School of Pharmacy and Research People’s University, Bhopal (M.P.) 462037, India
Osteoporosis is a progressive bone disorder characterized by decreased bone mineral density (BMD) and increased fracture risk, particularly in postmenopausal women. The disease is primarily driven by an imbalance in bone remodeling, where osteoclast-mediated resorption exceeds osteoblast-mediated formation. Current treatment strategies include pharmacological and non-pharmacological approaches; however, challenges such as poor bioavailability, systemic side effects, and limited patient adherence hinder therapeutic efficacy. Raloxifene hydrochloride (R-HCl), a selective estrogen receptor modulator (SERM), has demonstrated efficacy in osteoporosis management, yet its clinical potential is limited by low solubility and first-pass metabolism. Novel drug delivery approaches, including nanostructured lipid carriers (NLCs) and sublingual formulations, offer promising solutions to enhance drug bioavailability and therapeutic outcomes. This review explores the pathophysiology of osteoporosis, current treatment challenges, and the advancements in nanocarrier-based drug delivery systems. The potential of combining R-HCl with vitamin D and the role of NLCs in improving drug permeability and retention are discussed. Future research directions emphasize optimizing these technologies for superior osteoporosis management.
Osteoporosis is a medical condition marked by reduced bone mineral density (BMD) and deterioration of bone microarchitecture, leading to an elevated risk of fractures. In the United States, it affects approximately 10.3% of adults aged 50 and above. [1] The likelihood of developing osteoporosis increases with age, with prevalence rates climbing to 46.3% among men and 77.1% among women over the age of 80. Women are more commonly affected than men, primarily due to hormonal fluctuations, especially after menopause, along with various lifestyle factors that contribute to bone loss in older age groups. [2]
Bone Remodeling
Bone remodeling is a lifelong process maintaining bone mass, quality, and mineral balance by releasing calcium and phosphorus. About 10% of the skeleton renews annually, involving coordinated bone resorption by osteoclasts and synthesis by osteoblasts. [3]
Classification of Osteoporosis
Osteoporosis can be categorized into two primary groups based on the factors that influence bone metabolism: primary osteoporosis and secondary osteoporosis.
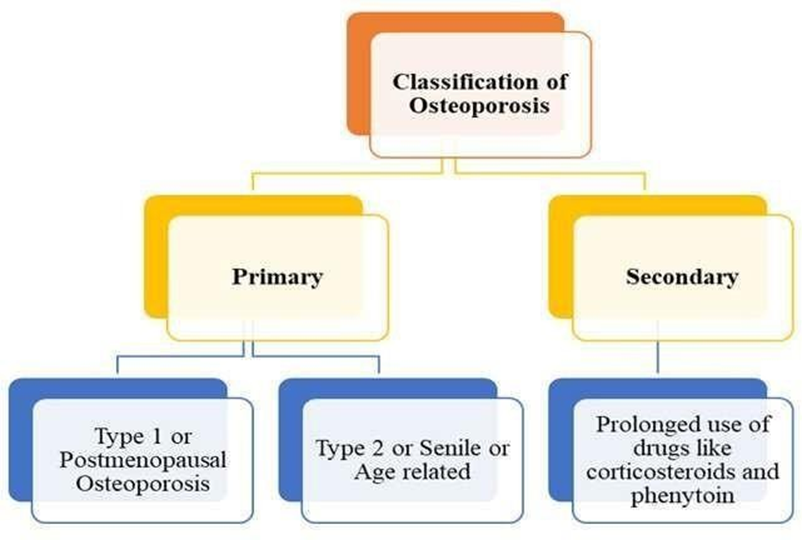
Figure 1: Classification of Osteoporosis
Pathophysiology
Bone is a dynamic tissue that continuously undergoes production and resorption to prevent microfractures, respond to mechanical demands, and maintain calcium balance. [4] This process, known as bone remodeling, involves five stages and relies on osteoclasts and osteoblasts. Osteoclasts handle bone resorption, while osteoblasts facilitate new bone formation. Osteoporosis arises when an imbalance favors resorption over formation, leading to bone fragility. In the activation phase, osteoclasts create an acidic environment to dissolve bone minerals. [5] During reversal, osteoclasts undergo apoptosis, and osteoblasts deposit collagen, which mineralizes into new bone. Osteoclast development requires RANKL and M-CSF, with RANKL binding to RANK on osteoclasts to stimulate resorption. Estrogen deficiency during menopause increases osteoclast activity without matching osteoblast function, causing bone loss—a process termed "decoupling." Osteoprotegerin (OPG) acts as a natural RANKL inhibitor, but reduced OPG in premature menopause elevates RANKL levels, accelerating bone resorption and loss. [6]
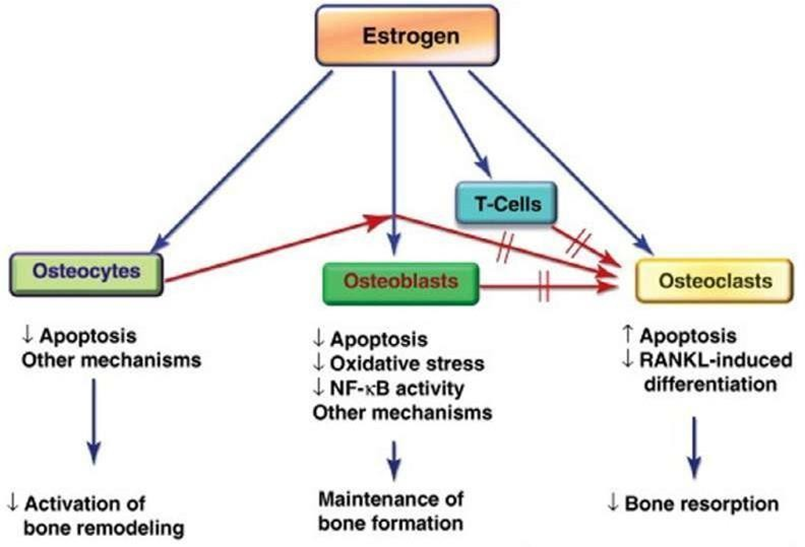
Figure 2: The estrogen regulation of bone turnover via effects on osteocytes, osteoblasts, osteoclasts, and T-cells
Diagnosis
Bone Mineral Density (BMD) testing is vital for diagnosing osteoporosis, especially in women with estrogen deficiency, vertebral abnormalities, or on long-term glucocorticoid therapy. [7] Central dual-energy X-ray absorptiometry (DXA) of the hip and spine is the gold standard due to its accuracy and low radiation. Peripheral devices are portable but less reliable. T-scores assess BMD, with -2.5 or lower indicating osteoporosis; fractures at this level indicate severe osteoporosis. Screening can employ peripheral bone mineral density (BMD) devices, but a definitive diagnosis requires central dual-energy X-ray absorptiometry (DXA). T- and Z-scores measure bone mineral density (BMD) (Cosman et al., 2014). The T-score shows the difference between a person's bone mineral density (BMD) and that of a normal adult of the same gender and age. Number of standard deviations below average. The Z-score compares an individual's bone mineral density (BMD) to the average BMD of people in their age and sex group. [8]
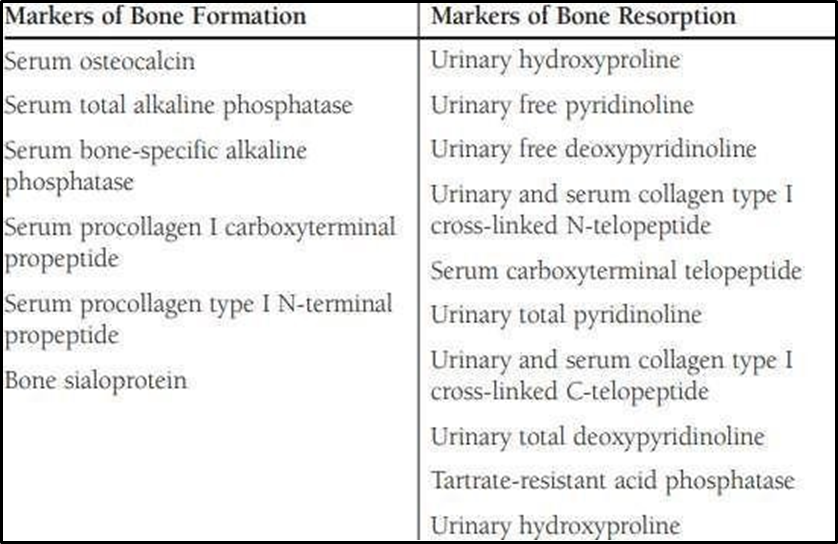
Table 1: Markers for bone formation and bone resorption in serum and urine
Treatment Strategies
For osteoporosis Non-pharmacological and pharmacological interventions are recommended, depending on fracture risk assessment.
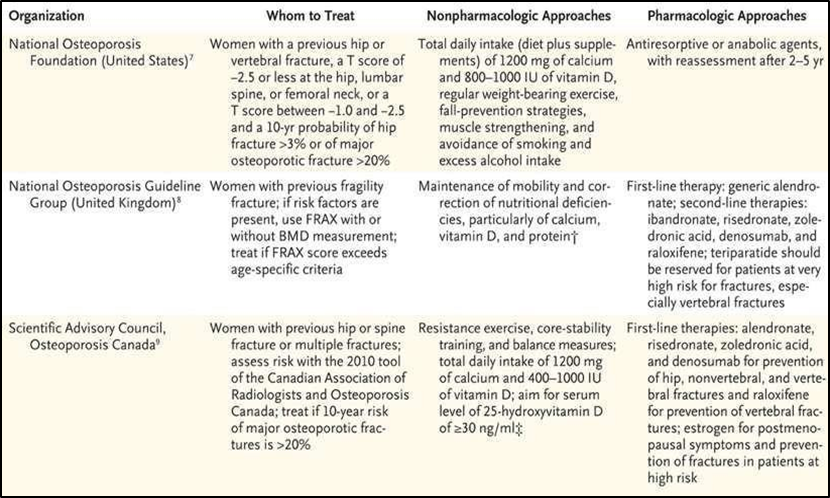
Figure 3: Guidelines for treatment of osteoporosis
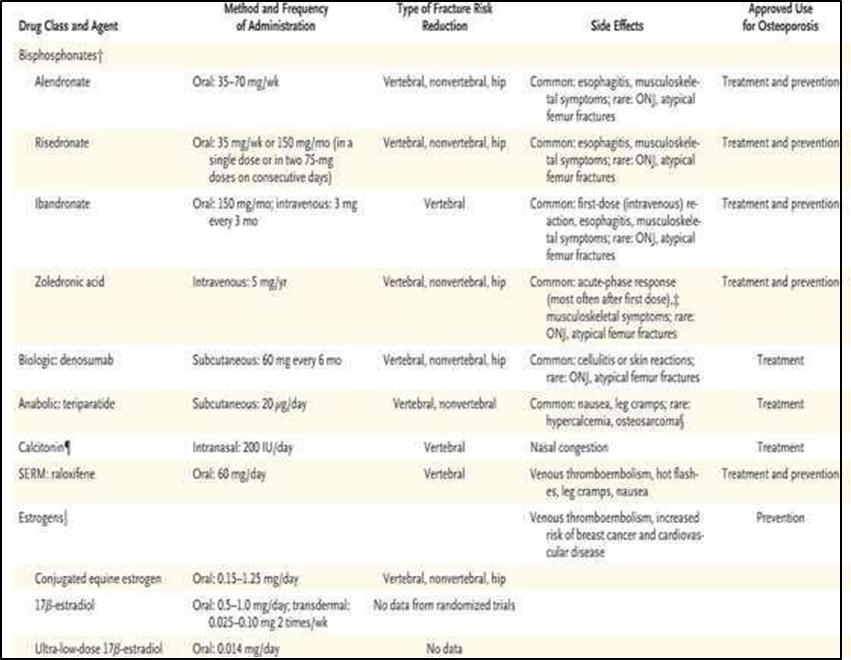
Figure 4: FDA approved drugs for PMO
Challenges with Current Treatment
Oestrogen replacement therapy (ERT) is usually the first treatment for osteoporosis in postmenopausal women since a shortage of oestrogen is thought to cause bone loss. The ERT has a lot of complications, such as endometrial cancer, breast cancer which are the main side effects along with them the patient can experience other complications like hypertension, thromboembolic disease, etc. [9] R- HCl did not cause breast or vaginal bleeding. R- HCl also reduced breast cancer risk. The 3-year treatment reduced breast cancer risk by 76%. However, R-HCl treatment increased hot flushes and venous thromboembolism in women. [10] Androgen therapy is more effective at treating osteoporosis than oestrogen monotherapy. In moderate to severe acne, clinical hirsutism, androgenic alopecia, pregnancy, breastfeeding, and probable androgen-dependent neoplasia, testosterone therapy is not indicated. Bisphosphonates may cause jaw osteonecrosis and unusual subtrochanteric femoral fractures.[11] Calcitonin is only used to treat acute pain after a recent osteoporotic fracture. Calitonin does not work for persistent pain lasting more than three months. This drug can cause nausea, vomiting, flushing, allergic reactions, hypocalcemia, nasal symptoms, calcitonin antibodies, and prostate cancer.
Strategies for addressing obstacles:
Alternative osteoporosis treatment includes transdermal oestrogen (0.05-0.10 mg/day) and progestin (in women with uteruses). Transdermal oestrogen may have similar side effects to oral conjugated oestrogen. USFDA-approved ultra-low oestrogen (0.014 mg/day) to prevents osteoporosis. The dosage was approved after it was shown to prevent bone mineral density (BMD) loss in postmenopausal women without causing uterine hyperplasia. In postmenopausal women, bazedoxifene, another selective oestrogen receptor modulator, and conjugated oestrogen diminish hot flashes and preserve bone mineral density. Hot flash and osteoporosis prevention medicine is FDA-approved. The American Association of Clinical Endocrinologists (AACE) recommends periodic hip and lumbosacral bone mineral density (BMD) assessments to assess osteoporosis treatment response, including bisphosphonates. After starting bisphosphonate therapy, this examination should be done every 1-2 years until BMD stabilizes, then every two years or fewer. [12]
R-HCl for the Treatment of PMO
Evista (R-HCl) is the only selective oestrogen receptor modulator (SERM) approved worldwide to prevent and treat postmenopausal osteoporosis (PMO) and fragility fractures.[13] Hydrophobic R-HCl molecules limit bioavailability in organisms. [14] Low solubility and gut wall glucuronide conjugation limit R-HCl oral bioavailability. For class II medications like R-HCl, low drug solubility is a major barrier to absorption, hence increasing solubility may improve bioavailability. [15]
Mechanism of Action of R-HCl
R-HCl, a benzothiophene, modulates estrogen. The investigated chemical has estrogen-agonistic effects on bone and lipid metabolism and estrogen antagonistic effects in uterine and breast tissues. R-HCl's strong affinity for estrogen receptors and gene expression regulation aid its biological effects. Binding affects oestrogencontrolled gene expression in diverse tissues. Estradiol can enter target cells' nuclei and bind to dormant estrogen receptors (ER). alpha (ERα) and beta (ERβ) are oestrogen receptor isoforms. The former activates, while the latter inhibits. Estradiol alters the proteins' structure, creating an E2-ER spatial arrangement. This facilitates dimerization and translocation. Figure 4 shows the occurrence. The entity has interacted with the ERE. A set of genes produces proteins with estrogenic effects on breast and uterine tissues. These genes need the estrogen response element (ERE) to work. [16]
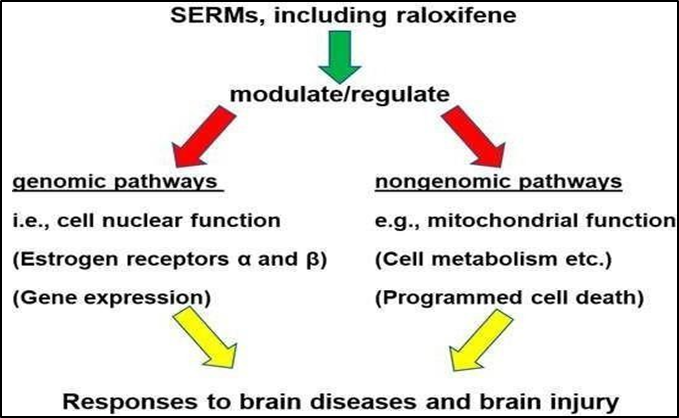
Figure 5: Mechanism of action of R-HCl
Pharmacokinetics
Absorption
Oral R-HCl absorption is fast. Pre-systemic glucuronide conjugation reduces oral dosage bioavailability to 2%, despite a 60% absorption rate. Through this channel, only a small portion of the drug enters the systemic circulation, while the rest is sent to non-target locations, causing peripheral side responses. [17] Enterohepatic cycle and systemic interconversion of R-HCl and its glucuronide metabolites control its maximal concentration and bioavailability. [18]
Distribution
A single oral dose (30–150 mg) has an apparent volume of distribution of 2348 L/kg, regardless of dosage. R-HCl and its monoglucuronide conjugate bind plasma proteins 95%. R-HCl is 0.25 mg/L soluble in water. Log P = 5.69 indicates its strong lipophilicity. Albumin and alpha-1-acid glycoprotein bind the parent molecule, while globulin prefers other sex steroids. [19]
Metabolism
This study examined R-HCl hydrochloride metabolism and pharmacokinetics in humans after oral radiolabeled C14 probe delivery. Extensive first-pass metabolism broke down R-HCl into glucuronide conjugates, including R-HCl-4'-glucuronide, RHCl-6-glucuronide, and R-HCl-6, 4'-diglucuronide. R-HCl biotransformation does not use cytochrome P450 metabolic pathways. Only 1% of plasma R-HCl is unconjugated. After intravenous injection, R-HCl clearance is anticipated to match hepatic blood flow. R-HCl's apparent oral clearance is 44.1 L/kg/hr. [11]
Excretion
R-HCl is mostly eliminated by faeces, however 0.2%) is excreted unchanged in urine. Glucuronide conjugates excrete 6% of the dosage (Bouxsein et al., 2009; D’Amelio & Isaia, 2013).
Pharmacodynamics
The impact on the skeletal system
Reduced bone turnover and higher bone mineral density reduce fracture risk. After ovariectomy, oestrogen receptor degrader (ERD) mRNA in bone marrow decreases and ERD and ERE are barely detectable in trabecular bone. R-HCl slightly upregulates ERD and ERE mRNA. It mostly affects ERD expression and little ERE expression. R- HCl decreased IL6, a biochemical marker of bone turnover, in mice. R-HCl treatment increased OPG and RANKL in osteoblasts of mice. Long-term R-HCl treatment reduced arthritis and osteoporosis. [6]
The impact on the female mammary gland (Breasts)
Oestrogen-dependent breast cancer can be prevented by binding to the mammary tissue ER and blocking DNA transcription. R-HCl significantly reduced serum IGF-I in postmenopausal breast cancer patients. In postmenopausal breast cancer, VEGF, CD34, and Ki-67 protein expression decreases. The intervention did not affect EST activity in nude mice implanted with human breast tissue. R-HCl was developed to impede cancer cell growth. [17]
The impact on the cardiovascular system
R-HCl estrogenizes lipid metabolism. The intervention lowers low-density lipoprotein cholesterol, fibrinogen, and lipoprotein (a) and raises HDL cholesterol without raising triglycerides. It also controls homocysteine levels, which are biological markers of cardiovascular risk. The meta-analysis found a 62% increase in deep venous thrombosis or pulmonary embolism in R-HCl patients. The findings strongly suggest that R-HCl causes platelet aggregation and subclinical thrombus via the Akt signal pathway.
The impact on the genitourinary system
Selective oestrogen receptor modulators (SERMs) can treat prostate cancer at various stages in the male genitourinary system. R-HCl inhibits proliferation, induces apoptosis, and arrests G1 cell cycle in human prostate cancer cells via MAPK cascades. R-HCl and tamoxifen have shown to suppress prostate epithelial and stromal cell growth suggesting prostate hyperplasia treatment. R-HCl induces mitochondria-mediated apoptosis in female genitourinary tract endometrial cancer cells. [16]
Combination of R-HCL and Vit D for Treatment of PMO
Osteoporosis reduces bone mass and quality by 50%, according to the WHO. Vit D, a steroid hormone, is essential for bone health and mineral metabolism. It regulates bone development and turnover by directly affecting osteoblasts, osteoclasts, and non- skeletal tissues. Vit D affects osteoblasts, osteoclasts, and osteocytes, which may affect bone formation, resorption, and quality. Active Vit D modulates the RANKL/OPG signaling pathway to balance bone production and resorption within physiological ranges. At therapeutic doses, active Vit D inhibits bone resorption more than bone production, affecting skeletal structure quality and quantity. Dietary Vit D, not active Vit D, activates osteoblasts and regulates blood 25-hydroxy\vitamin D levels (Yi-Chou Hou et al.,2018)
Novel Drug Delivery Approach
Nanocarriers promote permeability and retention. This technique may increase therapeutic value, decrease dosage, prolong pharmaceutical retention in the mucosal lining, and lower therapy costs. Nanotherapeutics can be delivered via multiple routes (V. Kakkar et al., 2019). Drug efficacy, biological effect, release, and patient acceptance can be improved by encapsulating pharmaceuticals in nanoparticles with a diameter of less than 1 mm (Mortazavian et al., 2014). A nano based formulation was proposed to improve R-HCl's water solubility. Nanotechnology is beneficial in oral, parenteral, and topical systems (Huang et al., 2017; Khan et al., 2016; Khosa et al., 2018; Patel et al., 2012; Salvi & Pawar, 2019; Shah et al., 2016). NLCs navigate several biological hurdles and move the Nano systems along the lymphatic channel through mechanistic paths. The latter enhances oral absorption of a drug. NLCs, biodegradable lipid nanoparticles, are secure nanocarriers. Their great tolerance in in vitro cytotoxicity and in vivo studies may explain this. Non-lamellar liquid crystalline phases (NLCs) are safer than emulsions because they include fewer surfactants and co-surfactants. [19]
Nanostructured Lipid Carriers (NLCS)
Nanostructured lipid carriers (NLCs) are lipid-based nanoparticles with growing interest nowadays. NLCs have lipid, aqueous, and surfactant phases. Careful selection and proportioning of designed product ingredients can significantly affect its final behavior. The mixture of solid and liquid lipids creates a solid lipid matrix with defects. [5] Nanolipid carriers (NLCs) represent a modified form of solid lipid nanoparticles (SLNs), characterized by the partial replacement of the solid constituent with an oil component. [19] Lipid nanoemulsions are oil-in-water (O/W) nanoparticles that resemble nanostructured lipid carriers (NLCs). Lipids, surfactants, and water are important components of the NLCs.
Table 2: Formulation ingredients of nanostructured lipid carriers
|
Formulation Components |
Examples |
|
Solid lipids |
Stearic acid Glyceryl Monostearate (GMS) Cetyl alcohol Carnauba Wax Cetyl Palmitate Glyceryl Palmitostearate (Precirol® ATO 5) Glyceryl Behenate (Compritol 888 ATO® 888 ATO) Grades of Witepsol® Grades of Softisan® Gelucire® |
|
Liquid lipids |
Soybean oil Medium chain triglycerides (MCT)/caprylic and capric Triglycerides Oleic Acid Isopropyl Myristate α-Tocopherol/ Vit E Corn oil Squalene |
|
Surfactants |
Poloxamer 188 Poloxamer 114 Tween® 80 Tween® 20 Sodium dodecyl sulfate (SDS) Sodium deoxy cholate (SDC) Phosphatidyl choline (Phospholipon 90 G) Polyvinyl alcohol (PVA) Soya lecithin Solutol® HS 15 |
Techniques for the Formulation of Nanostructured Lipid Carriers (NLCs)
NLCs are prepared of solid lipid, liquid lipid, emulsifier, and solvent using several methods as outlined in Figure 5.
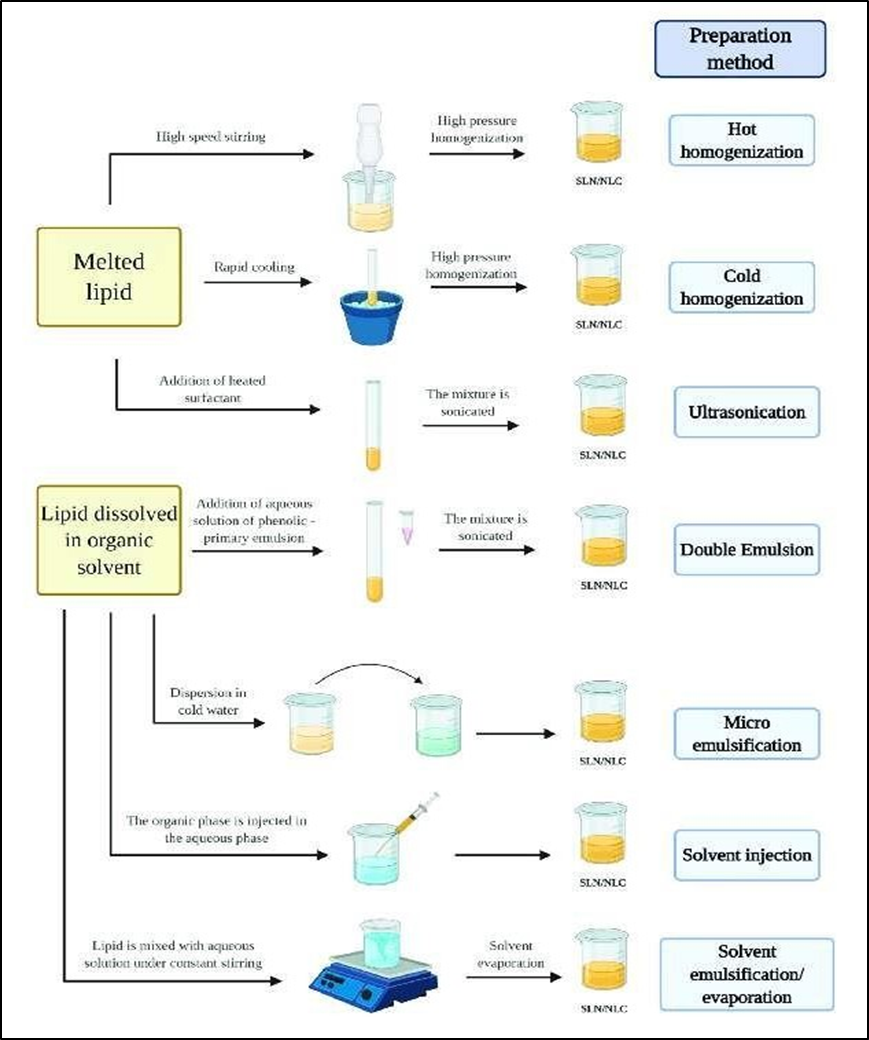
Figure 6: Methods of preparation of nanostructured lipid carriers
Physiological Factors Influencing Sublingual and Buccal Drug Delivery
CONCLUSION
Osteoporosis remains a major global health concern, particularly among postmenopausal women due to estrogen deficiency. Current treatments, including estrogen replacement therapy, bisphosphonates, and selective estrogen receptor modulators (SERMs) like Raloxifene Hydrochloride (R-HCl), have shown efficacy but also present challenges such as low bioavailability and adverse effects. Novel drug delivery systems, particularly nanostructured lipid carriers (NLCs), offer a promising strategy to enhance R-HCl's solubility, absorption, and therapeutic potential. NLCs improve drug permeability, bioavailability, and stability while minimizing systemic side effects. Additionally, combining R-HCl with vitamin D optimizes bone remodeling by balancing osteoblast and osteoclast activity. Advancements in nanotechnology and targeted drug delivery may revolutionize osteoporosis management, offering safer and more effective treatment alternatives. Future research should focus on refining these nanocarrier systems for clinical application, ensuring better patient compliance and outcomes. The integration of nanotechnology in osteoporosis therapy represents a significant step forward in addressing current treatment limitations.
REFERENCES

Sweta Jaiswal, Surendra Dangi*, Dr. Bhaskar Kumar Gupta, Rajni Dubey, Nanotechnology in Osteoporosis: Enhancing R-HCL Bioavailability for Effective Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2084-2095. https://doi.org/10.5281/zenodo.15638784
 10.5281/zenodo.15638784
10.5281/zenodo.15638784
