Swathi College Of Pharmacy.
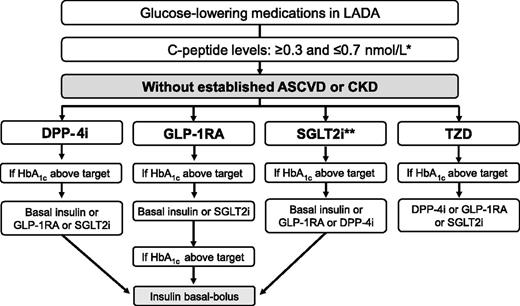
Latent autoimmune diabetes in adulthood (LADA) is a type of diabetes that has characteristics of both type – 1 and type -2 diabetes. LADA is also called as type 1.5 diabetes. This can be treated without insulin injection. Type 1.5 diabetes is mostly confused with type -1 and type 2 diabetes mellitus because there is delay in presenting features and early insulin independence. It was first discovered in the 1970’s while researching antibodies present in T1DM, some antibodies are also found in patients with T2DM. The prevalence of T2DM has been increasing over recent decades, about 537 million people in 2021. In 2019, the WHO classified LADA type diabetes as a form of diabetes that have combination features of both T1DM and T2DM , in which markers of autoimmune damage to islet cells are also found.
The global burden of diabetes is rising at an alarming rate and become a major concern of public health. Latent autoimmune diabetes (LADA) slowly progressive form of autoimmune diabetes that mainly observed in adults. It is a characterized by the presence of specific autoantibodies directed pancreatic beta cells islet and initial requirement of insulin therapy (1). LADA in adults a disease with a phenotype similar to type 2 diabetes (T2D), but with slow destruction of pancreatic β cells, has been recognized by the American Diabetes Association as a form of type 1 diabetes (T1D) in the 2022 classification (2). In initial stage of LADA it tends not to require insulin therapy for at least more than 6 months in LADA patients (3).
1. Age greater than 30years.
2. Positive autoantibodies to islet β cells.
3. Insulin independence for at least the initial 6 months after initial diagnosis (4).
LADA is immunologically similar to T1DM as antibodies to islet β cells are present although at lower levels and immune destruction progresses at a much slower rate when compared to classic T1DM. Most of these patients present with hyperglycemia that is not as same as T1DM and is misdiagnosed and managed as T2DM. Only later is it realized that they have poor control with many hypoglycemic agents, especially sulfonylureas, and eventually require insulin therapy.
LADA itself is a heterogeneous disease where some patients have high antibody levels , a low body mass index (BMI), and progress to insulin therapy rapidly. Others with low antibody levels and conditions of insulin resistance, such as a higher BMI, progress more slowly to requiring insulin. Early recognition of LADA is important so that appropriate strategies are applied to delay β-cell destruction and reduce complications.
Epidemiology:
Etiology:
Familial factors determine LADA. This in T1DM, the risk of causing LADA is inflated in bearer of definite HLA haplotypes (8). The HLA genes code for the serious tissue compatibility antigens with important Immuno regulatory functions. As a result, it is unsurprising that LADA is caused by dysregulated immunity. Although, the exact factors that abrupt, autoimmunity have not been completed. This is not like T2DM, there is an absence of studies explore the role of environmental factors like lifestyle in LADA. The causes for this are:
The non-existence of lifestyle information antecedent to the diagnosis of LADA
In some studies, LADA shares a few lifestyle risk factors with T2DM: profusion body weight, greater waist circumference to hip circumference, low birth weight, ingestion of 2 or more sweetened beverages daily, and heavy smoking. These risk factors are of greater significance in the part of LADA with lower titers of autoantibodies and higher BMI. Although the association is less muscular, these risk factors are correlated in those with higher antibody titers. Increased physical activity, moderate alcohol use, and the ingestion of fatty fish have a protective effect on the risk of LADA. Two or more cups of coffee daily increase the risk for LADA (10), unlike the beneficial effect seen in T2DM, but this observation is collected from a single study and needs to be validated (11).
Genetic Background of Lada:
Genome-wide association studies suggest that LADA shares the same genetic features as T2DM and childhood-onset TIDM, supporting the concept that LADA may be recognized as admixture of the two major types of diabetes (12). In this regard, grant et al(13).Form a strong genetic linkage with T2DM within the transcription factor 7-like 2(TCF7L2) gene,that appears to be associated with both adult-onset autoimmune diabetes and T2DM(14),where as no connection with authoritative childhood onset T1DM has been found. On the other hand human leukocyte antigen(HLA),PTP(protein tyrosine phosphatase),non-receptor type 22(PTPN22), signal transducer and activator of transcription 4(STAT4), cytotoxic T-lymphocyte -assosciated antigen 4(CTLA4),interleukin 2 receptor alpha(IL2RA), and insulin (INS),which are strictly linked to young-onset T1DM,have been also combined with autoimmune diabetes in adults(15). In this particularly the detection of high-risk HLA genotypes in subjects with LADA is related to a higher risk of increasing insulin dependence compared with low-risk of HLA (16). In this regard the DRB1*0301/DRB1*0401 heterozygosity confers the highest risk for LAD. However, the prevalence of HLA-DQB1 risk genotype that is increased in LADA, is less common than in childhood-onset T1DM(17) ,as well as it has been observed for the Cyst 1858Thr single –nucleotide polymorphism in the PTPN22 gene and the INS variable number tandem repeat (VNTR)I/I genotype expression. Altogether, these data advise that a less pronounced effect of the same genes in LADA than in classical TIDM. In addition, there is a very low detection of HLA-DR3 and –DR4 heterozygotes in Chinese population might explain the low incidence of childhood-onset T1DM in Chinese subjects possessing moderate risk or protective HLA disease associated differences. In summary, it should be underlined that a genetic background that is exclusive for LADA is still lacking up to now.
Clinical Manifestations:
Clinical Heterogenity of Lada:
Clinical, Biochemical, And Pathogenetic Features of T1DM, Lada and T2DM:
Biochemical features:
Pathophysiology features:
Biochemical features:
Pathophysiology features:
Biochemical features:
Pathophysiology features:
Pathophysiology:
LADA is a polygenic disease that involves genetic defects causing gradual β-cells destruction and insulin deficiency, combined with autoimmune features (23). Genetically, LADA differs from T1DM and T2DM, with adult-onset LADA having a lighter genetic load, potentially explaining its gradual progression (24). LADA shares similarities with T1DM in terms of autoantibody expression, both leading to autoimmune attacks on pancreatic β-cells. Compared to T2DM, LADA is more prone to triggering autoimmune reactions (25-27). Currently, there are no autoantibodies specific to LADA, making it challenging to differentiate LADA from other types of diabetes based solely on immune markers. However, among the known autoantibodies, LADA can be detected early, similar to T1DM. This places LADA in the intermediate zone between the acute autoimmune response of T1DM and the slower progression of T2DM in the autoimmune diabetes spectrum (28). Research on gut micro biota indicates associations with diabetes onset. Contrasting gut micro biota in LADA, T1DM, and T2DM may reveal distinct microbial patterns, offering a new perspective on understanding the diseases’ pathogenic mechanisms (29).
Genitics:
Data available on genetic susceptibility suggest that LADA shows a lower genetic component than T1DM. In particular, the human leukocyte antigen (HLA)-DRB1*04-DQB1*0302 and HLA-DRB1*0301-DQB1*0201, which are very common in young-onset T1DM and decrease in frequency with the increasing age at disease onset, are less frequent in LADA than in adult-onset T1DM . Similar findings have been observed for the Cyst1858Thr single-nucleotide polymorphism in the protein tyrosine phosphatase nonreceptor 22 (PTPN22) gene and the insulin variable number tandem repeat (INS VNTR) I/I genotype expression. Otherwise, the frequency of the cytotoxic T-lymphocyte-associated antigen 4 (CTLA4) Ala49Gly polymorphism in exon 1 has been shown not to be associated with the age of onset of T1DM, suggesting a similar role in LADA susceptibility Another study carried out in Swedish and Finnish populations, showed that the frequency of T2DM associated CT/TT genotypes rs7903146 in the transcription factor 7 like 2 (TCF7L2) gene was increased in LADA subjects as in T2DM subjects as well as genetic similarities with T1DM have been observed related to HLA, INS VNTR, and PTPN22 These results suggest that patients with LADA may share genetic features with both T1DM and T2DM which further supports the concept that LADA is an admixture of the two major types of diabetes .
However, it should be noted that most of these studies have investigated genes previously associated with young-onset T1DM or T2DM. Further studies are needed to better characterize the genetic susceptibility of LADA in order to establish preventive strategies as well as allow safe and effective therapies.
Auto Antibodies:
Adult-onset autoimmune diabetes and classical T1DM are hardly distinguishable immunologically, although the young-onset T1DM has a greater immunogenetic load with faster impairment of β-cells, as demonstrated by the lower C-peptide levels and the faster C-peptide decrease. Thus, LADA appears to be characterized by the same diabetes-associated autoantibody (DAA) detectable in classical T1DM. On that note, glutamic acid decarboxylase autoantibodies (GADAs) represent by far the most sensitive marker in both adult-onset T1DM and LADA even in China where it is less recurrent. Otherwise, insulin autoantibodies (IAA), protein tyrosine phosphatase IA-2 (IA-2A), and islet-specific zinc transporter isoform 8 (ZnT8) autoantibodies, which are frequent in younger subjects with recent diagnosis of T1DM, are less prevalent in LADA patients. However, mixed data have been reported in literature. Silvia pieralica et al. observed that the specific IA-2 construct 256–760 appears to be more frequent in LADA than previously reported, stressing the concept that the occurrence of other DAA could be also indicative of LADA.
Autoimmunity:
LADA is a type of autoimmune-mediated diabetes from an etiological perspective. The immune characteristics of LADA include islet inflammation, islet autoantibodies, and reactive T cells to islet antigens (30). Research on LADA autoantibodies is mainly based on T1DM, including GADA, IAA, IA-2 A, ZnT8A, and ICA (25). Additionally, LADA have autoantibodies to transmembrane protein 7 (Tspan7) and carboxypeptidase H (CPH) (31, 32). Among them, GADA is the most sensitive diagnostic marker for LADA. In LADA, IA-2 A autoantibodies may be associated with a higher frequency of autoimmune diabetes HLA-susceptible genotypes and an increased risk of developing thyroid autoimmunity. Claudio suggests testing for IA-2 A autoantibodies can help identify islet autoimmunity. LADA may have one or more positive insulin autoantibodies, but fewer individuals have multiple positive antibodies. Simultaneous detection of multiple antibodies can improve diagnostic sensitivity. Although these antibodies assist in diagnosing LADA, their lack of specificity limits their application in research. Increasing evidence suggests that acquired immunity and innate immunity play a key role in the etiology of LADA (26,27). Besides, research has found that gut micro biota and metabolites can participate in the physiological and pathological status of LADA through immune regulation (33).
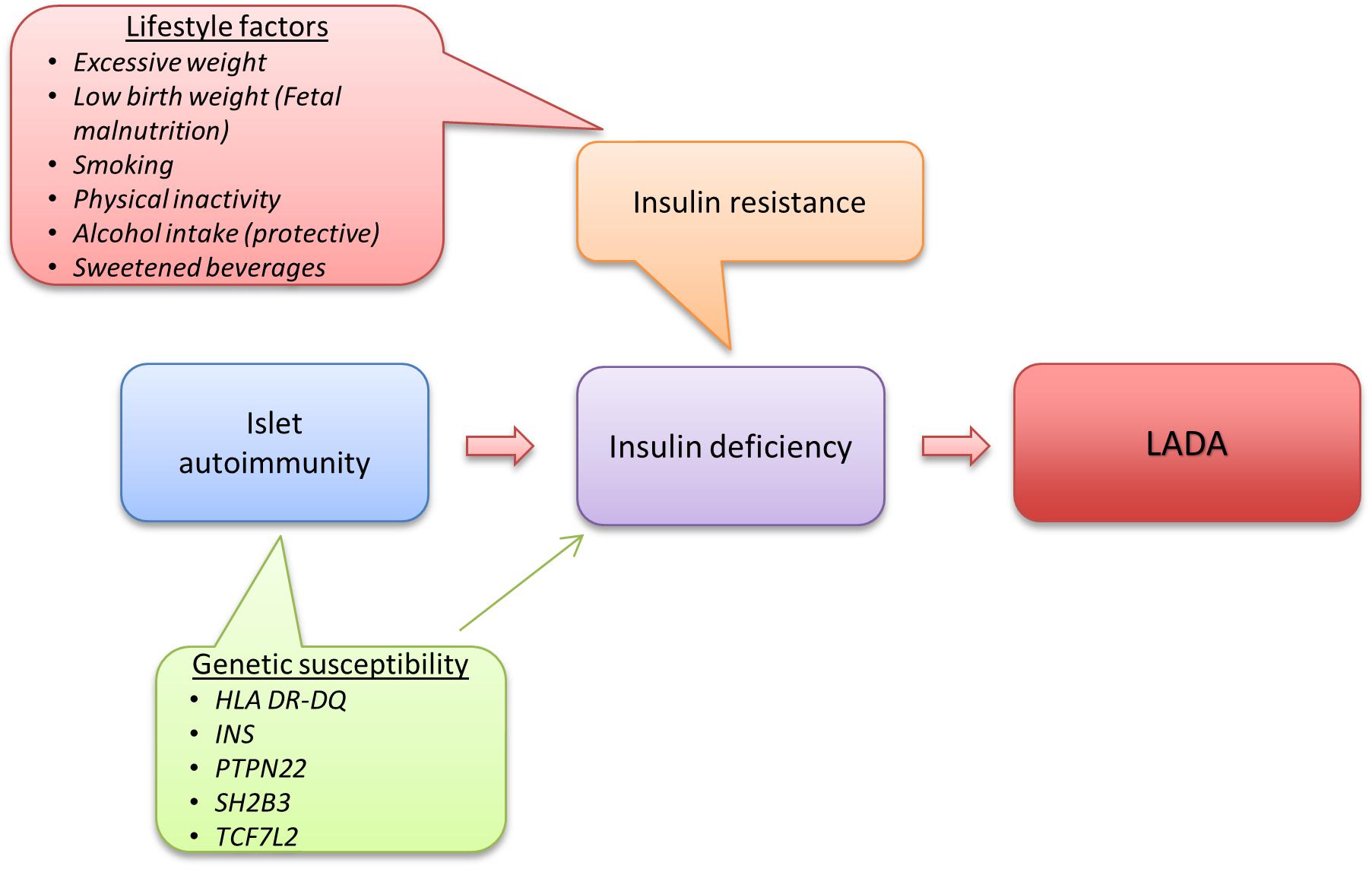
Figure: 1 Etiology and Pathogenesis of Latent Autoimmune Diabetes in Adults (LADA) Compared to Type 2 Diabetes
Characterstics Of Lada:
1. Phenotypical features:
Based on studies of the UK Prospective Diabetes Study (UKPDS) (34) and the Botnia study (35) show that the autoantibody frequency (GADA) in patients diagnosed with T2D is higher in younger patients compared with older patients. On average, patients with LADA, compared with those with antibody-negative T2D, are younger at diabetes diagnosis with lower BMI and have a family history of autoimmune diseases. Metabolic syndrome tends to have a similar or higher frequency in LADA compared with adult-onset T1D (35,36,37) but compared with autoantibody-negative T2D patients, LADA patients show a lower frequency, However, there is considerable heterogeneity, with some patients having a T1D phenotype (without metabolic syndrome) while others are misdiagnosed from T2D (with metabolic syndrome)(36,38) Although patients with LADA have less major cardiovascular risk factors, i.e., they are leaner, with better lipid and BP profiles, there is no difference in cardiovascular outcomes in them compared with T2D patients after adjustment for traditional cardiovascular risk factors (39,40).
2. Autoantibodies:
GADA (Glutamic acid decarboxylase autoantibodies) is the most sensitive marker of LADA as it is the most important autoantibody, whether in Europe or China, and in primary or in secondary care. GADA can be detected by commercially available radioimmunoassay and ELISA. GADA specificity has improved from 94% to 99% from 2010 to 2018 according to the international islet autoantibody standardization program (41).Patients with high GADA levels tend toward a T1D-like phenotype with lower BMI and lower prevalence of metabolic syndrome (42,43,44). In addition, UKPDS (United Kingdom prospective diabetes study) and all other studies found that high GADA levels were associated with an increased risk of insulin requirement (34). Diabetes-associated autoantibody positivity is predictive for progression both to non–insulin-dependent diabetes (45, 46,47)and especially to future insulin dependency after the diagnosis of diabetes. However, not all patients in UKPDS and in other studies required insulin, even after 10 years from diagnosis. An important feature of LADA is the more risk of other organ-specific autoantibodies and autoimmune diseases. GADA are predictive of thyroid autoimmunity (42, 48, 49, 50), while IA-2 autoantibodies confer a high risk of celiac disease–associated autoimmunity in China (15). Moreover, in LADA, high GADA levels are strongly associated with thyroid autoimmunity and inversely related to the serum cytokine profile (49, 50).
3. Genetic susceptibility:
The shared genetic susceptibility of LADA and T1D includes polymorphisms within the HLA, DQB1 and DRB1 genes and within the insulin and protein-tyrosine-phosphatase nonreceptor 22 (PTPN22) genes (51); all these gene polymorphisms and the Src (SH domains) homology 2-B (SH2B3) gene were identified in a recent large well-powered genome-wide association study (52). In relatively small studies, LADA was associated with the strongest T2D variant transcription factor 7–like 2 (TCF7L2) (53-55), especially in obese persons (56), but not in the genomewide association study or in a Chinese study, the latter potentially due to ethnic differences(52,57). Moreover, class I genes (HLA-A and HLA-B) are not associated with LADA, whereas they are strongly associated with childhood-onset T1D (58). Application of gene risk scores may assist stratification of rates of progression to insulin dependency in patients with diabetes-associated autoantibodies and help identify cases likely to have false positive autoantibodies (59).
Diagnosis:
The diagnosis is mainly classified on three criteria 1) adult age at onset of diabetes, 2) The presence of circulating islet autoantibodies, which differentiate LADA from type 2 diabetes , 3)insulin independence , which differentiate LADA from type 1 diabetes . Insulin production eventually decreases due to the autoimmune destruction of pancreatic beta cells. In LADA patients the often detected conditions are autoantibodies to glutamic acid decarboxylase (GAD), islet antigen-2 (IA-2), and insulin independence .Metformin is often used as first line treatment for type 1.5diabetes to improve insulin sensitivity, reducing glucose production in the liver.
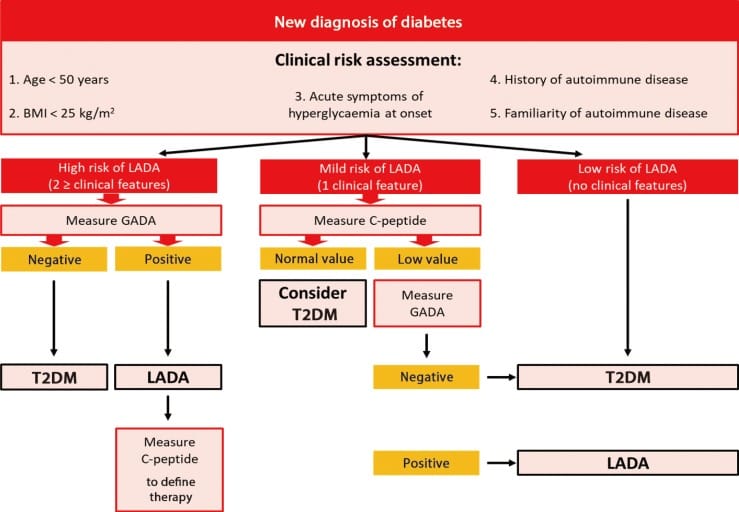
Figure: 2 Algorithm for diagnosis of latent autoimmune diabetes in adults (LADA) vs type -2 diabetes mellitus 2.
The individuals with type 1.5 diabetes have the same symptoms of type 1 diabetes and some of the antibodies.
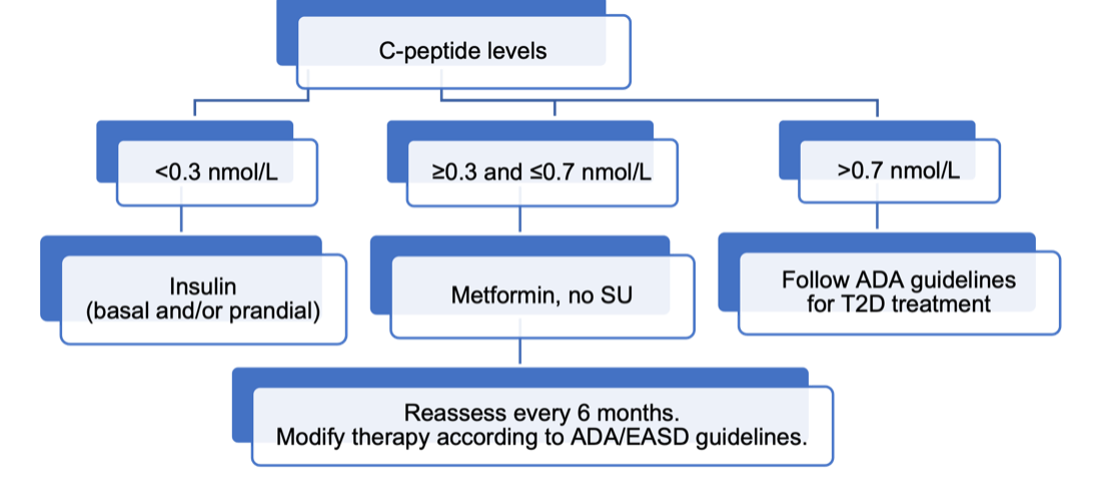
Figure:3 C-peptide levels during diagnosis of latent autoimmune diabetes in adult (LADA).
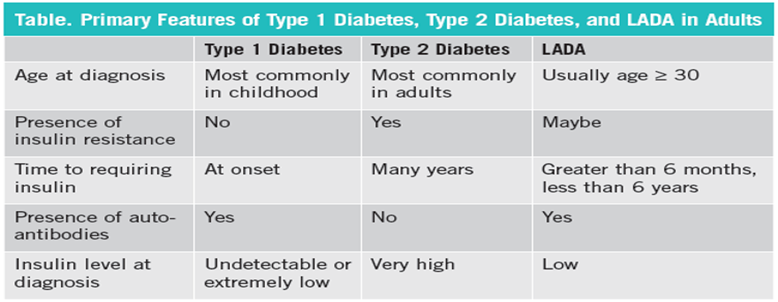
Table: 1 Primary features of Type 1 diabetes, Type 2 diabetes and Latent autoimmune diabetes in adult.
Treatment:
Goals Of Treatment:
-To preserve maintaining beta cell function and even regenerate beta cells.
-To improve glucose levels.
-To decrease long-term complications.
Hypoglycemic Agents:
Insulin Sensitizers (Metformin, Thiazolidinediones): The majority of LADA are clinically diagnosed as T2DM and primarily treated with Metformin before they are identified as having LADA. Although there is a minor evidence for the use of Metformin, there is no evidence against its use. Results from ongoing clinical trials investigating the effects in LADA patients of monotherapy/ adjunct Metformin on metabolic control, beta – cell function will provide more evidence on the precise role of Metformin. Thiazolidinediones enhances insulin sensitivity by activating nuclear peroxisome proliferator-activated receptors gamma receptors. Limited data is available on their use in patients with LADA. More long-term studies are warranted, and clinicians need to be aware of potential side effects, including weight gain, edema, and congestive heart failure, fractures, and macula edema (49).
Insulin:
While insulin therapy is essential in all cases with undetectable C-peptide, patients diagnosed with LADA have, by definition, residual β-cell function and, in general, slow progression toward insulin dependency. A major question is whether insulin therapy should be the initial treatment for LADA (60). Most studies are agree that insulin intervention is effective and safe for LADA with residual beta cell function. Results from preclinical studies advices that the administration of exogenous insulin supports beta cell function and decrease the insulitis 59 both because reduction of the glucotoxicity and also reduces the islets cell activation. Furthermore, insulin therapy can suppress auto reactive T-cells through local release of regulatory cytokines.
Dipeptidylpeptidase (DPP) 4 Inhibitors:
Dipeptidyl peptidase (DPP) 4 inhibitors alone or when combined with insulin in preserving β-cell function in LADA. They affect metabolic control by prolonging endogenous glucagon-like peptide-1 (GLP1) and other peptides. Their main action is to enhance the levels of GLP1, suppressing glucagon and increasing insulin secretion after a glucose load. DPP4 receptors have also been identified on the surface of T lymphocytes, where they may affect immune regulation. This latter action may be play a role in slowing the β-cell immune destruction in LADA.(61) Some studies with DPP4 inhibitors have demonstrated improved diabetic control and preservation of β-cell function.(62,63,64,65,) There is limited data to assess the use of GLP1 agonists in managing patients with LADA. However, dulaglutide studies have shown decrease in HbA1c levels.
Sulfonyl Ureas:
Sulfonylureas (e.g., glipizide, glimepiride, glyburide) are not recommended for the treatment of LADA. Sulfonylureas increase the release of insulin from pancreatic β-cells. This mechanism solely depends on functioning β-cells, which is not present in LADA. There is also an increased risk of hypoglycemia when combining sulfonylureas and insulin therapy.
Sodium-Glucose Co Transporter 2 Inhibitors:
Sodium-glucose co transporter 2 inhibitors (e.g., canagliflozin, dapagliflozin, empagliflozin) reduce reabsorption of glucose in kidney tubules. A few studies suggest that this medication class may be promising for LADA. The increased risk of ketoacidosis in patients with medium to low C-peptide is a limiting factor to the use of SGLT2is in patients with LADA. Ketoacidosis may be more common in patients who are not overweight (BMI <27 kg/m2).
Glucagon –Likepeptide-1 Receptor Agonists:
Glucagon-like peptide-1 receptor agonists (e.g., dulaglutide, liraglutide, semaglutide) have shown beneficial results in terms of improving metabolic control in patients with LADA, unless C-peptide levels are very low. The AWARD trial studied the effect of dulaglutide on glycemic control in a small portion of patients with LADA. Results showed comparable A1C reductions in both populations that were GAD65 antibody positive and negative at 12 months. This data was the first to represent GLP-1RA effectiveness in patients with LADA.
CONCLUSION:
In recent years, the incidence and prevalence patients with adult-onset autoimmune diabetes have gradually increased. LADA, which indicates for the majority of adult-onset autoimmune diabetes, has clinical features of both T1D and T2D. Due to disease heterogeneity, it is difficult to determine the therapeutic regimen for LADA and therapy should individualized according to the features of LADA patient. The therapy of LADA includes majorly insulin therapy or a combination of insulin and other types of hypoglycemic agents. In LADA patients we observe rapid decline in beta cell function and more likely to suffer from diabetic complications. The main goal of LADA treatment is metabolic control and preservation of insulin residual insulin secretion function. LADA is immunologically similar to T1DM as antibodies to islet β cells are present although at lower levels and immune destruction progresses at a much slower rate when compared to classic T1DM. Most of these patients present with hyperglycemia that is not as same as T1DM and is misdiagnosed and managed as T2DM. Only later is it realized that they have poor control with many hypoglycemic agents, especially sulfonylureas, and eventually require insulin therapy.
REFRENCES





Dr. N. Muthurani*, S. K. Sheema, O. Sushmitha, V. Jokesh, P. Deepa, Over View On Latent Autoimmune Diabetes in Adulthood, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 944-958. https://doi.org/10.5281/zenodo.15010546
 10.5281/zenodo.15010546
10.5281/zenodo.15010546
