School of Pharmacy and Research People’s University, Bhopal, Madhya Pradesh, India 462037
Microneedle-mediated transdermal drug delivery (TDD) has emerged as a promising alternative to conventional oral and injectable dosage forms. This minimally invasive technology offers several advantages, including painless administration, enhanced patient compliance, and circumvention of first-pass hepatic metabolism, thereby improving drug bioavailability. Microneedles can effectively breach the stratum corneum without stimulating pain receptors or causing tissue damage, enabling efficient drug transport into systemic circulation. Lovastatin, a widely used lipid-lowering agent, has recently garnered attention for its additional wound healing properties. However, its poor aqueous solubility and limited skin permeability restrict its therapeutic efficiency through traditional routes. Microneedle systems offer an innovative platform to overcome these limitations by enhancing the systemic availability of lovastatin, particularly for wound management. This review highlights the fundamental concepts, types, fabrication techniques, and materials used in microneedle systems. It further explores current advancements in microneedle- based delivery of lovastatin, supported by preclinical and clinical findings, and evaluates the potential of these systems to transform transdermal drug delivery in modern therapeutics.
Wound healing is a complex physiological process that can be severely compromised in patients with chronic conditions such as diabetes. Lovastatin, a statin class drug, exhibits not only lipid-lowering effects but also angiogenic and anti-inflammatory properties beneficial in wound healing. Transdermal drug delivery systems (TDDS) offer a non- invasive method to bypass the limitations of oral and injectable routes. Among TDDS, microneedle (MN) technology has gained attention for its minimally invasive yet effective drug delivery potential. Microneedles penetrate the stratum corneum, enabling the transport of hydrophilic and macromolecular drugs directly to systemic circulation.1
Classification of wounds:
Wounds that heal via the standard wound-healing process are known as acute wounds. Acute wound healing usually takes five to ten days or up to thirty days. Five categories are used to further categorize acute wounds.
Acute wounds are categorized as chronic wounds if they fail to heal to the typical stage. They can only heal partially and at a significantly slower rate; even after partial and competitive healing, they may recur. They require extra medical attention as well as specialized surgical care. Any acute wound can turn into a chronic wound if the patient has risk factors that interfere with the healing process. Chronic injuries come in a variety of forms, such as leg ulcers, diabetic ulcers, pressure injuries, and more.2,3,4
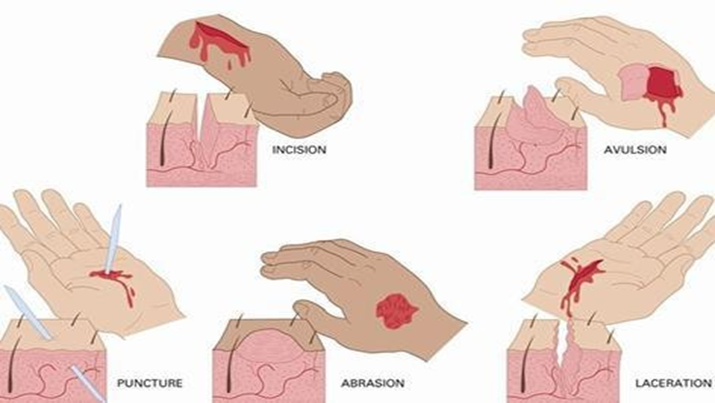
Fig. 1: Types of wounds
Wound healing
The four phases of wound healing—haemostasis, inflammation, proliferation, and maturation—all overlap and proceed in a precise and controlled way. Wound healing is a complex and dynamic process. A cellular immune response is set off by the injury, and this response results in downstream signaling, activation, and responses. This step results in the activation of the keratinocytic system.5,6
Transdermal Drug Delivery (TDD) is a painless, non-invasive method that allows drugs to pass through the stratum corneum into deeper skin layers for systemic absorption. It bypasses first-pass metabolism, offers a steady pharmacokinetic profile, and enhances patient compliance by reducing dosing frequency. TDD is especially beneficial for individuals with needle phobia, swallowing issues, or those unable to take oral medication, and supports self-administration, Additionally, TDD provides a stable pharmacokinetic profile with fewer peaks and troughs, thereby minimizing side effects and improving therapeutic outcomes.7,8,10,11
Structure of skin
The skin, which makes up 16% of an average person's total body mass, is the largest and most accessible organ in the body, covering 1.7 m2. The skin's primary purpose is to act as a barrier of defense between the body and the outside world, keeping out germs, toxins, allergies, ultraviolet (UV) radiation, and water loss. The three primary sections of skin are the outermost layer, known as the epidermis, which contains the stratum corneum; the middle layer, known as the dermis; and the innermost layer, known as the hypodermis.13-15
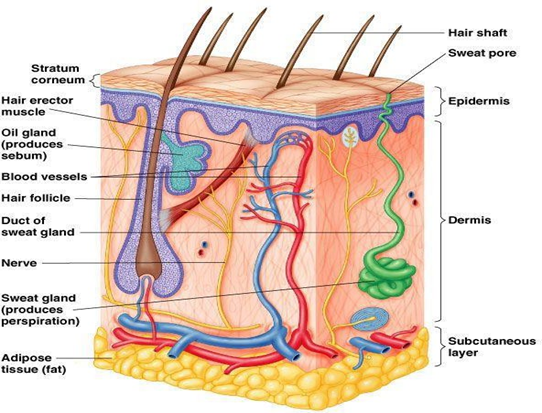
Fig. 2: Structure of skin
Penetration routes
Drugs can penetrate the skin through three main pathways: intercellular, transcellular, and transappendageal. Hydrophilic molecules move through cells (transcellular), lipophilic drugs pass between cells (intercellular), and others enter via hair follicles or sweat glands (transappendageal). These routes enable absorption through the stratum corneum into deeper skin layers. 16
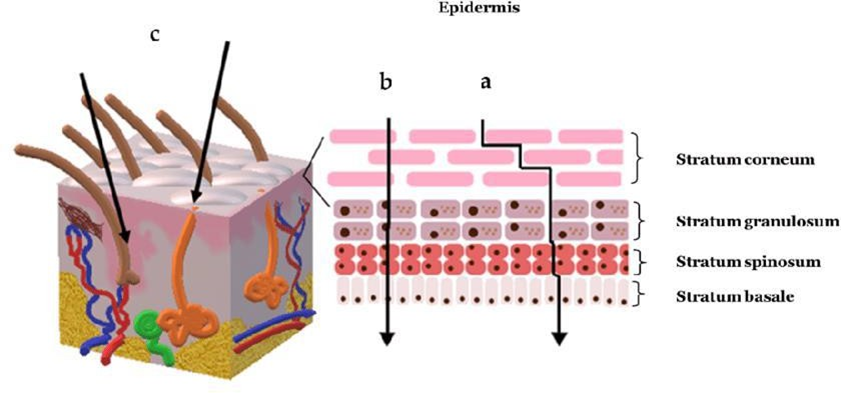
Fig. 3: Penetration routes: a) Intercellular, b) transcellular and c) transappendageal pathways
Microneedle drug delivery system
The position and size of the skin make it an appropriate, non-invasive site for the delivery of therapeutic drugs as well as the collection of interstitial fluid samples for the identification of biomarkers. MN-based delivery and sampling are essentially non- invasive, painless, self-administered methods that replace hypodermic needles and improve patient compliance. Microneedles (MNs) are made utilizing a variety of constituent materials with a range of patterns and shapes, from metals and glass to polymers and hydrogels, in conjunction with a variety of delivery methods, as a result of the field's increased research activity over the past few decades.17
Four of the approaches—poke and patch (solid MNs), coat and poke (coated MNs), poke and flow (hollow MNs), poke and dissolve (dissolving MNs), and poke and release (hydrogel-forming MNs)—were first suggested, with one more developed later.18,19
Solid microneedles penetrate the stratum corneum to enhance drug delivery to the dermis, improving bioavailability. They are especially effective for vaccines due to their strong and lasting immune response. Compared to hollow types, they are simpler to manufacture, mechanically stronger, and can be made from materials like silicon, metals, or polymers.20
Hollow microneedles contain an internal channel to deliver or store liquid drugs, making them ideal for high- dose or high molecular weight formulations. They offer controlled release, are suitable for vaccines, and allow pressure-based drug flow similar to hypodermic needles. Their design supports both burst and sustained drug delivery.20
Coated Microneedle (CMN)
Coated microneedles are solid needles layered with a drug solution. They deliver small drug doses rapidly and are useful for proteins and DNA. Though minimally invasive and effective—comparable to intradermal vaccines—they pose risks of cross-contamination if drug residues remain on the needle tips.20
Dissolving Microneedle (DMN)
Dissolving microneedles are made of water-soluble materials that release drugs as the needles break down in the skin. Suitable for single-step administration of macromolecules, they offer fast release and patient-friendly use. However, they require precise insertion and have slower dissolution rates, which can limit efficiency.20
Table 1: Methods for preparation of microneedle
|
Sr. No. |
Type of microneedle |
Method of preparation |
|
1. |
Solid Microneedle |
Isotropic and anisotropic wet etching, Silicon dry-etching process, and Three- dimensional laser ablation. |
|
2. |
Coated Microneedle |
Dipping or spraying the microneedles |
|
3. |
Dissolving Microneedle |
Micro molding or Solvent casting or Mold- cast |
|
4. |
Hollow Microneedle |
Lithographic molding technique |
Materials used in the preparation of microneedle
The principal factor driving MN manufacture is their unbreakable and pliable skin penetration. The MN manufacturing difficulty has been addressed by taking into account a number of elements, including material, manufacturing process, and design. Different kinds of MNs have been fabricated using a range of materials. Polymers, metals, ceramics, and silicon are a few examples of these materials.
Advantages of Microneedles
Applications of Microneedle drug delivery system.
Microneedles, especially solid types made of titanium or stainless steel, improve the delivery of short DNA/RNA strands by enabling better skin penetration. Combined with iontophoresis, they enhance intracellular uptake more effectively than traditional methods.
Microneedles deliver vaccines with better immune response and lower doses compared to injections. Hollow and dissolving types were successful in delivering DNA vaccines for influenza, rabies, and anthrax, showing higher antibody levels and better patient comfort.
Microneedles overcome enzymatic degradation of peptides like desmopressin and cyclosporin A, ensuring better skin penetration and release. Polymer-based microneedles have also been engineered to treat conditions like keloids by delivering specific peptide blockers.21
Microneedles significantly enhance transdermal delivery of hormones like insulin and parathyroid hormone. They can be combined with smart materials or glucose-sensing systems for responsive delivery, showing faster absorption and reduced blood glucose levels.
Used in skincare, microneedles improve the delivery of cosmetic agents like retinyl retinoate and ascorbic acid. E-rollers and nanoliposomes help deliver these ingredients deeper into the skin for better anti-aging and pigmentation control effects.
Microneedles coated with lidocaine offer rapid and painless local anesthesia, with quicker onset than topical creams. PEG-lidocaine dispersions show better penetration within minutes, making them ideal for minor procedures.
Microneedles filled with pain relievers like meloxicam provide fast, localized relief. They offer higher drug deposition, especially for neuropathic pain, by targeting receptors without systemic side effects or skin irritation.
In ophthalmology, microneedles combined with iontophoresis enhance drug delivery to the posterior eye segment, allowing over 30% of nanoparticles to reach target areas, improving treatment for conditions like macular degeneration.22
Microneedles are used for localized delivery of anticancer agents like 5-fluorouracil and tamoxifen. They increase drug permeability in tumors like melanoma and breast cancer while minimizing systemic side effects.
Clinical studies show microneedles cause minimal pain and no skin irritation. Participants preferred them over hypodermic needles. Trials for lidocaine and psoriasis treatment confirmed faster drug action and improved outcomes with daily use.
DRUG PROFILE
Lovastatin: A Multifunctional Lipid-Lowering Agent with Therapeutic Potential in Wound Healing
Lovastatin is a widely prescribed statin drug primarily used for lowering cholesterol levels. Beyond its lipid-lowering capabilities, it exhibits promising properties including bone regeneration, anti-inflammatory action, and enhancement of wound healing, particularly when delivered through novel systems such as microneedle patches. This section provides a comprehensive overview of the physicochemical, pharmacokinetic, and pharmacodynamic characteristics of lovastatin along with dosage and storage information.
Lovastatin is a competitive inhibitor of the enzyme 3-hydroxy-3-methylglutaryl- coenzyme A (HMG-CoA) reductase, which catalyzes the conversion of HMG-CoA to mevalonate — a key step in cholesterol biosynthesis. Originally developed as a lipid- lowering agent, recent studies have highlighted its broader therapeutic potential, including effects on bone tissue regeneration, fracture healing, and cutaneous inflammation.
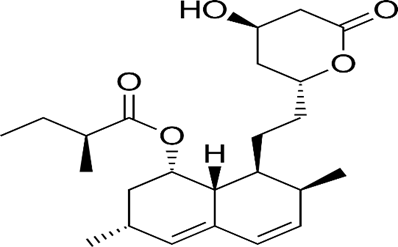
Structure of lovastatin
Physicochemical Properties of Lovastatin
|
Sr. No. |
Property |
Description |
|
1. |
Chemical Name |
[(1S,3R,7S,8S,8aR)-8-[2-[(2R,4R)-4-hydroxy-6- oxooxan-2-yl] ethyl]-3,7-dimethyl-1,2,3,7,8,8a- hexahydronaphthalen-1-yl] (2S)-2-methylbutanoate |
|
2. |
Molecular Formula |
C??H??O? |
|
3. |
CAS Number |
75330-75-5 |
|
4. |
Molecular Weight |
404.5 g/mol |
|
5. |
Melting Point |
174.5°C |
|
6. |
Physical State |
White to off-white crystalline powder |
|
7. |
UV-Vis λmax |
238 nm |
|
8. |
Log P |
4.26 |
Pharmacological Profile
Pharmacodynamics
Lovastatin belongs to BCS Class II, characterized by poor solubility and high permeability. It effectively reduces levels of total cholesterol, low-density lipoprotein cholesterol (LDL- C), apolipoprotein B (apoB), non-HDL-C, and triglycerides (TG), while modestly increasing high-density lipoprotein cholesterol (HDL-C). It is commonly used for the treatment and prevention of cardiovascular conditions.
Pharmacokinetics
Lovastatin (branded as Mevacor) is a fungal metabolite derived from Aspergillus terreus. It is a lipophilic prodrug that undergoes first-pass hepatic metabolism. It inhibits cholesterol biosynthesis by competitively blocking HMG-CoA reductase, leading to reduced intracellular cholesterol and increased uptake of LDL-C by the liver. This action helps in lowering cardiovascular risk, especially in patients with Type 2 diabetes and those with a history of cardiac events.
Storage Conditions
Lovastatin should be stored between 5°C and 30°C, preferably in tightly sealed containers. Under these conditions, the tablets remain stable for up to 24 months from the date of manufacture. Optimal storage is at room temperature, between 20°C and 25°C.
Dosage Guidelines
The recommended dosage of lovastatin ranges from 10 to 80 mg/day, typically administered twice daily. The starting dose may be gradually increased in 20 mg increments, with a maximum dose of 80 mg/day.
CONCLUSION
Lovastatin holds considerable promise in wound healing applications, particularly for managing diabetic ulcers, owing to its ability to modulate VEGF expression, promote angiogenesis, and exert anti-inflammatory effects. Despite these therapeutic benefits, its clinical use in topical formulations is hindered by poor aqueous solubility and limited skin permeability. Microneedle-based drug delivery systems offer an innovative and effective solution to these limitations by enabling targeted, controlled, and enhanced transdermal delivery of lovastatin. The selection of appropriate polymers, microneedle geometry, and fabrication techniques plays a critical role in optimizing drug delivery performance. As research in this area advances, microneedle-mediated systems are poised to transform the landscape of wound care therapeutics. Continued interdisciplinary efforts are necessary to refine fabrication technologies, ensure safety and patient compliance, and facilitate clinical translation, ultimately paving the way for commercial adoption and improved patient outcomes.
REFERENCES

Rani Namdev, Rajni Dubey, Dr. Bhaskar Kumar Gupta, Mariya Beg, Microneedle-Based Transdermal Delivery of Lovastatin for Enhanced Wound Healing: A Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1423-1430. https://doi.org/10.5281/zenodo.17113088
 10.5281/zenodo.17113088
10.5281/zenodo.17113088
