P.R. Pote Patil College of Pharmacy, Amravati Maharashtra 444604.
Alzheimer's disease (AD), recognized more than a century ago, is a progressive neurological condition and the primary cause of dementia, representing 60–80% of cognitive impairments in older adults. It typically starts with mild memory lapses, especially in recalling recent events, and gradually worsens over time. As the disease advances, individuals may experience difficulties with language, disorientation, mood shifts, neglect of personal care, and behavioral changes, ultimately leading to social withdrawal, loss of bodily functions, and death. While the onset of symptoms usually occurs after the age of 65, brain alterations linked to AD can begin many years or even decades before symptoms manifest. Although Alzheimer’s is not a normal aspect of aging, there is no cure available as of now. Medications approved by the FDA, such as donepezil, rivastigmine, galantamine, and memantine, offer temporary relief by improving memory, cognition, and daily functioning but do not halt or reverse the disease. Research is focused on understanding the role of beta-amyloid plaques and tau protein tangles in the brain, which are defining characteristics of AD pathology. Scientists aim to explore how these abnormalities harm neurons in hopes of discovering more effective treatments. Lifestyle choices, including mental and physical exercises, may help delay the onset of the disease. The National Institute of Neurological Disorders and Stroke (NINDS) funds research efforts to deepen our understanding of Alzheimer's disease and develop interventions to slow its progression, providing hope for future therapeutic breakthroughs.
The diagnosis of Alzheimer's disease (AD) was made over a century ago. It is a brain degenerative illness that causes 60% to 80% of late-life cognitive dysfunction and is the most frequent cause of dementia in older adults. Alzheimer's disease (AD), a neurological condition that often begins slowly and gets worse over time, is the cause of 60–70% of dementia cases [2]. The most typical Having trouble recalling recent events is an early indication. Language difficulties, mood swings, disorientation (including getting lost easily), lack of motivation, self-neglect, and behavioral problems are some of the symptoms that may appear as the condition progresses [1]. A person's withdrawal from family and society is common as their health worsens. Body functions gradually deteriorate, eventually resulting in death. Clinical signs of Alzheimer's disease often appear after the age of 65, although Alzheimer's-related brain alterations that may not cause symptoms can start years or even decades earlier. AD is not a typical aspect of aging, even though its symptoms start in older adults. Although there is currently no cure for Alzheimer's, some people may find that certain therapies can lessen the severity of their symptoms. Additionally, there are medications that slow down the disease to prevent brain damage from occurring too quickly. Additionally, people can develop personal practices that could assist postpone the onset of the disease [18]. The majority of researchers studying Alzheimer's disease focus on the amyloid plaques and fibrillary tangles that are common in the brain tissues of patients who have the condition. There are currently no medications that can halt AD's progression. Nonetheless, the symptoms of AD are treated using four FDA-approved drugs. By preserving thinking, memory, or speaking abilities, these medications assist people in performing daily tasks. Additionally, they can assist with some of the psychological and behavioral changes linked to AD. They seem to benefit people for a few months to a few years, but they cannot reverse or stop AD. Galantamine, donepezil, and rivastigmine are recommended to treat mild to moderate symptoms of AD. Recently, donepezil was authorized to treat severe AD as well. Memantine, the newest drug, is given to treat moderate to severe symptoms of AD [2]. Through grants to significant medical institutions nationwide, the National Institute of Neurological Disorders and Stroke (NINDS) funds basic and translational research on AD. Current research is looking into how tau protein abnormalities produce the distinctive neurofibrillary tangles of AD and how beta amyloid plaque growth damages neurons [3].
The Origins and Development of Alzheimer's Disease
Dr. Alois Alzheimer (1864-1915), a German physician and neuropathologist, made the initial discovery and description of Alzheimer's disease, the most prevalent cause of dementia, in 1906. He was employed in a mental health facility in Frankfurt in 1901 when Auguste Deter, then 51, was brought in for treatment. She was experiencing dementia, delusions, hallucinations, melancholy, and paranoia. Over the next few years, the patient would become his preoccupation. She passed away in April 1906 at the age of 55. She displayed symptoms and indicators of a disease process that was unfamiliar to him and had not yet been documented in the literature, as Dr. Alzheimer acknowledged. In order to work at Emil Kraepelin's lab in Munich, Dr. Alzheimer had the patient's brain transported there. He would utilize the new staining methods to look at her brain tissue under a microscope and find neurofibrillary tangles and amyloid plaque. At the Southwest German Psychiatrists' meeting in Tubingen on November 3, 1906, Dr. Alzheimer gave a brief talk titled "On the Peculiar Disease Process of the Cerebral Cortex," outlining the symptoms and pathology of presenile dementia. The name would become well-known due to Dr. Kraepelin's inclusion of Alzheimer's disease in a textbook. By 1911, European doctors were using Alzheimer's description of this specific form of dementia to diagnose patients in the United States. The fact that Dr. Alzheimer was acquainted with and collaborated with Dr. Frederick Lewy, the man who gave Lewy Body Dementia its name, is historically significant. Additionally, he was acquainted with Dr. Arnold Pick, who was the first to characterize the behavioral form of frontotemporal dementia (formerly known as Pick's disease) in 1892 [4] [5]. It's important to highlight that Mrs. Deter had dementia before the age of 65, which is now categorized as early-onset or younger-onset Alzheimer's dementia. Ninety-five percent of Alzheimer's dementia cases happen to people over 65. Alzheimer's disease was comparatively uncommon in 1900, when the average life expectancy from birth was 47.3 years. The majority of people did not live long enough for Alzheimer's dementia to manifest and develop in those who were predestined to get it. On his rail journey to the University of Breslau, where he had been appointed professor of psychiatry in 1912, Dr. Alzheimer fell unwell in December of 1915. He is thought to have had a streptococcal infection, which led to rheumatic fever and renal failure. At the age of 51, he passed away in Breslau from heart failure [19].
Organ Anatomy and Physiology Before and After of Alzheimer’s Disease:
Table No. 1 Organ Anatomy and Physiology Before and After of Alzheimer’s Disease
|
Sr. No. |
Organs (Parts) |
Before of AD |
After of AD |
|
1. |
Cerebral Cortex |
Responsible for higher level brain functioning |
Several shrinkages, impact memory, judgment, and thinking. |
|
2. |
Hippocampus |
Essential for creating fresh memories. |
Early and multiple damage: Impact the development of new memories |
|
3. |
Ventricles |
Normal protection of tissues |
Ventricles enlargement |
|
4. |
Amygdala |
Contributes to memory and emotion |
Deterioration of emotions |
|
5. |
Parietal Lobe |
Sensory Information (Touch, Pain & Temperature) |
Affect the sensory information |
|
6. |
Temporal Lobe |
Processes language, emotion, and memory |
Make it possible to feel and remember |
|
7. |
Occipital Lobe |
Primarily responsible for vision |
Effect on eye or vision |
|
8. |
Frontal Lobe |
Regulates motor function, problem-solving, and decision-making |
Problem in decision making |
Brain Anatomy
The human brain is made up of several key regions that play vital roles in various cognitive and bodily functions:
Cerebral Cortex: Higher order brain processes including thinking, memory, language, and voluntary movement are controlled by the cerebral cortex, an outer layer of the brain.
Frontal lobe : The frontal lobe regulates motor function, decision-making, and problem-solving.
Parietal lobe: The parietal lobe is responsible for controlling touch, pain, and temperature.
Memory, language processing, and emotion are all influenced by the temporal lobe.
Occipital lobe: The occipital lobe is mostly in charge of vision.
Hippocampus: The formation of memories and spatial navigation depend on the hippocampal region. It is one of the first areas impacted by Alzheimer's disease.
Amygdala: Involved in memory and emotions, especially emotional memories.
Hypothalamus and thalamus: The hypothalamus controls body processes including appetite, sleep, and body temperature, whereas the thalamus transmits motor and sensory information.
Basal ganglia: The basal ganglia are involved in several forms of learning and movement regulation.
Cerebellum: Balance, coordination, and precise motions are all regulated by the cerebellum.
Brainstem: Regulates essential functions like breathing, heart rate, and blood pressure.
Physiology of a Healthy Brain
Neurons: The brain is made up of billions of nerve cells called neurons, which exchange chemical and electrical impulses with one another. Complex networks of neurons facilitate learning, memory, cognition, and body coordination.
Neurotransmitters: To send messages across synapses (junctions between neurons), neurons release chemical messengers such acetylcholine, dopamine, and serotonin.
Synaptic Plasticity: A crucial mechanism in memory and learning, synaptic plasticity allows neurons to create new connections or fortify preexisting ones.
Brain Blood Flow: Oxygen and nutrients must be continuously supplied to the brain through blood flow. The delivery of oxygen and glucose, which are essential for brain activity, is ensured by healthy blood vessels.
Anatomy and Physiology of Organs Following Alzheimer's disease
A. Anatomy of the Brain Following Alzheimer's
Significant structural damage is caused to several parts of the brain by Alzheimer's disease, which results in atrophy, or a noticeable decrease in brain volume. The key changes in brain anatomy include:
Cerebral Cortex
Amygdala
The ventricles
Cerebellum and Brainstem
Areas like the brainstem and cerebellum, which regulate fundamental body processes like breathing, movement, balance, and heart rate, may be impacted in the final stages of Alzheimer's. This makes it harder to move, swallow, and maintain basic autonomic processes.
B. Physiological Alterations Following Alzheimer's
Alzheimer's causes significant changes in the physiological components of brain function. These alterations affect brain metabolism, synaptic plasticity, and neuronal communication.
Neuronal Death (Neuron Loss)
Neuron Degeneration: Alzheimer's causes the brain to lose a significant number of neurons. The buildup of harmful proteins (amyloid plaques and neurofibrillary tangles) limits the function of the neurons that survive.
Synapse Loss: When synapses, or connections between neurons, are broken, there is less communication between them. This contributes to cognitive decline by impairing the brain's ability to process and transfer information.
Tangles and Plaques Amyloid Plaques: Beta-amyloid protein clusters build up in between neurons, obstructing communication between cells. These poisonous plaques lead to the degeneration of neuronal function.
Neurofibrillary Tangles: Tau proteins inside neurons twist abnormally into tangles that impair the movement of nutrients and other necessary components within the cells, ultimately resulting in neuronal death.
Heart and Vascular System: Elevated Risk of Cardiovascular Disease: Due in part to common risk factors including inflammation, high cholesterol, and diabetes, Alzheimer's has been linked to an increased risk of cardiovascular disorders like hypertension and heart disease. Alzheimer's disease may increase the risk of stroke or heart attack by causing atherosclerosis, which is the buildup of plaque in arteries [37].
Lungs: Decreased Respiratory Function: In the later stages of Alzheimer’s, people can have difficulty coordinating breathing and swallowing, leading to aspiration pneumonia (when food or liquids enter the lungs).
Digestive System: Aspiration hazards, poor nutrition, and weight loss are all consequences of dysphagia, or trouble swallowing, which is prevalent in the latter stages of Alzheimer's disease. Constipation and Digestive Issues: Reduced mobility and dietary changes in Alzheimer’s patients can lead to constipation and other gastrointestinal issues.
Musculoskeletal System: Muscle Weakness and Reduced Mobility: People with Alzheimer's disease frequently lose their ability to walk, balance, and coordinate as their brain function deteriorates. This results in muscle atrophy, frailty, and a higher risk of falls.
Kidneys and Bladder: Incontinence: As Alzheimer's progresses, many people have a loss of control over their bladder and bowel movements because the brain is unable to regulate these organs.
Immune System: Weakened Immunity: Patients with Alzheimer's disease, especially those in the latter stages, frequently have compromised immune systems, which leaves them more vulnerable to diseases including urinary tract infections and pneumonia.
Endocrine System: Impaired hormone Regulation: Sleep may be impacted by changes in the hypothalamus and other brain regions that control hormone regulation, rhythms, body temperature, and metabolism. In conclusion, Alzheimer's disease can indirectly impact different organs and systems in the body, particularly as it advances to more severe stages, even though it is predominantly a neurodegenerative condition.
Signs and Symptoms
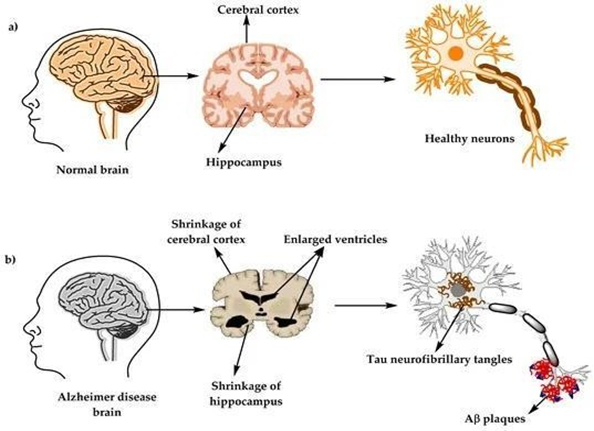
Figure No. 1 Brain structure a) healthy brain and b) Alzheimer’s Disease
Alzheimer's disease typically progresses in three phases, characterized by a gradual pattern of cognitive and functional decline. Early or mild, middle or moderate, and late or severe are the terms used to characterize the three stages [7]. The earliest signs of memory impairment are thought to be caused by the disease's targeting of the hippocampus, which is linked to memory. The degree of memory impairment increases with the progression of the disease [6].
Initial Signs
Many times, the initial symptoms are misdiagnosed as stress or age. Up to eight years before a person meets the clinical criteria for an Alzheimer's disease diagnosis, thorough neuropsychological testing can identify modest cognitive impairments. The most difficult daily tasks may be impacted by these early signs. The most obvious impairment is short-term memory loss, which manifests as an inability to retain new knowledge and trouble recalling recently learned data. Early-stage Alzheimer's disease symptoms can also include subtle issues with executive skills including planning, flexibility, abstract thought, and concentration, as well as deficits in semantic memory (the recall of meanings and idea links). [9] At this point, despair and apathy are both evident, with apathy continuing to be the most enduring symptom during the length of the illness. [11] Moderate cognitive impairment (MCI) is frequently identified as a stage that lies between dementia and normal aging. A number of symptoms can accompany MCI, but when memory loss is the main one, it's known as amnestic MCI and is often considered a prodromal stage.
Figure No. 02 Stages of Atrophy in Alzheimer’s
Early stage:
A final diagnosis of Alzheimer's disease is made when a person's memory and learning become increasingly impaired. Memory issues are less common in a tiny number of people than issues with language, executive processes, perception (agnosia), or movement execution (apraxia). [13] Not every memory function is equally impacted by Alzheimer's disease. In contrast to fresh facts or memories, older memories of the person's life (episodic memory), facts learnt (semantic memory), and implicit memory (the body's knowledge of how to perform tasks, such eating with a fork or drinking from a glass) are less influenced. [14] A general decline in spoken and written language is the result of language issues, which are primarily characterized by a declining vocabulary and a drop in word fluency. [13] [15] At this point, the Alzheimer's patient can typically express simple concepts clearly. [13] [15] Some movement coordination and planning issues (apraxia) may be evident when executing fine motor tasks like writing, sketching, or dressing, but these are frequently overlooked.[13]As the illness worsens, Alzheimer's patients illness may frequently still carry out a lot of chores on their own, but the most cognitively taxing jobs may require help or supervision. [13]
Middle stage:
As independence is gradually impeded by progressive degradation, subjects are unable to carry out the majority of everyday tasks. An failure to recall vocabulary causes frequent inaccurate word replacements, or paraphasia’s, which are a sign of speech difficulties. Additionally, writing and reading abilities are gradually declining. [13] As Alzheimer's disease worsens as time goes on, complex motor sequences become less coordinated, increasing the risk of falling. Memory issues get worse during this stage, and the person could not recognize close family members. Previously unaffected long-term memory is compromised. [13] Changes in behavior and neuropsychiatry become more common. Wandering, irritation, and emotional vulnerability that results in sobbing, unplanned violent outbursts, or refusal to provide care are common symptoms. Sundowning is another possibility. About 30% of Alzheimer's patients experience delusional symptoms, including illusionary misidentifications. Urinary incontinence may develop, and subjects lose awareness of their disease process and restrictions (anosognosia). Transferring the individual from home care to another long-term care facility might alleviate the stress these symptoms cause for family members and caregivers. [13]
Later stage :
The latter stage, referred to as the severe or late-stage stage, is characterized by total reliance on caregivers. [7] [13] Eventually, communication is lost entirely as language is reduced to basic sentences or even single words. Even when verbal language skills are lost, people can still comprehend and react to emotional cues. Extreme apathy and fatigue are far more prevalent symptoms, however aggression might still be present. As their muscle strength and movement decrease to the point where they are bedridden and unable to feed themselves, people with Alzheimer's disease will eventually be unable to carry out even the most basic duties on their own. Usually, an external factor—like pneumonia or pressure ulcer infection—rather than the illness itself is the cause of death. [13] Sometimes, just before passing away, there is a paradoxical lucidity in which mental clarity unexpectedly returns.
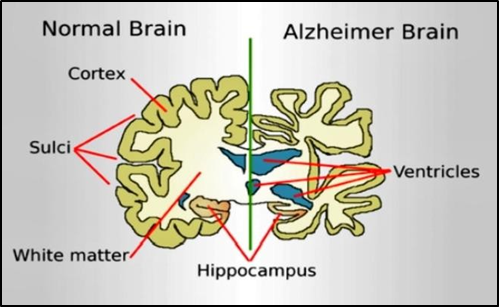
Figure No. 03 Normal brain and Alzheimer’s brain
Causes
It is thought that Alzheimer's disease develops when the brain accumulates abnormal amounts of amyloid beta (AB), which can build up intracellularly as neurofibrillary tangles or extracellularly as tau proteins and amyloid plaques. This impairs neuronal connectivity and function, leading to a progressive loss of brain function. [16] Age-related, brain cholesterol-regulated, and linked to other neurodegenerative disorders, this reduced protein clearance ability [17]
Pathophysiology of Alzheimer's disease
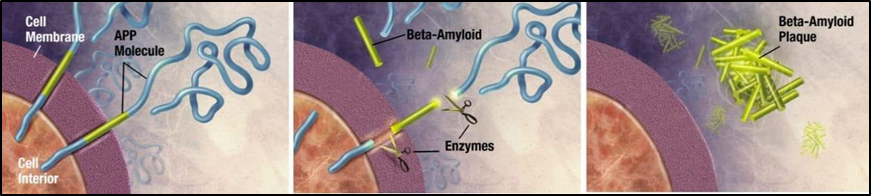
Figure No. 04 Amyloid-beta (Aβ) Plaque Formation
Enzymes act on the amyloid-beta precursor protein and cut it into fragments. The beta-amyloid fragments are crucial in the formation of amyloid plaques in Alzheimer's disease. Amyloid precursor protein (APP), a transmembrane protein, is processed abnormally by the enzymes β-secretase and γ-secretase in AD. Amyloid-beta (Aβ) peptides, especially Aβ42, which is extremely prone to aggregation, are produced as a result of this cleavage. [18]
Plaque deposition: Amyloid plaques form in the brain as a result of the extracellular accumulation of these Aβ peptides in the form of oligomers and insoluble fibrils. These plaques interfere with cell-to-cell communication, set off inflammatory reactions, and cause damage to neurons.
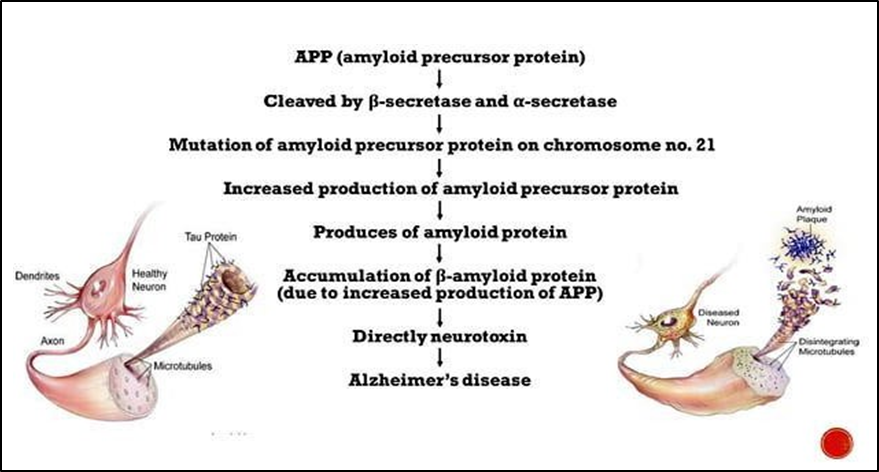
Figure No. 05 Mechanism of Amyloid-beta (Aβ) Plaque Formation
Neurofibrillary Tangles (NFTs)
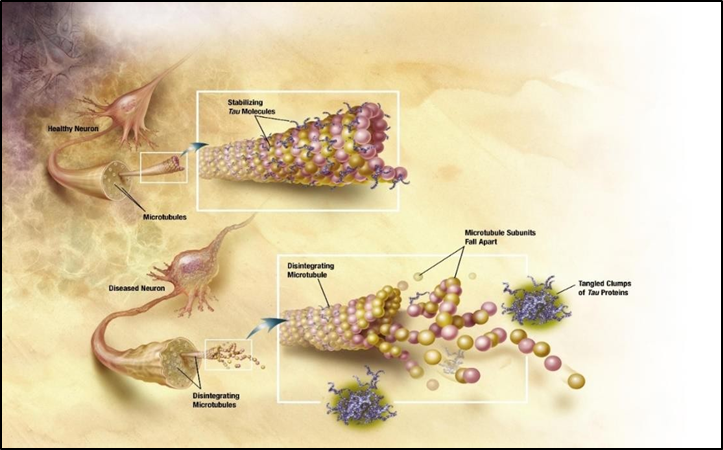
Figure No. 06 Changes in Tau Protein
Destabilization of microtubules: When tau function is compromised, the cytoskeleton of the neuron becomes unstable, axonal transport is compromised, and eventually the cell dies.
3. Dysfunction of Synapses
It is believed that Aβ oligomers are especially harmful to synapses, which are where neurons communicate with one another. One of the first things that happens in AD is synaptic disruption, which impairs neuronal connection and contributes to cognitive loss.
4. Inflammation of the neurons
Activation of microglia: The buildup of amyloid plaques triggers the activation of microglia, the immune cells in the brain. Although initially beneficial, long-term microglial activation can exacerbate neuronal injury by releasing pro-inflammatory cytokines and neurotoxic substances.
Participation of astrocytes: Another glial cell type that becomes reactive in AD is the astrocyte, which increases oxidative stress and the inflammatory response.
5. The Cholinergic Theory
Acetylcholine, a neurotransmitter essential for memory and learning, is decreased in AD due to a substantial loss of cholinergic neurons in the basal forebrain. This serves as the foundation for the therapeutic approach of using cholinesterase inhibitors to improve cholinergic function.
6. Contributions from Vascular
By aggravating Aβ deposition, encouraging tau pathology, and impairing the brain's capacity to eliminate harmful proteins, cerebrovascular dysfunction—which includes compromised blood-brain barrier integrity and decreased cerebral blood flow—may be a contributing factor to the pathophysiology of AD.
7. Mitotic dysfunction and oxidative stress
In AD, oxidative damage to proteins, lipids, and DNA results from increased formation of reactive oxygen species (ROS) and mitochondrial dysfunction, which exacerbates neuronal degeneration.
Classification of drugs for Alzheimer’s disease
Ex. Rivastigmine, Donepezil, Galantamine.
Ex. Memantine.
Ex. Haloperidol
Ex. Paroxetine, Venlafaxine
Ex. Ibuprofen, Indomethacin
Ex. Pravastatin, Lovastatin
Table No.02 Possible Medication Brand Name, Business, And Indication
|
Sr. no. |
API |
Brand Name |
Company |
Indicated for |
|
1. |
Donezepine |
T. Donep T. Donecept T. Aricept |
Alkem laboratories Ltd Cipla Ltd Eisai pharmaceutical India Pvt Ltd |
Mild cognitive impairment or Mild dementia caused by Alzheimer’s Disease |
|
2. |
Rivastigmine |
C. Exelon T. Rivamer
T. Zeemine |
Novartis India Ltd Sun pharmaceuticals industries Ltd Psyco Remedies |
Mild to moderate dementia due to Alzheimer’s or Parkinson’s |
|
3. |
Memantine |
T. Mentadem
T. Axura |
Torrents Pharmaceuticals Ltd. Win Medicare Pvt Ltd. |
Moderate to severe dementia. Due to Alzheimer’s |
|
4. |
Galantamine |
T. Razadyne |
Janssen Pharmaceuticals, Belgium |
Mild to moderate dementia due to Alzheimer's |
|
5. |
Donanemab |
Inj. Kisunla |
Illy Lilly corporate company |
Mild cognitive impairment or Mild dementia caused by Alzheimer’s Disease |
Potential side effects of drugs which are used to treat Alzheimer's Disease
Potential negative consequences of medications used to treat Alzheimer's are Sickness, diarrhea, and vomiting, decrease in appetite, pain in the head, bewilderment, vertigo, falls, sore muscles, sleep issues, fatigue, weight loss or itching.
Pharmacological Treatments:
1. Memantine: The UK's National Institute for Clinical Excellence has now issued a limited recommendation for memantine, which is approved for the treatment of moderate to severe AD in people who do not respond to other forms of treatment. For individuals with moderate AD who are intolerant of or contraindicated for AchE (acetyl cholinesterase inhibitors) with severe AD, memantine is suggested as a treatment option in the guidelines. Memantine has been linked to a moderate reduction in clinical detenoranon in AD. According to a systematic analysis of randomized consulted trials, memantine has an uncertain effect in mild to moderate AD but a slight favorable impact on mood, behavior, cognition, and the capacity to carry out daily tasks in moderate to severe AD [32].
2. Galantamine:
Galantamine is used to treat mild-to-moderate AD and a number of other memory problems, especially those that have a vascular cause. Galantamine is a reversible and competitive inhibitor of cholinesterase. It tends to enhance the concentration of acetylcholine in the brain by decreasing the function of AchE. This action is thought to alleviate some of the symptoms of Alzheimer's disease by binding to the nicotinic acetylcholine receptor as an allosteric ligand. AD is treated with galantamine. More precisely, it helps patients with mild to moderate AD with their memory, attention, reasoning, language, and capacity to carry out basic daily tasks. On occasion, the drug is also prescribed to treat other ailments. Galantamine is frequently used to treat cognitive disorders such as Durative Syndrome and ADHD.[33]
3. Rivastigmine:
It is a cholinergic or parasympathetic drug used to treat mild to severe Alzheimer's disease dementia as well as dementia brought on by parkinsonism. Either an oral or transdermal patch can be used to administer the medication; the latter lessens the likelihood of adverse effects, which usually include nausea and vomiting. Rivastigmine is a cholinesterase inhibitor that inhibits both butyryl cholinesterase and acetyl cholinesterase. It is thought that Rivastigmine works by inhibiting this cholinesterase enzyme which would otherwise break down the brain chemical acetyl choline. The US Food and Drug Administration has approved Rivastigmine capsule and Rivastigmine patch for the treatment of mild to moderate dementia of the Alzheimer type and for mild to moderate dementia related to parkinsonism disease. [34]
4. Tacrine:
It works through a variety of mechanisms. AD is thought to work as a noncompetitive, reversible inhibitor of acetylcholinesterase. Somewhat selective for action in the CNS. But the lesions of Alzheimer’s exceed the boundaries of the cholinergic systems to include nor-adrenaline neuro-transmitters decrease vascular perfusion. It may be fortunate that Tacrine has a wide variety of actions. Tacrine blocks Na-K channels. It has direct post synaptic muscarinic activity alters MAO uptake, increase release of 5 HT, NA and Dopamine, inhibit MOA A and B, stimulate cholinergic firing, interacts with N-methyl-D-aspartate phencyclidine receptors, 121.22) Tacrine significantly increases cerebral blood flow in patients who have Alzheimer’s disease. Much has been made of the role of amyloid deposition in the pathology of Alzheimer’s disease. Tacrine actually blocks secretion of ?-amyloid precursor protein. It appears that Tacrine is uniquely suited to treat AD[35].
5. NSAIDS:
Long-term NSAID use may protect against AD, according to several epidemiological studies, particularly for patients who had one or more epsilon 4 alleles of the Apo lipoprotein E. Uncertainty surrounds the biological protection, which might entail COX activity suppression. inhibition of beta secretase activity, activation of PPAR-Gamma, or stimulation of neutrophil synthesis in addition to inhibition of beta amyloid (1-42) (A beta 42) generation. Sadly, long-term placebo control studies using COX-2 selective and long selective NSAIDs in AD patients provide unfavorable outcomes. Both a main prevention research using Naproxen and Celecoxib in older adults with a family history of AD and a second prevention study using Rofecoxib in patients with mild cognitive impairment yielded negative results. It is thought that long-term NSAID use may only be advantageous in healthy brains because it prevents beta 42 from being produced. Because NSAIDs decrease activity on activated microglia of the AD brain, which mediate A beta clearance and trigger compensatory hippocampus neurogenesis, they lose their effectiveness and may even be harmful once the A beta deposition process has begun. 1271l is prescribed to treat mild to moderate AD symptoms. By raising the amount of accessible Ach, it inhibits acetyl cholinesterase in a specific and reversible manner. Donepezil might make up for the loss of cholinergic brain cells that are still functional. Lewy body dementia (s) and vascular dementia are among the other cognitive illnesses for which donepezil has been investigated. For these purposes, however, it is now approved. Bradycardia, nausea, diarrhea, anorexia, and abdominal pain are typical adverse effects. [36]
Recently Approved Drugs Used in Treatment of Alzheimer’s Disease
1. Donanemab (Kisunla™)
An anti-amyloid antibody intravenous (IV) infusion treatment called donanemab (Kisunla) is administered every four weeks. The FDA has given it traditional permission to treat early-stage Alzheimer's disease, including moderate cognitive impairment (MCI) and mild dementia caused by Alzheimer's disease in individuals with confirmed increased beta-amyloid in the brain. Data regarding the safety and efficacy of starting treatment earlier or later in the disease than was examined are lacking. The third treatment to show that eliminating beta-amyloid from the brain slows down cognitive and functional deterioration in individuals with early-stage Alzheimer's disease was donanemab.
2. Lecanemab (Leqembi®)
The anti-amyloid antibody intravenous (IV) infusion treatment lecanemab (Legembi) is administered every two weeks. The FDA has given it traditional permission to treat early-stage Alzheimer's disease, including moderate cognitive impairment (MCI) and mild dementia caused by Alzheimer's disease in individuals with confirmed increased beta-amyloid in the brain. Data regarding the safety and efficacy of starting treatment earlier or later in the disease than was examined are lacking. The second treatment to show that eliminating beta-amyloid from the brain slows cognitive and functional deterioration in individuals with early-stage Alzheimer's disease was lecanemab [21] [22].
3. Donanemab (Kisunla™)
The monoclonal antibody donanemab, marketed under the Kisunla trademark, is used to treat Alzheimer's disease. Eli Lilly and Company created donanemab. [22] Headache and anomalies in imaging caused by amyloid are the most frequent adverse effects. The Food and Drug Administration authorized the use of donanemab for medicinal purposes in the United States in July 2024. The target population for the treatment was the same group that the clinical trials examined: patients with mild cognitive impairment or mild dementia.
Medical uses
Donanemab is indicated for the treatment of Alzheimer’s disease for people with mild cognitive impairment or mild dementia stage of disease. [2]
Clinical Trials
Clinical trials occurred in 3 phases
1. Phase- I
First study
Eli Lilly conducted the phase I trial in the US and Japan between May 2013 and August 2016. [23] Individuals with moderate Alzheimer's disease, as shown by a positive amyloid PET scan, were the subjects of the study. Donanemab was administered intravenously to 100 subjects up to four times each month. One control group was employed in all trials throughout Phase I of a multi-armed investigation. The positive finding showed that the individuals' brains had an excess of amyloid protein, which is a precursor to Alzheimer's disease. At an average age of 74, males and non-fertile females received monthly injections of 0.1 mg/kg to 10 mg/kg. [24] Lilly disclosed that 12 volunteers who received a placebo and 37 patients who received the medication experienced negative side effects. The effect of the plaque burden in the brain was lessened by the maximum dose of donanemab. 110 Overall, it was discovered that the increased dosage resulted in a 40% decrease in brain protein plaques.
Side effects
Until side effects forced Lilly to change the experiment, upping the number of injections to eight monthly and raising the patient dosage from 0.1 mg/kg to 0.3 mg/kg, up to four injections were given each month. The reduction in participants from 37 recorded volunteers to 9 individuals with publicly available findings coincided with the dosage changes. When they received a single dose, no negative symptoms appeared. It was discovered that donanemab is very immunogenic, eliciting an immunological response that boosts the effectiveness of the initial antibody infusion. Six patients experienced an infusion reaction, which included chills, flushing, disorientation, rash, and fever, during the subsequent phase of the experiment, in which patients got repeated doses. There were instances of ARIA-H causing minor brain hemorrhages, but no individuals had ARIA-E. There were no symptoms in either of the two ARIA-H patients. With a short half-life of ten days, the majority of persons acquired anti-drug antibodies, which reduced the drug's potency.
Second study
In December 2015, the second phase I study was carried out in Japan and the United States. [23] With 150 participants in this study, the sample size increased by 50. Compared to the initial study, the methodology was changed. Three distinct dosing schedules were used in this trial: 10, 20, or 40 mg/kg as a single dosage, 10 mg/kg every other week for 24 weeks, and 10 or 20 mg/kg monthly for 16 months. In a 3:1 ratio, the individuals were chosen at random to be in the true experiment or the placebo group. Similar to the first experiment, the primary goal of this one was to see how well it reduced amyloid brain plaques. [23]
Side effects
The proportion of participants who experienced symptomatic ARIA-E increased to 1 in 4 as a result of the dosage increase. Additionally, auto-antibodies were starting to cause issues for donanemab, identifying the medication as a non-self cell and causing the body to fight against it. Almost all of the patients developed anti-drug antibodies, which are classified as auto-antibodies. Although the amyloid PET scan turned negative for participants receiving monthly dosages for 16 months, this experiment ended in August 2019. [22]
2. Phase-II: -Trailblazer -Alz
The length of the phase II experiment, the dosage of donanemab, and the patient count were all systematically changed from the phase I trial. Over the course of 72 weeks, the amount of donanemab administered into the blood increased monthly. With a total of 257 patients, the patients who received donanemab and the placebo were infused equally, forming a nearly 1:1 ratio. 700 mg of donanemab was administered for the first three doses, and 1400 mg for each additional dose. The quantity of plaque in the brain was also measured using a PET scan. TRAILBLAZER-ALZ was the randomised technique utilized to enhance the placebo-controlled group. It evaluated donanemab's effectiveness and safety. Two investigational medications under Lilly that target different aspects of the amyloid cascade were combined in this trial. This phase II study sought to determine the safety, tolerability, and 4/8 at month term of donanemab both by itself and in conjunction with Lilly's BACE inhibitor LY32. Unlike donanemab, which is injected intravenously, this BACE inhibitor was given orally. Studying three distinct groups allowed for an effective comparison between patients using donanemab alone and individuals taking both of Lily's medications. Lilly's BACE inhibitor was administered orally to one group while donanemab injections were administered to another, and a placebo was administered to the third group. There were 257 participants instead of the 375 who were supposed to be enrolled since their memory had been failing for at least six months and they had a score higher than a specified threshold on the Cogitates Bridging Test.
Results
Improved cognition and the capacity to carry out daily tasks demonstrated a decrease in plaque levels. Phase II initially produced encouraging results without a thorough analysis of the data and its impacts. It was determined that the patients who received donanemab infusion and the placebo group did not significantly differ in their outcomes. The trial was terminated following phase II.
Side effects :
An overview of adverse drug reactions (iADRS) during donanemab use was conducted, and the results showed no discernible difference from the placebo group. ARIA-E cases did occur, although they were asymptomatic, which is better than the symptomatic individuals observed in phase 1. [22] In October 2018, Lilly made the decision to continue donanemab trials while ending the BACE inhibitor trials. Donanemab is now effective in slowing the progression of AD, according to the results of the TRAILBLAZER-ALZ study, which was finished in 2021. However, because of the side effects, more research was required.
3. Phase – III
In October and November 2020, Lilly extended the TRAILBLAZER-ALZ to have a second study. It was run with 87 sites across Canada, The Netherlands, and Poland.[23] In May 2023, the company reported its phase III study showed the drug could slow the pace of Alzheimer’s disease by 35%. [25] In July 2023, results from 1,736 people treated with donanemab showed slowing of Alzheimer’s progression at 76 weeks, with 24% of the people displaying cerebral edema.
Promising therapeutic herbs for Alzheimer's disease include:
Figure No. 07: The effects of medicinal herbs on Alzheimer's illness
1. Ginkgo biloba (terpenoids and flavonoids)
It has been demonstrated that ginkgo biloba extract possesses anti-inflammatory and antioxidant properties that may help to reduce the progression of Alzheimer's disease. Additionally, it increases blood flow to the brain and may help prevent damage to neurons. [27]
2.Curcuma longa curcumin, or turmeric
Strong anti-inflammatory and antioxidant qualities are possessed by curcumin. It has demonstrated promise in halting the development and buildup of beta-amyloid plaques, a hallmark of Alzheimer's disease. [28]
3. Withania somnifera, or ashwagandha
The adaptogenic qualities of ashwagandha are well-known. In laboratory tests, it has demonstrated neuroprotective benefits against beta-amyloid-induced neurotoxicity and the ability to improve cognitive performance. [29]
4. Epitallocatechin-3-gallate (EGCG) in green tea (Camellia sinensis)
The possible neuroprotective benefits of EGCG, a kind of catechin, are being investigated. It is believed to reduce the neurotoxicity associated with Alzheimer's disease and prevent beta-amyloid aggregation.[30]
5. Rosmarinus Officinalis, or rosemary: (Carnosic acid, Rosmarinus acid)
In preclinical research, these substances have demonstrated neuroprotective properties, such as lowering neuroinflammation and oxidative stress, two important variables in the development of Alzheimer's disease. [31]
CONCLUSION:
Between 60 and 80 percent of cases of late-life cognitive impairment are caused by Alzheimer's disease (AD), a progressive neurodegenerative illness that is the primary cause of dementia in older people. It was first recognized by Dr. Alois Alzheimer in 1906 and is typified by the buildup of neurofibrillary tangles and amyloid plaques in the brain, which causes extensive cell death and brain atrophy. Memory, language, and decision-making skills are among the cognitive processes that are negatively impacted by these alterations, which subsequently impair fundamental physiological processes. The three stages of Alzheimer's disease progression are early (mild), middle (moderate), and late (severe). More serious deficits including speech loss, mental instability, and loss of motor control can develop from early symptoms like short-term memory loss and trouble learning new material. In the latter stages, people usually pass away from problems like infections and become totally reliant on caregivers. Alzheimer's is not regarded as a typical aspect of aging, while being largely an aging disease. Cases with early onset, such as Auguste Deter's, highlight the disease's intricacy and unpredictability. Although there isn't a cure, medications including memantine, galantamine, rivastigmine, and donepezil can enhance quality of life and momentarily reduce symptoms. Understanding the disease's molecular causes, particularly the function of tau proteins and beta-amyloid plaques, is the main goal of ongoing research funded by organizations like as the National Institute of Neurological Disorders and Stroke (NINDS). There is hope for managing this debilitating disorder through lifestyle changes, early diagnosis, and therapies meant to limit its growth. Alzheimer's disease is still a major problem in neuroscience and medicine, underscoring the need for more study and creative approaches to diagnosis, treatment, and prevention. Memantine, galantamine, rivastigmine, tacrine, and other recently approved medications are used to treat AD, and certain promising plants are being used to treat the condition.
REFRENCES



Abhijeet Welankiwar* Ashish Khade, Ankita Gawande, Pradyumna Keche, Overview of Alzheimer’s Disease (Dementia) and its Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 1404-1420. https://doi.org/10.5281/zenodo.15031491
 10.5281/zenodo.15031491
10.5281/zenodo.15031491
