St. Wilfred’s Institute of Pharmacy, Panvel 410206
Non-alcoholic fatty liver disease (NAFLD) has emerged as the most common chronic liver disorder worldwide, affecting nearly one-fourth of the global population. It encompasses a spectrum ranging from simple steatosis to non-alcoholic steatohepatitis (NASH), progressive fibrosis, cirrhosis, and hepatocellular carcinoma (HCC). NAFLD is strongly linked with obesity, insulin resistance, type 2 diabetes mellitus, and dyslipidaemia, making it a hepatic manifestation of metabolic syndrome. The disease pathogenesis involves excessive hepatic lipid accumulation driven by increased fatty acid uptake, de novo lipogenesis, impaired fatty acid oxidation, and defective lipid export, ultimately leading to lipo-toxicity, oxidative stress, inflammation, and fibrosis. Diagnosis traditionally relies on liver biopsy, but non-invasive biomarkers and imaging modalities are increasingly employed. Lifestyle modification through diet and exercise remains the cornerstone of management, while pharmacological options such as pioglitazone and vitamin E are recommended in selected patients. Emerging therapies, including FXR agonists (obeticholic acid), PPAR ligands (elafibranor), and GLP-1 receptor agonists (liraglutide, semaglutide, resmetirom), hold promise for disease modification. Despite advances, no FDA-approved drug is yet available, highlighting the urgent need for effective therapies. This review summarises the molecular mechanisms, diagnostic strategies, current management, and future therapeutic perspectives in NAFLD.
ANATOMY, STRUCTURE, AND FUNCTION OF THE LIVER
The liver is the largest internal organ and gland in the human body, weighing approximately 1.4 to 1.8 kilograms in adults and accounting for about 2–3% of total body weight[1]. It is located in the right upper quadrant of the abdomen, beneath the diaphragm, and extends across the midline into the left hypochondrium[2]. The liver has a wedge-shaped structure, with a smooth convex diaphragmatic surface and a concave visceral surface that rests upon adjacent abdominal organs such as the stomach, duodenum, and right kidney. It is divided anatomically into four lobes—right, left, caudate, and quadrate—by the attachment of ligaments and fissures. The falciform ligament separates the right and left lobes on the anterior surface and contains the round ligament, a remnant of the foetal umbilical vein. The liver is attached to the diaphragm and anterior abdominal wall by peritoneal folds, including the falciform, coronary, and triangular ligaments. The inferior surface bears the porta hepatis, which serves as the hilum of the liver and allows passage of the hepatic artery, portal vein, and bile ducts[4].
Functionally, the liver is divided into eight segments according to the Couinaud classification, each with its own vascular inflow, outflow, and biliary drainage[3]. This segmental anatomy is based on the branching pattern of the portal vein and hepatic artery and is of great clinical importance in hepatic surgery and transplantation. The structural framework of the liver is enclosed in a thin connective tissue layer known as Glisson’s capsule, which extends into the parenchyma to form sheaths around the portal triads. The liver parenchyma is composed of hepatocytes—polygonal epithelial cells arranged in plates or cords radiating from a central vein. Between these plates lie hepatic sinusoids, specialised vascular channels lined by fenestrated endothelial cells and Kupffer cells that act as macrophages to remove pathogens and debris from the blood[5]. Blood from the hepatic artery and portal vein mixes in the sinusoids, allowing for metabolic exchange before draining into the central vein and subsequently into the hepatic veins, which empty into the inferior vena cava.
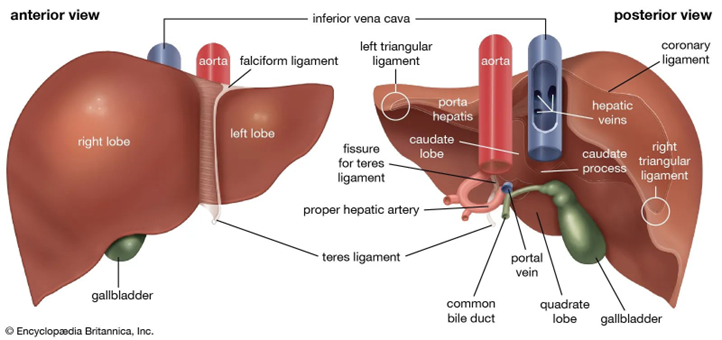
Fig. 1: Structure of Liver
Several models can describe the functional unit of the liver, the most clinically relevant being the hepatic acinus model, which divides the parenchyma into three zones based on proximity to the blood supply. Zone I (periportal) receives oxygen-rich blood and is active in oxidative metabolism and gluconeogenesis, while Zone III (pericentral) is more hypoxic and primarily involved in glycolysis, drug metabolism, and detoxification processes. This zonal organisation explains the varying susceptibility of hepatocytes to toxins and ischemic injury[6]. The space of Disse, located between the sinusoidal endothelium and hepatocytes, facilitates nutrient and waste exchange and contains hepatic stellate (Ito) cells that store vitamin A and contribute to fibrosis during chronic injury.
In addition to its vascular organisation, the liver possesses a complex biliary system that begins with bile canaliculi formed between adjacent hepatocytes. These canaliculi drain bile into the canals of Hering, then into intrahepatic bile ducts lined by cholangiocytes, which progressively unite to form the right and left hepatic ducts. These merge to form the common hepatic duct, which joins the cystic duct from the gallbladder to form the common bile duct that empties into the duodenum. The liver’s lymphatic system, consisting of superficial and deep networks, drains interstitial fluid toward hepatic and celiac lymph nodes and eventually into the thoracic duct.
FUNCTION OF LIVER
Functionally, the liver plays a central role in maintaining metabolic homeostasis. It is responsible for carbohydrate metabolism, including glycogen synthesis and gluconeogenesis, lipid metabolism, such as cholesterol and triglyceride synthesis, and protein metabolism involving the production of albumin, clotting factors, and transport proteins[7,8]. The liver also detoxifies endogenous and exogenous substances through enzymatic modification and conjugation, making them suitable for excretion via bile or urine. Furthermore, it serves as a major storage site for glycogen, vitamins (A, D, B12), and minerals (iron and copper)[9]. The bile produced by hepatocytes aids in emulsifying dietary fats and facilitates the absorption of fat-soluble vitamins in the intestine.
Overall, the liver’s intricate anatomy and microscopic structure are closely integrated with its diverse physiological functions. Its dual blood supply, segmental organisation, and specialised cellular architecture enable efficient processing of nutrients, detoxification of harmful substances, synthesis of vital biomolecules, and excretion of metabolic waste. Understanding this structure–function relationship is essential for comprehending both normal hepatic physiology and the mechanisms underlying liver diseases.
NON-ALCOHOLIC FATTY LIVER DISEASE (NAFLD)
Non-alcoholic fatty liver disease (NAFLD) is recognised as the liver disease epidemic of the 21st century, with a global prevalence ranging from 23–32% depending on geographical region[2,3]. In India and other developing nations, the rising incidence of obesity, sedentary lifestyles, and type 2 diabetes has contributed to a growing NAFLD burden[4]. The disease represents a broad clinicopathological spectrum, beginning with non-alcoholic fatty liver (NAFL), characterised by simple hepatic steatosis without significant inflammation, and progressing to non-alcoholic steatohepatitis (NASH), in which steatosis is accompanied by hepatocyte ballooning, inflammation, and variable fibrosis. Over time, these changes can progress to cirrhosis, hepatocellular carcinoma (HCC), and end-stage liver disease, making NAFLD a leading cause of liver transplantation[1].

Fig. 2: Healthy Liver vs Fatty Liver
Unlike viral hepatitis, NAFLD is tightly interlinked with metabolic syndrome, with insulin resistance playing a central role in its pathogenesis[7]. Current evidence highlights the imbalance between lipid acquisition and disposal in the liver as a fundamental mechanism. Increased lipid uptake via fatty acid transporters, enhanced de novo lipogenesis driven by transcription factors such as SREBP1c, impaired mitochondrial fatty acid oxidation, and reduced very low-density lipoprotein (VLDL) export collectively contribute to hepatic lipid accumulation[5,6]. These changes trigger lipotoxic oxidative stress and pro-inflammatory signalling, promoting hepatocyte injury and fibrosis[8].
Clinically, NAFLD is often silent, and many patients remain undiagnosed until advanced stages. While liver biopsy remains the gold standard for diagnosing NASH and staging fibrosis, non-invasive methods such as elastography and serum fibrosis scores are increasingly applied in clinical practice. Importantly, fibrosis stage rather than steatosis per se is the strongest predictor of long-term outcomes. Currently, there are no FDA-approved pharmacological agents for NAFLD[9]. Lifestyle modification with dietary intervention, weight reduction, and regular physical activity remains the cornerstone of therapy. Pioglitazone and vitamin E are considered in selected patients with biopsy-proven NASH, while emerging therapies such as farnesoid X receptor (FXR) agonists, peroxisome proliferator-activated receptor (PPAR) ligands, and glucagon-like peptide-1 (GLP-1) receptor agonists show promise in clinical trials[10,11].
This review aims to provide a comprehensive overview of the molecular mechanisms underlying NAFLD, current diagnostic approaches, therapeutic strategies, and future directions in disease management.
PATHOPHYSIOLOGY OF NAFLD
The pathogenesis of non-alcoholic fatty liver disease (NAFLD) is multifactorial, involving a complex interplay between genetic, metabolic, and environmental factors. Central to the disease process is an imbalance between hepatic lipid acquisition and disposal, leading to intrahepatic lipid accumulation and subsequent lipotoxic injury[1].
1. Substrate Overload and Lipotoxicity
The “substrate overload lipotoxic injury (SOLLI) model” explains NAFLD pathogenesis as a result of excessive delivery of glucose, fructose, and fatty acids to the liver[2].
While triglyceride accumulation (steatosis) may initially serve as a protective mechanism, the diversion of fatty acids into toxic lipid species such as diacylglycerols, ceramides, and lysophosphatidylcholines triggers endoplasmic reticulum (ER) stress, mitochondrial dysfunction, oxidative stress, and hepatocyte apoptosis[3].
These processes activate Kupffer cells and hepatic stellate cells, resulting in inflammation and fibrogenesis.
2. Molecular Mechanisms of Hepatic Lipid Accumulation
Hepatic steatosis develops when lipid acquisition exceeds disposal. Four main pathways are implicated:
(a) Increased fatty acid uptake:
Mediated by CD36, fatty acid transport proteins (FATP2, FATP5), and caveolins. Overexpression of these transporters in NAFLD enhances hepatic lipid influx[4].
(b) Enhanced de novo lipogenesis (DNL):
Excess carbohydrates are converted into fatty acids through insulin- and carbohydrate-mediated transcription factors.
SREBP1c (stimulated by insulin) and ChREBP (stimulated by glucose/fructose) upregulate lipogenic enzymes such as acetyl-CoA carboxylase (ACC) and fatty acid synthase (FASN).
In NAFLD, selective insulin resistance preserves the lipogenic action of insulin, sustaining high rates of DNL even during fasting[4].
(c) Impaired fatty acid oxidation:
Normally regulated by PPARα, mitochondrial β-oxidation is insufficient in NAFLD[5,6].
Lipid overload shifts oxidation to peroxisomes and cytochrome P450 isoforms, generating excessive reactive oxygen species (ROS). ROS amplify hepatocyte injury, inflammation, and fibrogenesis[5].
(d) Defective lipid export:
The liver exports triglycerides as very-low-density lipoprotein (VLDL) particles.
In NAFLD, microsomal triglyceride transfer protein (MTTP) and ApoB100 activity are impaired, limiting VLDL secretion and worsening lipid retention.
3. Genetic and Epigenetic Factors
Variants in PNPLA3 (I148M) and TM6SF2 (E167K) are strongly associated with increased risk of steatosis, NASH, and fibrosis progression.
Epigenetic changes (DNA methylation, microRNAs) also influence lipid metabolism and inflammatory signalling[6,7].
4. Gut-Liver Axis
Altered gut microbiota, increased intestinal permeability, and translocation of bacterial endotoxins promote systemic inflammation and hepatic injury. Short-chain fatty acids and bile acid metabolism also modulate NAFLD progression via FXR and TGR5 signalling[8].
5. Inflammation and Fibrosis
Damaged hepatocytes release danger signals (DAMPs), activating Kupffer cells. Activated hepatic stellate cells (HSCs) produce extracellular matrix proteins, leading to fibrosis[9,10]. The fibrosis stage has been identified as the strongest predictor of long-term outcomes, surpassing steatosis severity[11,12].
DIAGNOSIS OF NAFLD
Diagnosis of non-alcoholic fatty liver disease (NAFLD) involves determining (1) the presence of hepatic steatosis, (2) whether inflammation/ ballooning is present (i.e. NASH), and (3) the fibrosis stage[1]. Because liver biopsy is invasive and not always practical, the focus is shifting toward non-invasive biomarkers and imaging methods.
1. Liver Biopsy (Gold Standard)[2]
2. Serum / Circulating Biomarkers & Diagnostic Panels [3,4]
Routine Clinical Biochemistry
Novel Biomarkers / Omics / Molecular Markers
3. Non-Invasive Imaging and Elastography[5,6]
Imaging plays a central role in diagnosing and quantifying hepatic fat content, inflammation, and fibrosis.
Conventional Imaging Modalities
Elastography & Quantitative Imaging
4. Hybrid / Combined Approaches[7,8]
CURRENT MANAGEMENT / THERAPEUTIC APPROACHES IN NAFLD
Because there is no single approved “magic bullet” treatment for NAFLD/NASH, current management comprises a combination of lifestyle interventions, off-label pharmacotherapies, surgical approaches in selected cases, and investigational/emerging therapies.
1. Lifestyle Modification (Foundational Therapy)
Lifestyle changes remain the backbone of NAFLD management according to most guidelines and reviews[1].
a. Weight Loss
b. Dietary Interventions
c. Physical Activity / Exercise
d. Behavioural Support & Long-Term Adherence
The absence of a pharmacologic remedy underscores why lifestyle remains first-line, and many trials use weight loss as a comparator or adjunct.
RECENT ADVANCES & EMERGING THERAPIES IN NAFLD
In the last decade, there has been significant progress in the development of pharmacological agents targeting various pathogenic mechanisms of NAFLD/NASH. Although no drug has yet received full FDA approval for NAFLD, several agents in phase 2 and phase 3 clinical trials have shown promising results.
1. Thyroid Hormone Receptor-β (THR-β) Agonists
2. FXR (Farnesoid X Receptor) Agonists
3. PPAR (Peroxisome Proliferator-Activated Receptor) Agonists
4. GLP-1 Receptor Agonists & Incretin-Based Therapies
5. FGF (Fibroblast Growth Factor) Analogues
6. Anti-Fibrotic and Anti-Inflammatory Agents
7. Combination Therapies
Table. 1: Drugs and their mechanism and trial data
|
Drug/Class |
Target Mechanism |
Trial Outcomes |
Current Status |
|
Resmetirom (THR-β agonist) |
↑ Lipid metabolism, ↓ steatosis |
Reduced liver fat, improved fibrosis (MAESTRO-NASH) |
Phase 3 (FDA Fast Track) |
|
Obeticholic Acid (FXR agonist) |
Modulates bile acid, anti-fibrotic |
Fibrosis improvement, pruritus side effect (REGENERATE) |
Phase 3 |
|
Lanifibranor (pan-PPAR) |
Improves insulin sensitivity, ↓ inflammation |
Improved NASH histology (NATIVE trial) |
Phase 2 |
|
Semaglutide (GLP-1 RA) |
Weight loss, insulin sensitization |
NASH resolution, improved histology |
Phase 2/3 |
|
Tirzepatide (GLP-1/GIP dual) |
Incretin pathway modulation |
Significant weight loss, liver fat reduction |
Phase 3 |
|
Efruxifermin (FGF21 analogue) |
Fat oxidation, insulin sensitization |
Fibrosis regression in trials |
Phase 2 |
|
Belapectin (Galectin-3 inhibitor) |
Anti-fibrotic, prevents varices |
Mixed results, ongoing studies |
Phase 2 |
|
Cenicriviroc (CCR2/CCR5 antagonist) |
Blocks inflammatory signalling |
Limited benefit in fibrosis |
Development paused |
CHALLENGES AND LIMITATIONS IN NAFLD MANAGEMENT
Despite remarkable advances in understanding the molecular basis of NAFLD and numerous clinical trials, the translation into effective therapies has been slow. Several key challenges contribute to this gap:
1. Absence of FDA-Approved Drugs
2. Disease Heterogeneity
3. Diagnostic Limitations
4. Slow Disease Progression
5. Adherence to Lifestyle Interventions
6. Safety Concerns of Emerging Therapies
7. Comorbidities and Extrahepatic Outcomes
8. Economic and Healthcare Burden
FUTURE PERSPECTIVES IN NAFLD MANAGEMENT
With the global prevalence of NAFLD increasing and no approved pharmacotherapy yet available, research is shifting toward novel strategies and precision medicine. Future management will likely combine lifestyle, pharmacological, and technological interventions tailored to individual patient profiles.
1. Personalized and Precision Medicine
2. Gut–Liver Axis Modulation
3. Nanomedicine and Targeted Drug Delivery
4. Combination Therapies
5. Digital Health and Lifestyle Support
6. Early Detection and Preventive Strategies
MARKETED PREPARATION FOR NAFLD
Here are some of the marketed or recently approved preparations for non-alcoholic fatty liver disease (NAFLD) / non-alcoholic steatohepatitis (NASH), along with mechanism, status, and limitations. Note that many treatments are off-label or approved only in certain countries; always check local regulatory status.
Resmetirom (brand name Rezdiffra) is one of the newest agents approved by the U.S. FDA (in March 2024) for treatment of noncirrhotic NASH (now also called metabolic dysfunction-associated steatohepatitis, or MASH) with moderate to advanced fibrosis (F2–F3). It is a thyroid hormone receptor-β agonist, which acts by increasing hepatic fat oxidation and reducing inflammation and fibrosis.
In India, saroglitazar (dual PPAR α / γ agonist) has been approved by the Drug Controller General of India (DCGI) for the treatment of NAFLD/NASH in non-cirrhotic patients. Saroglitazar improves lipid parameters (via PPAR-α) and insulin sensitivity (via PPAR-γ), thereby impacting steatosis, inflammation, and metabolic comorbidities.
Very recently, in India, nor-ursodeoxycholic acid (NorUDCA) 500 mg tablets have also been approved by CDSCO for the treatment of NAFLD. NorUDCA is claimed to have choleretic and anti-inflammatory properties, enhancing bile flow, reducing hepatic inflammation and potentially slowing disease progression.
Besides these, other pharmacologic agents are often used off-label or in clinical trials. For example, vitamin E and pioglitazone have been used in selected non-diabetic NASH patients for inflammation improvement, though effects on fibrosis are less consistent.
CONCLUSION
Non-alcoholic fatty liver disease (NAFLD) has emerged as the most common chronic liver disorder worldwide, closely linked with obesity, type 2 diabetes, and metabolic syndrome[1]. Its spectrum, ranging from simple steatosis to cirrhosis and hepatocellular carcinoma, underscores the importance of early recognition and intervention. Advances in understanding disease pathogenesis highlight the central roles of lipotoxicity, insulin resistance, inflammation, and fibrogenesis, with genetic and gut microbiota factors further modulating disease progression[2,3].
Diagnosis has shifted from invasive liver biopsy toward non-invasive biomarkers and imaging modalities, although limitations remain in identifying patients with “at-risk NASH”[4]. Lifestyle modification remains the cornerstone of therapy, but long-term adherence is a major challenge. Pharmacological therapies such as pioglitazone, vitamin E, and GLP-1 receptor agonists show promise, while newer agents resmetirom, obeticholic acid, lanifibranor, and FGF analogues are advancing through late-stage clinical trials[5,6].
Despite these developments, the absence of FDA-approved therapies, patient heterogeneity, and safety concerns remain major hurdles[7]. The future of NAFLD management will likely rely on precision medicine approaches, gut–liver axis modulation, nanotechnology-based drug delivery, and rational combination therapies[8,9,10]. Furthermore, integration of digital health solutions and population-level preventive strategies will be essential to curb the rising global burden.
In conclusion, NAFLD represents both a clinical challenge and an opportunity for innovative research. Continued multidisciplinary collaboration between clinicians, researchers, and policymakers is crucial to translate scientific advances into effective, accessible therapies that improve long-term patient outcomes[11,12].
REFERENCES


Amit Namde, Amey Dhuri, Nutan Gaikwad, Rini Punathil, Dr. Kamlesh Soni, Non-Alcoholic Fatty Liver Disease: Pathophysiology, Diagnosis, and Emerging Therapies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 863-875. https://doi.org/10.5281/zenodo.17313048
 10.5281/zenodo.17313048
10.5281/zenodo.17313048
