1, 2Chandra Shekhar Singh College of Pharmacy, Prayagraj, Uttar Pradesh
3Department of Pharmaceutics, Faculty of Pharmacy, Integral University Lucknow, Uttar Pradesh
4, 5Malti Memorial Trust CSM Group of Institutions, Faculty of B. Pharmacy, Iradatganj Prayagraj, Uttar Pradesh
Ocular drug delivery remains a significant challenge due to the unique anatomical and physiological barriers of the eye, such as tear turnover, blinking, nasolacrimal drainage, and limited corneal permeability. This results in frequent dosing and decreased patient compliance because traditional ophthalmic dose forms, especially eye drops, have poor ocular bioavailability, frequently below 5%. Ocular inserts are a cutting-edge drug delivery method that can get beyond these restrictions by extending the duration of residence in the conjunctival sac and facilitating regulated, prolonged drug release. This review provides a comprehensive overview of developments in ocular insert technology, focusing on formulation tactics, polymer selection, manufacturing methods, release mechanisms, and therapeutic uses. Discussions are held regarding the mechanical strength, mucoadhesive qualities, biocompatibility, and biodegradability of both natural and manufactured polymers. The function of various design architectures, such as matrix and reservoir systems, in accomplishing regulated ocular medication administration is assessed. It highlights recent advancements in manufacturing techniques such solvent casting, hot-melt extrusion, and electrospinning for better drug loading effectiveness and release control.Important evaluation techniques are also described in the review, such as ex vivo permeation tests, in vitro drug release investigations, physicochemical characterisation, and in vivo performance evaluation. Ocular inserts' versatility and clinical potential are demonstrated by their therapeutic applications in glaucoma, ocular infections, inflammation, and dry eye syndrome. The final section discusses the present obstacles and potential advancements in patient-centered and customized ocular medication delivery systems
The eye poses significant obstacles to medication distribution that have plagued pharmaceutical researchers for many years. For anterior segment illnesses, topical administration with eye drops is still the most popular therapeutic option; nevertheless, this strategy has inherent inefficiencies. The generation of tears, blinking reflexes, and nasolacrimal drainage are some of the eye's natural defense systems that combine to quickly remove foreign objects from the ocular surface. Because of this, less than 5% of a dose usually reaches the intraocular tissues; the majority of the medication is either absorbed systemically through the nasal mucosa or washed away[1].For conventional eye drops to maintain therapeutic concentrations, regular administration is necessary, usually three to six times per day. In chronic illnesses like glaucoma, where non-compliance rates surpass 50%, this dosage schedule presents serious difficulties for patient adherence[2,3]. Ointments can lengthen hospital stays, but patients may not take them because they induce discomfort and blurred vision[4]. Because of these constraints, research has focused on controlled-release devices that can lower dosage frequency while maintaining effective medication levels over prolonged periods of time.Ocular inserts have become viable substitutes that solve a number of issues with traditional formulations. These solid or semi-solid implants release medication in a controlled manner while remaining in the conjunctival sac or fornix for hours to days. Inserts increase bioavailability, decrease systemic adverse effects, and improve patient compliance by extending contact time with ocular tissues and offering sustained release[5, 6, 7]. Electrospun nanofibers, biodegradable polymers, mucoadhesive systems, and nanotechnology integration are just a few of the impressive advancements in insert technology that have occurred during the last 20 years[8,9,10]. With an emphasis on design concepts, material selection, drug release mechanisms, fabrication techniques, assessment methodologies, and therapeutic applications, this review explores the state of ocular insert technology today.
2. Ocular Barriers and Drug Delivery Challenges
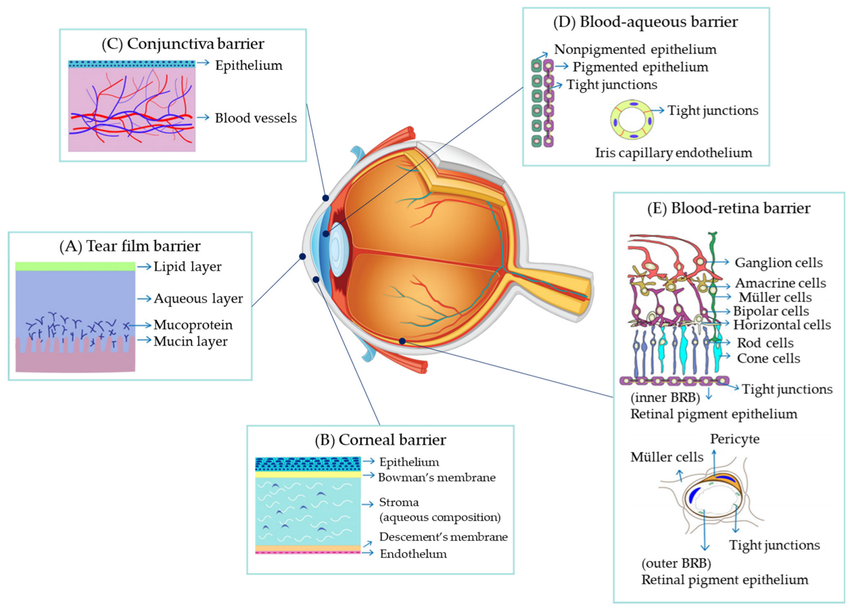
Figure 1. Major anatomical and physiological barriers to ocular drug delivery.
2.1 Anatomical Barriers
The structure of the eye makes drug administration challenging in a number of ways. Even though it is tiny, the precorneal region has dynamic barriers that quickly remove drugs that have been administered topically. The tear film, which has a volume of roughly 7–10 μL, is continuously rotated every two to three minutes[11]. Extra volume that exceeds the tear film's capacity is rapidly emptied through the nasolacrimal duct when eye drops are administered. Blinking, which happens 15–20 times per minute, speeds up the elimination of drugs[12].Although the cornea is the main entrance to the anterior chamber, it has a high permeability rate. Its multilayered structure, which consists of an endothelium, hydrophilic stroma, and lipophilic epithelium, forms alternate barriers that prevent the passage of both lipophilic and hydrophilic medications. The only molecules that can effectively pass through all corneal layers are those with appropriate lipophilicity (log P of 2-3)[13, 14]. The rate-limiting barrier for the majority of hydrophilic substances is represented by the tight junctions of the epithelium.
With a larger surface area (17 cm2) than the cornea (1 cm2), the conjunctiva provides an alternate absorption channel; nevertheless, medications absorbed via this pathway are quickly cleared by lymphatics and blood vessels[15]. Designing inserts with a longer residence duration and continuous release that can overcome these obstacles requires an understanding of these obstacles.
2.2 Physiological Clearance Mechanisms
Physiological processes aggressively eliminate foreign contaminants from the ocular surface in addition to anatomical barriers. Lacrimal gland-controlled tear production keeps the ocular surface hydrated while also diluting and washing away medications that have been delivered. About 80–90% of injected eye drops drain within two to five minutes thanks to nasolacrimal drainage, which offers a direct elimination channel[16]. Drug molecules can be bound by tear proteins such as lactoferrin and lysozyme, which lowers the amount of free drug that is accessible for absorption. Furthermore, some medications can be broken down by metabolic enzymes found in tears and ocular tissues before they reach their intended targets[17]. Through mucoadhesion, physical properties that hinder ejection, or strategic placement, ocular inserts must be made to withstand these clearance mechanisms.
3. Classification and Design of Ocular Inserts
3.1 Classification Systems
Ocular inserts can be classified based on multiple criteria including solubility, drug release mechanism, and structural design. Understanding these classifications helps in selecting appropriate systems for specific therapeutic applications.
Solubility-Based Classification:
Release Mechanism Classification:
3.2 Design Considerations
A number of criteria must be balanced for an ocular implant to be designed successfully. The conjunctival fornix must be accommodated by size and shape without causing discomfort; the usual dimensions are 3-10 mm in diameter and 0.5-2 mm in thickness[24]. Comfort during eye movements and blinking is ensured by flexibility. While some opacity may be tolerated by inserts positioned in the lower fornix, transparency or translucency reduces visual interference.
By creating connections with the mucin in the tear film, mucoadhesive qualities improve retention. Polymers like chitosan, carbomer, and certain cellulose derivatives exhibit strong mucoadhesion through hydrogen bonding and electrostatic interactions[25, 26]. Surface characteristics including smoothness, wettability, and charge influence comfort and retention.For therapeutic doses to be administered during the planned release period, the drug loading capacity must be adequate. For chronic conditions requiring weeks of therapy, higher loading is necessary. Release kinetics should be in line with therapeutic needs; some applications require continuous zero-order release, while others benefit from an initial burst release followed by sustained levels[27].
4. Polymer Selection for Ocular Inserts
4.1 Natural Polymers
Natural polymers offer excellent biocompatibility, biodegradability, and often inherent mucoadhesive properties. Chitosan, derived from chitin, has gained particular attention due to its positive charge that interacts with negatively charged mucin. Studies have demonstrated chitosan-based inserts for various drugs including antibiotics, anti-inflammatories, and antiglaucoma agents[28, 29]. Its antimicrobial activity provides additional therapeutic benefits for ocular infections.Sodium alginate, extracted from brown seaweed, forms gels in presence of divalent cations like calcium. Alginate inserts exhibit good biocompatibility and can be easily fabricated through ionic crosslinking. Combinations with other polymers enhance mechanical properties and release characteristics[30]. Gelatin, a collagen derivative, offers excellent biocompatibility and can be crosslinked to control degradation rates and drug release[31].Hyaluronic acid, a glycosaminoglycan naturally present in ocular tissues, provides exceptional biocompatibility and mucoadhesion. Its viscoelastic properties enhance precorneal residence time. However, its high cost and rapid degradation may limit applications[32]. Cellulose derivatives including hydroxypropyl methylcellulose (HPMC) and hydroxypropyl cellulose (HPC) are widely used due to their safety profile, water solubility, and film-forming properties[33].
4.2 Synthetic Polymers
Synthetic polymers offer advantages in reproducibility, tunable properties, and mechanical strength. Polyvinyl alcohol (PVA) is widely employed for its excellent biocompatibility, transparency, and film-forming ability. PVA-based inserts have been commercialized and show good patient acceptance[34]. Polyvinylpyrrolidone (PVP) serves as a hydrophilic carrier with good solubility and low toxicity.Polyacrylic acid derivatives, particularly carbomers, exhibit strong mucoadhesive properties through hydrogen bonding with mucin. These polymers form clear gels at physiological pH and have been extensively studied for ophthalmic applications[35]. Eudragit polymers, pH-sensitive methacrylate copolymers, enable pH-triggered release and have been used in combination with other polymers to modulate release kinetics[36].Biodegradable polyesters including poly(lactic-co-glycolic acid) (PLGA), polylactic acid (PLA), and polycaprolactone (PCL) offer controlled degradation through hydrolysis. PLGA's degradation rate can be adjusted by varying the lactide:glycolide ratio, allowing customization of release duration from days to months[37, 38]. These polymers are particularly suitable for long-acting inserts and have excellent safety profiles with FDA approval for various medical applications.
4.3 Polymer Combinations
Combining multiple polymers often yields superior properties compared to single-polymer systems. Blends can optimize mechanical strength, mucoadhesion, release kinetics, and patient comfort simultaneously. For example, chitosan-alginate combinations leverage chitosan's mucoadhesion and alginate's gel-forming ability [39]. PVA-PLGA blends combine PVA's comfort and transparency with PLGA's sustained release capabilities[40].Interpenetrating polymer networks (IPNs) create intimate polymer mixing at the molecular level, producing synergistic properties. Semi-IPNs, where one polymer is crosslinked while the other remains linear, offer intermediate characteristics[41]. Selection of polymer combinations requires consideration of compatibility, processing methods, and desired final properties.
5. Drug Release Mechanisms
5.1 Diffusion-Controlled Release
Diffusion represents the primary release mechanism in many ocular inserts. In matrix systems, drugs dispersed throughout the polymer diffuse through the hydrated matrix to the surrounding tear fluid. Release rate depends on drug solubility, diffusion coefficient, polymer swelling, and matrix tortuosity[42]. Higuchi's model often describes this process for matrix systems with drug loading below solubility limits.Reservoir systems employ rate-controlling membranes that govern diffusion. The membrane's permeability, thickness, and surface area determine release kinetics. Reservoir designs can achieve near zero-order release, providing constant drug levels over extended period[43]. However, membrane defects or rupture can cause sudden dose dumping, a significant safety concern.Factors affecting diffusion include polymer hydration state, drug-polymer interactions, and environmental conditions. Hydrophilic polymers swell in aqueous media, creating channels for drug diffusion. Drug molecular weight, charge, and lipophilicity influence diffusion rates through polymer matrices[44].
5.2 Erosion-Controlled Release
Biodegradable polymers release drugs through surface erosion or bulk degradation. Surface erosion occurs when degradation proceeds from the outer surface inward, potentially providing zero-order release if erosion rate remains constant[45]. Bulk degradation involves water penetration throughout the matrix with random chain scission, typically showing first-order kinetics.PLGA and related polyesters degrade through hydrolysis of ester bonds, with degradation rate influenced by molecular weight, crystallinity, and lactide:glycolide ratio. Higher glycolide content accelerates degradation due to greater hydrophilicity[46]. PCL degrades more slowly than PLGA, suitable for very long-term release applications.Erosion-controlled systems offer advantages for poorly soluble drugs that might not release adequately through diffusion alone. As the polymer erodes, encapsulated drug is liberated regardless of its solubility characteristics[47].
5.3 Swelling-Controlled Release
Some inserts utilize polymer swelling as the primary release mechanism. Glassy polymers initially restrict drug diffusion, but upon hydration, they undergo glass transition and swell, creating pathways for drug release[48]. The swelling rate governs release kinetics. Hydrogels represent a special class of swelling-controlled systems. These three-dimensional networks absorb large amounts of water while maintaining structural integrity. Drug release from hydrogels depends on mesh size, crosslinking density, and drug-polymer interactions[49]. Stimuli-responsive hydrogels can respond to pH, temperature, or ionic strength changes, enabling triggered or modulated release.
5.4 Combination Mechanisms
Many modern inserts employ multiple release mechanisms simultaneously. For instance, microparticle-loaded matrix systems combine diffusion from the matrix with erosion of PLGA microparticles, producing biphasic release profiles[50]. Initial burst release from the matrix surface provides rapid therapeutic levels, followed by sustained release from embedded microparticles.
Understanding and controlling release mechanisms enables rational design of inserts with desired pharmacokinetic profiles. Mathematical modeling helps predict release behavior and optimize formulations before extensive experimental work[51].
|
Release mechanism |
Controlling principle |
Kinetic model |
Typical polymers/systems |
|
Diffusion-controlled |
Drug diffusion through hydrated polymer matrix |
Higuchi model |
PVA, HPMC |
|
Erosion-controlled |
Polymer degradation and matrix erosion |
Zero- or first-order |
PLGA, PCL |
|
Swelling-controlled |
Polymer swelling and chain relaxation |
Korsmeyer–Peppas |
Hydrogels |
|
Combined mechanisms |
Concurrent diffusion and degradation |
Biphasic kinetics |
Composite systems |
6. Manufacturing Technologies
6.1 Solvent Casting
Solvent casting remains the most common method for preparing ocular inserts due to its simplicity and versatility. The process involves dissolving polymers and drugs in appropriate solvents, casting into molds, and evaporating the solvent to form films[52]. Plasticizers like glycerol or propylene glycol may be added to improve flexibility.Advantages include ease of scale-up, ability to incorporate heat-sensitive drugs, and control over film thickness through solution concentration and mold depth. Disadvantages include potential solvent residues, environmental concerns, and lengthy drying times. Careful solvent selection and drying conditions minimize residual solvents below regulatory limits[53].Variations include layer-by-layer casting for multilayer inserts and incorporation of microparticles or nanoparticles into the casting solution for composite systems[54].
6.2 Hot-Melt Extrusion
Hot-melt extrusion (HME) has gained attention as a solvent-free manufacturing technique. Polymers and drugs are mixed and heated above the glass transition temperature, then forced through a die to produce films or shaped inserts[55]. The process offers advantages of continuous manufacturing, no solvent residues, and excellent content uniformity.Recent studies have demonstrated HME for producing biodegradable ocular inserts with sustained release characteristics. Process parameters including temperature, screw speed, and die design significantly influence product properties[56]. HME is particularly suitable for hydrophobic drugs and polymers.Challenges include thermal degradation of heat-sensitive drugs, limited drug loading capacity, and equipment costs. However, advances in processing aids and low-temperature HME are expanding applications[57].
6.3 Electrospinning
Electrospinning produces nanofiber-based inserts with high surface area and porosity. The technique applies high voltage to a polymer solution, creating a charged jet that solidifies into ultrafine fibers collected on a target[58]. Nanofiber inserts offer rapid hydration, good mechanical properties, and high drug loading capacity.Recent innovations include coaxial electrospinning for core-shell fibers enabling dual-drug delivery, and emulsion electrospinning for incorporating hydrophilic drugs into hydrophobic polymer fibers[59, 60]. Nanofiber orientation can be controlled through collector design, influencing mechanical properties and release kinetics.Electrospun inserts have shown promise for antiglaucoma drugs, antibiotics, and anti-inflammatory agents. The high surface area facilitates rapid drug release, while fiber composition and diameter control release rates[61].
6.4 3D Printing
Additive manufacturing technologies enable fabrication of complex geometries and personalized inserts. Fused deposition modeling, inkjet printing, and stereolithography have been explored for ocular inserts[62]. 3D printing allows precise control over dimensions, drug distribution, and release patterns.Advantages include design flexibility, rapid prototyping, and potential for personalized medicine based on individual patient anatomy and needs. Challenges include limited material options, resolution constraints, and regulatory considerations for patient-specific devices[63].
7. Nanotechnology Integration
7.1 Nanoparticle-Loaded Inserts
Incorporating nanoparticles into ocular inserts combines advantages of both technologies. Nanoparticles can enhance drug solubility, protect labile compounds, and provide controlled release, while the insert matrix offers prolonged retention and ease of application[64]. Various nanoparticle types have been investigated including polymeric nanoparticles, liposomes, solid lipid nanoparticles, and niosomes.PLGA nanoparticles loaded into PVA or chitosan matrices demonstrate sustained release over weeks, with the nanoparticles providing an additional diffusion barrier[65]. Liposomal inserts enhance corneal penetration of hydrophilic drugs through membrane fusion mechanisms[66]. Solid lipid nanoparticles offer advantages for lipophilic drugs and can be produced without organic solvents.The dual-barrier system nanoparticle encapsulation plus matrix diffusion enables complex release profiles including initial burst followed by sustained release. This biphasic pattern can provide rapid symptom relief while maintaining therapeutic levels[67].
7.2 Mucoadhesive Nanovesicles
Mucoadhesive nanovesicles including niosomes and transfersomes incorporated into insert matrices enhance both retention and permeation. These vesicular systems can deform and penetrate through intercellular spaces, improving bioavailability[68]. Chitosan-coated nanovesicles show enhanced mucoadhesion and prolonged release when loaded into insert matrices. Recent studies demonstrate mucoadhesive nanovesicle-loaded spongy inserts with superior performance compared to conventional formulations. The spongy structure provides comfort and flexibility while nanovesicles ensure sustained release and enhanced penetration[69].
7.3 Nanofiber-Nanoparticle Composites
Advanced systems combine electrospun nanofibers with embedded nanoparticles, creating hierarchical structures with multiple length scales. Nanoparticles can be incorporated during electrospinning or loaded onto nanofibers post-fabrication[70]. These composites offer high drug loading, controlled release, and excellent mechanical properties. Core-shell nanofibers with drug-loaded nanoparticles in the core and polymer shell provide sequential release shell dissolution followed by nanoparticle-controlled release[71]. Such systems enable dual-drug delivery with independent release kinetics for combination therapy.
8. Evaluation Methodologies
8.1 In Vitro Characterization
Comprehensive characterization ensures insert quality and predicts in vivo performance. Physical characterization includes dimensions, thickness uniformity, weight variation, folding endurance, and surface morphology via scanning electron microscopy[72]. These parameters affect comfort, handling, and clinical performance.Drug content uniformity must be assessed to ensure consistent dosing. High-performance liquid chromatography (HPLC) or spectroscopic methods quantify drug loading across different insert batches[73]. Content uniformity typically should be within 85-115% of the labeled amount.Mechanical properties including tensile strength, elongation at break, and elasticity indicate insert flexibility and durability during handling and blinking. Texture analyzers measure these properties, with acceptable inserts showing sufficient strength without brittleness[74].
8.2 In Vitro Drug Release Studies
Release studies predict in vivo behavior and support formulation optimization. Dissolution apparatus must simulate ocular conditions including limited fluid volume, physiological pH, and temperature. USP apparatus modifications or custom cells are employed, typically using 2-5 mL of simulated tear fluid or phosphate buffer pH 7.4 at 37°C[75].Sink conditions may not be maintained due to small volumes, requiring consideration of saturation effects. Sampling at predetermined intervals followed by HPLC or spectroscopic analysis generates release profiles. Mathematical modeling using zero-order, first-order, Higuchi, Korsmeyer-Peppas, and Hixson-Crowell equations elucidates release mechanisms[76].Release studies should continue until 80-90% drug release or until the intended wear time is reached. Accelerated studies at elevated temperatures can predict long-term stability and release characteristics[77].
8.3 Mucoadhesion Assessment
Mucoadhesive strength determines retention time in the conjunctival sac. Ex vivo methods using excised animal cornea or conjunctiva in texture analyzers measure detachment force or work of adhesion[78]. The insert is applied to the tissue under controlled force and time, then detachment force is measured.In vitro wash-off tests evaluate retention under flow conditions simulating tear drainage. Inserts are attached to tissue or model surfaces in a flow-through apparatus, and time to detachment is recorded[79]. Longer retention correlates with better mucoadhesion.Rheological studies of polymer-mucin mixtures provide insights into mucoadhesive interactions. Increased viscosity or elastic modulus upon mixing indicates strong interactions[80].
8.4 In Vivo Studies
Animal studies assess ocular tolerance, pharmacokinetics, and therapeutic efficacy. Rabbits are commonly used due to their large eyes and availability, though anatomical differences from humans must be considered[81]. Studies evaluate irritation potential using Draize scoring of redness, swelling, and discharge.Retention time is measured by observing insert presence in the conjunctival sac over time. Fluorescent markers or radiolabels enable tracking[82]. Pharmacokinetic studies measure drug concentrations in tears, aqueous humor, and ocular tissues using bioanalytical methods.Efficacy studies in disease models such as glaucoma models using topical corticosteroids or surgical procedures demonstrate therapeutic benefit. Intraocular pressure reduction, infection clearance, or inflammation resolution are assessed depending on the indication[83].
8.5 Clinical Evaluation
Human trials ultimately determine clinical utility. Phase I studies assess safety and tolerability in healthy volunteers, evaluating comfort, vision effects, and retention. Phase II/III studies in patient populations compare efficacy and safety against standard treatments[84].Patient-reported outcomes including comfort, ease of insertion/removal, and quality of life are critical endpoints. Objective measures include intraocular pressure for glaucoma, bacterial counts for infections, or clinical grading scores for inflammation[85].
9. Therapeutic Applications
9.1 Glaucoma Management
Glaucoma, characterized by elevated intraocular pressure damaging the optic nerve, represents a major application for ocular inserts. Standard therapy requires daily eye drops, often multiple medications, leading to poor adherence. Inserts delivering antiglaucoma drugs offer improved compliance and sustained pressure reduction[86].Prostaglandin analogs, beta-blockers, alpha-agonists, and carbonic anhydrase inhibitors have been formulated in inserts. Recent studies demonstrate nanofiber inserts delivering timolol and dorzolamide combination therapy with sustained release over 7 days and significant IOP reduction in rabbit models[87]. Brimonidine-loaded electrospun inserts showed comparable efficacy to eye drops with reduced dosing frequency[88].Biodegradable PLGA-based inserts provide month-long drug release, potentially reducing administration to monthly intervals. Such extended-release systems could transform glaucoma management, particularly for patients struggling with daily drop regimens[89].
9.2 Ocular Infections
Bacterial, viral, and fungal infections of the anterior segment benefit from sustained antimicrobial delivery. Conventional antibiotic drops require frequent dosing often hourly in severe infections which is impractical for patients and caregivers. Inserts can maintain therapeutic concentrations continuously[90].Fluoroquinolone antibiotics including ciprofloxacin, levofloxacin, and moxifloxacin have been incorporated into various insert formulations. Studies demonstrate sustained release over 3-7 days with effective bacterial clearance in infection models[91]. Antifungal inserts containing natamycin or voriconazole address fungal keratitis, a sight-threatening condition requiring prolonged therapy[92].Combination antibiotic-steroid inserts treat infectious inflammation, common after ocular surgery. Dual-drug nanofiber inserts with independent release profiles optimize therapy by providing initial high antibiotic levels with sustained anti-inflammatory effects[93].
9.3 Inflammation and Allergy
Corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) formulated in inserts treat various inflammatory conditions including uveitis, post-operative inflammation, and allergic conjunctivitis. Sustained delivery reduces the high peak concentrations associated with drops while maintaining therapeutic levels[94].Dexamethasone and prednisolone inserts have shown efficacy in inflammatory models with reduced systemic exposure compared to topical drops. This is particularly important given the risk of systemic corticosteroid side effects[95]. NSAID inserts containing bromfenac, ketorolac, or diclofenac provide prolonged anti-inflammatory effects for post-surgical patients[96]. Dual-phase inserts with PLGA microparticles in PVA matrices demonstrate biphasic release initial burst for rapid symptom relief followed by sustained release for continued inflammation control. Such profiles align well with post-operative inflammation patterns[97].
9.4 Dry Eye Disease
Dry eye disease affects millions globally, causing discomfort and visual disturbance. Treatment typically involves frequent artificial tear application. Sustained-release inserts can provide continuous lubrication and hydration[98].Hydroxypropyl cellulose inserts (Lacrisert®) have been commercially available for decades, slowly dissolving to supplement tear film. Modern developments include inserts incorporating cyclosporine or lifitegrast for immune-mediated dry eye, providing sustained immunomodulation[99].Hyaluronic acid-based inserts offer superior lubrication due to hyaluronan's water-retention properties and presence in natural tears. Mucoadhesive formulations prolong residence time, reducing the need for frequent reapplication [100].
10. Challenges and Future Perspectives
10.1 Current Challenges
Despite significant advances, several challenges limit widespread adoption of ocular inserts. Patient acceptance remains a concern some individuals find insert placement and removal uncomfortable or difficult. Design improvements focusing on flexibility, size reduction, and ease of handling can address these issues[101].Manufacturing scale-up from laboratory to commercial production presents challenges, particularly for advanced techniques like electrospinning and 3D printing. Ensuring batch-to-batch consistency, sterility, and quality control at large scale requires process optimization and validation[102].Stability during storage is critical for commercial viability. Some polymers and drugs degrade over time, particularly in humid conditions. Packaging in moisture-proof containers with desiccants and stability testing under ICH guidelines are necessary[103].Cost considerations affect accessibility. Advanced manufacturing techniques and specialized materials increase production costs compared to conventional eye drops. Health economic analyses demonstrating improved outcomes and reduced overall healthcare costs through better adherence may justify higher initial costs[104].
10.2 Emerging Technologies
Several emerging technologies promise to advance ocular insert capabilities. Stimuli-responsive systems that release drugs in response to specific triggers pH changes, temperature, enzymes, or biomarkers could enable on-demand therapy[105]. For example, inserts responding to inflammatory mediators could provide targeted treatment during disease flares. Microneedle-integrated inserts combine minimally invasive penetration with sustained release, potentially enabling posterior segment drug delivery from an anterior insert[106]. This approach could expand applications to conditions like diabetic retinopathy or age-related macular degeneration. Smart inserts incorporating sensors and electronics could monitor intraocular pressure, glucose levels, or other biomarkers while delivering therapy. Integration with smartphones would enable real-time monitoring and personalized dose adjustments[107]
CONCLUSION
Ocular inserts represent a significant advancement in ophthalmic drug delivery, addressing fundamental limitations of conventional eye drops through sustained release and prolonged retention. Two decades of research have produced sophisticated systems incorporating natural and synthetic polymers, nanotechnology, and advanced manufacturing techniques. Matrix, reservoir, and hybrid designs enable tailored release kinetics matching therapeutic needs. Manufacturing innovations including hot-melt extrusion, electrospinning, and 3D printing expand design possibilities while improving scalability. Nanotechnology integration enhances drug solubility, permeation, and controlled release. Comprehensive evaluation methodologies ensure quality and predict clinical performance. Therapeutic applications span glaucoma, infections, inflammation, and dry eye disease, with clinical evidence supporting efficacy and safety. Challenges remain in patient acceptance, manufacturing scale-up, and cost, but ongoing research addresses these barriers. Future directions point toward stimuli-responsive systems, personalized medicine, and smart inserts with monitoring capabilities. As the field matures, ocular inserts have strong potential to transform ophthalmic therapy, improving patient adherence, therapeutic outcomes, and quality of life for millions affected by eye diseases.
REFERENCES





Aleema Bano, Dr. Malti arya, Kaif Haroon, Nitesh Dubey, Rishabh Kumar Chandra, Ocular Inserts as Controlled Drug Delivery Systems: Design Principles, Mechanisms, and Evaluation, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3234-3249. https://doi.org/10.5281/zenodo.18713980
 10.5281/zenodo.18713980
10.5281/zenodo.18713980
