S.S.P. Shikshan Sanstha’s Siddhi College of Pharmacy, Chikhali, Pune, Maharashtra, India 411062
Novel pharmaceutical formulations called nanostructured lipid carriers (NLCs) are composed of surfactants and co-surfactants along with physiologically and biocompatible lipids. The core of nanostructured lipid carriers (NLCs), which are colloidal drug delivery systems at the nanoscale, is a lipid mixture made up of both liquid and solid lipids. In contrast to polymeric or metallic nanoparticles, this lipid-based Nano system is presented as a safe, non-toxic, and biocompatible Nano-drug delivery method. in contrast to other lipid-based nanocarriers, because of its excellent drug loading capacity, stability, and safety. Alzheimer's disease, Parkinson's disease, dementia, epilepsy, depression, migraine, and other neurological conditions are impacting an increasing number of older adults every day. In order to achieve the required concentration of medicine at the site of action for therapeutic impact, the blood-brain and blood-cerebrospinal fluid (CSF) barrier present a significant challenge to the conventional route of administration for treating these disorders. As a result, the intranasal route of administration is seen as a viable and different way to accomplish targeted outcomes. Researchers have examined brain targeting techniques extensively over the past forty years and believe they have a lot of promise, particularly intranasal delivery because of its advantages. Numerous Nano formulations, including dendrimers, hydrogels, in situ gels, Nano emulsions, nanosuspensions, and lipidic formulations, are being extensively researched. The number of studies outlining formulations based on NLCs has greatly increased in the last several years. This review concludes that how oils and liquid lipids may work in concert with synthetic medications to produce significant therapeutic effects.
Nanoparticles are colloidal areas with size ranging from 10 to 1000 nm. They belong into two different groups: nanocarriers and nanodrugs. Accoutrements created by dissolving or dispersing specifics with colourful nanoparticles which can be categorised as either nanospheres or Nano capsules are appertained to as nanocarriers. The accoutrements used to make nanoparticles can be separated into two orders lipid accoutrements and polymers. The former is known as PNP and comprises polymeric micelles, polymer Nano capsules, and polymer nanospheres. The ultimate contains NLCs and nanoliposomes and is appertained to as a lipid nanoparticle. [1] The treatment of neurological conditions, including Alzheimer's complaint, Parkinson's complaint, brain tumours, and stroke, could be significantly impacted by nanotechnology. multitudinous exploration on neurodegeneration have demonstrated the effectiveness of using nanomaterials to treat problems of the central nervous system. Consequently, the targeted administration of chemotherapeutics made possible by nanocarriers has effectively braked the progression of nasty brain tumours. Because it increases the overall effect of the medicine and emphasises the significance of nano- rectifiers, the most effective use of nanomaterials is in the treatment of central nervous system conditions. The thing of this work was to examine the data regarding the use of nanotechnology in creating medicine delivery systems that can access the blood- brain hedge (BBB) and deliver remedial medicines to the central nervous system (CNS). [2]
Medicine delivery styles intermediated by nanotechnology have employed both non-specific and picky processes with respect to certain brain regions. The maturity of current exploration has concentrated on developing medicine delivery systems using nanoparticles, carbon nanotubes, liposomes, micelles, dendrimers, or proteins, peptides, nucleic acids, or vaccines. [3]
Neuronal loss and progressive declination of neurones in the central or supplemental nervous systems are emblems of a different set of complicated diseases known as neurodegenerative conditions. nonetheless, their essential hazards, like immunogenicity, circumscribe their capability to transport specifics, and the implicit detriment to central nervous system cells disqualifies viral carriers from practical treatments for neurodegenerative ails. Non-viral vectors have clear benefits like lower pathogenicity, affordability, and ease of manufacture. An overview of the use of polymeric nanoparticles as medicine delivery vehicles in neurodegenerative ails, particularly Parkinson's complaint (PD), Alzheimer's complaint(announcement), A summary of the early intervention options grounded on polymeric nanoparticles will also be handed, with an emphasis on gene remedy. [4]
STRUCTURE AND COMPOSITION:
Structural Model of NLC: NLCs were created as advancements over SLNs. In contrast, both liquid and solid lipids are present in the NLC lipid phase. By adding more liquid lipid, NLC causes the nanoparticles to stack and take on an irregular shape, creating an amorphous structure and an imperfect lattice. The lipid content of NLCs exhibits greater application potential than that of SLNs since increasing the liquid lipid can improve the solubility of active ingredients, and active ingredients can aid in better encapsulation. NLCs decrease medication leakage during storage while increasing drug stability and loading capacity. The primary difference between these colloidal particles and the structure of SLN is found in their cores. Lipid liquid and a solid lipid core combine to generate an unorganised drug matrix in NLC, in contrast to SLN, which has a solid lipid core with highly organised lipid. Because of its disorganised structure, more medicines can be loaded into the core. Additionally, NLC can address stability problems caused by crystallisation and drug expulsion that arise during long-term storage of SLN. The NLC core is distorted because it is composed of liquid and solid lipids in a 70:30 to 99.9:0.1 ratio. As the lipophilic molecule is more soluble in liquid lipid, and the imperfections generated by lipid blends, more space is accessible for drug inclusion in these nanocarriers. [5]
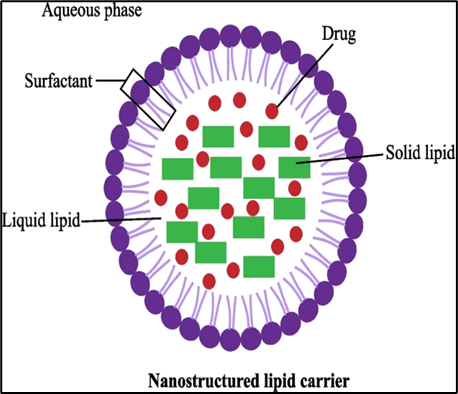
Figure 1: Schematic Diagram Of Nanostructured Lipid Carriers (NLC)
Composition of NLC: Different liquid lipids, solid lipids, and surfactants are mixed in specific ratios and dispersed across aqueous solutions to form NLCs. For NLCs that can be disseminated throughout the body and include therapeutic drug molecules, it is crucial to select nontoxic, biodegradable components. A substantial portion of the oil component of the O/W emulsion is replaced by a solid lipid in NLC, creating a solid particle matrix of this carrier system at body temperature. To make combinations for the particle matrix, liquid lipids (oils) are mixed with solid lipids, preferably in a 70:30 to 99.9:0.1 ratio. [6]
Lipids are the fundamental component of nanostructure lipid carriers that control drug loading capacity, duration of action, and formulation stability. In order to create NLC, solid lipids such fatty acids, triglycerides, diglycerides, monoglycerides, steroids, and waxes were utilised. For the production of lipid nanoparticles, it is preferable to use lipids that are physiologically acceptable, biodegradable, non-toxic, and generally acknowledged as safe. Selecting the right lipids is crucial before using them to create nanoparticulate carriers. The kind and structure of the lipid influence the various properties of nanocarrier. [7]
Emulsifying agents – surfactants: Surfactants are emulsifying agents that reduce surface tension between the two lipid phases and inhibit aggregation, increasing the surface area between lipids while maintaining nanoscale particle size. The addition of a surfactant will increase the zeta potential. NLCs are usually prepared utilising a combination of water- and oil-soluble surfactants rather than a single surfactant since this frequently yields stronger physical stability and improved functional properties. [8]
The concentration of the surfactant is one of the key elements that influences the Nanostructured Lipid Carrier's (NLC) stability, particle size, distribution, degree of crystallisation, and polymorphism. The surfactant is a stabilising agent that is crucial to the production of lipid nanoparticles. In order to create a superb NLC with good properties and stability, the right surfactant concentration must be chosen and used because it lowers surface tension and makes particle partitioning easier during the homogenisation process. [9]
NLC’s lipid-based nanoparticles for better drug delivery:
The main reasons for the increase in NLC utilisation are the removal of technological obstacles in the synthesis of lipid-based nanoparticles and a better understanding of the fundamental principles behind the transport of NLCs via various routes of administration. [10]
A type of lipid-based nanoparticle with uses similar to SLNs is called a Nanostructured Lipid Carrier (NLC). NLCs are created by combining liquid and solid lipids, which improves their drug loading, particle capacity, and release characteristics. [11]
By using physiological transport mechanisms across the blood–brain barrier, such as drug-loaded SLN/NLCs that adsorb apolipoproteins from the systemic circulation and are taken up by endothelial cells via low-density lipoprotein (LDL)-receptor mediated endocytosis, lipid nano formulations, SLNs (solid lipid nanoparticles), and NLCs (nanostructured lipid carriers) have therefore emerged to overcome these difficulties. These mechanisms then unload drugs at the target site (neuronal tissue), which imparts selectivity, target ability, and lower toxicity. [12]
CNS targeting: Overcoming the BBB (Blood Brain Barrier)
In order for the complex brain to successfully evolve, the BBB must develop. It is mostly made up of cells that promote immunological function along with astrocytes, pericytes, and capillary endothelial cells, including microglia, neurones, and basement membrane. To guarantee appropriate activation of the central nervous system, these components—often referred to as a Neurovascular Unit (NVU)—maintain a healthy blood-brain barrier. [13] Because of its structure and physiological barriers, including the blood–brain barrier (BBB), delivering a medicine to the brain is the most difficult undertaking. Active molecules' ability to enter the central nervous system (CNS) is significantly hampered by the blood-brain barrier (BBB). The physiochemical characteristics of over 98% of CNS-active medications prevent them from passing through the barrier because they do not meet the requirements for molecules to enter the central nervous system. Drugs with lipophilic molecules, defined as those with a molecular weight of less than 600 Dalton (Da) and a partition coefficient (Log P) between 1.5 and 2.7, may be permeable to the blood-brain barrier. Diffusion of most medicines from the blood to receptors in the central nervous system (CNS) is effectively impeded by the blood-brain barrier (BBB), which divides the brain interstitial fluid from the circulating blood. The CNS has been targeted using a variety of invasive and non-invasive techniques. [14]
The BBB makes it difficult to produce effective CNS medications since it is not selective in allowing drugs to cross by active transport or diffusion. In addition to inadequate membrane penetration capabilities, negligible transport via the brain capillary endothelium impacts the availability of the drug at theoretically substantial concentrations. A drug's ability to enter the brain must also be assessed in terms of interactions with neuronal receptors, structure-activity correlations, and structure-transport relationships, or membrane permeation. [15]
Through the elimination of waste, the metabolism of many chemicals, including drugs and toxics, and the defence against alterations in the ionic makeup of the cerebrospinal fluid, the BBB also serves a crucial metabolic role. The electrical resistance across the BBB is quite high, which is one of its primary features. The brain's ability to absorb therapeutic and diagnostic substances is significantly restricted by these structures, which also keep harmful substances or pathogens from entering the central nervous system. Additionally, the availability of medications and imaging probes in the central nervous system is further restricted by the presence of ATP-binding cassette transporters (ABC transporters) in BBB endothelial cells, which eject certain substances that may cross the BBB back into the bloodstream. Thus, only a small number of molecules are effectively delivered into the brain. Delivering these substances into the brain using nanoparticles via the blood-brain barrier is one of the most potential substitutes. In recent years, a number of evaluations have been conducted on this topic. [16]
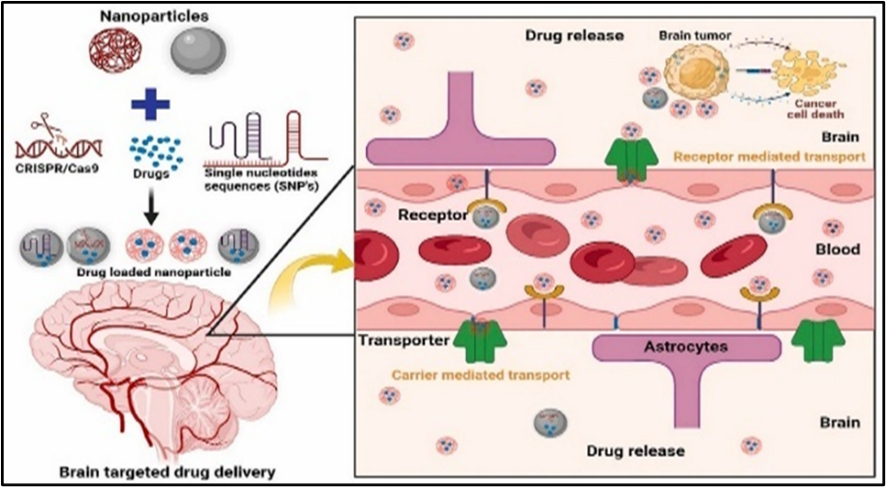
Figure 2: Nanoparticles Through Blood-Brain Barrier
Novel Drug Delivery System Using Nanostructured Lipid Carrier (NLCs)
A mixture of liquid and solid lipids makes up this second-generation lipid nanoparticle, which was first created from SLN but has more flaws in the lipid matrix. In general, NLC is preferable over SLN due to improved stability, reduced drug ejection during storage, controlled drug release, and increased drug-loading capacity. As a result, studies aimed at altering water solubility, improving oral and gastrointestinal absorption, regulating release, extending circulation time by decreasing reticuloendothelial system (RES) identification, and co-delivery have added a variety of active ingredients to NLC. [17]
In a similar vein, NLC offer greater stability by preventing solid lipids from recrystallizing, hence keeping their size nearly constant throughout storage. An average size of 10-500 nm characterises the hybrid carrier that is the binary mixture of liquid lipid (oil) and solid lipid (solid) that constitutes NLCs. The mixture of NLCs consists of a long chain of liquid and lipid with a ratio of 99.9:0.1 and a short chain of solid and lipid with a ratio of 70:30. NLCs have drawn interest from researchers as a substitute for liposomes, emulsions, microparticles, polymeric nanoparticles, SLNs, and others. These nanocarriers can be used to transport both lipophilic and hydrophilic medications. For the oral, parenteral, ophthalmic, pulmonary,topical, and transdermal routes of pharmacological administration, NLCs have shown great promise. [18]
Principles of NLCs:
Improved drug solubility and storage stability, increased surface area, excellent biocompatibility, improved bioavailability, reduced side effects, extended half-life, and effective targeted drug administration are just a few of the many benefits of nanostructured lipid carriers (NLC). NLC is made up of biocompatible and biodegradable lipids and surfactants that are appropriate for lipophilic and poorly soluble medicines in water, hence enhancing oral absorption. Additionally, primary metabolism is decreased and bioavailability is increased as a result of lymphatic transport. [19]
The selection of lipids in NLCs is based on their physicochemical characteristics and capacity to create a stable lipid matrix. The choice of solid and liquid lipids is critical for achieving desired medication loading and release properties. Because of their capacity to maintain structural integrity and regulate medication release, solid lipids such stearic acid, glyceryl monostearate, and propirol ATO5 are favoured. For the purpose of trapping the drug molecules and improving stability throughout transit, these lipids provide a solid matrix. [20] Drugs encapsulated in lipid nanoparticles (NPs) have a longer half-life in the bloodstream, fewer adverse effects, and greater therapeutic efficacy on central nervous system illnesses. Lipid NPs are highly useful for drug delivery to the central nervous system because of these properties. In the central nervous system, liposomes are quickly taken up by macrophages, microglia, and steroids. They can be adsorbed either selectively or non-specifically onto the cell surface, releasing their contents into the cytoplasm of the cell. Enhancing the effectiveness, safety, and precision of drug delivery to the central nervous system (CNS) is the goal of novel techniques, which could completely change how neurological illnesses are managed. To bridge the blood-brain barrier, nanoparticles (NPs) are a versatile and promising approach. The size, shape, surface charge, and functional properties of nanoparticles can be changed to influence how they interact with BBB endothelial cells. Transcytosis and endocytosis are two of the transport systems that can be used to effectively deliver therapeutic medications to the brain thanks to these changes. NPs can protect medications from enzymatic degradation and improve their pharmacokinetic properties. [21]
Types of NLCs
The solid matrix of an imperfect type of NLC is disorganised. A fraction of solid lipid is incorporated by liquid lipid (or oil), which results in imperfect form. This causes tiny cavities to emerge. As a result, there is more room for drug molecules to be accommodated, which increases the drug payload. A small amount of glycerides can be used to get around this problem. Therefore, the creation of irregular forms allows for more room for the loading of drugs, preventing the construction of a highly ordered and structured matrix that would have forced the drug out of the core. [22]
The amorphous core of NLC is formed by combining liquid lipids and oils with solid lipids that remain in the alpha polymorph after solidification and storage. The solid lipid's beta polymorph form yields a crystalline matrix or core. The medication stays lodged in the core of this type of NLC since no crystalline structure is forced. [23]
Because oil molecules can readily enter the lipid matrix at low oil concentrations, Type II NLCs have significant amounts of oil mixed with solid lipids. Different phases may split if more oil is injected than is required for its solubility; this leads to the solid lipid matrix enclosing the tiny, oily nano compartments. [24]
In essence, this kind of NLC is oil-in-solid or fat-in-water, and it can only be created using the phase separation technique. It is advantageous to produce drugs using the phase separation technique if they exhibit greater solubility in oil or liquid lipid than certain types of NLC. Consequently, it enhances the stability and loading capacity of drugs. Small oil droplets are first distributed in the solid lipid phase and then in the aqueous phase. The phase separation approach is covered in further detail in the section on NLC production methods. [25] The w/o/w emulsion concept was used to create this multiple-type product. This kind of NLC is basically fat-in-water or oil-in-solid, and the phase separation Journal Pre-proof method is the only way to make it. To improve drug loading capacity and stability, this technique can be employed to create NLCs with a drug that has higher oil solubility. [26] When it comes to drug delivery, NLCs are superior to conventional methods including liposomes, solid lipid nanoparticles, polymer-based nanoparticles, and micelles. NLCs are less poisonous, more stable, and more effective in encapsulation than liposomes. NLCs feature better drug release kinetics and a larger drug loading capacity than SLNs. In general, NLCs are more biocompatible and less hazardous than polymer-based nanoparticles. NLCs are more stable and have a greater drug loading capacity than micelles. [27]
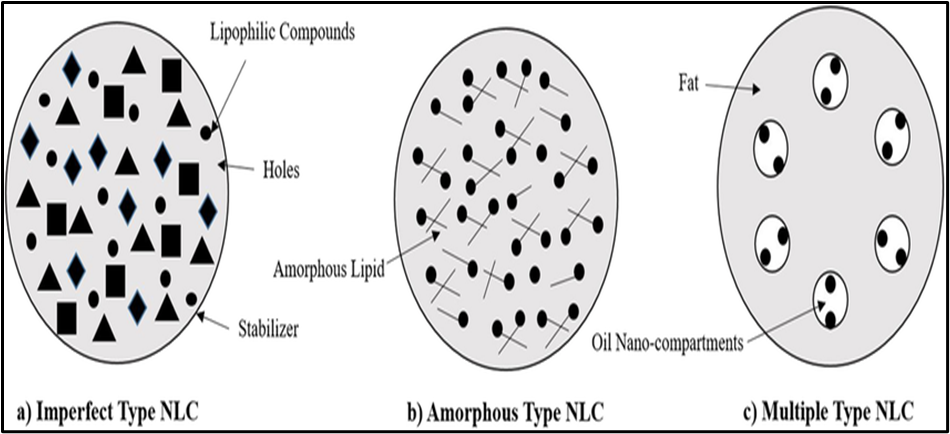
Figure 3: Structure of Different Types of NLCs
Methods for Preparing NLCs
There have been several methods reported for preparing NLCs. Various preparation methods are as follows:
1. High-Pressure Homogenization Method:
Because it doesn't require the use of organic solvents, the high-pressure method used in the production of NLCs is extremely environmentally benign. Additionally, this process may be scaled up to larger capacities and is very adaptable for small-scale production. Melting the lipid component until it reaches a temperature 5–10°c over its melting point is the first step in the formation of NLCs. [28]
The lipid melt is heated to the same temperature as this phase. These two phases are combined and subjected to high shear homogenisation at high temperatures for a short period of time to create pre-emulsion. The pre-emulsion is immediately passed through HPH three to five times at different pressures. In general, the number of cycles is determined by the desired average droplet size of the nano-emulsion. The emulsion is then cooled to room temperature while stirring. The solidification of droplets occurs due to recrystallization of solid lipid. [29] Two commonly used approaches for homogenization are hot homogenization and cold homogenization.
2. Microemulsion technique:
In this technique, the lipids are melted and drug is incorporated in molten lipid. A mixture of water, co-surfactant(s) and the surfactant is heated to the same temperature as the lipids and added under mild stirring to the lipid melt. A transparent, thermodynamically stable system is formed when the compounds are mixed in the correct ratios for microemulsion formation. Thus, the microemulsion is the basis for the formation of nanoparticles of a requisite size. This microemulsion is then dispersed in a cold aqueous medium under mild mechanical mixing of hot microemulsion with water in a ratio in the range 1:25–1:50. This dispersion in cold aqueous medium leads to rapid recrystallisation of the oil droplets. The medication is first mixed with the liquid and solid lipids that have melted. After that, the mixture of co-surfactants and surfactants—such as sodium tauro deoxycholate as a co-surfactant and lecithin as a surfactant—is heated to the lipid phase's melting point. A phase of oil-in-water (o/w) emulsion is created by homogenising these two mixes. The mixture is quickly submerged in cold water and stirred after homogenisation. Initially larger emulsions become smaller particles due to dilution and abrupt temperature fluctuations. This approach is thought to be a simple way to create an NLC. Its disadvantage is that the resulting particle sizes are frequently microscale. [32]
3. Hot?melt extrusion (HME) Method
In the plastics sector, it is one of the most popular processing methods. Pipes, plastic bags, and tubes were previously manufactured using the HME process. But since the 1980s, the pharmaceutical industry has become more interested in using HME, and it is currently being used to make tablets, capsules, implants, and other products. Using a heated rotating screw (extruder), the APIs and excipients are pumped at a greater pressure and then passed through a die to create uniformly sized nanoparticles. An emulsion is formed when the APIs and excipients are passed through an extruder, and afterwards, the size of the obtained emulsion is reduced by passing through the die. One of the many benefits of the HME method is that it eliminates the requirement for the drying process because it doesn't utilise any solvents. Furthermore, the equipment is somewhat costly, and the energy consumption of the driving unit is high. [33]
4. Phase Inversion Method
This method is based on the idea that an emulsion's phase can be inverted due to temperature, as the name implies. Non-ionic polyoxyethylated surfactants, whose characteristics vary with temperature, are employed in this procedure. The hydration of the hydrophilic groups in these surfactants results in a high hydrophilic–lipophilic balance (HLB) value at low temperatures. However, due to the dryness of the ethoxy groups, their HLB value begins to drop as the temperature rises. The term "phase inversion temperature" refers to the temperature at which the surfactant molecule exhibits equal affinity for both lipophilic and hydrophilic phases. [34] W/o-type emulsion is created when the temperature rises above the phase inversion temperature, and vice versa. Using a magnetic stirrer, the lipids, oils, water, and surfactants are combined, heated above the phase inversion temperature, and then stirred to create a w/o emulsion. At a pace of 4 °C/min, three cycles of heating and cooling (85 °C–60 °C–85 °C) are then administered. In order to facilitate phase inversion (from w/o emulsion to o/w emulsion) and the creation of NLCs, this heated liquid is subsequently diluted with cold water. Without the need for an organic solvent, this innovative technique has the benefit of combining thermolabile medications. [35]
Advantages of NLCs
Compared to SLN, physical stability has improved. Hydrophilic and lipophilic medicines exhibit high entrapment efficiency due to greater dispersion in the aqueous phase. Particle sizes are regulated and the NLC demonstrated higher penetrating ability. As with the synthesis of other nanoparticulate systems, organic solvents are not used in the production of NLC. Lipids used to make NLCs are quickly excreted from the body, biodegradable, and well tolerated. [36]
Because of the simplicity it offers, the oral route is the most popular method for medication delivery. Every formulator primarily considers oral drug delivery since it is less expensive, easier to administer without pain, and improves patient compliance compared to parenteral drug delivery. However, a number of obstacles make drug delivery via the preferred route challenging. The main problems in the hostile stomach environment are low solubility and permeability, as well as low stability, which forces the adoption of carrier systems or alternative routes for drug delivery. One effective method for delivering medications orally is NLC.
They created oral medications, such as antibiotics and enzymes, that were insoluble or susceptible to being broken down by digestive enzymes. The lymphatic system has the ability to absorb the particles. The controlled-released particles have the ability to improve the bioavailability of pharmaceuticals studied as a carrier for transdermal delivery systems by slowing down drug degradation and removal. Similar to SLN, NLC's tiny particles can create a thin layer on the skin, preventing medications contained in it from breaking down chemically. In the meantime, NCL preserves the skin, regulates drug release, and stops skin atrophy after prolonged medication use.
CNS Targeting Via NLCs
Communicating with the central nervous system, the BBB is vital to the body's neurovascular system. Because it prevents the CNS from absorbing a range of potentially beneficial therapeutic and diagnostic compounds, the BBB is known to be the main obstacle to effectively treating neurological illnesses. Additionally, it restricts the unrestricted movement of neurotransmitters across brain cells. Endothelial cells, astrocytic end-foot connections, basal lamina, tight junctions, and pericytes are the main components of the blood-brain barrier. [37]
By preserving peripheral circulation from the central nervous system, harmful chemicals can be kept out of the brain. The BBB carries out filtering functions and selectively allows the passage of molecules, including as water, nutrients, and hydrophobic chemicals, through passive transport. Treatments are made more difficult by the blood cerebrospinal fluid barrier (BCSFB), which also makes the central nervous system more complex. A group of ependymal cells called the choroid plexus separates blood from cerebrospinal fluid (CSF), acting as a barrier in the brain. [38]
Challenges: BBB Limits Drug Delivery to The Brain
Targeting brain malignancies orally is a significant difficulty, partly because of the BBB's barrier function, short plasma half-life, and restricted oral absorption. When hydrophilic medications are administered orally, they must first be absorbed and infiltrated through the gastrointestinal tract (GIT) before passing through the blood-brain barrier. Furthermore, hydrophilic medicines and the watery contents of the GIT produce hydrogen bonds that impede absorption and further restrict the process of epithelial infiltration. Additionally, the GIT quickly breaks down peptide medications once they are administered, reducing their plasma half-lives. [39] Intranasal delivery is a new therapeutic medication delivery method that goes straight to the brain via the anatomical connections of the trigeminal nerve (cranial nerve V) and olfactory nerve (cranial nerve I). Since the nanoparticles are injected into the nasal cavity, they shield the chemotherapy medication from the BBB and other biophysical barriers. Nevertheless, the medication cannot distinguish between healthy and malignant brain tissue. Anticancer medications (such methotrexate, 5-fluorouracil, and raltitrexed) have been successfully delivered to the brain through intranasal delivery in some trials. This research has evaluated the cellular processes, cellular receptors, and primary vectors. Since this approach is new, more research is needed to evaluate its advantages and disadvantages for treating brain cancer. [40]
Delivering antisense oligonucleotides to treat spinal muscular atrophy has been authorised. Additional invasive techniques for brain drug delivery were developed, such as deep-brain stimulation and convection improved delivery intracranial implantation. In order to manage CNS diseases, recent advancements in minimally invasive microneedle and polymeric wafer technology offer sustained drug release that avoids the blood-brain barrier. However, these invasive techniques' potential for long-term usage was constrained by the risks of brain exposure and injury. Several non-invasive methods to get across the blood-brain barrier have been used to safely and precisely deliver medications into the brain. Intranasal injection, ligand conjugation, membrane coating, passive transcytosis, and BBB rupture by light, focused ultrasound, biochemical reagents, and radiation are some of these tactics. [41]
Strategies for BBB Penetration
Cerebrovascular disorders, brain tumours, and neurodegenerative conditions like multiple sclerosis, Parkinson's disease, and Alzheimer's disease are all severe CNS disorders. The lack of efficient techniques to allow medications to overcome the brain's natural defences and preserve homeostasis while blocking drug molecules' access into the central nervous system, however, limits the potential for treating these difficult illnesses. Invasive techniques are frequently used to provide a variety of medications for the treatment of various conditions and symptom management. One common technique for delivering drugs into the entire ventricular system without going through the blood-brain barrier is intrathecal drug administration.
The delivery of anti-sense oligonucleotides for the treatment of spinal muscular atrophy has been authorised. For the transport of drugs to the brain, further invasive techniques such as deep-brain stimulation and convection-enhanced administration intracranial implantation were developed. The BBB is circumvented by the recent development of minimally invasive microneedles and polymeric wafers, which offer prolonged medication release for the treatment of CNS diseases.
NOSE TO BRAIN DRUG DELIVERY
Numerous researches have examined and documented nose-to-brain delivery routes. When a drug formulation, drug molecules, or drug-loaded particles are administered, they travel straight from the nose to the brain through the olfactory and trigeminal neurones. They then indirectly enter the systemic circulation before passing through the blood-brain barrier and arriving at the brain. A medication is dispersed to the respiratory and olfactory systems once it enters the nasal cavity. Olfactory nerves in the olfactory area terminate at the olfactory bulb after starting in the olfactory epithelia. [42]
Drugs are endocytosed by olfactory neurones and released in the olfactory bulb before being distributed to various parts of the brain via the intraneuronal route, which might take hours or days. [43]
The brain's intranasal transport pathway: New research suggests that the nose-to-brain channel may be a non-invasive means to deliver therapeutic modalities or neurocarriers straight to the brain, avoiding the blood-brain barrier. Three distinct pathways, including the systemic, trigeminal, and olfactory pathways, are involved in the transport process. Olfactory and Trigeminal pathways: The dorsal nasal mucosa and the front part of the nose are innervated by branches of the trigeminal nerve's ophthalmic division, whilst the nasal mucosa's lateral walls are innervated by branches of the maxillary division. There are no direct neural inputs to the nasal cavity from the trigeminal nerve's mandibular division, which reaches to the lower jaw and teeth. After joining at the trigeminal ganglion, the trigeminal nerve's three branches travel centrally to enter the brain at the pons level and end in the brainstem's spinal trigeminal nuclei. [44]
Systemic pathway: This is an indirect method in which the medications go through the bloodstream and lungs before arriving to the brain. As a result, this route requires the medications to pass across the blood-brain barrier in order to reach the brain, which lengthens the time it takes to provide the desired therapeutic effect and restricts the quantity of drug that can actually reach the brain. Furthermore, the amount of drug in the brain following intranasal administration differs between patients and suffers elimination via renal and hepatic mechanisms. Thus, depending on the characteristics of the medicine, it might enter the brain directly or through the systemic route. For example, after being administered intranasally, certain lipophilic medications enter the brain through the systemic pathway. [45]
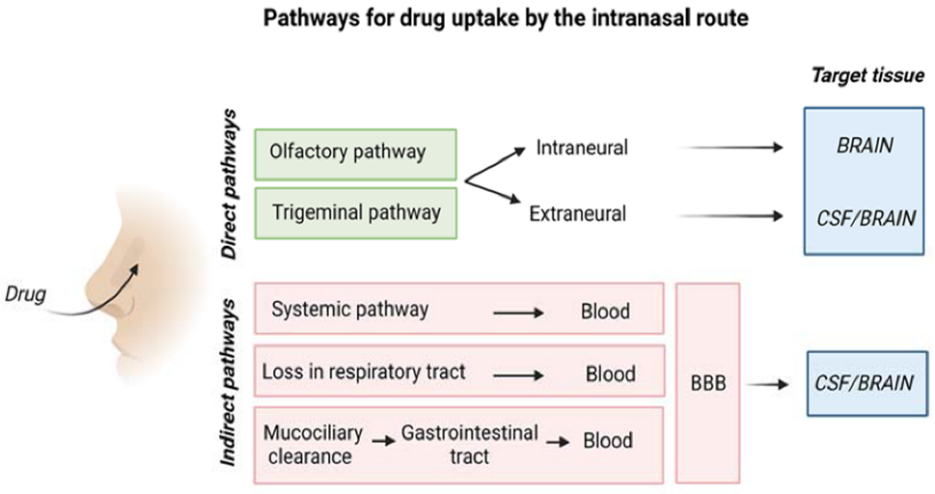
Figure 4: Schematic Representation of Drug Uptake by The Intranasal Route.
Nasal epithelial cells, the trigeminal nerve, and olfactory sensory neurones all activate intracellular pathways. Depending on the cells involved, these pathways involve two distinct mechanisms: transcytosis across the respiratory and olfactory epithelium cells to the lamina propria, or endocytosis by the neural cells on the nasal epithelial surface followed by intraneuronal transport. Paracellular diffusion through the respiratory and olfactory epithelia to the underlying lamina propria is one example of an extracellular transport system. It has been proposed that the nasal epithelium's frequent cell turnover may cause tight junctions to continuously reorganise and relax, favouring paracellular drug transport. [46]
Applications in targeting various diseases
Epilepsy
Recurrent seizures are the hallmark of epilepsy, a chronic neurological illness brought on by increased cellular activity in some brain regions as a result of membrane depolarisation and the consequent release of excitatory neurotransmitters. The seizures might include co-existing disorders and vary in strength and duration from person to person. Drug bioavailability through the oral route is hampered by a number of factors, including protein binding, hepatic first pass metabolism, GIT permeability, fluid dissolution in the GIT, and blood-brain barrier bridging. Despite the GIT's difficulties, the intravenous route has similar difficulties and is also intrusive. Therefore, a different approach that targets the brain might improve patient compliance and/or adherence and increase the drug's effectiveness. [47]
With a prevalence of 57 per 1000, epilepsy is the most common CNS condition. By 2001, there may be 5.5 million cases in India. Neuronal excitability and neuroinflammatory cytokine dysfunction in epilepsy are thought to be caused by abnormal neuronal discharges that are linked to oxygen deprivation, trauma, tumours, and infections. The side effects of anti-epileptic medications encourage the use of medications packaged into nanoparticles that can penetrate the blood-brain barrier and deliver medication directly. It has been found that solid lipid nanoparticles of chitosan loaded with carbamazepine are more effective than carbamazepine loaded in nanoemulges. [48]
Solutions, suspensions, pills, capsules, and extended-release medicines are examples of oral formulations. When medications are taken orally and absorbed by the gastrointestinal (GI) tract, they first travel via the liver before entering the systemic circulation. This can lead to first-pass metabolism, which lowers the drug's bioavailability. Because of the potential for significant inter-subject variability in the dose-concentration relationship, medications with low bioavailability resulting from substantial first-pass metabolism or low GI absorption cannot be taken orally. For lipid-soluble medications that undergo significant GI tract or liver metabolism, buccal and sublingual routes that circumvent gastric and hepatic first-pass metabolism are optimal. [49]
Depression
These conditions, which include complex alterations in brain structure, function, and neurotransmitter systems, are impacted by both hereditary and environmental factors. Examples of these conditions include depression, schizophrenia, bipolar disorder, and anxiety disorders. Neurotransmitter systems that are essential for mood regulation, cognition, and emotional reactions, such as dopamine, serotonin, and glutamate pathways, are frequently dysregulated in psychiatric illnesses. [50]
Alzheimer’s disease
The sole known treatment for Alzheimer's disease, one of the most prevalent neurodegenerative disorders, is symptomatic. The main clinical symptom observed is dementia, which is followed by cognitive and learning impairment. Irritability, disorientation, and behavioural abnormalities may continue as the illness worsens. Alzheimer's disease patients' brains exhibit a distinctive pattern of neurofibrillary tangles and β-amyloid (Aβ) plaques, which are thought to be the pathological hallmarks of the illness's course. Peptides of 39–42 amino acids, known as Aβ plaques, are produced when amyloid precursor protein metabolism is compromised. [51]
Donepezil was encapsulated in chitosan nanosuspensions between 150 and 200 nm in size for the treatment of AD. A cannula was used to intranasally inject the created nanosuspensions into the Sprague-Dawley rats' noses. Both brain and plasma concentrations were considerably increased by the use of formulations as opposed to free drug delivery. The overall high acceptability of these formulations was demonstrated by in vivo investigations, which also showed that no toxicity, death, or changes in body weight or haematological conditions occurred in animals following treatment. An alternative approach involved loading donepezil into liposomes made of DSPC/Chol/PEG, which had a diameter of around 100 nm and a negative surface charge. Following the intranasal injection of a liposomal formulation to Wistar rats, donepezil's bioavailability in the brain and plasma was much higher than in any other organ. All of the liposome formulations had high encapsulation efficiency, negative Z-potential values, and mean diameters between 175 and 219 nm. These multifunctional liposomes demonstrated a significant increase in tacrine permeability across phospholipid vesicle-based barriers and sheep nasal mucosa in addition to their strong mucoadhesive qualities. Tacrine-functionalized liposomes' neuroprotective efficacy and antioxidant qualities were further enhanced by the addition of α-tocopherol to the formulation. [52]
Migraine
Traditionally, migraine attacks are divided into four phases: premonitory, aura, migraine headache itself, and postdrome. These episodes can last anywhere from a few hours to several days. The premonitory phase, which starts a few hours to days before the headache phase, is marked by a number of symptoms, such as weariness, stiff neck, and difficulty concentrating. Approximately one-third of patients encounter the aura phase, which is marked by symptoms associated with visual, sensory, and/or motor abnormalities, at the same time as the premonitory and migraine headache phases. The majority of individuals, however, do not go through this stage and instead have headache-related symptoms as light and sound sensitivity and nausea. The intensity of the several stages of migraine and its accompanying symptoms is illustrated by the postdrome phase, which follows the headache phase and is marked by non-headache symptoms such as exhaustion, trouble focussing, and stiff neck that can linger for up to 24 to 48 hours. [53]
The American Headache Society examined the effectiveness of drugs used to treat acute migraines in a revised literature evaluation. These studies used one or a combination of several endpoints of efficacy, such as headache freedom, reduced disability, absence of nausea or vomiting, absence of photophobia or phonophobia (increased sensitivity to light or sounds), and headache relief (i.e., reduction from severe or moderate intensity to mild or none). Following the administration of various drugs, outcomes were assessed at different intervals. A helpful guide for determining which drugs have proven superior to placebo and the level of the evidence proving that superiority is provided by this and other evidence-based guidelines. [54]
There are many different approaches to treating epilepsy because of its complicated etiopathogenesis. Antiseizure drugs (ASM) can be categorised based on their mechanism of action or biological characteristics. Generally speaking, they work by reducing or modifying neuronal excitability, which halts the growth of electrical discharges at the brain level. Although there have been significant advancements in the treatment of epilepsy since its first mention in ancient literature, problems still exist. Cognitive deficits, emotional swings, and systemic toxicity are some of the negative effects that traditional ASMs may cause. Furthermore, some epilepsy syndromes could be very resistant to standard therapies, requiring the use of other strategies in order to improve results. The main goals of this review are to give a thorough picture of the state of epilepsy care today, emphasising the shortcomings of conventional ASMs and the necessity of alternative treatment modalities. [55]
Parkinson’s Disease
Using the mucoadhesive polysaccharide glycol chitosan, Cometa et al. studied new SLNs to enhance dopamine brain delivery by intranasal dosing. SLNs had a high dopamine entrapment effectiveness, positive surface charge, and an average diameter of about 140 nm. Dopamine-loaded SLNs were demonstrated to be capable of prolonged and continuous neurotransmitter release in vitro. Parkinson's disease is a neurodegenerative condition that is primarily linked to intracellular inclusions of aberrant proteins known as Lewy bodies and the loss of striatal and dopaminergic neurones in the substantia nigra that control motor movements. Thus, stiffness, tremors, hypokinesia, and decreased balance are typical signs of Parkinson's disease. Lewy bodies, which are eosinophilic inclusions seen in diseased neurones, are thought to be the defining feature of Parkinson's disease and related. In animal models of Parkinson's disease, the restoration of dopaminergic neurones has improved with the administration of glial-derived neurotrophic factor.
FUTURE DIRECTIONS
Neuroscience and emerging nanotechnology are similar to a game of risk and reward. Nowadays, nanomedicine is regarded as a useful technique for medication delivery that crosses the blood-brain barrier. Clinical trials for these nanomedicines are now underway, although it is yet unclear how they should be transported and whether there are any safety issues. The characteristics and makeup of nanoparticles can produce oxidative stress, modification of amino acids, and disruption of the blood-brain barrier, all of which can result in neurotoxicity in the brain. Despite their ability to successfully target drugs, functionalised nanoparticles may aggregate and have restricted drug loading due to their vast surface area and nanosize structure. [56]
The bioavailability of many medications, particularly those that target the central nervous system, has been greatly increased via intranasal administration. For example, when sumatriptan is administered intranasally to treat migraines, its bioavailability is around 15-20%, whereas when it is administered orally, it is just 1-2%. This improvement results from first-pass hepatic metabolism, direct absorption through the nasal mucosa, and passage through the gastrointestinal system. According to pharmacokinetic research, intranasal administration may provide greater peak plasma concentrations and a quicker beginning of effect than oral methods. [57]
The translation of treatment outcomes can be greatly impacted by the differences between animal models and humans, such as differences in nasal anatomy, mucosal permeability, and metabolic processes. By directly targeting the brain and boosting the medications' availability in the brain, continued development of nanoparticles promises to improve the treatments' efficacy in intranasal drug delivery systems while lowering resistance and side effects. [58] According to research published over the years, the brain's bioavailability may be increased by optimising formulation characteristics such liposome surface modification, PEGylation, phospholipid composition, carrier selection, and edge activators. Chitosan-based nanoparticles, which have demonstrated better medication absorption and mucosal adhesion in preclinical studies, are a viable method for optimising formulations for nose-to-brain administration. [59]
In order to treat neurological and psychiatric disorders, basic research should be conducted to clarify the mechanism of medication delivery to specific brain regions. This is because the mechanism of drug delivery to the brain is also obscure. Focus must also be placed on formulation techniques, drug delivery systems, the recherche of novel excipients to increase nasal bioavailability, and the examination of polymers' adhesive qualities in order to prevent drug expulsion and improve its period of action. In addition, a thorough appraisal of the nanotoxicity of nanocarriers and toxicodynamic searches of drugs and excipients must be conducted. [60]
CONCLUSION:
Due to its lipophilic properties and biocompatibility, the nano-based drug delivery system has garnered interest and is regarded as one of the developing technologies. Because of their many benefits over other nanocarriers, nanostructured lipid carriers (NLC) have demonstrated exceptional potential for the effective delivery of the medicine to the brain via the nose-to-brain pathway. Because of a number of crucial features, NLC is a very promising drug delivery technique. These include their simplicity of preparation, ability to improve stability, and ability to increase drug loading. NLCs have more promise as a medication delivery system since they are non-toxic and biocompatible. NLC has encouraging prospects for commercialisation because of its simplicity of large-scale manufacturing and laxer regulatory concerns. NLC is a versatile nanocarrier system that can deliver a range of medications to treat central nervous system illnesses via the intranasal route. This review article covers NLCs' structure, kinds, formulation, and advantages over their predecessors. As essential elements in creating a stable drug delivery system, the characterisation of NLCs and several formulation techniques are also covered.
ACKNOWLEDGEMENT:
We Would like to thank the SSP Shikshan Sanstha’s Siddhi College of Pharmacy, Chikhali, Pune for providing infrastructure.
FUNDING SOURCES: The author(s) received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST: The authors do not have any conflict of interest.
ETHICS STATEMENT: This research did not involve human participants, animal subjects, or any material that requires ethical approval.
CONSENT TO PARTICIPATE: This study did not involve human participants, and therefore, informed consent was not required.
CLINICAL TRIAL REGISTRATION: This review does not involve any clinical trials.
PERMISSION TO REPRODUCE MATERIAL FROM OTHER SOURCES: Not Applicable
CONSENT TO PUBLISH: Not applicable. This article does not contain any individual person’s data in any form (including individual details, images, or videos).
REFERENCES






Madhuri Sonawane, Vidhya Thorat, Pooja Paliwal, Yashashri Deore, Rohan Sawant, Dr. P. N. Sable, Nanostructured Lipid Carriers as Brain-Targeted Drug Delivery Vehicles in Neurodegenerative Diseases, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 504-523. https://doi.org/10.5281/zenodo.17522207
 10.5281/zenodo.17522207
10.5281/zenodo.17522207
