine, and oxidative injury to renal tubules. These nephroprotective effects are valuable, especially in women undergoing long-term NSAID therapy for menstrual or pelvic pain [87].
8. Lactation and Postpartum Recovery
Shatavari's historical use in postpartum care is increasingly validated by research showing enhanced milk production, faster uterine involution, and reduced postnatal weakness. Phytoestrogens stimulate prolactin release and enhance mammary gland development, while its nutritive and anabolic effects aid in tissue repair and energy restoration [69,88].
9. Bone Health and Osteoprotective Properties
Shatavari has shown promise in osteoporosis models, where phytoestrogenic activity leads to increased bone mineral density, calcium retention, and improved bone microarchitecture. This suggests its potential use as a natural alternative to hormone replacement therapy (HRT) in postmenopausal osteoporosis [89].
10. Wound Healing and Dermatological Applications
The herb’s antimicrobial, anti-inflammatory, and fibroblast-stimulating properties make it effective in wound healing. Topical formulations of Shatavari have demonstrated accelerated wound contraction, collagen deposition, and epithelial regeneration in animal models [90].
Mechanistic Pathways of Shatavari (Asparagus racemosus) in Menorrhagia
Menorrhagia, defined as menstrual blood loss exceeding 80 mL per cycle or prolonged bleeding beyond 7 days, affects up to 30% of reproductive-age women. The underlying causes range from endocrine disorders and coagulopathies to iatrogenic and idiopathic etiologies. Shatavari has been widely used in traditional medicine to manage excessive menstrual bleeding, and recent in vitro and in vivo studies provide a mechanistic foundation for its therapeutic efficacy. The herb’s multifactorial pharmacodynamics include hormonal modulation, uterine stabilization, anti-inflammatory action, and hematopoietic support.
1. Phytoestrogenic Receptor Binding and Hormonal Regulation
The steroidal saponins in Shatavari particularly shatavarins I–IV act as plant-derived phytoestrogens. These compounds exhibit selective oestrogen receptor modulator (SERM)-like behaviour, which means they can exert estrogenic effects in tissues such as the uterus while being neutral or even antagonistic in others like the breast. This tissue-selective interaction supports their safety profile in long-term use [91].
By binding to ER-α and ER-β receptors, these saponins mimic endogenous oestrogen action in hypoestrogenic states, such as post-menstrual or perimenopausal phases. This interaction leads to:
These effects restore hormonal homeostasis, directly correcting the anovulatory cycles and unopposed oestrogen exposure that underlie many cases of dysfunctional uterine bleeding [92].
2. Endometrial Stabilization and Anti-Proliferative Activity
In oestrogen-dominant conditions, the endometrium becomes excessively thickened and hyper vascularized, increasing susceptibility to heavy bleeding. Shatavari regulates endometrial dynamics by:
Additionally, its influence on the PI3K/Akt and Wnt/β-catenin pathways, which are central to endometrial proliferation, may contribute to the anti-hyperplastic and anti-secretory actions observed in preclinical models.
3. Anti-inflammatory and Cytokine Modulation
Endometrial inflammation is a key component in the pathogenesis of menorrhagia. Shatavari modulates inflammatory cascades by:
This anti-inflammatory profile contributes not only to reduced menstrual blood loss but also to pain relief, particularly in cases of menorrhagia with dysmenorrhea.
4. Antioxidant Protection of Endometrial Tissue
Oxidative stress is increasingly recognized in the pathophysiology of abnormal uterine bleeding. Elevated reactive oxygen species (ROS) can cause cellular apoptosis, endometrial instability, and impaired vascular integrity.
Shatavari root extracts are rich in flavonoids such as quercetin, kaempferol, and rutin, which exert antioxidant activity via:
Such antioxidant effects enhance endometrial resilience, promote tissue healing, and reduce oxidative tissue injury associated with irregular shedding.
5. Hematopoietic and Anti-anaemic Effects
Menorrhagia often results in iron-deficiency anaemia, manifesting as fatigue, pallor, and reduced work capacity. Shatavari supports haematopoiesis through:
Moreover, its natural iron and trace mineral content (including copper and manganese) may synergize with its hematopoietic actions. When co-administered with iron supplements or tonics, Shatavari has shown improved outcomes in haemoglobin recovery.
6. Uterotonic and Anti-spasmodic Activity
Shatavari has dual regulatory effects on uterine contractility. While mild uterotonic activity ensures complete evacuation of the endometrial lining, thus preventing residual tissue from perpetuating bleeding, its spasmolytic action helps alleviate uterine cramps and dysmenorrhea. Experimental studies demonstrate that methanolic extracts of Shatavari modulate calcium influx and prostaglandin-mediated contractions, leading to:
This dual effect supports both menstrual regulation and symptomatic relief.
7. Adaptogenic Modulation of HPA Axis
Chronic psychological stress is known to impact menstrual function via the hypothalamic–pituitary–adrenal (HPA) axis, leading to disruptions in gonadotropin release. Shatavari, classified as a rasayana (rejuvenative), acts as an adaptogen by:
These effects help reduce stress-induced menstrual irregularities, making Shatavari beneficial not only for physical but also psychosomatic contributors to menorrhagia.
Figure 1: Schematic Representation of Mechanistic Pathways of Shatavarin.
Clinical Implications and Translational Gaps in the Use of Shatavari (Asparagus Racemosus) for Menorrhagia
Despite compelling pharmacological evidence and longstanding traditional use, the clinical adoption of Asparagus Racemosus (Shatavari) in modern gynaecological therapeutics particularly for menorrhagia remains limited. Bridging this divide between bench and bedside necessitates a critical evaluation of existing clinical data, formulation challenges, regulatory barriers, and implementation science.
1. Clinical Evidence Supporting Use in Menstrual Disorders
While a rich ethnopharmacological tradition underlines Shatavari's role in regulating female reproductive health, controlled clinical evidence is comparatively sparse. Most studies available are small-scale or observational and often embedded in Ayurvedic multi-herbal formulations. A randomized clinical trial by Sharma et al. (2017) involving 60 women reported significant improvement in bleeding frequency and volume, but lacked biomarker correlation or long-term follow-up [99].mMoreover, Ayurvedic formulations like Pushyanuga Churna and Rajah Pravartini Vati, which contain Shatavari in combination with Ashoka (Saraca indica) and Lodhra (Symplocos racemosa), have shown positive outcomes in dysfunctional uterine bleeding (DUB), though their polyherbal nature complicates isolation of Shatavari's individual contribution [100].
What remains critically missing is:
The integration of AI-driven data mining and meta-analytic frameworks could help consolidate small trials to provide a broader evidence base [101].
2. Dosage Standardization and Phytochemical Consistency
One of the pivotal barriers in modern clinical practice is the absence of dose uniformity and lack of standardization across Shatavari preparations. Variability in:
can significantly affect levels of Shatavarin IV, asparagamine A, and flavonoid content, leading to inconsistent therapeutic outcomes [102]. The establishment of Good Agricultural and Collection Practices (GACP) and Standard Operating Procedures (SOPs) for cultivation, harvesting, and extraction are vital for batch-to-batch reproducibility. Moreover, implementation of Quality by Design (QbD) and chemical fingerprinting via HPLC/LC-MS should be mandated in all marketed formulations [103].
Future studies should also explore bioavailability-enhanced formulations such as:
3. Safety, Toxicity, and Drug-Herb Interactions
Although traditional usage indicates Shatavari's safety, modern regulatory frameworks demand comprehensive toxicological profiling. While acute and sub-chronic animal studies reveal no toxicity up to 2 g/kg body weight, data on:
are absent or inconclusive [105]. No significant adverse drug interactions have been documented, but given its estrogenic and immunomodulatory properties, caution is warranted in patients on:
In pregnant and lactating women, Shatavari is traditionally used to enhance milk production, yet clinical safety data based on RCTs or pharmacovigilance reports remain scarce [107].
4. Integration into Clinical Guidelines
Despite wide therapeutic use, Shatavari does not currently feature in:
Its exclusion reflects a broader disconnect between traditional systems and evidence-based medicine (EBM). For formal integration, evidence must be:
Collaboration between Ayurveda experts, clinicians, pharmacologists, and regulatory authorities is essential to evolve interdisciplinary clinical practice guidelines that include validated herbal alternatives like Shatavari, especially for functional uterine disorders [109].
5. Patient Perception, Accessibility, and Global Outreach
In India and Southeast Asia, Shatavari’s cultural acceptance and traditional legitimacy make it a household remedy for menstrual issues. However, in Western countries, several barriers limit its uptake:
Educational campaigns targeting both patients and healthcare providers can address misconceptions, particularly if coupled with:
Moreover, to ensure widespread access, standardized Shatavari formulations must be:
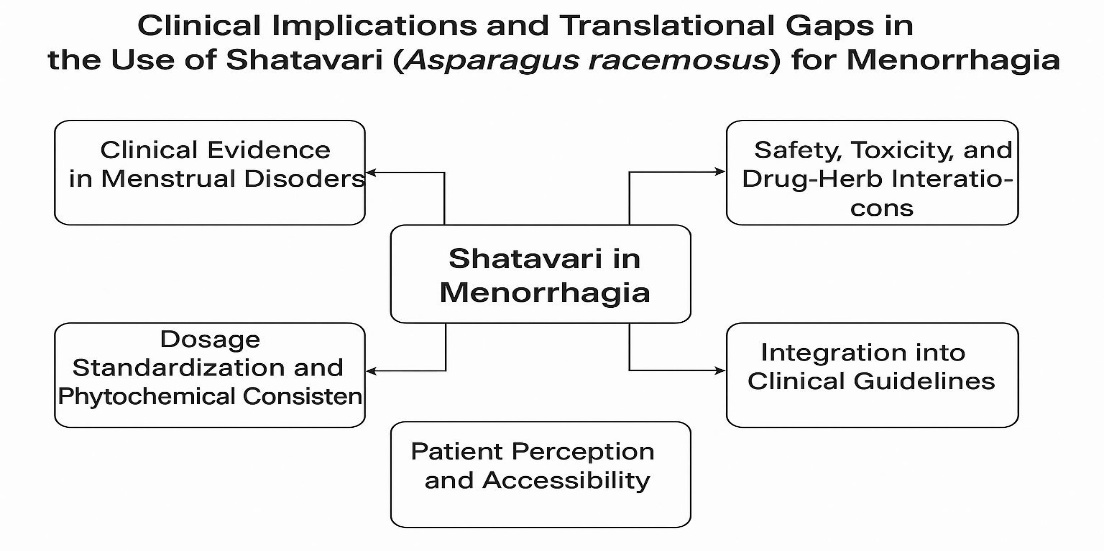
Figure 2: Schematic Representation of Clinical Implications and Translational gaps in use of Shatavarin.
Table 3: Summary of Clinical and Translational Considerations for Shatavari in Menorrhagia.
|
Domain |
Key Issues |
Implications |
|
Clinical Evidence |
Limited RCTs; small sample sizes; polyherbal studies dominate |
Need for high-quality monotherapy trials with objective endpoints |
|
Standardization |
Variable phytochemical content (e.g., Shatavarin IV); lack of extraction consistency |
Requires HPLC-based standardization and SOPs for cultivation and processing |
|
Dosage & Delivery |
No fixed clinical dose; low bioavailability in crude form |
Development of nano- or lipid-based standardized extracts |
|
Safety and Interactions |
Limited long-term toxicity data; potential risk with HRT, anticoagulants, etc. |
Comprehensive toxicological, pharmacovigilance, and interaction studies needed |
|
Regulatory Inclusion |
Absent in modern guidelines (NICE, ACOG); no EML status |
Needs evidence synthesis and clinical guideline proposals |
|
Cultural and Regional Use |
Accepted in India; poorly adopted in the West due to scepticism |
Requires education, cultural integration, and accessible consumer formulations |
|
Future Directions |
Lack of pharmacodynamic/kinetic profiling; no biomarker-linked studies |
Interdisciplinary research, AI-assisted meta-analysis, integrative approaches |
Pharmacological Applications of Shatavari (Asparagus racemosus) Beyond Menorrhagia
Beyond its traditional use in menstrual and reproductive health, Asparagus racemosus (Shatavari) demonstrates a wide array of pharmacological properties that span various physiological systems. Its broad therapeutic potential stems from its rich composition of bioactive constituents such as steroidal saponins (Shatavarins), alkaloids, flavonoids, and polysaccharides. These components act through multi-targeted mechanisms, making Shatavari a prime candidate for inclusion in modern polypharmacological strategies.
1. Galactagogue and Lactogenic Effects
Shatavari is historically considered one of the most effective herbal galactagogues in Ayurvedic postpartum care. Steroidal saponins, particularly Shatavarin IV, are believed to enhance prolactin release via pituitary stimulation, mimicking estrogenic activity at receptor sites [113]. In clinical settings, supplementation with Shatavari has led to:
These effects are particularly valuable in regions with high prevalence of hypogalactia or in mothers recovering from caesarean delivery. Additionally, Shatavari may exert a calming effect on the hypothalamic–pituitary axis, which indirectly promotes lactogenesis by reducing stress-induced prolactin suppression.
2. Gastrointestinal and Anti-ulcer Effects
Preclinical studies highlight Shatavari's potent gastroprotective effects. The root extract has shown efficacy in various ulcer models including:
Mechanistically, it reduces gastric acid output, enhances gastric mucin secretion, and preserves gastric prostaglandin E2 levels [115]. Histological analyses show improved epithelial integrity, reduced leukocyte infiltration, and preservation of goblet cells. Its mucilage content may serve as a demulcent, forming a protective layer on the gastric lining, which explains its use in Ayurvedic formulations like Shatavaryadi Churna for treating hyperacidity, reflux, and peptic ulcers.
3. Immunomodulatory and Anti-inflammatory Properties
Immunopharmacological studies have shown that Shatavari upregulates both innate and adaptive immune responses. It increases:
These immune-enhancing effects are mediated by the regulation of Th1/Th2 cytokine balance and inhibition of NF-κB signalling pathways, leading to decreased expression of IL-1β, TNF-α, and COX-2 [117]. In models of immunosuppression (e.g., cyclophosphamide-induced), Shatavari restores white blood cell counts and improves spleen and thymus weights. Such effects make it a potential candidate in adjuvant therapy for chronic infections, autoimmunity, and as a supportive agent in chemotherapy-induced immunosuppression.
4. Neuropharmacological and Cognitive Enhancing Effects
Shatavari exhibits promising neuroprotective properties, especially against oxidative damage and cholinergic dysfunction two hallmarks of neurodegenerative diseases like Alzheimer’s. Animal studies reveal that it:
Additionally, it demonstrates anxiolytic and antidepressant effects in behavioural models such as the elevated plus maze and forced swim test. These findings suggest Shatavari could be integrated into natural nootropic formulations, particularly for perimenopausal women experiencing cognitive decline due to hormonal changes.
5. Antidiabetic and Metabolic Effects
In diabetic rodent models, Shatavari significantly reduces fasting glucose levels, improves insulin sensitivity, and modulates lipid profiles. The antidiabetic mechanisms include:
Moreover, flavonoids in Shatavari inhibit α-glucosidase and α-amylase enzymes, delaying carbohydrate absorption and postprandial hyperglycaemia. These properties make it a promising adjunctive agent in type 2 diabetes and metabolic syndrome management.
6. Reproductive Health and Fertility Enhancement
Shatavari has long been regarded as a rasayana (rejuvenator) for the reproductive system. In males, it has shown:
In females, it promotes ovarian folliculogenesis, supports luteal function, and may improve endometrial receptivity. This makes it suitable for use in unexplained infertility, PCOS-related subfertility, and post-infertility treatment recovery.
7. Anti-aging and Antioxidant Actions
Shatavari is rich in polyphenolic antioxidants such as quercetin, rutin, and kaempferol. These compounds exert:
In preclinical models, Shatavari delays aging markers like telomere shortening and neurodegeneration. Topical formulations containing Shatavari are also gaining attention in cosmeceuticals for their anti-wrinkle, anti-inflammatory, and hydration-enhancing properties.
Adverse Reactions and Safety Considerations of Shatavari (Asparagus racemosus)
While Asparagus racemosus (Shatavari) is generally regarded as a safe and well-tolerated medicinal plant with centuries of traditional use, it is essential to evaluate its safety profile critically in the context of modern pharmacovigilance. As with any phytotherapeutic agent, adverse reactions may occur, especially in sensitive individuals or when used inappropriately. This section outlines the known and potential adverse effects, contraindications, and safety concerns related to Shatavari.
1. Gastrointestinal Disturbances
Mild gastrointestinal complaints are among the most reported adverse effects associated with Shatavari usage, particularly at higher doses or in individuals with sensitive digestive systems. These include:
These symptoms are usually transient and dose-dependent, often resolving upon dose reduction or discontinuation [122].
2. Allergic Reactions and Hypersensitivity
Although rare, hypersensitivity reactions to Shatavari have been documented. Being a member of the Liliaceae family, Shatavari may elicit cross-reactivity in individuals allergic to other species in this family, such as:
Reported allergic responses include:
Patients with a known history of plant-based allergies should exercise caution.
3. Endocrine and Hormonal Effects
Shatavari’s phytoestrogenic activity while beneficial in oestrogen-deficient states can be problematic in certain hormone-sensitive conditions. Caution is advised in:
In these cases, the oestrogen-like action of Shatavari could theoretically exacerbate the condition by stimulating oestrogen-responsive tissues [124]. Hence, the use of Shatavari in individuals with a history of oestrogen-dependent malignancies should only be under clinical supervision.
4. Interactions with Conventional Medications
Shatavari may interact with certain classes of drugs, especially those with overlapping pharmacodynamics. Potential interactions include:
Healthcare professionals should be informed of any concurrent herbal and allopathic drug use to avoid adverse herb-drug interactions.
5. Reproductive and Pregnancy-Related Concerns
Although traditionally used during pregnancy and lactation to improve maternal health and lactogenesis, robust clinical safety data are limited in:
Animal reproductive toxicity studies have not shown teratogenic effects at therapeutic doses, but rigorous human clinical trials are still lacking [126]. Hence, caution is warranted, especially in the early stages of pregnancy.
Methods of Shatavari (Asparagus racemosus) Preparation and Formulation
The therapeutic efficacy and clinical applicability of Asparagus racemosus (Shatavari) are closely tied to its method of preparation. Different preparation methods yield varying concentrations of active constituents such as steroidal saponins (e.g., Shatavarin IV), flavonoids, alkaloids, and polysaccharides. These preparations range from traditional Ayurvedic formulations to modern pharmaceutical extracts. Understanding these methods is essential for standardizing therapeutic dosing, ensuring quality, and optimizing bioavailability.
1. Traditional Ayurvedic Preparations
In classical Ayurvedic texts, Shatavari is prepared using time-tested procedures. Some of the common traditional forms include:
a. Churna (Powder)
Prepared by shade-drying the roots and grinding them into a fine powder, Churna is one of the simplest and most widely used forms [127]. It is usually administered with milk or ghee to enhance absorption.
b. Kwatha (Decoction)
This involves boiling the coarse powder of roots in water until the volume is reduced to one-fourth. Kwatha extracts primarily water-soluble components such as glycosides and polysaccharides [128].
c. Ghrita (Medicated Ghee)
Here, Shatavari root paste or decoction is processed with clarified butter (ghee). It is especially recommended for reproductive and rejuvenation therapies due to its lipophilic delivery matrix [129].
d. Avaleha (Herbal Jam)
Formulated with jaggery, ghee, and decoction, this form is known for its palatability and tonic properties, particularly in postpartum care (e.g., Shatavari Kalpa) [131].
2. Modern Extraction and Standardization Techniques
Scientific extraction techniques aim to isolate and preserve bioactive constituents while ensuring batch-to-batch consistency.
a. Hydroalcoholic Extraction
Utilizes ethanol and water as solvents to yield extracts rich in both polar and non-polar phytochemicals. This method is widely used in industrial production for capsules and syrups [132].
b. Supercritical Fluid Extraction (SFE)
Using CO? as a solvent under high pressure and temperature, SFE offers a solvent-free and thermally stable extraction option for obtaining high-purity saponins like Shatavarin IV [133].
c. Microwave-Assisted Extraction (MAE)
This eco-friendly technique accelerates the extraction of phenolics and saponins using microwave energy, reducing extraction time and solvent use [134].
3. Formulation Types in Modern Use
Modern pharmaceutical formulations have adapted Shatavari into various dosage forms:
|
Formulation Type |
Use and Description |
|
Capsules/Tablets |
Standardized to 20–40% saponins; used for hormonal, adaptogenic, and fertility support. |
|
Syrups/Suspensions |
Combined with other herbs for gynaecologic and paediatric use. |
|
Granules |
Used in regulating menstruation and improving lactation (e.g., Shatavari Kalpa). |
|
Nano formulations |
Under development for enhanced absorption and targeted delivery. |
|
Topical Creams |
Applied in cosmeceuticals for moisturizing and anti-aging effects. |
4. Stability and Storage Considerations
Standardized extracts, particularly in capsule or tablet form, show longer shelf lives when stored under controlled conditions (cool, dry environment), unlike decoctions and aqueous suspensions, which are more prone to microbial spoilage [139].
Toxicological Evaluation of Shatavari (Asparagus racemosus): Preclinical and Safety Assessment Profile
A thorough understanding of the toxicological profile of Asparagus racemosus (Shatavari) is essential to ensure its safe therapeutic application, especially as interest grows in its integration into evidence-based medicine. Although Shatavari has a long-standing reputation for safety in traditional medicine, scientific validation through standardized toxicology studies is critical for global acceptance. This section highlights findings from acute, sub-chronic, and chronic toxicity studies, along with reproductive and genotoxicity assessments.
1. Acute Toxicity Studies
Several animal models have demonstrated that Shatavari is well tolerated even at high doses:
These results support the classical Ayurvedic perspective of Shatavari as a rasayana (rejuvenator) with minimal acute toxicity.
2. Sub-chronic and Chronic Toxicity
Long-term exposure studies provide further insight into the safety margin of Shatavari:
These findings suggest that Shatavari is non-toxic at therapeutic and moderately elevated doses, supporting its long-term use in clinical practice.
3. Reproductive and Developmental Toxicity
Given its traditional use in pregnancy and postpartum care, reproductive safety is of particular concern:
Nonetheless, high-dose exposure studies suggest that extremely elevated doses (≥3,000 mg/kg) may lead to delayed foetal development, indicating the need for careful dose control during pregnancy [143].
4. Genotoxicity and Mutagenicity Studies
Preliminary Ames tests and chromosomal aberration assays have found no evidence of mutagenic or genotoxic effects associated with Shatavari extract:
These results confirm that Shatavari lacks significant DNA-damaging potential under tested conditions.
5. Histopathological Findings
Detailed microscopic evaluations of major organs (liver, kidney, reproductive tissues, brain, spleen) have consistently shown:
Such evidence aligns with the herb’s rejuvenative and adaptogenic properties.
6. Limitations and Research Gaps
Despite promising toxicological safety data, some important research gaps remain:
These limitations warrant further preclinical and clinical trials under Good Laboratory Practices (GLP) and OECD guidelines to establish definitive safety thresholds for various demographic groups.
CONCLUSION
Asparagus racemosus (Shatavari) has long been revered in Ayurvedic medicine as a cornerstone herb for female reproductive health. This review consolidates emerging in vitro, preclinical, and limited clinical evidence supporting its role in managing menorrhagia a condition with complex hormonal, inflammatory, and hematologic underpinnings. Shatavari exhibits a multifaceted pharmacological profile that includes phytoestrogenic, anti-inflammatory, antioxidant, hematopoietic, and endometrial-stabilizing actions, making it a promising natural intervention for menstrual bleeding disorders. Its broad spectrum of action is mediated through modulation of oestrogen receptors, inflammatory cytokines, oxidative stress markers, and uterine contractility pathways. Modern investigations into its safety profile suggest a high therapeutic index, minimal toxicity, and tolerability across a range of formulations. However, the translation of Shatavari into evidence-based clinical practice is hampered by gaps in standardization, large-scale randomized controlled trials, regulatory recognition, and mechanistic clarity. Future advancements in standardized extraction, nano formulation technologies, systems biology approaches, and clinical trial design are essential for optimizing its therapeutic utility. With growing global interest in plant-based medicine, Shatavari holds the potential to emerge as a valuable adjunct or alternative to conventional therapies in the management of menorrhagia and broader gynecological disorders provided that scientific rigor continues to guide its exploration and integration.
REFERENCES


Bandi Aasritha*, Mandali Abhinav Sai, Dr. Adusumalli Surendra, Pharmacological Perspectives on Shatavari (Asparagus Racemosus): Therapeutic Potential in Menorrhagia and Beyond, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 893-921 https://doi.org/10.5281/zenodo.17076149
 10.5281/zenodo.17076149
10.5281/zenodo.17076149
