Rashtrasant Janardhan Swami College of Pharmacy, kokamthan, Ahmednagar, Maharashtra- 414001
Chronic obstructive pulmonary disease (COPD) remains a leading cause of death worldwide, yet only one new drug class has been approved in the last decade. However, a recent surge in COPD treatment has been fueled greater understanding of the pathophysiology and natural history of the disease, as well as a growing prevalence and a population that is aging. Currently, there are nearly 25 novel drug targets in development. Furthermore, the indication has undergone some fundamental changes over the last couple of years, including an updated diagnosis paradigm, validation, and approval of patient-reported outcome questionnaires for clinical trials, and drug development tools, such as a prognostic biomarker for patient selection. In the context of clinical trials, this review aims to summarize recent changes to the diagnosis and evaluation of COPD and to provide an overview of US and European regulatory This review provides a concise overview of the literature regarding the impact of COPD exacerbations on both the patient and the healthcare system, the recommendations for pharmacologic management of COPD and the methods used to provide better care to patients and cut down on hospitalizations and readmissions guidance. Chronic obstructive pulmonary disease (COPD) continues to be a chronic and progressive illness in spite of significant advances in treatment. frequently results in premature death. COPD is associated with a constellation of significant symptoms, including dyspnea, cough, wheezing, pain, fatigue, anxiety, depression, and insomnia, and is associated with increased morbidity. Palliative care is appropriate to support these patients. However, historically, palliative care has focused on supporting patients with malignant disease, rather than progressive chronic diseases such as COPD. Therapies for COPD often result in functional and symptomatic improvements, including health-related quality of life (HRQL), and palliative care may further improve symptoms and HRQL. Provision of usual palliative care therapies for this patient population requires understanding the pathogenesis of COPD and common disease- targeted pharmacotherapies, as well as an approach to balancing life-prolonging and HRQL care strategies.This Review Describes COPD And Current Targeted Therapies and Their Effects on Symptoms, Exercise Tolerance, HRQL, And Survival
Despite significant advances in treatment, chronic obstructive pulmonary disease (COPD) remains a chronic and progressive disease associated with significant morbidity and premature mortality.1 COPD is also associated with significant symptom burden. Palliative care is appropriate to support these patients. However, palliative care historically has focused on supporting patients with malignant disease Clinicians are not traditionally trained to manage patients utilizing a with progressive chronic diseases like COPD palliative approach. In addition, patients with COPD may often not be referred to palliative care. This review is specifically targeted to clinicians that will be providing a palliative approach to COPD patient care and require further information to support the balance of life-sustaining or disease-targeted therapies and care that can improve quality of life. These clinicians need to understand disease-targeted therapy and how it works in conjunction with or hinders symptomatic optimization. To do this, we describe COPD and current targeted therapies and more specifically, their effects on symptoms, exercise tolerance, health-related quality of life (HRQL), and survival (highlighting data from randomized controlled trials and systematic reviews). Additionally, we offer a comprehensive summary of pharmacologic interactions and highlight precautions to be taken with commonly used palliative care medications analyzed using Lexi-comp Interaction analysis, and medication monographs coupled with expert opinion.
COPD Epidemiology and Symptom Burden
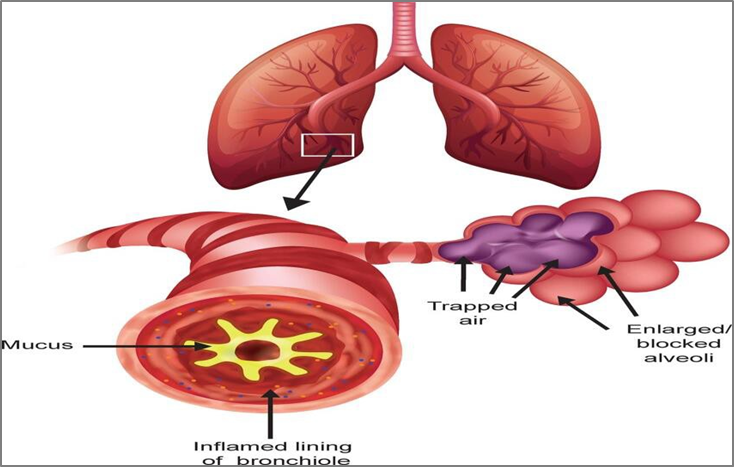
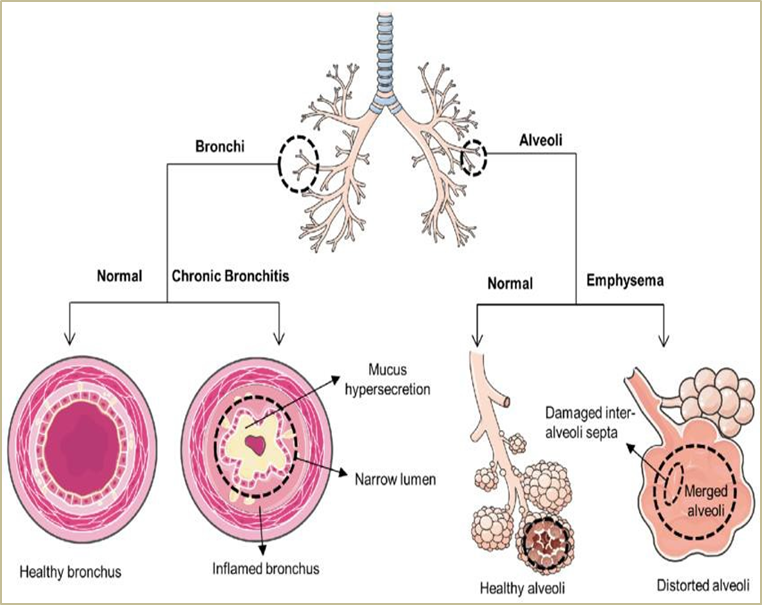
COPD is a common and progressive respiratory disorder that encompasses patients with chronic bronchitis and emphysema. It is currently the fourth leading cause of death in the world; it is projected to rise to the third most common cause of death by 2020. It is also associated with high rates of health care utilization characterized by frequent office visits and hospitalizations because of acute exacerbations Chronic bronchitis refers to a productive cough for three months in each of two successive years in a patient in whom other causes of chronic cough (e.g. bronchiectasis) have been excluded. Emphysema is a pathological term that describes abnormal and permanent enlargement of the airspaces distal to the terminal bronchioles, and destruction of the airspace walls, without obvious fibrosis.
Either of these features can be present in the absence of significant airflow limitation. As per Global Initiative for Chronic Obstructive Guidelines for Lung Disease (GOLD), spirometry is required to make the diagnosis of COPD. The presence of a post bronchodilator ratio of forced expiratory volume in the first second (FEV1) to forced vital capacity (FVC) (FEV1/FVC) <0.70 or that below the lower limit of normal confirms the presence of persistent airflow limitation. Classification of airflow limitation severity is quantified by FEV1. For example, GOLD 1, or mild air flow limitation, is quantified as FEV1 >80% predicted, and GOLD 4, or very severe air flow limitation, is quantified as FEV1 <30% predicted. Risk factors for COPD include both environmental and host factors. The most common risk factor for COPD is chronic exposure to tobacco smoke. Other risk factors from the environment that harm the airways and lung tissue includes occupational exposures. (e.g., dusts or chemicals) or smoke from cooking and heating fuels. Host factors include genetics, airway hyper-responsiveness, and poor lung development during childhood. Patients with COPD have a significantly higher symptom burden than patients with cancer or heart failure. The three cardinal symptoms of COPD are dyspnea, chronic cough, and sputum production with the most common early symptom being exertional dyspnea. Patients may also experience wheezing, pain, anxiety, depression, insomnia, and other symptoms. Several studies and texts have explored the management of these symptoms and can offer strategies to readers who are interested, but this is not the focus of this article. Disease Course. Although COPD is both a preventable and manageable condition, it remains a leading cause of morbidity and mortality worldwide. A wide variety of factors may influence disease severity and prognosis, including airway hyper-responsiveness, infection (e.g., atypical mycobacterial infection, respiratory viral infection), decreased exercise capacity, age, gender/ sex, weight loss/anorexia, hospitalization (s) for COPD exacerbation, and the presence of other comorbidities. COPD Assessment and Prognostication Tools. A number of tools exist to evaluate symptoms and prognosis for patients with COPD. These include the ABCD assessment tool, BODE index, GOLD staging, modified Medical Research Council dyspnea scale, COPD assessment test, and other multidimensional indices. Despite a number of prognostic tools, the disease trajectory for patients with COPD typically is variable and unpredictable. Physicians continue to find prognostication and identification of individuals who have less than a few months of life to be challenging
Diagnosing COPD
Maximum lung function is found in individuals who are healthy and never smoke. typically reached by early adulthood and remains at a constant level over the subsequent ten years, and then gradually decreases with age. In Lung function declines in those who are susceptible to the effects of smoking. at an accelerated rate resulting in development of respiratory symptoms, which may prompt clinical assessment and a diagnosis of COPD. However, the consequences of smoking vary and include factors, including early life events, may influence optimal lung growth. In a landmark prospective study by Lange combining datasets from the Lovelace Smokers cohort, Framingham Offspring cohort, and Copenhagen City Heart study, found that approximately half of individuals subsequently diagnosed with COPD had low forced expiratory volumes in 1 second (FEV1) as young adults. This suggests that some early life events contributed to these patients failing to reach maximal potential lung growth, resulting in lasting airflow limitations and COPD. Spirometry can be used to measure airflow, which is typically expressed as FEV1% predicted, relative to the average FEV1 in the population for any person of similar age, sex, and body composition. compelled vital capacity (FVC) refers to the volume of air forcibly exhaled in one breath from the point of maximal inspiration. Both measurements are usually evaluated by comparison to reference values based on age, height, sex, and race After administration of a bronchodilator, the ratio of both measurements (i.e., FEV1/FVC) is calculated A ratio of <0.7 confirms airflow obstruction and, therefore, suggests COPD. With, airways can be opened, bronchodilation can be achieved. either a short-acting β2-adrenoreceptor agonist or short-acting anticholinergics, or combined medications for this procedure. When an FEV1/FVC <0.7 is determined, severity of airflow limitation in COPD is then assessed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) system. Based on predicted FEV1 There are four levels of GOLD: mild (GOLD 1), 50%–79%, and moderate (GOLD 2), severe (GOLD 3), and less than 30% groups that are very severe (GOLD 4) The GOLD system is widely applied for COPD staging, however some national respiratory societies use slightly different FEV1 cutoffs Although the GOLD stages 1–4 are used to describe the severity of airflow limitation and represent important cutoffs for clinical study inclusion/exclusion criteria, this patient characterization based on FEV1 alone lacks sufficient precision to predict those at risk of adverse outcomes, including disease exacerbations or mortality and to adequately guide treatment decisions. Therefore, the GOLD consortium issued a combined approach for COPD grading in 2017. In this paradigm, patients undergo spirometry to determine severity of airflow limitation (which helps define prognosis) and are assessed for severity of symptoms and history of exacerbations. The best predictor of future exacerbations is a history of treated exacerbations.
Frequent exacerbators are defined as those reporting two or more per year or at least one requiring hospitalization or an emergency department visit. The COPD Symptom Assessment Tool and the COPD Assessment Test or the modified Medical Research Council questionnaires.
COPD Assessment Test is an eight-item questionnaire with a total score of that captures information regarding health status and the modified Medical Research Council is a 4-grade scale for breathlessness. Based on these outcomes, patients are categorized into four GOLD grades A−D reflecting symptom burden and exacerbation risk The GOLD grades are intended to guide clinician treatment decisions as well as pharmacological therapy escalation and de-escalation if required
Management of COPD
Stable COPD. Reduction in the possibility of escalation, in addition to symptom management, is the cornerstone of the current strategy for management of COPD.1
|
Class |
Subclass |
Examples |
Purpose |
|
Bronchodilators |
Beta-2 Adrenergic Agonists |
SABA: Salbutamol, Terbutaline LABA: Salmeterol, Formoterol, Indacaterol |
Relax airway smooth muscles |
|
|
Anticholinergics (Muscarinic Antagonists) |
SAMA: Ipratropium LAMA: Tiotropium, Aclidinium, Glycopyrronium |
Block muscarinic receptors to reduce bronchoconstriction |
|
|
Methylxanthines |
Theophylline, Aminophylline |
Mild bronchodilation and anti-inflammatory effect |
|
Anti-inflammatory Agents |
Corticosteroids |
ICS: Budesonide, Fluticasone Oral: Prednisone, Methylprednisolone |
Reduce airway inflammation |
|
|
PDE-4 Inhibitors |
Roflumilast |
Decrease inflammation via cAMP modulation |
|
Combination Therapies |
LABA + ICS |
Salmeterol + Fluticasone Formoterol + Budesonide |
Dual bronchodilation and anti-inflammation |
|
|
LAMA + LABA |
Tiotropium + Olodaterol |
Enhanced bronchodilation |
|
|
Triple Therapy |
Trelegy Ellipta (LAMA + LABA + ICS) |
Maximum symptom control |
|
Antibiotics |
- |
Azithromycin, Doxycycline |
Treat infections during exacerbations |
|
Mucolytics |
- |
N-acetylcysteine, Carbocisteine |
Thin mucus and aid clearance |
The main components of COPD management are appropriate medication (that) addresses both management of symptoms and exacerbation prevention), promotion of smoking cessation, pulmonary rehabilitation, and regular follow-up monitoring for disease progression. The GOLD ABCD tool combines the severity of the symptoms, using either COPD Assessment Test score or the restructured Medical Research Council scale, as well as the risk of an exacerbation, determined by either spirometry defined airflow limitation or exacerbation history, to categorize patients into disease “risk stratification” groups ABCD to guide pharmacotherapy Bronchodilators play a crucial role in management of COPD at all levels of severity. GOLD recommends specific treatment options for the initial therapy upon diagnosis of COPD in patients according to the ABCD classification they were given. This initial therapy differs from the follow-up treatment, which is based on current medication(s) and the most treatable trait (e.g., dyspnea or exacerbation)
Bronchodilators
Bronchodilators are the mainstay of pharmacological treatment of COPD. Two classes of bronchodilators can be distinguished: β2-adrenoreceptor agonists and muscarinic antagonists. The β2-adrenoreceptor agonists stimulate airway smooth muscles to induce bronchodilation. Although their anti-inflammatory Adapted from GOLD guidelines granting permission. COPD, chronic obstructive pulmonary disease; CAT, COPD Assessment Test ICS stands for inhaled; GOLD stands for the Global Initiative for Chronic Obstructive Lung Disease. corticosteroid; LABA, long-acting β2-adrenoreceptor agonist; LAMA, long acting muscarinic antagonist; mMRC, modified Medical Research Council properties have been postulated to contribute to their efficacy in COPD treatment, this has not been proven to be relevant for the clinical setting. Muscarinic receptors affect bronchial motor tone and mucus secretion through the cholinergic system by coupling to G-proteins Gαq/11 (M1, M3, and M5 receptor subtypes) or Gαi/o (M2 and M4 receptor subtypes). Despite M2 receptors indirectly affect airway smooth muscle contraction, M3 receptors dominantly contribute to relaxation and dilation of airway smooth muscles. M3 receptors also mediate cholinergic effects on mucus secretion. Selective M3- muscarinic receptor inhibition improves bronchodilation as well as mucus production. GOLD class A patients are typically well managed on either a short-acting or long-acting bronchodilator depending upon their symptoms. GOLD class B patients may start on a single long-acting β2-adrenoreceptor (LABA) or long-acting muscarinic antagonists (LAMA). If symptoms of breathlessness persist on monotherapy, they may be escalated to dual therapy with LABA and LAMA treatments. Patients with GOLD class C (currently defined as relatively low symptom burden but high exacerbation risk) often start on an LAMA and advance to LABA + LAMA upon further exacerbations. Combined treatment with LABA and inhaled corticosteroids (ICS) can also be considered. Finally, LABA + LAMA is a recommended starting therapy for GOLD class D patients. In patients who develop further exacerbations, the guideline recommends considering escalation to triple therapy (LAMA + LABA + ICS or switching to LABA + ICS). lists the maintenance COPD medication approved in the European Union and the United States. Triple therapy has been shown to have favorable characteristics compared with single LAMA or dual LAMA + LABA or LABA + ICS therapy, and its use is currently also under consideration for patients with less severe COPD or selected phenotypes.
Glucocorticoids
ICS can provide anti-inflammatory activity; however, they may also increase the risk of pneumonia in some patients among other adverse events. Current GOLD recommendations suggest peripheral blood eosinophil counts may be used as a biomarker to guide use of ICS therapy for exacerbation prevention. Based on clinical trial evidence, patients with peripheral eosinophil counts > 300 cells per microliter (μL) may be best offered LABA + ICS as first choice for preventions of exacerbations. Once COPD symptoms are stable, withdrawal of ICS can be considered. This de-escalation stems from results from the Withdrawal of Inhaled Steroids during Optimized Bronchodilator Management (WISDOM) trial. WISDOM was a large 52-week randomized controlled trial that investigated the stepwise withdrawal of an ICS from triple therapy (LAMA: tiotropium + LABA: salmeterol + ICS: fluticasone) in patients with severe or very severe COPD. The results demonstrated noninferiority compared with continuation of all three therapies with respect to risk of moderate or severe exacerbations.
Phosphodiesterase type 4 inhibitor
Roflumilast is the latest “add-on” COPD treatment to gain approval Roflumilast is a phosphodiesterase type 4 inhibitor indicated for GOLD group D patients with chronic bronchitis. PDE4 antagonism lowers pro-inflammatory response, reduces mucus secretion, and decreases tumor necrosis factor alpha (TNF-α) expression, a cytokine associated with airway remodeling. In clinical studies, Roflumilast improved FEV1 to a similar degree as treated with ICS; however, due to gastrointestinal side-effects as well as substantial weight loss and potential psychiatric symptoms, it is indicated as an add-on therapy in patients with advanced COPD.
Other COPD treatments
In addition to the maintenance medication, there are also exacerbation treatments and preventative therapies (e.g., influenza and pneumococcal vaccines) not captured in the COPD treatment algorithm depicted. Non-pharmacological treatments include physical activity, pulmonary rehabilitation, oxygen therapy, and lung a surgery to reduce the volume. Smoking cessation is also recommended to prevent further disease progression. Supportive tools for smoking cessation include counseling programs as well as for tobacco dependence. Varenicline is an effective drug to help quit smoking. Nicotine patches, lozenges, and other non-combustible cigarettes, such as electronic cigarettes (E-cigarettes), may also aid smokers attenuate their habit or at least reduce exposure to toxic and carcinogenic chemicals found in traditional cigarettes.
CONCLUSION:
COPD exacerbations, particularly those that require ED visits or hospitalization, lead to substantial economic burden. The quality of life of patients who experience frequent exacerbations decreases, and their disease progresses more quickly. Appropriate therapy with maintenance bronchodilators has been shown to reduce exacerbation frequency but is underused, highlighting a need for in-creased awareness of treatment recommendations among treating physicians, prescribers, and healthcare organizations in which patient care could be improved. Several studies have found that COPD aftercare programs that in-crease patient support are beneficial in improving outcomes and reducing hospitalizations. It has been demonstrated that programs that include pulmonary rehabilitation, patient education and inhaler technique training, referrals to pulmonologists, and appropriate maintenance therapy can improve the lives of patients who experience frequent exacerbations. This demonstrates that better outcomes can be achieved by continuing the shift toward integrated COPD care.
REFERENCES





Shivam Limbore*, Varad Lad, Shubham Pathak, Akshay Nikhade, Bankar Ganesh, Management of Chronic Obstructive Pulmonary Diseases, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 3224-3231. https://doi.org/10.5281/zenodo.15286997
 10.5281/zenodo.15286997
10.5281/zenodo.15286997
