GIET School of Pharmacy GIET Institutions, Rajamahendravaram-533796, Andhra Pradesh
Metformin, a widely prescribed medication for Type 2 Diabetes Mellitus (T2DM), is associated with an increased risk of vitamin B12 deficiency. This review explores the epidemiology, mechanisms, clinical manifestations, and management strategies of metformin-induced B12 deficiency. Studies indicate a dose-dependent rise in deficiency incidence, emphasizing the need for vigilant monitoring, particularly in long-term users and high-risk individuals. The mechanisms by which metformin impacts B12 absorption are multifaceted, potentially involving disruptions in enterohepatic circulation, reduced intrinsic factor production, and altered receptor binding. Clinical manifestations of deficiency range from subtle neurological symptoms to severe neuropathy and neuropsychiatric complications, necessitating careful evaluation and timely intervention. Management strategies include supplementation with appropriate B12 forms, such as hydroxocobalamin or methylcobalamin, along with regular monitoring of B12 levels. Future research should focus on refining supplementation protocols and evaluating long-term outcomes to optimize patient care and minimize complications associated with metformin-induced B12 deficiency.
Metformin plays a central role in managing type 2 diabetes mellitus (T2DM) and is prescribed to millions globally.(1) Over time, studies have increasingly linked long-term metformin use with vitamin B12 deficiency, a connection noted as far back as 1971. Despite this consensus, many aspects remain unclear.(2) The prevalence of metformin-induced vitamin B12 deficiency varies widely, ranging from 5.8% to 52%, due to differing study criteria and participant characteristics. Neuropathy, often presenting without typical hematological signs, has become a key indicator of vitamin B12 deficiency, mimicking diabetic neuropathy and potentially exacerbating it.(3) Research faces challenges in establishing precise vitamin B12 requirements for neural health and attributing neuropathy solely to metformin use. Addressing these complexities primarily relies on observational studies, given the impracticalities of randomized controlled trials.(4) This study aims to fill gaps in understanding by exploring these issues in African populations, focusing on prevalence, neuropathy correlation, and risk factors for vitamin B12 deficiency in metformin-treated T2DM patients.(5)
MECHANISM OH ACTION OF THE METFORMIN
Metformin, categorized as a biguanide within the class of oral hypoglycemic drugs, operates through several mechanisms that contribute to its glucose-lowering effects, although some aspects of its mode of action remain incompletely understood. (6)Primarily, metformin is believed to lower glucose levels by inhibiting gluconeogenesis in the liver, thereby reducing the production of glucose.(7) Additionally, it enhances insulin sensitivity, inhibits lipogenesis, increases glucose uptake in the intestine and muscles, and delays gastric emptying, which in turn reduces appetite.(8) Both the American Diabetes Association and the European Association for the Study of Diabetes recommend metformin as the initial therapeutic Categorized as a biguanide in the class of oral hypoglycemic drugs, metformin works through several mechanisms that contribute to its glucose-lowering effects, although some aspects of its mechanism of action remain incompletely understood. (6)Primarily, metformin is thought to lower glucose levels by inhibiting gluconeogenesis in the liver, thereby reducing glucose production.(7)In addition, it increases insulin sensitivity, inhibits lipogenesis, increases glucose uptake in the gut and muscles, and slows gastric emptying, which in turn reduces appetite to food.(8) Both the American Diabetes Association and the European Association for the Study of Diabetes recommend metformin as an initial therapeutic approach in type 2 diabetes for its ability to increase peripheral insulin sensitivity, reduce cardiovascular mortality. take risks and promote weight loss.(9) Prescribing metformin is warranted in a variety of medical scenarios, as shown in Table 2, with precautions taken into account. Common side effects such as nausea, vomiting and diarrhea affect a significant percentage of patients, less common include headache, sweating, weakness and runny nose.(10).
VITAMIN B12
Cobalamin, generally known as nutrition B12, is a essential water-soluble nutrient containing cobalt, serving as a co-aspect for enzymes important in metabolism. diverse energetic forms of cobalamin, along with cyanocobalamin, hydroxocobalamin, methylcobalamin, and five-deoxyadenosine cobalamin (known as adenosyl-Cbl), are termed as diet B12. but, industrial merchandise provide special dosage types of the primary three types.(eleven) The physiologically active bureaucracy, adenosyl-Cbl and methylcobalamin, are produced intracellularly from all nutrition B12 paperwork. This nutrition is crucial for intracellular enzyme sports worried in DNA synthesis, amino acid, and fatty acid metabolism, together with helping erythropoiesis and the critical worried gadget.(12)
ABSORPTION OF VITAMIN B12
The absorption process of nutrition B12 is complicated and involves a couple of proteins and receptors. knowledge this multistep technique is crucial for greedy the relationship among nutrition B12 malabsorption and other medicines like metformin.(thirteen) nutritional nutrition B12 usually exists in a protein-bound shape, that is freed in the stomach due to gastric acid and pepsin. The released vitamin then binds to R-binder, a glycoprotein shielding it from belly acidity. Pancreatic proteases inside the duodenum ruin down R-binder, freeing nutrition B12. Intrinsic element (IF), released by means of stomach parietal cells, binds the diet to form the IF-nutrition B12 complex.(14) The IF-diet B12 complicated passes through receptor-mediated endocytosis within the terminal ileum, binding to the ileal cubilin receptor and keeping off degradation at the same time as performing as a service. Calcium plays a vital function in this interaction, enhancing the complex's affinity for the receptor. Upon endocytosis, the IF-nutrition B12-cubilin receptor complicated separates, with diet B12 getting into the cytoplasm after IF breakdown in the lysosome.(15) within the cytoplasm, nutrition B12 circulates sure to transcobalamin-I (TC-I) or TC-II proteins, with around 20%-30% sure to TC-II. those proteins shipping the diet to target tissues thru receptor-mediated internalization, facilitating absorption and utilization in various cellular processes.(16)
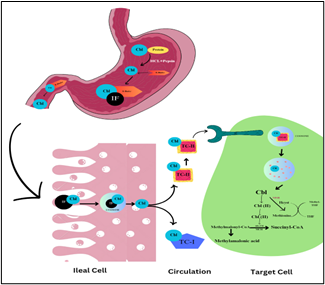
Fig 1: Mechanism of inhibition of vitamin B12 absorption by metformin
(Note : Ado-cbl - Adenosylcobalamin;ATR - Adenosyltransferase;Cbl Cobalamin;Hcyst - Homocysteine;IF Intrinsic factor; MCH - Methylmalonyl-CoA hydrolase;MCM - Methylmalonyl-CoA mutase;Me-cbl - Methylcobalamin;methyl-THF - Methyltetrahydrofolate;MSR - Methionine synthase reductase;TC-I-Transcobalamin-I;TC-II-Transcobalamin-II; THF-Tetrahydrofolate)
Epidemiology of Metformin-Induced Vitamin B12 Deficiency
The affiliation between metformin use and nutrition B12 deficiency has been drastically studied, dating back to the 1970s. A current systemic evaluate of 17 observational research located that 10 said substantially lower diet B12 degrees in metformin users with type 2 diabetes mellitus (T2DM).(17) Concurrent use of proton pump inhibitors or histamine H2-antagonists improved the chance by using 22%. studies display a dose-dependent decrease in serum nutrition B12 with metformin use, probable due to impaired absorption in the terminal ileum. but, the impact of nutritional intake on this dating remains uncertain. The excessive occurrence of T2DM and the morbidity rate of diet B12 deficiency with metformin use underscore the importance of know-how this issue.(18)
How Metformin Impacts on absorption of the Vitamin B12 ?
Metformin's impact on vitamin B12 absorption remains somewhat unclear, with multiple theories attempting to explain this phenomenon.(19) One possibility is that metformin disrupts the enterohepatic circulation of B12, alters hepatic storage, reduces intrinsic factor (IF) production, or slows intestinal motility, potentially leading to bacterial overgrowth. A widely accepted theory suggests that metformin interferes with calcium cations, preventing the calcium-dependent IF-vitamin B12 complex from binding to the ileal cubilin receptor, thus hindering vitamin B12 endocytosis. This interference may occur by altering the cubilin receptor's membrane surface charge, causing repulsion forces that push away calcium cations crucial for IF-vitamin B12 complex binding, ultimately resulting in vitamin B12 malabsorption.(20,21)
Symptoms of Vitamin B12 Deficiency :
Numerous observational and interventional studies have identified the correlation between chronic metformin usage and decreased vitamin B12 levels, and hence it was important to elucidate the clinical effects of this link.
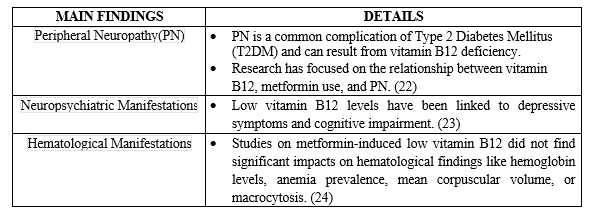
Table 1: Clinical symptoms of cobalamin deficiency
Management of Vitamin B12 Deficiency :
According to the MHRA guidelines, Vitamin B12 deficiency often afflicts those who are taking Metformin. The danger increases for both higher doses of the drug and longer periods of treatment, as well as in patients with certain risk factors for B12 insufficiency such as:
The management and treatment of cobalamin (vitamin B12) deficiency, especially in the context of metformin use, involve several key considerations and options:
The incidence of B12 deficiency among patients receiving metformin is significantly higher (about 2.5-fold) than it was in the past. This shortage set in as early as three months, whereas it may take up to five years or more for the liver’s B12 stores to become depleted.(27)
Metformin use over time has been found to be associated with an increased likelihood of developing B12 deficiency syndrome that varies according to dosage. There is a greater risk of developing vitamin B12 in people who have been extensively using metformin at higher doses e.g., 850 mg three times daily as seen in previous studies.
Management of B12 deficiency primarily revolves around supplementation. For instance, NICE (2022a) recommends regular 1mg intramuscular injection of hydroxocobalamin every three months for managing B12 deficiency.
An active form known as methylcobalamin can be taken orally or sublingually, so it is more effective than cyanocobalamin for those with neuropathy linked to a lack of cobalamin.
If oral therapy is used, you should check your level of vitamin B12 regularly at set periods such as every eight weeks until you are sure that treatment is going well.
Research supports the use of vitamin B12 supplements for both treatment and prevention purposes against metformin-induced deficiency and neuropathy among diabetic individuals taking metformin.Supplementation causes an increase(28,29,30)
Overall, the management of cobalamin deficiency involves supplementing with B12 in appropriate forms and doses, regular monitoring of B12 levels, and considering alternative forms like methylcobalamin for specific conditions like neuropathy.
CONCLUSION :
In conclusion, metformin-induced vitamin B12 deficiency presents a significant concern in the management of Type 2 Diabetes Mellitus (T2DM). Vigilant monitoring and supplementation with appropriate B12 forms are crucial to mitigate the risks associated with long-term metformin use. Future research should focus on refining supplementation protocols and evaluating long-term outcomes to optimize patient care and minimize complications. Enhanced awareness and proactive management strategies are essential for improving the overall health outcomes of individuals with T2DM on metformin therapy.
REFERENCE:
Sai Shashank Gudla, Metformin-Induced Cobalamin Deficiency: A Comprehensive Review And Management Strategies, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 4, 1192-1198. https://doi.org/10.5281/zenodo.11080459
 10.5281/zenodo.11080459
10.5281/zenodo.11080459
