Central India College of Pharmacy, Nagpur, Maharashtra, India
Non-alcoholic fatty liver disease (NAFLD) is a rapidly growing global health concern characterized by excessive hepatic fat accumulation in the absence of significant alcohol consumption. It represents a wide clinical spectrum ranging from simple steatosis to non-alcoholic steatohepatitis (NASH), fibrosis, cirrhosis, and hepatocellular carcinoma. The condition is strongly associated with obesity, insulin resistance, dyslipidemia, and metabolic syndrome, and has become the leading cause of chronic liver disease worldwide. Despite extensive research, no pharmacological therapy has yet received definitive regulatory approval, making lifestyle modification and nutritional strategies the foundation of management. Dietary interventions such as calorie restriction, the Mediterranean diet, low-fructose and low-carbohydrate patterns, and supplementation with omega-3 fatty acids and antioxidants have shown significant benefit in reducing hepatic fat, improving insulin sensitivity, and attenuating inflammation. Emerging therapies—including gut microbiota modulation, bioactive phytochemicals, and insulin-sensitizing nutraceuticals—offer additional promise in slowing disease progression. This review summarizes the current evidence-based nutritional strategies and critically evaluates the pipeline of emerging pharmacological agents, highlighting their mechanisms of action and potential to address the unmet therapeutic needs in NAFLD.
Non-alcoholic fatty liver disease (NAFLD) is a chronic metabolic liver disorder characterized by excessive triglyceride accumulation in hepatocytes in the absence of significant alcohol intake or other secondary causes of steatosis [1]. It is widely recognized as the hepatic manifestation of metabolic syndrome and is closely associated with central obesity, insulin resistance, dyslipidemia, and type 2 diabetes mellitus [2,3]. NAFLD encompasses a broad pathological spectrum ranging from simple hepatic steatosis to non-alcoholic steatohepatitis (NASH), progressive fibrosis, cirrhosis, and hepatocellular carcinoma (HCC) [4].
Globally, NAFLD affects nearly one-quarter of the adult population, with prevalence rates exceeding 50% in individuals with obesity or type 2 diabetes mellitus [5]. The increasing burden of NAFLD parallels modern lifestyle patterns characterized by high-calorie dietary intake, excessive consumption of processed foods, and reduced physical activity [6]. Consequently, NAFLD has become the leading cause of chronic liver disease worldwide and a major indication for liver transplantation in developed countries [7].
The pathogenesis of NAFLD is multifactorial, involving complex interactions among insulin resistance, lipotoxicity, oxidative stress, mitochondrial dysfunction, and gut–liver axis alterations [8,9]. Pro-inflammatory cytokines, adipokines, and microbial-derived metabolites further contribute to hepatocellular injury and fibrogenesis, promoting progression to advanced disease stages [10,11]. This review will first explore the etiological factors and pathophysiological mechanisms of NAFLD to provide context for a detailed analysis of current and investigational pharmacotherapies and nutraceutical interventions.
CAUSES AND RISK FACTORS
Non-alcoholic fatty liver disease (NAFLD) develops through a multifactorial interplay of genetic, metabolic, dietary, hormonal, and environmental factors that collectively promote hepatic fat accumulation, inflammation, and fibrosis. NAFLD leads to hepatic fat accumulation, which then contributes to two major pathways: insulin resistance (leading to inflammation) and oxidative stress (leading to fibrosis) as illustrated in the Figure 1.
Figure 1- NAFLD Disease Progression Chart
1. Genetic Susceptibility
Genetic variants strongly influence individual vulnerability to NAFLD. The PNPLA3 I148M polymorphism is the most robustly associated genetic determinant and increases hepatic triglyceride accumulation and fibrosis risk [1]. Variants in TM6SF2, MBOAT7, and GCKR also contribute to altered lipid handling, impaired very-low-density lipoprotein (VLDL) secretion, and dysregulated hepatic metabolism [2]. Ethnic differences in allele distribution partially explain variation in disease prevalence across populations.
2. Insulin Resistance and Metabolic Syndrome
Insulin resistance is considered the central pathophysiological driver of NAFLD. It promotes increased adipose tissue lipolysis, elevating circulating free fatty acids (FFAs) that accumulate in hepatocytes [3]. Hyperinsulinemia further enhances de novo lipogenesis through activation of sterol regulatory element-binding protein-1c (SREBP-1c) [4]. Accumulation of lipotoxic intermediates such as ceramides and diacylglycerols disrupts insulin signaling, promoting oxidative stress and inflammation [5].
3. Obesity and Visceral Adiposity
Central (visceral) obesity plays a key role in disease development. Visceral adipose tissue secretes pro-inflammatory cytokines including tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), while reducing the anti-inflammatory adipokine adiponectin, collectively promoting hepatic steatosis and fibrogenesis [6]. Even modest weight gain can increase hepatic fat content, whereas weight loss of 7–10% can reverse steatohepatitis and early fibrosis [7].
4. Dietary Patterns and Nutritional Factors
Diets rich in saturated fats, trans fats, and refined carbohydrates significantly increase NAFLD risk. Fructose, particularly from sugar-sweetened beverages, enhances hepatic lipogenesis by bypassing key glycolytic regulatory steps, increasing uric acid production, and worsening oxidative stress [8]. Conversely, dietary patterns such as the Mediterranean diet, rich in monounsaturated fats, polyphenols, legumes, and omega-3 fatty acids, demonstrate protective effects against steatosis and inflammation [9].
5. Gut Microbiota and Gut–Liver Axis
Dysbiosis contributes to NAFLD by increasing intestinal permeability and permitting translocation of microbial products such as lipopolysaccharide (LPS) into portal circulation. These endotoxins activate toll-like receptor-4 (TLR4) pathways in hepatocytes and Kupffer cells, promoting inflammation and fibrosis [10]. Reduced abundance of beneficial species such as Bifidobacterium and Faecalibacterium prausnitzii is frequently observed in NAFLD patients [11].
6. Sedentary Lifestyle
Physical inactivity reduces mitochondrial fatty acid oxidation and increases insulin resistance. Regular aerobic and resistance exercise improves hepatic fat content even without major weight loss, highlighting the independent role of exercise in NAFLD prevention and treatment [12].
7. Endocrine and Hormonal Disorders
Endocrine abnormalities—including hypothyroidism, polycystic ovary syndrome (PCOS), and hypogonadism—are established risk factors for NAFLD. Hypothyroidism impairs lipid clearance, while PCOS-associated hyperandrogenism exacerbates insulin resistance and hepatic fat accumulation [13]. Postmenopausal estrogen deficiency increases susceptibility to steatosis and fibrosis [14].
8. Medications and Environmental Exposures
Medications such as corticosteroids, tamoxifen, amiodarone, valproic acid, and some antiretroviral agents may induce or worsen hepatic steatosis [15]. Environmental toxins including bisphenol-A (BPA) and heavy metals contribute to metabolic disruption and oxidative stress, further promoting NAFLD development [16].
9. Genetics–Environment Interactions
Epigenetic modifications—including DNA methylation, histone changes, and microRNA dysregulation—mediate interactions between lifestyle factors and genetic susceptibility, influencing disease progression and therapeutic response [17].
COMPLICATIONS
Non-alcoholic fatty liver disease (NAFLD) is associated with a wide range of hepatic and extrahepatic complications. While many individuals remain in the simple steatosis stage, a substantial proportion progress to more severe conditions such as non-alcoholic steatohepatitis (NASH), fibrosis, cirrhosis, and hepatocellular carcinoma (HCC). In addition, NAFLD significantly increases the risk of cardiovascular, renal, endocrine, and malignant disorders.
1. Progression to NASH and Fibrosis
Approximately 15–20% of individuals with simple steatosis progress to NASH, which is characterized by hepatocellular ballooning, inflammation, and early fibrogenesis [1]. Among those with NASH, nearly 20–30% develop significant fibrosis over time [2].
Fibrogenesis is driven by activation of hepatic stellate cells (HSCs), stimulated by oxidative stress, lipotoxicity, and inflammatory cytokines such as transforming growth factor-β (TGF-β) [3].Advanced fibrosis is the strongest predictor of liver-related morbidity and mortality in NAFLD [4].
2. Cirrhosis
Persistent inflammation and progressive fibrosis can culminate in cirrhosis, characterized by architectural distortion, regenerative nodules, and portal hypertension [5]. Compensated cirrhosis may remain asymptomatic for years, but can later progress to decompensation manifested by ascites, variceal bleeding, hepatic encephalopathy, or jaundice [6].
3. Hepatocellular Carcinoma (HCC)
NAFLD is now one of the fastest-growing causes of HCC worldwide. Unlike viral hepatitis–related disease, HCC may develop even in non-cirrhotic NAFLD, likely related to chronic metabolic inflammation, oxidative DNA damage, and insulin resistance–mediated oncogenic pathways [7].NAFLD-related HCC has become a significant indication for liver transplantation in many regions [8].
4. Cardiovascular Disease (CVD)
Cardiovascular disease is the leading cause of death among individuals with NAFLD, surpassing liver-related mortality [9].NAFLD is associated with systemic inflammation, endothelial dysfunction, atherogenic dyslipidemia, and increased carotid intima–media thickness, all contributing to accelerated atherosclerosis [10].Consequently, NAFLD is considered an independent cardiovascular risk factor requiring aggressive management of metabolic comorbidities.
5. Chronic Kidney Disease (CKD)
Multiple studies indicate that NAFLD significantly increases the risk of CKD via shared mechanisms such as insulin resistance, systemic inflammation, oxidative stress, and altered adipokine signaling [11].Meta-analyses suggest that NAFLD patients have nearly 1.8-fold higher risk of developing CKD compared to the general population [12].
6. Endocrine and Metabolic Complications
NAFLD substantially increases the likelihood of developing type 2 diabetes mellitus (T2DM).Individuals with NAFLD have nearly double the risk of incident diabetes, and those with coexisting T2DM show faster fibrosis progression and higher cardiovascular mortality [13]. Additionally, endocrine disorders such as hypothyroidism, PCOS, and hypogonadism are associated with more severe steatosis and metabolic dysfunction [14].
7. Extrahepatic Malignancies
NAFLD is linked to increased incidence of several extrahepatic cancers, including colorectal, breast, pancreatic, and uterine malignancies [15]. Chronic low-grade inflammation, insulin resistance, and elevated insulin-like growth factors may contribute to this heightened oncogenic risk.
8. Psychological and Quality-of-Life Impairments
Patients with NAFLD frequently report reduced health-related quality of life, including fatigue, reduced physical functioning, anxiety, and depression [16].These symptoms correlate with obesity, insulin resistance, and advanced fibrosis.
9. Liver-Related Mortality
Advanced fibrosis and cirrhosis are the primary determinants of liver-related mortality in NAFLD. Long-term studies indicate that individuals with NASH-related cirrhosis face a 10–20% risk of liver-related death within ten years [17]. Non-invasive fibrosis scores such as FIB-4 and the NAFLD Fibrosis Score (NFS) are recommended for risk stratification and early identification of high-risk patients [18].
PATHOPHYSIOLOGY
The pathogenesis of non-alcoholic fatty liver disease (NAFLD) is multifactorial and involves a dynamic interplay of metabolic, inflammatory, hormonal, and environmental mechanisms. Although the “two-hit hypothesis” was historically used to describe disease progression, current understanding supports a multiple parallel-hit model, in which several dysregulated pathways occur simultaneously to drive hepatic steatosis, inflammation, and fibrosis [1]. Important Pathophysiological Processes in Non-Alcoholic Fatty Liver Disease are shown in Table 1
Table 1. Key Pathophysiological Mechanisms Involved in Non-Alcoholic Fatty Liver Disease
|
Mechanism |
Key Features |
Outcome |
|
Insulin Resistance |
↑ Adipose lipolysis, ↑ free fatty acids, ↑ de novo lipogenesis |
Hepatic triglyceride accumulation |
|
Lipotoxicity |
Ceramides, DAGs, toxic lipid intermediates |
Hepatocyte injury & metabolic dysfunction |
|
Oxidative Stress |
Excess ROS, mitochondrial overload |
Lipid peroxidation, inflammation |
|
ER Stress |
Unfolded protein response activation |
Hepatocyte apoptosis |
|
Inflammation |
Kupffer cell activation, cytokines (TNF-α, IL-6) |
Transition from steatosis → NASH |
|
Gut–Liver Axis Dysfunction |
Dysbiosis, ↑ intestinal permeability |
Endotoxin translocation, fibrogenesis |
|
Fibrogenesis |
Hepatic stellate cell activation, ↑ TGF-β |
Fibrosis → Cirrhosis |
1. Hepatic Lipid Accumulation
Excessive lipid accumulation within hepatocytes is the hallmark of NAFLD. Hepatic steatosis results from an imbalance between lipid acquisition and disposal, influenced by:
Insulin resistance upregulates SREBP-1c and ChREBP, key transcription factors that stimulate hepatic fatty acid synthesis [3]. High fructose intake further increases DNL by bypassing glycolytic control steps and generating lipogenic substrates [4].
2. Insulin Resistance and Metabolic Dysregulation
Insulin resistance is the central metabolic abnormality in NAFLD. In adipose tissue, impaired insulin signaling increases lipolysis, elevating FFAs that accumulate in hepatocytes. In the liver, selective hepatic insulin resistance occurs: insulin fails to suppress gluconeogenesis but continues to promote lipogenesis, worsening steatosis [5]. Lipotoxic intermediates such as ceramides and diacylglycerols (DAGs) activate protein kinase C (PKC) isoforms, disrupting insulin receptor signaling and promoting oxidative stress and inflammation [6].
3. Oxidative Stress and Mitochondrial Dysfunction
As lipid accumulation increases, mitochondrial β-oxidation pathways become overloaded, leading to excessive production of reactive oxygen species (ROS). ROS-mediated damage includes:
Lipid peroxidation products such as malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE) activate Kupffer cells and hepatic stellate cells, contributing to inflammation and fibrogenesis [8].
4. Endoplasmic Reticulum (ER) Stress and Apoptosis
Excess hepatic lipid induces ER stress by disrupting protein folding homeostasis.
Activation of the unfolded protein response (UPR) initially promotes adaptation but can trigger apoptosis when chronic, via:
ER stress is closely linked with mitochondrial dysfunction and oxidative stress, amplifying hepatocellular injury.
5. Inflammation and Immune Activation
Chronic inflammation is a key driver of progression from steatosis to NASH.
Inflammatory activation occurs through:
Activation of pathways such as NF-κB and NLRP3 inflammasome increases secretion of cytokines including TNF-α, IL-1β, and IL-6, promoting hepatocellular injury and recruiting immune cells [11].
6. Adipokine and Hormonal Imbalance
Adipose tissue dysfunction alters secretion of adipokines that regulate hepatic metabolism:
Adiponectin exerts protective effects by activating AMP-activated protein kinase (AMPK) and PPAR-α, enhancing lipid oxidation and reducing inflammation.
7. Gut–Liver Axis and Microbiota Dysregulation
Altered gut microbiota contributes to NAFLD through several mechanisms:
Dysbiosis reduces beneficial bacteria including Bifidobacterium and Faecalibacterium, while increasing pathogenic species that promote inflammation [14].
8. Fibrogenesis and Progression to Cirrhosis
Persistent hepatocellular injury activates hepatic stellate cells (HSCs), leading to extracellular matrix (ECM) deposition and fibrosis.
Key profibrogenic mediators include:
Accumulation of ECM causes architectural distortion, progressing to bridging fibrosis and eventually cirrhosis [16].
9. Reversibility and Emerging Molecular Targets
Early NAFLD is reversible through weight reduction, improved insulin sensitivity, and decreased oxidative stress.
Therapeutic targets under investigation include:
These approaches aim to reduce steatosis, enhance lipid oxidation, and prevent progression to fibrosis.
CURRENT AND INVESTIGATIONAL PHARMOTHERAPY
Although lifestyle modification remains the cornerstone of NAFLD management, several pharmacological agents have shown promising benefits in improving hepatic steatosis, inflammation, and fibrosis. However, no drug has yet received universal regulatory approval specifically for NAFLD or NASH. Current pharmacotherapies target underlying metabolic dysfunction, oxidative stress, inflammation, and fibrogenic pathways. An overview of the mechanisms underlying the current allopathic treatments for NAFLD as shown in Table 2.
Table 2. Overview of Current Allopathic Treatment Options for NAFLD and Their Mechanisms
|
Drug/ Class |
Mechanism |
Benefits |
Limitations |
|
Pioglitazone |
PPAR-γ agonist |
↓ Inflammation, improved histology |
Weight gain, edema |
|
Vitamin E |
Antioxidant |
↓ Steatosis, ↓ ballooning |
Not for diabetics; long-term risks |
|
Metformin |
Insulin sensitizer |
Improves metabolic status |
No histologic benefit |
|
GLP-1 RA (Liraglutide, Semaglutide) |
Weight loss, insulin sensitivity |
NASH resolution |
Cost, GI symptoms |
|
SGLT2 Inhibitors |
Glycosuria→weight loss |
↓ Liver fat, CV benefit |
Limited histologic data |
|
FXR Agonists (OCA) |
Bile acid signaling |
Fibrosis improvement |
Dose-limiting pruritus, atherogenic lipid profile. |
|
FGF21 Analogues |
Lipid oxidation, ↓ inflammation |
↓ Steatosis |
Under trials |
|
THR-β Agonists (Resmetirom) |
↑ Lipid oxidation |
↓ Liver fat |
Under evaluation |
1. Insulin Sensitizers
Pioglitazone
Pioglitazone, a PPAR-γ agonist, improves insulin sensitivity, increases adiponectin levels, and reduces hepatic steatosis and inflammation [1]. Clinical trials demonstrate histologic improvement in NASH, including reduction in hepatocellular ballooning and inflammation, with variable effects on fibrosis. Common limitations include weight gain, edema, and potential heart failure risk.
Metformin
Although metformin improves insulin resistance and glycemic control, it has not consistently demonstrated histologic improvement in NASH [2]. It may still be used in NAFLD patients with diabetes due to its metabolic benefits.
2. Antioxidants
Vitamin E (α-tocopherol)
Vitamin E is the best-studied antioxidant therapy for non-diabetic NASH. The PIVENS trial showed significant improvement in steatosis, inflammation, and ballooning with 800 IU/day vitamin E [3].Long-term concerns include risk of haemorrhagic stroke and prostate cancer at high doses.
3. GLP-1 Receptor Agonists
Glucagon-like peptide-1 (GLP-1) receptor agonists, including liraglutide and semaglutide, promote weight loss, reduce appetite, and improve insulin sensitivity.
These agents are especially beneficial in overweight or diabetic NAFLD patients.
4. SGLT2 Inhibitors
Sodium–glucose cotransporter-2 (SGLT2) inhibitors, such as empagliflozin, dapagliflozin, and canagliflozin, reduce hepatic fat by promoting glycosuria, lowering insulin levels, and improving β-oxidation.
Meta-analyses show reductions in:
They provide additional cardiovascular and renal benefits in diabetic NAFLD patients.
5. FXR Agonists
The farnesoid X receptor (FXR) regulates bile acid metabolism, glucose homeostasis, and inflammation.
Obeticholic Acid (OCA)
OCA improved fibrosis in the REGENERATE trial, but pruritus and adverse lipid changes limit its use [7].
Next-generation FXR agonists
Agents such as cilofexor and tropifexor are being evaluated with fewer side effects and improved tolerability [8].
6. Fibroblast Growth Factor (FGF) Analogues
FGF19 and FGF21 analogues improve insulin sensitivity, lipid oxidation, and hepatic inflammation.
These agents target mitochondrial dysfunction, inflammation, and lipid metabolism.
7. Thyroid Hormone Receptor-β (THR-β) Agonists
THR-β agonists selectively stimulate hepatic fatty acid oxidation.
Resmetirom (MGL-3196)
Resmetirom has shown:
It is one of the most promising emerging therapies in advanced trials.
8. PPAR Agonists
Lanifibranor (PPAR-α/δ/γ agonist)
Lanifibranor improves steatosis, inflammation, and fibrosis simultaneously. Phase III data show significant improvements in NASH resolution and fibrosis without major safety concerns [11].
Elafibranor (PPAR-α/δ agonist)
Shows anti-inflammatory and lipid-modulating effects, though phase III results were mixed.
9. Anti-Fibrotic and Immunomodulatory Agents
Several agents aim to directly target inflammation and fibrosis:
Fibrosis-targeting drugs remain a major unmet need.
10. Lipid-Lowering Therapies
Statins
Statins are safe in NAFLD and reduce cardiovascular morbidity. Though not primarily used for NASH, they may modestly reduce inflammation [13].
Omega-3 Fatty Acids
Doses of 2–4 g/day of EPA/DHA improve triglyceride levels and reduce hepatic fat in many patients [14].
Research in this area is rapidly expanding.
NUTRACEUTICAL AND DIETARY INTERVENTIONS IN NAFLD MANAGEMENT
Nutritional therapy is the cornerstone of NAFLD management because dietary intake directly influences hepatic fat accumulation, insulin sensitivity, oxidative stress, and inflammation. Evidence demonstrates that properly structured dietary strategies can significantly reduce hepatic steatosis and halt or reverse early-stage disease.The energy percentage composition of three diets—Normal, Western, and Mediterranean—in the context of Non-Alcoholic Fatty Liver Disease (NAFLD) visually breaks down the proportion of energy sources (like fats, carbohydrates, and proteins) in each diet to highlight their differing impacts on NAFLD as illustrated in Figure 2.
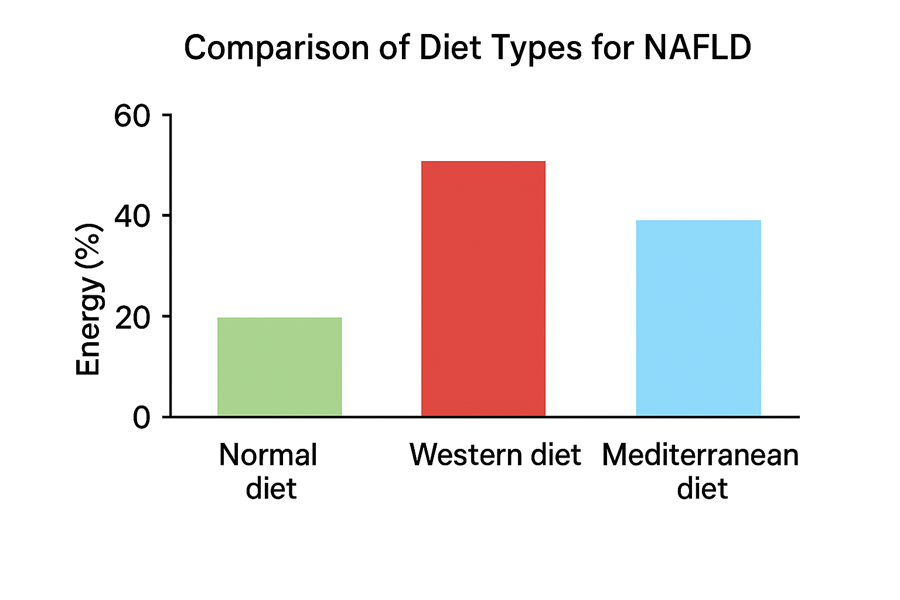
Figure 2- Comparison of Diet Types for NAFLD
1. Caloric Restriction and Weight Reduction
Sustained weight loss remains the most effective intervention for improving NAFLD.
However, rapid weight loss (>1.6 kg/week) should be avoided because it may exacerbate hepatic inflammation due to excessive mobilization of fatty acids [3].
2. Macronutrient Composition of Diet
2.1 Mediterranean Diet (MD)
The MD is considered the most effective dietary pattern for NAFLD, emphasizing:
Clinical studies consistently show:
These benefits occur even without significant weight loss.
2.2 Low-Carbohydrate and Low-Fructose Diets
Carbohydrate restriction lowers hepatic lipogenesis and improves insulin sensitivity.
Low-fructose diets show substantial reductions in liver fat even in adolescents and young adults.
2.3 Low-Fat and Plant-Based Diets
Diets rich in vegetables, whole grains, legumes, and fiber promote:
Plant-forward diets also improve gut microbiota composition, supporting metabolic and hepatic health.
2.4 Protein Sources
Moderate protein intake (1.0–1.2 g/kg/day) from lean and plant sources is recommended.
3. Micronutrients and Antioxidant Support
3.1 Vitamin D
Low vitamin D levels correlate with hepatic inflammation and fibrosis. Supplementation improves insulin resistance and liver enzymes in deficient individuals [10].
3.2 Vitamin E
Vitamin E is a potent antioxidant that reduces oxidative stress and improves histologic features in non-diabetic NASH patients [11].
3.3 Zinc and Selenium
These trace minerals support antioxidant enzyme systems such as glutathione peroxidase and superoxide dismutase. Deficiencies exacerbate oxidative stress and inflammation [12].
4. Gut Microbiota Modulation
Gut dysbiosis contributes to NAFLD through increased intestinal permeability, endotoxin translocation, and inflammation.
4.1 Probiotics
Strains such as Lactobacillus rhamnosus GG, Bifidobacterium breve, and Lactobacillus plantarum improve:
4.2 Prebiotics
Fibers like inulin, fructo-oligosaccharides, and resistant starch selectively enhance growth of beneficial microbiota, improving gut barrier function [14].
4.3 Synbiotics
Combined probiotic–prebiotic formulations show synergistic effects on liver fat, metabolic markers, and inflammation [15].
5. Nutraceutical Interventions
5.1 Curcumin
Curcumin suppresses NF-κB signaling and enhances antioxidant pathways.
Clinical trials show reductions in liver enzymes and hepatic steatosis [16].
5.2 Resveratrol
A SIRT1 activator that improves mitochondrial function and lipid oxidation.
Resveratrol supplementation reduces liver enzymes and improves steatosis markers [17].
5.3 Quercetin & Green Tea Catechins
Flavonoids with strong antioxidant properties that reduce inflammation and hepatic lipid accumulation [18].
5.4 Omega-3 Fatty Acids
EPA and DHA at doses of 2–4 g/day reduce hepatic triglycerides, inflammation, and serum lipids [19].
5.5 L-Carnitine
Facilitates mitochondrial transport of fatty acids; supplementation reduces hepatic fat and improves ALT levels [20].
5.6 N-Acetylcysteine (NAC)
A precursor to glutathione that enhances antioxidant capacity and reduces oxidative stress [21].
6. Functional Foods and Dietary Innovations
Functional foods enriched with antioxidants, omega-3s, probiotics, or polyphenols—such as fortified dairy products and plant-based beverages—can improve adherence and support metabolic health [22].
7. Physical Activity and Combined Lifestyle Therapy
Combining dietary intervention with at least 150 minutes/week of aerobic plus resistance exercise:
Exercise provides hepatic benefits independent of weight loss.
8. Emerging Nutrigenomic and Personalized Nutrition Approaches
Genetic polymorphisms such as PNPLA3, TM6SF2, and MBOAT7 influence individual responses to diet. Nutrigenomics aims to tailor dietary strategies based on genetic and metabolic profiles, microbiome composition, and metabolomics, representing the future direction of NAFLD nutritional therapy [24].
CONCLUSION
Non-alcoholic fatty liver disease (NAFLD) is a complex metabolic disorder driven by the interplay of genetic, environmental, hormonal, and lifestyle-related factors. Its progression from simple steatosis to non-alcoholic steatohepatitis, fibrosis, cirrhosis, and hepatocellular carcinoma highlights the importance of early detection and comprehensive management. Although no single pharmacological therapy has achieved universal approval for NAFLD or NASH, meaningful improvements can be achieved through sustained lifestyle modification.
Nutritional management remains the cornerstone of therapy, with strong evidence supporting the benefits of caloric restriction, gradual weight loss, the Mediterranean diet, and reduced intake of refined carbohydrates and fructose. Targeted supplementation with antioxidants, omega-3 fatty acids, and micronutrients further supports metabolic and hepatic health. Adjunctive therapies—including modulation of the gut–liver axis, use of nutraceuticals, and emerging pharmacological agents targeting metabolic and inflammatory pathways—provide additional therapeutic potential.
A multidisciplinary approach that integrates personalized nutrition, physical activity, behavioural counselling, and selected pharmacologic interventions offers the most effective strategy for improving liver-related outcomes and reducing long-term cardiometabolic risk. As research advances, individualized treatment informed by nutrigenomics, metabolic profiling, and microbiome analysis may become central to the future of NAFLD management.The future of NAFLD management lies in a personalized, multi-targeted approach. This will likely combine foundational lifestyle and dietary changes with a new generation of pharmacotherapies—including FXR agonists, THR-β agonists, and FGF analogues—alongside standardized, high-quality nutraceuticals that target complementary pathways such as oxidative stress and gut microbiota dysbiosis.
ACKNOWLEDGMENT
The authors express their sincere gratitude to Mrs. Rubeena Sheikh, Department of Pharmacology, for her invaluable guidance, constant encouragement, and insightful suggestions throughout the preparation of this review article. Her expert supervision greatly contributed to the clarity, depth, and quality of the manuscript.
The authors also extend their deep appreciation to Dr. Sayyed Sajjauddin Gulab, Principal, Central India College of Pharmacy, Nagpur, for his continuous support, academic motivation, and for providing an environment that fosters learning and research excellence. His leadership and commitment to academic growth have been a source of inspiration for the successful completion of this work.
REFERENCES






Abeera Khan, Mohammad Raza, Mohamid Ashraf, Pooja Gonde, Naveera Firdos, Rubeena Sheikh, Prerona Das, Sayyad Sajjauddin Gulab, Nutritional Management and Emerging Therapies in Non-Alcoholic Fatty Liver Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 106-119. https://doi.org/10.5281/zenodo.17777835
 10.5281/zenodo.17777835
10.5281/zenodo.17777835
