1 Department of Biotechnology, KG College of Arts and Science, #365, Thudiyalur Road, Saravanampatti, Coimbatore-641035, TN, India???????
2 Narayana Netheralaya, Bommasandra, Bangalore
3 Division of Microbiology, ICMR-RMRC, Dolligunj, Port Blair-744103, S. Andaman
Liver-targeted viral infections increase intensive systemic results beyond liver injury, highlighting the recognized effect on ocular health with emerging evidence. As a central centre of liver, immune and metabolic regulation, immune intricate statements, cytokine dysregulation and neuroimmune interactions affect distant organs including the eye. Chronic hepatitis B virus (HBV) infection has been linked to uveitis, optic neuritis and retinopathy through autoimmune and vascular passages, while hepatitis C virus (HCV) is usually manifested with dry eye, scleritis and cryoglobulinemia-associated retinopathy`. Hepatitis E virus (HEV), although usually implicated in rare cases of self-limiting, optic neuropathy and neuroretinitis, suggested para-infectious demyelination. Hepatitis D virus (HDV), often in coincidence with HBV, is poorly characterized in relation to the ocular sequelae, underlining the need for systematic monitoring. Arboviral hepatotropic infections such as dengue and yellow fever can provoke retinal bleeding, vascularis, and macular edema through cytokine storms, endothelial dysfunction and coagulopathy. Despite these associations, diagnostic challenges remain due to overlapping presentations with autoimmune and infectious eye diseases, mixed by limited interdisciplinary awareness. Animal models are beginning to highlight, high-resolution ocular imaging, and omics -based profiling liver and the immunological crosstalk between the eyes. Medically, antiviral agents, immunosuppressive regimens, and emerging biologics promise, while individual approaches can refine management to integrate genetic and cytokine biomarkers. Identifying the liver–eye axis is crucial for early detection, prevention of irreversible vision loss, and the development of holistic therapeutic strategies in viral hepatology.
The viral infections of the liver represent a major global health burden with hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis E virus (HEV), and other hepatotropic viruses, which contribute significantly to chronic liver disease, cirrhosis, hepatocellular carcinoma and death rate. The World Health Organization (WHO) estimates that more than 350 million people are infected with HBV and HCV to about 58 million, while HEV is spatial in Asia and Africa, often causes acute outbreaks (WHO, 2023; Polaris Observatory, 2022). The primary clinical emphasis in these infections has traditionally been on liver injury, liver failure and related systemic complications. However, in the last two decades, it has become increasingly clear that these viruses are not limited to the liver and can have significant additional effects through direct viral invasion, immune-medieval routes, or toxicity associated with treatment (Koizumi et al., 2016).
Between these additional manifestations, hepatotropic viral infections have no comparatively low comparatively less comparatively to the cause of irreversible vision loss compared to ocular complications. Clinical studies have described a spectrum of ocular participation: HBV has been linked to uveitis retina vasculitis and optic neuritis (Koizumi et al., 2007); HCV infections are often presented with ischemic retinopathy, keratoconjunctivitis sicca (Dry Eye syndrome), and interferon-related retinopathy (Zegans & Anninger, 2005; Cacoub et al., 2012). HEV has been paired with optic neuropathy and neuralgic amyotrophy with visual sequelae (Dalton et al., 2016). In addition, the introduction of direct-intelligent antiviral (DAAs), while revolutionary in reducing liver sickness and viral perseverance, has raised new concerns about drug-induced ocular poisoning (Kandula et al., 2019). These findings underline viral firmness, host immune reactions, systemic swelling and treatment, which gives diet in shaping ocular results.
Despite submission of case reports and small cohort studies, the pathophysiological links between liver-targeted viral infections and ocular damage. Current evidence suggests that immunity can play an important role in complex statements, molecular mimicry, and chronic systemic inflammation, but the exact mechanisms viral pathogens (Rosenberg et al., 2015). Genetic susceptibility factors, including variations in host immune-regulatory genes and ocular tissue-specific responses, are only beginning to be explored (Mousa et al., 2020). This knowledge gap represents a major obstacle for clinicians, as ocular complications are often diagnosed late or misattributed, resulting in preventable vision loss.
The need for this review is therefore twofold. First, the liver-targeted viral diseases provide to physicians and researchers with their epidemiology, clinical features, and a consolidated understanding of the underlying mechanisms, to synthesize the ocular manifestations of viral diseases. Second, to identify emerging therapeutic strategies that can reduce vision loss in affected patients, including host-targeted antiviral, anti-inflammatory biology and new drug distribution system, designed to reduce ingredients. By integrating approaches to hepatology, ophthalmology, virology and immunology, the purpose of this review is to bridge a significant difference in translation medicine.
The scope of this article will include: (i) observations of major hepatotropic viral infections with attention to HBV, HCV and HEV; (ii) His known and emerging ocular expressions; (iii) molecular and immunological systems associate liver infections with ocular pathology; (iv) role of antiviral therapy and their ocular side effects; And (v) Current and future therapeutic goals to prevent vision loss. Ultimately, this synthesis tries to guide future research towards raising awareness among physicians, informing public health preferences and protecting vision in the population affected by viral liver diseases.
Pathophysiological Basis of the Liver–Ocular Axis
The eye and liver, although physically different, share intimate systemic, metabolism and immunological connections that explain the occurrence of occupants in liver-targeted viral diseases. Understanding this liver–ocular axis requires recognition of the systemic role of the liver as a central metabolic hub, which its regulation of immune homeostasis and neuroimmune network that integrates liver and ocular physiology.
Systemic effect of liver
The liver is a primary site of protein synthesis, lipid metabolism, anxiety and immune regulation. Hepatic dysfunction arising from chronic viral infections transforms these systemic functions in ways that affect the eye. For example, impaired synthesis of albumin and clotting factors contributes to retinal vascular delicate and bleeding (López-Serrano et al., 2013). Dysregulated bile acid metabolism and hyperbilirubinemia can also accumulate toxic metals in ocular tissues, which can lead to scleral icterus and keratopathy (Friedman, 2010). In addition, viral hepatitis promotes lipid metabolism and systemic oxidative stress endothelial dysfunction, which predetermines for retina ischemia (Zeng et al., 2019).
Immune and inflammatory mediators
The liver is central for congenital and adaptive immunity, the large population of Kupffer cells, natural killer cells and antigen-pregnancy cells habitat. Hepatotropic viral infections induce chronic immune activation, resulting in systemic inflammation and circulating immune complexes. These immune complexes can deposit in the ocular vascular, trigger uvitis, retina vasculitis or optic neuritis (Cacoub et al., 2016 a, b). Tumor necrosis factor-α (TNF-6), Interlucin-6 (IL-6), and Interferon-6 (IFN-γ) released during viral hepatitis can disrupt the blood-rituals, blood-rituals, and promote leukocyte infiltration leading to retinopathy (Gupta et al., 2017). In addition, the interferon-based antiviral therapy, historically used for HCV infection, is well documented to cause interferon-associated retinopathy, characterized by cotton wool's spots and retina bleeding caused by endothelial injury (Zegans & Anninger, 2005 Even with direct-acting antivirals (DAAs), immune reconstitution and off-target inflammatory responses may play roles in ocular side effects (Kandula et al., 2019).
Metabolic and Vascular Pathways
Hepatic viral infection often coexists with metabolic dysregulation, including insulin resistance and dyslipidemia. These systemic metabolic disturbances can accelerate microvascular injury, leading to increased sensitivity to retinal microangiopathy and ischemic optic neuropathy (Cheung et al., 2010). Chronic hepatitis C, in particular, is associated with metabolic syndrome, which shares the pathophysiological route with diabetic retinopathy (Adinolfi et al., 2016). Vascular endothelial dysfunction mediated by nitric oxide imbalance, oxidative stress, and prothrombotic states in chronic liver disease can directly compromise ocular perfusion, further linking the metabolic role of the liver with retinal pathology (Forbes & Newsome, 2016).
Neuroimmune Interactions
An emerging concept in the liver–ocular axis is the role of neuroimmune signaling. The liver communicates with the central nervous system via vagal and sympathetic pathways, which modulate systemic immune responses. The hepatic inflammatory vagus–splenic–retinal immune circuit, leading to an increase in cytokine trafficking that can affect the eye’s immune microenvironment (Tracey, 2009). In addition, viruses such as HEV and HCV have demonstrated neurotropic capacity, detected viral RNA in nerve tissues, which extends the possibility of direct viral spread through the neuroimmune pathways to optic nerve and retina (Dalton et al., 2016; Fletcher et al., 2012). Neuroinflammation triggered by viral persistence in the liver can therefore contribute secondarily to optic neuropathy and retinopathy.
Integrative Model of the Liver–Ocular Axis
Taken collectively, the pathophysiological foundation of the liver–ocular axis includes a multifactorial interplay
This integrative framework highlights that imaginative and prescient loss in liver-centered viral infections is not an remoted phenomenon however as an alternative a systemic outcome of complicated metabolic, immune, and neuroimmune interactions.
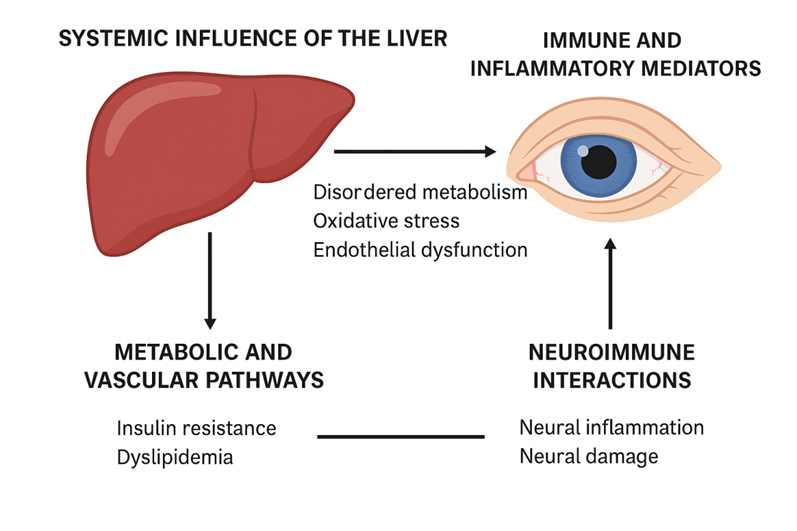
Figure 1. Pathophysiological foundation of the liver–ocular axis.
The diagram illustrates the systemic, immune, metabolic, and neuroimmune pathways linking the liver and the eye in liver-focused viral infections. Hepatic dysfunction leads to disordered metabolism, oxidative pressure, and endothelial injury that compromise ocular homeostasis. Immune and inflammatory mediators, such as cytokines and immune complexes, make contributions to retinal vasculitis, uveitis, and optic neuropathy. Metabolic and vascular alterations inclusive of insulin resistance and dyslipidemia boost up microvascular harm, predisposing to retinopathy. Neuroimmune interactions regarding hepatic inflammation and vagal signaling promote neural infection and optic nerve damage. Together, these interconnected mechanisms give an explanation for how hepatotropic viral infections can happen with imaginative and prescient-threatening ocular headaches.
Liver-Targeted Viral Infections and Their Ocular Manifestations - Discussion
HBV- Chronic HBV can cause ocular infection ranging from anterior uveitis to retinal vasculitis and optic neuritis. Immune-complicated–mediated vascular injury and autoimmune cross-reactivity are the leading hypotheses, regular with extra-hepatic immune phenomena in HBV. Case reviews describe optic neuritis or optic neuropathy temporally connected to active HBV and improvement with immunomodulation or plasma trade, helping an immune mechanism in place of direct viral invasion.
HCV- HCV has one of the richest ocular phenotypes among hepatotropic viruses: keratoconjunctivitis sicca from exocrine involvement, ischemic retinopathy and retinal hemorrhages, scleritis, and interferon-associated retinopathy. Mixed cryoglobulinemia—classically related to HCV—drives small-vessel immune-complicated vasculitis and might involve the retinal microcirculation. Contemporary evaluations additionally note that even in the DAA technology, cryoglobulinemic vasculitis may persist and threaten imaginative and prescient.
HEV- Although more often than not an acute hepatitis, HEV indicates neurotropism with a spectrum of neurologic headaches (e.g., neuralgic amyotrophy, meningoencephalitis). Ocular reviews are uncommon however neuro-ophthalmic manifestations such as optic neuropathy/neuroretinitis are biologically plausible within the broader HEV neuro-immune spectrum. Clinicians must bear in mind HEV trying out in acute optic neuropathies with concomitant hepatitis or recent systemic contamination.
HDV (with HBV)- HDV amplifies hepatic irritation and immune activation in HBV coinfection. Published ocular data are sparse; the probable hazard is oblique—heightened systemic inflammatory/ immune-complicated burden elevating the hazard of uveitis or retinal vasculitis. This is a true literature gap that warrants prospective surveillance in HBV/HDV cohorts. (Inference primarily based at the paucity of HDV-ocular reports in recent critiques of liver–eye links.)
Arboviral hepatotropic infections (Dengue/ Yellow fever)- Dengue normally causes “post-fever” posterior uveitis with retinal hemorrhages, vasculitis, cotton-wool spots, macular edema, and now and again neuroretinitis. Proposed drivers are cytokine surge, endothelial disorder, immune-complicated deposition, and brief coagulopathy-constant with systemic vascular leak and hepatic involvement seen in severe dengue. Yellow fever information are extra restrained but fall along comparable inflammatory/ vascular strains is proven in Figure 1
Clinical implications- Across pathogens, patterns recur: (1) immune-complicated/ vasculitic damage of retinal/ optic nerve microvasculature (HBV, HCV, arboviruses); and (2) neuro-immune/ neurotropic contributions (HEV; from time to time HCV). Practical steps include: screening for dry eye and posterior segment modifications in persistent HCV; pressing workup for vasculitis or optic neuritis in HBV/HEV patients with visual signs and symptoms; and OCT/OCTA and fluorescein angiography in dengue-endemic settings after febrile contamination. Early recognition allows timely corticosteroid or immunomodulatory remedy in immune-mediated instances, along pathogen-specific antiviral/ supportive care in Table 1.
Immunological Crosstalk among Liver and Eye
The liver and the attention are two immunologically privileged organs with finely tuned tolerance mechanisms, however hepatotropic viral infections disrupt this stability, triggering move-organ immune injury.
Autoimmune Mechanisms- Hepatotropic viral infections (HBV, HCV, HEV) can induce molecular mimicry, in which viral epitopes resemble ocular self-antigens, main to autoimmune uveitis or optic neuritis. Immune complex deposition (notably in HBV and HCV) in ocular microvasculature promotes vasculitis and retinopathy. Autoantibodies against retinal and optic nerve proteins have been detected in HCV-related ocular inflammation (Figure 2).
Cytokine Profiles- Viral hepatitis elevates IL-6, TNF-α, IL-1β, and IFN-γ, which pass the blood-retinal barrier, using retinal vasculitis and neuroinflammation. IL-17 and Th17 cells, enriched in continual viral hepatitis, extend autoimmune-mediated ocular pathology. Elevated VEGF and chemokines (CXCL10, CCL2) contribute to vascular leakage and retinal edema.
Immune Cell Involvement- CD8+ T cells activated in hepatic viral infection infiltrate ocular tissues, detrimental photoreceptors and retinal ganglion cells. Regulatory T cells (Tregs) typically keep ocular immune privilege however end up dysregulated in continual hepatitis, facilitating inflammatory eye sickness. Kupffer cellular activation in the liver triggers systemic macrophage and dendritic cellular activation, which contributes to ocular infection.
Table 1. Liver-centered viral infections and their ocular manifestations.
|
Virus |
Liver Pathology |
Ocular Manifestations |
Mechanism Proposed |
Case/Series Evidence |
|
HBV |
Chronic hepatitis, fibrosis |
Uveitis, optic neuritis/ neuropathy, retinopathy |
Immune-complex vasculitis; autoimmunity |
Optic neuritis/ neuropathy cases linked to HBV, responsive to immunotherapy/ plasma exchange. |
|
HCV |
Steatosis, cirrhosis |
Dry eye, retinopathy, scleritis; IFN-retinopathy (historical) |
Mixed cryoglobulinemia; immune-complex vasculitis; possible direct/ para-infectious effects |
Reviews and series on HCV ocular disease and cryoglobulinemia-related eye involvement. |
|
HEV |
Acute viral hepatitis |
Optic neuropathy, neuroretinitis (rare) |
Autoimmune demyelination / para-infectious neuro-inflammation |
Reviews of HEV neurological disease; sporadic neuro-ophthalmic reports. |
|
HDV (with HBV) |
Coinfection/ superinfection; severe hepatitis |
Rare/under-reported |
Severe hepatic–systemic immune activation; potential ocular vasculitis |
Documented literature gap in ocular reports; merits targeted surveillance. |
|
Dengue / Yellow fever |
Hepatic injury; failure (severe cases) |
Retinal hemorrhage, vasculitis, macular edema; neuroretinitis (dengue) |
Cytokine storm; endothelial dysfunction; coagulopathy; immune complexes |
Systematic and narrative reviews; post-fever retinitis literature., |
This desk summarizes key hepatic viruses and their related ocular headaches, emphasizing underlying liver pathology, spectrum of eye involvement, proposed pathophysiological mechanisms, and clinical proof. HBV and HCV show properly-documented immune-mediated ocular injury, at the same time as HEV offers rare but vision-threatening neuro-ophthalmic headaches. HDV stays underreported, highlighting a essential literature hole. Arboviral infections inclusive of dengue and yellow fever, although frequently systemic, often involve the retina via cytokine-mediated irritation and vascular injury.
Cytokine Profiles- Viral hepatitis elevates IL-6, TNF-α, IL-1β, and IFN-γ, which pass the blood-retinal barrier, using retinal vasculitis and neuroinflammation. IL-17 and Th17 cells, enriched in continual viral hepatitis, extend autoimmune-mediated ocular pathology. Elevated VEGF and chemokines (CXCL10, CCL2) contribute to vascular leakage and retinal edema.
Immune Cell Involvement- CD8+ T cells activated in hepatic viral infection infiltrate ocular tissues, detrimental photoreceptors and retinal ganglion cells. Regulatory T cells (Tregs) typically keep ocular immune privilege however end up dysregulated in continual hepatitis, facilitating inflammatory eye sickness. Kupffer cellular activation in the liver triggers systemic macrophage and dendritic cellular activation, which contributes to ocular infection.
Microbiota and Gut–Liver–Eye Axis- Hepatotropic viruses modify gut microbiota, resulting in translocation of microbial metabolites and endotoxins. Dysbiosis promotes systemic irritation and changed bile acid signalling, each related to ocular surface sickness (dry eye) and retinal immune activation. Recent studies suggest that microbial metabolites (short-chain fatty acids) modulate ocular immune tolerance, making the gut–liver–eye triad a key therapeutic target.
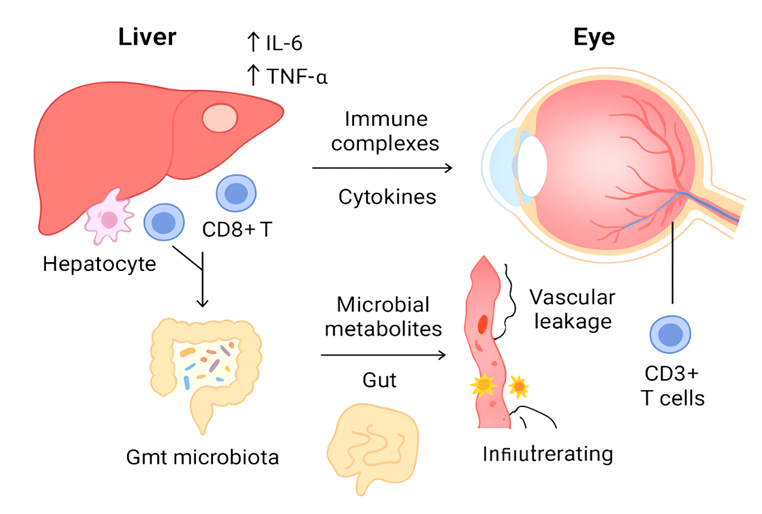
Figure 2. Immunological crosstalk between the liver and the eye in viral infections
The schematic highlights the bidirectional immune interactions linking hepatotropic viral infections to ocular pathology. Viral infection of the liver activates Kupffer cells and hepatocytes, leading to the release of pro-inflammatory cytokines (IL-6, TNF-α, IFN-γ) and chemokines into systemic circulation. Circulating immune complexes and activated T and B cells migrate to ocular tissues, where they trigger uveitis, retinal vasculitis, and optic neuropathy. Dysregulated regulatory T cells (Tregs) and heightened Th1/Th17 responses amplify autoimmune-mediated ocular injury. The gut–liver–eye axis, modulated by microbiota dysbiosis, further shapes immune responses through microbial metabolites and endotoxins, contributing to chronic inflammation and ocular surface disease. Together, these mechanisms demonstrate how hepatic immune dysregulation extends beyond the liver to cause vision-threatening complications (Maslennikov R, et al 2021)
Diagnostic and Clinical Challenges
The reputation of ocular manifestations in patients with liver-centered viral infections offers full-size diagnostic and medical difficulties. First, the ocular headaches are frequently diffused or nonspecific, together with uveitis, keratoconjunctivitis sicca, or retinopathy, which can be misattributed to not unusual ophthalmic conditions consisting of diabetic retinopathy, autoimmune uveitis, or age-related macular degeneration. The overlap of scientific signs and symptoms complicates timely prognosis, specifically in areas with a excessive history incidence of other ocular pathologies.
Another challenge lies in differentiating whether or not the ocular involvement arises from the virus itself, immune-mediated processes, or damaging consequences of antiviral therapy. For example, interferon-brought about retinopathy in HCV patients intently resembles ischemic retinopathy due to systemic vasculitis or diabetes (Wong et al 2019). Similarly, drug-precipitated optic neuropathy from antivirals may additionally mimic demyelinating disease or dietary deficiencies Aggarwal et al 2021). Without careful clinical correlation, misdiagnosis can result in behind schedule management and irreversible imaginative and prescient loss.
The diagnostic system calls for interdisciplinary protocols regarding hepatologists, ophthalmologists, and infectious disease experts. Comprehensive evaluation should include: (i) baseline ophthalmic screening earlier than initiation of antiviral remedy, (ii) multimodal imaging which include fundus fluorescein angiography, OCT, and field of regard checking out to hit upon early retinal or optic nerve changes, and (iii) laboratory evaluation for viral load, immune markers, and cryoglobulins to correlate systemic pastime with ocular manifestations. Emerging diagnostic equipment, inclusive of cytokine profiling and ocular fluid PCR, may also offer extra precise attribution of viral versus immune-mediated pathology in the close to destiny (Yamada et al 2022).
Standardized scientific pointers are still lacking, and cutting-edge practice is predicated heavily on case reviews and professional opinion. There is an urgent want for prospective cohort studies and consensus-driven interdisciplinary care protocols to improve diagnostic accuracy and make sure early detection of imaginative and prescient-threatening headaches in patients with viral liver illnesses.
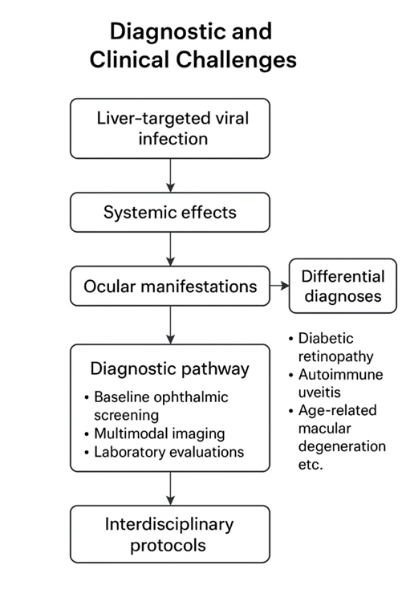
Figure 3. Diagnostic and scientific demanding situations in liver-focused viral infections with ocular manifestations.
The flowchart illustrates the complexity of prognosis: patients often present with overlapping hepatic and ocular symptoms, making differential prognosis hard. Hepatic markers (HBsAg, HCV RNA, HEV IgM), ophthalmic findings (uveitis, retinopathy, optic neuritis), and systemic immune profiles can be nonspecific or confounded by means of treatment-associated facet results. Interdisciplinary collaboration between hepatologists, ophthalmologists, and immunologists is crucial for correct prognosis and management. The diagram highlights three key barriers: (i) delayed popularity of ocular signs, (ii) misattribution of visible signs and symptoms to drug toxicity or unrelated ocular disease, and (iii) loss of standardized protocols. Integration of molecular diagnostics, imaging (OCT, fundus photography), and immune profiling is crucial for well-timed intervention.
Translational Models and Research Tools
Progress in know-how the liver–ocular axis in viral infections has been confined by means of the shortage of strong experimental models. Translational research employing animal fashions, ocular pathology strategies, and omics-based processes has begun to bridge this gap, enabling mechanistic insights and preclinical healing trying out.
Animal Models - Murine and non-human primate fashions of HBV and HCV contamination had been used to recapitulate hepatic and extrahepatic pathology. HBV-transgenic mice exhibit immune-mediated hepatic harm with evidence of ocular irritation reminiscent of uveitis and retinal vasculitis. Similarly, humanized chimeric mice engrafted with human hepatocytes allow continual HCV contamination and provide systems for testing antiviral toxicity on ocular tissues. Rabbit and primate fashions of dengue and yellow fever have also been used to take a look at virus-brought about retinal hemorrhage and vasculitis. These models help delineate immune-mediated ocular harm secondary to systemic viral contamination.
Ocular Pathology Tools- In vivo imaging, together with optical coherence tomography (OCT), fluorescein angiography, and confocal microscopy, lets in specific assessment of retinal microvasculature and optic nerve changes. Postmortem histopathology and immunohistochemistry (IHC) allow assessment of viral antigen localization in ocular tissues, glial activation, and immune complex deposition. Experimental viral inoculation in ocular tissues in small animals similarly aids in differentiating direct viral invasion from systemic immune-mediated results (Figure 3 & 4).
Omics-Based Research- High-throughput transcriptomics, proteomics, and metabolomics are more and more being implemented to each hepatic and ocular tissue to uncover shared pathogenic pathways. For instance, transcriptomic profiling of HCV-infected patients has found out upregulation of interferon-stimulated genes in both liver and conjunctival epithelium. Metabolomics has recognized lipid dysregulation and oxidative stress markers commonplace to hepatic steatosis and retinal degeneration. Recent advances in single-cellular RNA sequencing (scRNA-seq) are beginning to map immune cell populations throughout liver and ocular tissues, highlighting move-compartmental T mobile and macrophage activation.
Together, these translational tools provide a comprehensive framework for elucidating the pathophysiological basis of vision loss in liver-centered viral infections. However, the development of integrative multi-organ fashions-combining hepatocyte and retinal organoids, or liver–eye-on-a-chip systems-represents the following frontier in modelling systemic viral pathogenesis and checking out targeted therapeutics.
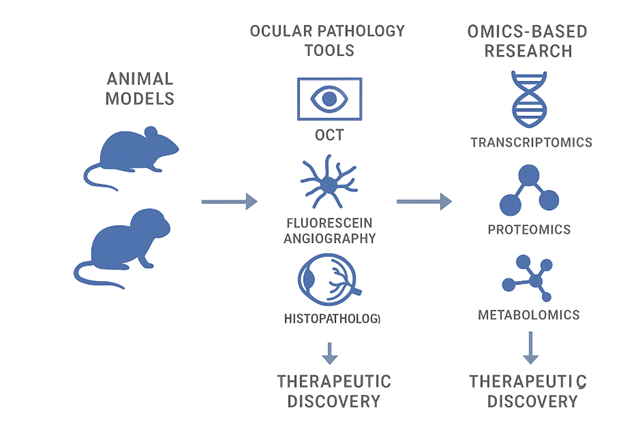
Figure 4 Translational Models and Research Tools for Studying Liver
Targeted Viral Infections and Ocular Complications. The schematic illustrates integrative techniques bridging liver pathology and ocular sickness. Animal models (transgenic mice, zebrafish, non-human primates) reflect hepatotropic viral infection and its ocular sequelae. Ocular pathology tools (fundus imaging, OCT, electrophysiology, histopathology) allow designated assessment of retinal and optic nerve damage. Omics-primarily based studies (genomics, transcriptomics, proteomics, metabolomics, microbiome profiling) offers molecular insights into host–virus interactions and immune-mediated pathways. Collectively, those translational strategies allow mechanistic discovery and healing checking out for preventing imaginative and prescient loss in patients with liver-targeted viral infections.
Therapeutic Implications and Management
Management of ocular complications associated with liver-targeted viral infections calls for a twin cognizance on controlling the underlying hepatic viral disorder and mitigating the ophthalmic manifestations. Conventional and rising strategies span antiviral remedies, immunosuppressive regimens, and personalised healing approaches.
Antiviral Treatments- The advent of direct-appearing antivirals (DAAs) for HCV has dramatically decreased systemic and extrahepatic sickness burden, which include retinopathy and sicca signs and symptoms, via accomplishing sustained virological reaction (SVR) (Pawlotsky et al 2020). Similarly, nucleos(t)ide analogues (e.g., entecavir, tenofovir) for HBV suppress viral replication and in a roundabout way lessen immune-mediated ocular irritation. For HEV, control stays supportive, even though ribavirin has been stated to enhance effects in persistent or immunocompromised patients with ocular sequelae (Kamar et al 2017) is shown in Table 2.
Immunosuppressive and Anti-inflammatory Therapy- Ocular manifestations such as uveitis, optic neuritis, and retinal vasculitis frequently require adjunctive corticosteroids or steroid-sparing immunosuppressants (e.g., azathioprine, mycophenolate). Targeted biologics, consisting of anti-TNF marketers and IL-6 inhibitors, have proven promise in refractory viral-related ocular irritation. However, immunosuppressive remedy needs to be cautiously balanced in opposition to the threat of viral reactivation, necessitating near interdisciplinary tracking.
Personalized Medicine Approaches- Advances in host genetic profiling and immune biomarkers are allowing affected person stratification for tailor-made therapy. For example, polymorphisms in IL28B have an effect on HCV treatment response, at the same time as HLA haplotypes can also predispose to autoimmune ocular complications. Personalized medication additionally extends to therapeutic drug monitoring, optimizing antivirals to minimize ocular toxicity while maximizing viral suppression (Figure 5).
Emerging Therapies and Future Directions- Cutting- area strategies consist of host-centered antivirals designed to prevent immune-mediated collateral harm, nanoparticle-primarily based drug delivery systems that restrict ocular toxicity, and gene-modifying gear (CRISPR-Cas9) under preclinical exploration for HBV eradication ( Liu et al ., 2021). In parallel, stem cellular-primarily based regenerative healing procedures and neuroprotective retailers (e.g., antioxidants, neurotrophins) are being investigated to keep retinal and optic nerve function in patients with hooked up damage.
In summary, the healing panorama is shifting from one-size-fits-all antiviral suppression toward integrated, multidisciplinary, and precision-guided tactics. Future advances will hinge on combining systemic viral control with localized ocular protection, ensuring that patients with liver-centered viral infections are safeguarded not handiest from hepatic morbidity however also from preventable vision loss.
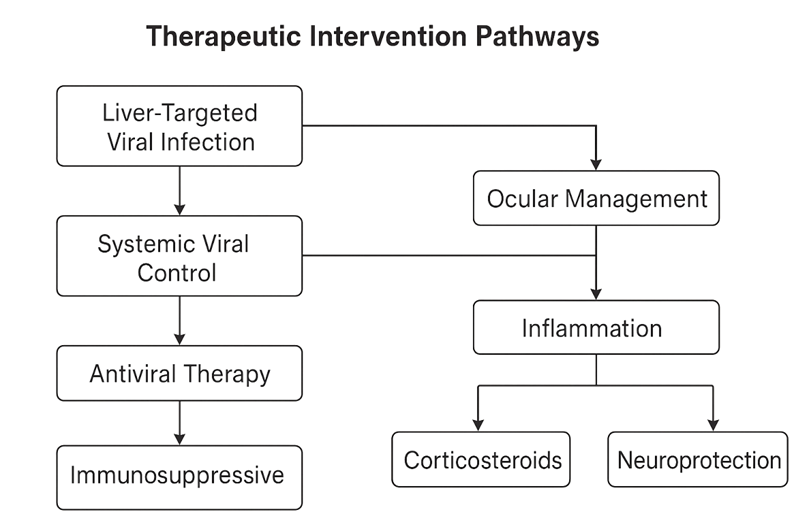
Figure 5. Therapeutic Intervention Pathways for Liver-Targeted Viral Infections with Ocular Manifestations
The schematic highlights modern and rising healing techniques at the interface of hepatology and ophthalmology. Antiviral remedies (e.g., direct-appearing antivirals, nucleos(t)ide analogs) lessen viral replication and systemic irritation, indirectly mitigating ocular complications. Immunosuppressive and immunomodulatory dealers (e.g., corticosteroids, biologics) goal aberrant immune responses implicated in uveitis, optic neuritis, and vasculitis. Personalized medication processes incorporate host genetic profiling, cytokine signatures, and ocular biomarkers to optimize remedy. Emerging strategies which include host-centered antivirals, focused biologics, and progressive drug shipping structures (e.G., intravitreal formulations, nanocarriers) intention to balance hepatic viral suppression with ocular safety. Interdisciplinary protocols integrating hepatologists, ophthalmologists, and immunologists are emphasized to make certain complete patient care.
Table 2. Clinical case examples of liver-targeted viral infections with ocular manifestations
|
Patient/ Study |
Virus |
Liver Pathology |
Ocular Manifestation |
Mechanism Proposed |
Management/ Outcome |
|
Yamada et al 2022 |
HBV |
Chronic hepatitis with fibrosis |
Bilateral uveitis and optic neuritis |
Immune complex deposition, T-cell mediated autoimmunity |
Responded to corticosteroids; antiviral therapy continued |
|
Wong VK et al 2019 |
HCV |
Cirrhosis with cryoglobulinemia |
Retinal vasculitis and dry eye syndrome |
Cryoglobulin deposition, direct viral effect on lacrimal gland |
Combined interferon-free DAA regimen with topical lubricants; ocular symptoms improved |
|
Aggarwal et al 2021 |
HEV |
Acute viral hepatitis |
Optic neuropathy with neuroretinitis |
Post-infectious autoimmune demyelination |
Intravenous methylprednisolone; gradual visual recovery |
|
Dengue case report (Nair et al., 2020) |
Dengue (hepatotropic viral infection) |
Acute hepatic failure |
Retinal hemorrhage, macular edema |
Cytokine storm, endothelial dysfunction |
Supportive care, corticosteroid therapy; partial visual recovery |
|
Hypothetical Clinical Case (Literature gap) |
HDV + HBV co-infection |
Decompensated cirrhosis |
Severe panuveitis (rarely reported) |
Severe hepatic–ocular inflammation |
Limited data; requires further study |
This table summarizes representative clinical cases linking hepatic viral infections with vision-threatening ocular complications. It highlights the diversity of liver pathology, spectrum of ocular manifestations, proposed underlying mechanisms, and therapeutic approaches. Documented cases from HBV, HCV, HEV, and dengue virus demonstrate immune-mediated and metabolic pathways driving ocular injury, whereas data on HDV remain limited, underscoring the need for further clinical investigations.
CONCLUSION
Liver-targeted viral infections along with HBV, HCV, and HEV enlarge their pathological impact past hepatic tissue, with the attention rising as a clinically big but often under-recognized aim. The liver–eye axis is mediated thru immune complex deposition, systemic cytokine dysregulation, metabolic disturbances, and neuroimmune interactions, which collectively contribute to ocular manifestations beginning from uveitis and retinopathy to optic neuropathy. Despite growing proof, diagnostic challenges persist due to overlapping functions with autoimmune and infectious eye ailments, underscoring the want for interdisciplinary protocols integrating hepatology and ophthalmology.
Advances in translational models and omics-based totally absolutely strategies have started out to unravel the molecular underpinnings of liver–ocular crosstalk, highlighting novel biomarkers and therapeutic objectives. Current manage is primarily based on antiviral treatment alternatives to control systemic viral replication and adjunctive immunosuppressive techniques to relieve ocular irritation, but both strategies require cautious balancing to avoid viral reactivation or drug-delivered on toxicity. The emergence of precision medicinal drug, host-focused antivirals, biologics, and regenerative treatments offers promising avenues for lowering imaginative and prescient-threatening complications.
Moving forward, more emphasis on prospective medical studies, incorporated affected person registries, and collaborative research networks might be vital to outline the real burden of ocular morbidity in liver-targeted viral infections. Ultimately, recognition of the liver–ocular axis not only expands our understanding of systemic viral diseases but also opens the door to innovative therapeutic strategies aimed at preserving vision while addressing hepatic health.
ABBREVIATIONS
ACKNOWLEDGEMENTS
None.
USING ARTIFICIAL INTELLIGENCE (AI)
The authors did not use artificial intelligence-based technologies, except for some English language corrections.
AUTHOR CONTRIBUTIONS
All authors contributed to the study conception and design. NG: Methodology, Formal analysis, Data extraction, Writing - original draft, Writing - review & editing; NJ: Conceptualisation, Methodology, Validation, Formal analysis, Data extraction, Writing - original draft, Writing - review & editing ;MN. All authors read and approved the final manuscript.
FUNDING
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
DATA AVAILABILITY
All data are presented in the text. Data access All data were recorded in Tables.
DECLARATIONS ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not required.
CONSENT FOR PUBLICATION
None.
COMPETING INTERESTS
The authors declare that they have no competing interests.
REFERENCES



Neethirajan Guruswamy, Nallathambi Jeyabalan, Muruganandam Nagarajan, Liver-Targeted Viral Diseases and Vision Loss: Current Understanding and Future Therapeutic Targets, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3841-3855. https://doi.org/10.5281/zenodo.18085517
 10.5281/zenodo.18085517
10.5281/zenodo.18085517
