Sudhakarrao Naik Institute of Pharmacy, Pusad-445204 Dist.- Yavatmal, Maharashtra, India.
Ocular inserts are a modern solution to the limitations of traditional eye treatments like drops and ointments, offering improved drug delivery through controlled and sustained release. These devices enhance drug bioavailability, reduce the frequency of administration, and improve patient compliance. This review provides an overview of ocular inserts, covering their types, such as soluble, insoluble, and collagen-based forms, and the materials used to create them, including polymers and hydrogels. It also examines key design factors, like shape, size, and drug release mechanisms, that influence their effectiveness. The therapeutic applications of ocular inserts in treating conditions like glaucoma, dry eye, and uveitis are explored, along with the challenges, including patient comfort, drug delivery consistency, and application difficulties. Looking ahead, emerging technologies like nanotechnology, smart delivery systems, and 3D printing are set to drive significant advancements in this field. This review highlights how ongoing innovations in design, materials, and technology are shaping the future of ocular inserts, making them an essential tool for improving eye care.
Drug delivery to the eye has always been a challenging task for pharmaceutical scientists. The intraocular bioavailability of drugs administered through conventional eye drops is extremely low due to several factors, including nasolacrimal drainage, lacrimation, dilution by tear fluid, tear turnover, and conjunctival absorption [1]. Additionally, drug binding to proteins contributes to drug loss through precorneal parallel elimination pathways [2]. As a result, only a minimal amount (approximately 1-3%) of the drug penetrates the cornea and reaches intraocular tissues. [3] Efforts to enhance the contact time of ophthalmic drugs with the cornea have shown limited success. These strategies include incorporating viscosity-enhancing agents into eye drops or utilizing water-insoluble ointment bases in formulations, which aim to increase the drug’s retention time on the corneal surface [4]. However, such approaches provide only modest improvements in corneal contact and fail to ensure consistent drug availability, often necessitating frequent reapplication throughout the day. [5] This has driven the search for alternative ocular drug delivery systems. Recent advancements have focused on ocular inserts, which act as platforms for the controlled release of one or more active substances.[6] The development of these systems aims to combine controlled drug release with minimal irritation to the patient. Ocular inserts represent an innovative drug delivery system designed to release drugs at predetermined and predictable rates, thereby reducing the need for frequent administration. [7] Ophthalmic inserts are sterile preparations, often thin, multilayered, and impregnated with drugs. These devices, with solid or semisolid consistency, are specifically fabricated for placement in the cul-de-sac or conjunctival sac, ensuring prolonged ocular residence and sustained drug release [8]. They offer numerous advantages over conventional dosage forms, such as improved ocular retention, controlled and sustained drug delivery, accurate dosing, and reduced frequency of administration.[9]
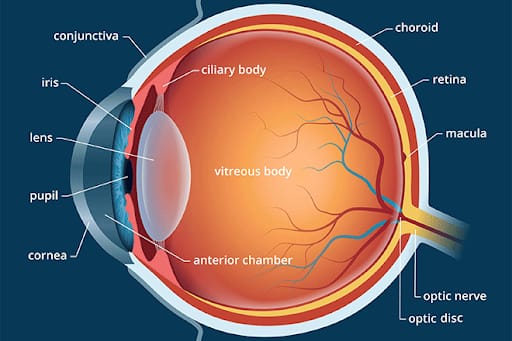
Fig.1
Human Eye
The human eye is a complex organ with amazing anatomical features. Because of corneal penetrability and tissue structure, drug administration to the eye is challenging. The protective function of the eyelids and lachrymal system causes the delivered medication to be quickly removed from the eye. [10] The material should be small and skin-compatible to prevent this.The eye is a sphere that is surrounded by a small front sphere and has a spherical component inside it [11]. To achieve a therapeutic drug concentration in the eye via local or systemic pathways, a number of ocular obstacles must be removed.The blood ocular barrier (BOB) regulates the composition and eye pressure of aqueous humor by controlling its inflow and outflow. The administration of ocular drugs is impeded by physiological and anatomical limitations. [12-15]
Physiological barriers
o Tear turn over
o Naso lachrymal drainage
o Blinking action of the eye
? Anatomical barriers, which include static and dynamic barriers, are responsible for restricting drugs into the anterior portion of the eye. Static barriers include
o Corneal epithelium
o Stroma
o Blood aqueous barrier (BAB)
? Dynamic barriers include
o Conjunctival blood
o Lymph flow
o Tear drainage [16]
Drug absorption in the eye
The majority of eye medications are given topically to the fornix. There are two ways that drugs can be absorbed from cul-de-sac: corneal and non-corneal. The cornea and aqueous fluid are where most medications are absorbed. The sclera and conjunctiva are included in non-corneal absorption; yet, this pathway restricts the amount of medication that can enter intraocular tissues. Both transcellular and paracellular routes allow drugs to enter the cornea.Lipophobic medications can pass through intercellular gaps via a process known as paracellular transit. A channel for lipophilic medications is part of the transcellular pathway. Both routes are penetrated by passive diffusion along the concentration gradient. [17]
Ocular Insert
Ocular inserts, commonly referred to as ocuserts, are innovative drug delivery systems designed to enhance the therapeutic efficacy of ocular medications. These small, sterile, and stratified solid devices are placed in the conjunctival sac, allowing for localized drug delivery. There are two primary types of ocular inserts: erodible and non-erodible. Erodible inserts are designed to dissolve over time, typically within 24 hours, which allows for the gradual release of the drug into the ocular environment. The rate of erosion is influenced by the type and concentration of polymers used in their formulation. In contrast, non-erodible inserts are constructed from either a matrix or reservoir system, which provides a sustained release of the drug over an extended period without the insert itself dissolving. The advantages of ocular inserts include increased residence time of the drug in the eye, improved bioavailability, and reduced dosing frequency, which can enhance patient compliance and therapeutic outcomes.[18,19]
Advantages of ocuserts
Various advantages of ocuserts are as follows -
2. Disadvantages of ocuserts
Various disadvantages of ocuserts are as follows -
Mechanism Of Ocuserts
A drug reservoir and a rate-controlling membrane made of different polymers make up the flat, flexible, solid, and semisolid Ocuserts device. The ocuserts, which release the medication at a preset rate constant, are placed in the eye's upper or lower cul-de-sac [23].
All types of ocuserts typically have three layers:
• A thin disc of drug complex serves as the central drug reservoir, where the drug is incorporated into a polymer to allow for drug diffusion.
• A rate-controlling membrane consists of two transparent discs of microporous membrane, usually made of ethylene vinyl acetate, a copolymer that permits controlled release of medication from the drug reservoir.
• An outer annual ring facilitates easy handling and correct insertion [23].
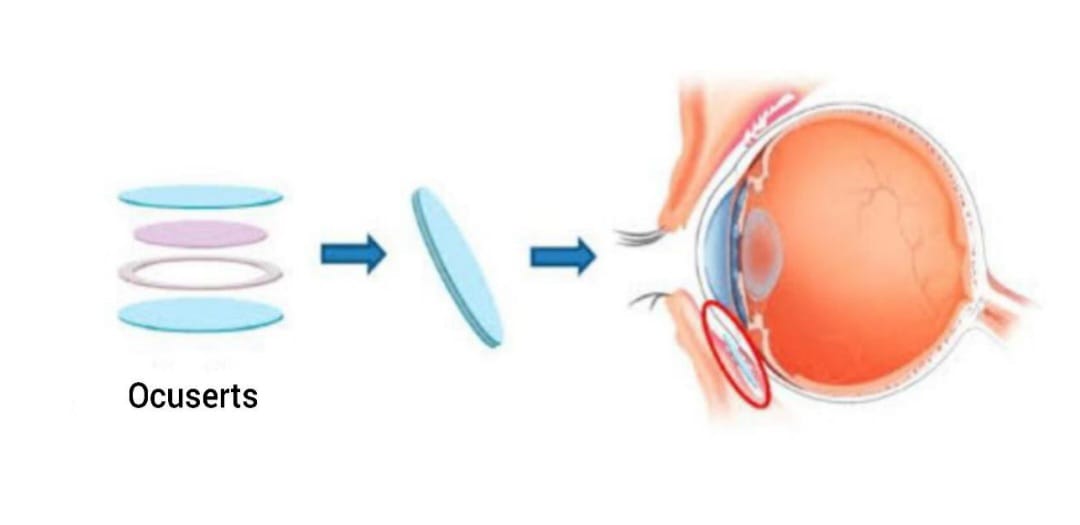
Fig.2
By allowing pharmaceuticals to diffuse from a reservoir through a rate-controlling membrane over a predetermined lifespan until the drug reservoir is empty, the Ocuserts system achieves zero order release. This uses a delicate sandwich technique that is insoluble. Tear fluid can enter the drug reservoir compartment and dissolve the drug from the complex because the reservoir is surrounded by microporous membranes that contain the drug complex. Patients can easily visualize the insert since it is surrounded by a retention ring made of the same material that has been treated with titanium dioxide [24].
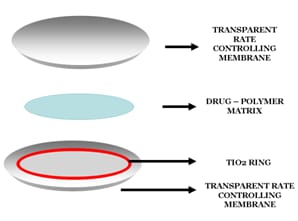
Fig .3
Controlled drug release of ocuserts is based on the following mechanisms:
1. Diffusion
2. Osmosis
3. Bio-erosion
In the diffusion process the medicine is released continually at a predetermined pace via the membrane into the tear fluid. If the insert is consisting of a solid non erodible body with pores and dispersed drug, the release of drug happens through the pores by diffusion. The slow disintegration of the solidly dispersed drug and, consequently, this matrix due to directed diffusion of aqueous solutions might further regulate controlled drug release. True dissolving in a soluble device mostly happens as a result of polymer swelling. The active component is uniformly distributed in a glassy polymer in swelling-controlled devices. In essence, there is no drug diffusion through the dry matrix of these glassy polymers. Water from the tear secretions starts to seep into the matrix when the ocular insert is placed in the eye, causing swelling, polymer chain relaxation, and drug diffusion. The swelling process, which is dependent on the polymer structure, is followed by the matrix's dissolution.
A transverse impermeable elastic membrane in the osmosis mechanism separates the insert's interior into a first compartment and a second compartment. The first compartment is surrounded by an impermeable elastic membrane and a semi-permeable membrane, while the second compartment is surrounded by an impermeable and elastic membrane. The insert's impermeable wall has a medication release hole. A solute that is unable to flow through the semi-permeable membrane is contained in the first compartment, while a medication that is in liquid or gel form is stored in the second compartment. Water diffuses into the first compartment when the insert is placed in the eye's aqueous environment, stretching and contracting the second compartment to force the drug through the drug release hole
The medicine is distributed within a matrix of biodegradable material that makes up the insert in the bio-erosion mechanism. When enter contact with tear fluid and gives results in controlled sustained release of the medication via bio-erosion of the matrix. Although the drug may be evenly distributed throughout the matrix, it is thought that a more controlled release occurs when the drug is only slightly concentrated in the matrix [25].
Materials Used in Ocular Inserts
The choice of material for an ocular insert is crucial as it directly influences:
* Drug release: The rate and extent of drug release depend on the polymer’s properties.
* Biocompatibility: The material must be well-tolerated by the ocular surface, causing minimal irritation or inflammation.
* Mechanical properties: The insert should have appropriate flexibility, strength, and resilience to withstand handling and insertion.
* Degradability: For erodible inserts, the material should degrade safely and predictably within the eye.
Commonly Used Materials:
* Hydrogels: These are hydrophilic polymers that absorb water and form a gel-like structure. They are biocompatible and offer good drug release control. Common examples include:
* HPMC (Hydroxypropyl methylcellulose): Used in Lacrisert, a commonly used insert for dry eye.
* PVA (Polyvinyl alcohol): A versatile polymer used in various ocular inserts, including SODI.
* Gellan gum: A natural polysaccharide with good biocompatibility and mucoadhesive properties.
* Biodegradable Polymers: These polymers are broken down by the body’s enzymes or other biological processes. They are preferred for erodible inserts to minimize the need for removal. Common examples include:
* PLGA (Poly(lactic-co-glycolic acid)): A widely used biodegradable polymer with tunable degradation rates.
* PLA (Polylactic acid): Another biodegradable polymer with good biocompatibility.
* PCL (Polycaprolactone): A slower-degrading polymer used for sustained release applications.
* Other Polymers:
* Silicone: Used in some contact lens-based inserts.
* Ethylene vinyl acetate (EVA): A thermoplastic polymer used in some non-erodible inserts.
Method Of Preparation of Ocuserts
The following methods are commonly used for formulation of ocuserts.
1. Solvent casting method
2. Glass substrate technique
3. Melt extrusion technique
1. Solvent Casting Method
In this method no. of batches are prepared using different proportion. The polymer is dissolved in suitable solvent. Into this solution plasticizer is added following continuous stirring the accurately weighed amount of drug is added to above solution and a uniform dispersion is obtained. When the proper blend is formed the solution is casted into the petridish using inverted funnel to allow slow and uniform evaporation at room temperature until the film is dried. The dried films thus obtained the film is cut into proper size and shape using cork borer. The ocuserts are prepared and stored in air tight container [26].
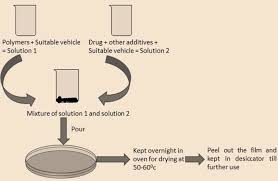
Fig.4
2.Glass Substrate Technique
In this method the polymer is soaked in 1%v/v Acetic acid solution for 24hrs, to get a clear solution. The solution is filtered. Required amount of drug is added and stirred for 15minutes to dissolve the complex in polymer solution. Plasticizer is added to the above solution. The viscous solution is obtained and kept aside for 30 minutes until air bubbles are removed. The rate controlling films are formed. The films are casted by discharging solution into the centre of leveled glass mould and allowing it to dry at room temperature for 24 hrs. The dried films are cut to form ocuserts in definite shape and size. Then, the matrix is sandwiched between the rate controlling membranes using gum which is non-toxic, non-irritating, and water insoluble. They are wrapped in aluminum foil separately and stored in a desiccators [14] .

Fig.5
3. Melt Extrusion Technique
Drug and the polymer are passed through sieve having mesh size of 60#, weighed andblended. In this mixture plasticizer is added. The blend is then discharged to the container of Melt flow rate apparatus and extruded. The extrudate was cut into appropriate size and packed in polyethylene lined Aluminium foil, heat sealed and sterilized by gamma radiation.[25]
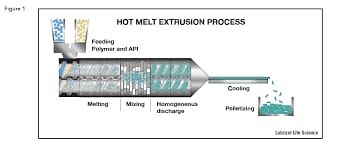
Fig.5
Evaluation Test for Ocuserts
1. Surface pH
2. Uniformity of thickness
3. Uniformity of weight
4. Swelling index
5. Folding endurance test
6. Drug content uniformity
7. In-vitro drug release study /In-vitro diffusion study
8. Percentage moisture absorption
9. Accelerated stability studies
10. Sterility studies
1.Surface pH
Ocuserts is placed in closed petridish in 1ml distilled water for 30min at room temperature. The swollen device was removed and placed under digital pH meter to determine the surface pH [10].
2. Uniformity Of Thickness
The thickness of ocuserts was determined using a Vernier caliper at five separated points of each device. For each formulation, five randomly selected ocuserts are tested for their thickness [15].
3. Uniformity Of Weight
From each batch, five ocuserts were taken out and weighed individually using digital balance. The mean weight of the ocuserts was noted [10].
4.Swelling Index
Small amount of film is cut and weighed initially, and then it is soaked in pH 7.4 tear fluid for 1hour. After 1hour, film is reweighed. [14] Swelling index is calculated by,
Swelling index = initial weight / final weight * 100
5. Folding Endurance Test
Folding endurance was determined by repeatedly fold the film at the same place till breaking or first sign of breaking. The number of fold occurred in film is its folding endurance till its breakage. The folding endurance of all the film is measured [10].
6. Drug Content Uniformity
To check the uniformity if drug in an ocuserts, each ocuserts was placed in a glass vials containing 10ml of artificial tear fluid. Then ocuserts was dissolved by aid of a magnetic stirrer, the solution was then filtered. 1ml from filtrate was withdrawn and diluted up to 10ml distilled water and absorbance was measured by using UV-Visible spectrophotometer [10]
7. In-Vitro Drug Release Study / In Vitro Diffusion Study
An in-vitro diffusion studies or in-vitro drug release study of ocuserts was done by using Franz diffusion cell. It is the instrument used to study the permeability study of drug. It consists of two compartments, one is donor compartment in which dosage form i.e., ocuserts is added and another is receptor compartment which is filled with 7.4 tear fluid to stimulate the tear fluid in the eye. A membrane, which might be an egg membrane or a permeable dialysis membrane, divides the two compartments. The instrument is turned on, and the temperature and RPM are changed. Tear fluid is put in the receptor compartment and occuserts in the donor compartment. After a predetermined amount of time (up to six hours) and after creating an appropriate dilution, 1 milliliter of the sample is removed. Using a UV spectrophotometer, the sample is examined. The drug release is computed once the sample is removed until a constant absorbance is not achieved. [14]

8. Percentage Moisture Absorption
This is carried out to check the physical stability and integrity at wet condition. The prepared ocuserts was accurately weighed and placed in desiccators containing 100ml of saturated solution of Aluminium chloride and it was kept for 3days. The ocuserts are taken out and reweighed after 3days [15]. The percentage of moisture absorbed by the ocuserts was calculated using the following formula: Percentage moisture absorption = Final weight – initial weight / initial weight* 100
9. Accelerated Stability Study
Stability studies done as per ICH guidelines, to ensure that the drug products retain their fitness for use until the end of their expiration date. Ocuserts are wrapped in aluminium foil stored in a glass bottle at 400c and 75% relative humidity (RH) in the stability chamber. The samples are tested for drug content after 0, 7, 15, 21 and 30 days respectively were evaluated for drug concentration, color, folding endurance etc [10].
10. Sterility Study
The test for sterility on the sterilized ocuserts was carried out by direct inoculation method.
* Culture media-
Alternate thioglycolate medium and soya bean digest casein medium was used as a culture medium for bacteria and fungi respectively. Media were prepared according to IP 2014 and taken into 20ml boiling test tube, properly plugged with cotton and sterilized by autoclaving at 1210c at 15ib/inch gauge pressure for 20 minutes.
* Inoculation and incubation-
Formulation was aseptically added in test tube containing respective media and simultaneously positive and negative control was prepared for each media. The inoculated media for bacteria and fungi were incubated t 300c-350c and 200c-250c respectively in incubator for not less than 14 days [25].
List Of Ocuserts of Different Ophthalmic Drugs Available in Market
The first marketed ocuserts is pilocarpine ocuserts by Alza Corporation, USA in 1973. It was the first relatively successful product for delivery of pilocarpine for the treatment of ocular hypertension. Pilocarpine ocuserts consists of a pilocarpine-alginate reservoir sandwiched between thin ethylene-vinyl acetate films. The devices are designed to deliver pilocarpine at either 20µg/hr. or 40µg/hr. It releases pilocarpine continuously at a steady rate for 7days [7]. The other drugs such as Ofloxacin, Norfloxacin, Moxifloxacin, Acyclovir, Timolol, and Aceclofenac as ocuserts are also available in the market. But these are not popular. In recent days, various researches are conducted in drug delivery through ocuserts [11].
|
Sr. No. |
Drug |
Category Of Drug |
|
1 |
Pilocarpine nitrate |
Mitotic agent |
|
2 |
Ciprofloxacin |
Antibacterial agent |
|
3 |
Ofloxacin |
Antibacterial agent |
|
4 |
Moxifloxacin |
Antibacterial agent |
|
5 |
Acyclovir |
Antiviral agent |
|
6 |
Fluconazole |
Antifungal agent |
|
7 |
Brimonidine tartrate |
Intra ocular pressure lowering agent |
|
8 |
Aceclofenac |
NSAID |
|
9 |
Levobunolol |
Betablocker agent |
|
10 |
Timolol maleate |
Anti-glaucoma agent |
CONCLUSION
Ocular inserts are a cutting-edge drug delivery method that provides distinct advantages over conventional approaches like eye drops and ointments. By ensuring sustained and controlled drug release, they enhance bioavailability, minimize the need for frequent dosing, and improve patient adherence. Different types of ocular inserts, including soluble, insoluble, and collagen-based forms, are tailored to treat a variety of eye conditions, such as glaucoma, dry eye, and uveitis. Innovations in materials, such as biocompatible polymers and hydrogels, have significantly enhanced the safety, comfort, and efficiency of these devices. Additionally, careful attention to design factors, including shape, size, and drug release mechanisms, ensures that these inserts function effectively and are user-friendly. However, certain challenges, such as patient acceptance, variability in drug delivery, and difficulties in application and retention, remain obstacles to widespread adoption. Emerging technologies like nanotechnology, 3D printing, and intelligent drug delivery systems offer exciting prospects for the evolution of ocular inserts. These advancements are expected to provide more targeted drug delivery, customized treatments, and improved therapeutic results. In summary, while challenges persist, ocular inserts hold immense potential for transforming ophthalmic care. Ongoing developments in materials, design, and technologies are paving the way for innovative solutions to address critical needs in eye health.
REFERENCES

Aniket Kadam*, Dr. Ravi Wanare, Rehan Beniwale, Akshay Jadhav, Sidharaj Solanke, Ram Gawande, Ocular Insert: Revolutionizing Drug Delivery System of Eye Care, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1678-1689 https://doi.org/10.5281/zenodo.15208753
 10.5281/zenodo.15208753
10.5281/zenodo.15208753
