Dr. D. Y. Patil College of Pharmacy, Akurdi, Pune
A progressive neurodegenerative disorder Alzheimer’s disease is characterised by memory loss and cognitive decline which primarily affect the elderly person. There have been few disease-modifying effects from traditional treatment options, which have mostly been symptomatic. By delaying the pathological progression of early Alzheimer's disease, lecanemab, a monoclonal antibody that targets soluble amyloid-beta protofibrils, has brought about a novel therapeutic approach. The development, mechanism of action, adverse effects, synthesis, clinical trial data, and marketing insights of lecanemab are all examined in this article. Early-stage patients' cognitive slowing has shown statistically significant results in the pivotal CLARITY-AD trial. However, there are also significant side effects linked to lecanemab use, including neuropsychiatric symptoms, infusion-related reactions, and amyloid-related imaging abnormalities (ARIA). Careful patient monitoring is required because post-marketing data, such as pharmacovigilance analysis from the FDA Adverse Event Reporting System (FAERS), highlights uncommon but serious events, including deaths. The article also covers future directions in Alzheimer's therapy, regulatory milestones, and formulation strategies. Lecanemab, a first-generation disease-modifying drug in this class, exemplifies both the advancement of science and the difficulty of converting laboratory results into clinical use.
The US Food and Drug Administration approved lecanemab, an amyloid beta-targeting antibody, on January 6, 2023, for the treatment of mild cognitive impairment caused by Alzheimer's disease (AD) and mild AD dementia through its Accelerated Approval pathway [1,2]. Emil Kraepelin's colleague, German psychiatrist Alois Alzheimer, originally referred to AD as "presenile dementia" in 1906. It is being developed by Eisai in partnership with Biogen and under a worldwide license from BioArctic (formerly BioArctic Neuroscience) for the treatment of Alzheimer's disease [3]. On January 6, 2023, it was approved for the first time in the United States under the Accelerated Approval Pathway. The US Food and Drug Administration (FDA) approved a lecanemab application for expedited clearance in July 2022 [1]. While many scientists contributed to a better knowledge of Alzheimer's disease, Dr. Lars Lannfelt, a Swedish neurologist, was the driving force behind the discovery of Lecanemab, which led to its development by BioArctic and Eisai. His research on amyloid-beta protofibrils paved the way for this revolutionary treatment. Lecanemab is based on research conducted by Professor Lars Lannfelt, the founder of BioArctic. Targeting the underlying condition and slowing down cognitive deterioration, it is the first and only fully approved medication for people with moderate cognitive impairment or mild Alzheimer's disease in the US and Japan.
Lecanemab (Leqembi™) was licensed by the Medicines and Healthcare Products Regulatory Agency (MHRA) in 2024, becoming one of the first disease-modifying treatments for Alzheimer's in the UK [3].Clinical trials began in the early 2010s, with early-stage trials concentrating on safety and dose. The crucial Phase 3 trial, known as the CLARITY AD research, revealed convincing evidence of the drug's efficacy in reducing cognitive deterioration in people with early Alzheimer's disease. Early in the 20th century, AD was first understood historically. A thorough description of instances characterised by severe cellular changes, such as extensive plaques and the loss of around one-third of the cerebral cortex, was reported by Emil Kraepelin in 1910. At a period when the disease's medical diagnosis was still ambiguous, Kraepelin's observations were crucial in helping to define it. In 1906, During discussion of the case Auguste Deter, the condition was identified by Dr Alois Alzheimer. But until later advancements, the clinical definition of AD was still a little unclear. Even though arteriosclerosis was not explicitly identified during clinical testing, its involvement could not be totally disregarded. The first Alzheimer's patient's brain was later reanalysed in 1998 by researchers from the Max Planck Institute and the University of Munich, providing fresh perspectives on the pathophysiology of the illness. Dr Gerber and his colleagues' additional histological examination in 1997 supported Alzheimer's pioneering findings by confirming the existence of amyloid plaques. Biogen reported encouraging findings from an ongoing phase III clinical trial in September 2022. The medication was declared a clinical trial success in November 2022, surpassing its target in achieving the primary endpoint [4].
PHYSICOCHEMICAL PROPERTIES:
Lecanemab (Leqembi) is a humanised whole antibody which has a high molecular weight (~150,000 DA) and a complex molecular formula. It exists in a liquid state, and it is also soluble in physiological buffers. The stability and bioavailability are enhanced by glycosylated molecules. It remains stable at temperatures ranging from (2to8 °c), which indicates good storage potential. These physiochemical properties are used as biological therapeutic targeting amyloid beta [5].
Table 1.1 Physiochemical properties of lecanemab:
|
Property |
Description |
|
Generic Name |
Leqembi |
|
Brand Name |
Lecanemab |
|
Molecular Formula |
C6544h10088n1744o2032s46 |
|
Molar Mass |
147181.62 G·Mol−1 |
|
Molecular Weight |
150000.0 Da |
|
State |
Liquid |
|
Type |
Whole Antibody |
|
Source |
Humanised |
|
Target |
Amyloid Beta |
|
Stability |
Stable At 2- 8°C |
|
Solubility |
Soluble in Physiological Buffers |
|
Glycosylation |
It is present and affects the stability and bioavailability. |
PHARMACOKINETIC PROPERTIES:
Dosage and administration: The FDA recommends lecanemab at a dose of 10 mg/kg body weight, which should be diluted before being administered intravenously once every two weeks over a period of approximately one hour. Next dose should be administered immediately if an infusion is missed. Give as an intravenous infusion via a terminal low-protein binding 0.2 micron in-line filter over a period of around one hour [6-10].
Table 1.2 Pharmacokinetics parameters of lecanemab:
|
Parameter |
Description |
Lecanemab Value |
|
Cmax |
Highest concentration of drug in plasma |
After IV administration, dependent on dose |
|
Tmax |
Time taken to reach Cmax |
Immediately after IV infusion |
|
T half |
Elimination half-life: 5–7 days. |
5 to 7 days (dose dependent) |
|
AUC |
Total drug exposure over time |
Increase proportionally with a dose range of 0.3 to 15 mg/kg |
|
Clearance (CL) |
Rate of drug removal from plasma |
0.434 (0.420-0.451) L/day |
Table 1.3 Pharmacokinetic parameters of IV lecanemab 10 mg/kg, biweekly:
|
Parameters |
Mean |
|
AUC (ng.h/ml) |
5720 (1230) |
|
Cmax (µg/ml) |
307 (70.2) |
|
Half-life (h) |
127 (30) |
After the final dose of lecanemab the parameters were evaluated.
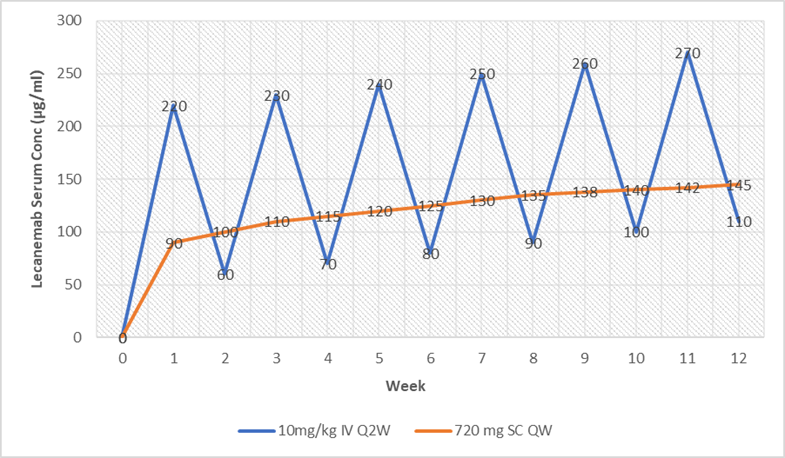
Figure 1.1 Pharmacokinetic parameters of IV lecanemab 10 mg/kg, biweekly
Table 1.4 Comparability. (A) PK comparability of SC dose (mg) to IV dose (mg/kg) [9]
|
Parameter |
Intravenous administration (10 mg/kg iv q2w) |
Subcutaneous administration (720 mg sc qw) |
|
Cmax |
Higher peak concentration due to direct infusion into the bloodstream. |
Approximately 22.8% of the IV, reflecting a prolonged absorption phase. |
|
Tmax |
Occurs at the end of the infusion (~1 hour). |
Approximately 72 hours post-injection. |
|
AUC |
Standard reference for bioavailability. |
Approximately 11% higher than IV administration |
|
T half |
Approximately 7 days. |
Like IV, around 7 days. |
Absorption: Lecanemab is administered via intravenous (IV) infusion, ensuring 100% bioavailability. Lecanemab given as an infusion every two weeks at a dose of 10 mg/kg of body weight. It is not absorbed through the gastrointestinal tract since it bypasses first-pass metabolism.
Distribution: Lecanemab primarily distributes in plasma and interstitial fluid. The volume of distribution for lecanemab is approximately 3.22 litres, indicating limited distribution beyond the vascular and interstitial spaces. Higher the VDss, the compound is more dispersed in tissue instead of plasma and lower the VDss indicates the molecule is needed to reach plasma concentration. It does not cross the blood-brain barrier (BBB) easily, but enough reach the brain to target amyloid-beta plaques. Poor cranial nervous system permeability indicating poor distribution to the brain.
Metabolism: Lecanemab undergoes proteolytic degradation like endogenous IgG antibodies, involving enzymatic breakdown into smaller peptides and amino acids.
Excretion: Lecanemab takes about 5 to 7 days for its levels in the blood to reduce by half, and the body clears it at a rate of 0.434 liters per day. Its elimination is primarily through proteolytic pathways rather than renal or hepatic routes.
MECHANISM OF WORKING:
Lecanemab is a humanised IgG1 monoclonal antibody* that is engineered to bind to soluble amyloid-beta (Aβ) protofibrils which are thought to be highly neurotoxic and are primarily responsible for the progression of Alzheimer's disease (AD). In contrast to other anti-amyloid treatments that mostly target insoluble Aβ plaques lecanemab targets soluble protofibrils and inhibits them from aggregating into large fibrillar structures [11].
Targeting Aβ Protofibrils: Aβ protofibrils are soluble early-stage Aβ peptide aggregates that account for synaptic impairment and neurotoxicity. Protofibrils have been implicated to [12]:
Lecanemab focuses on hitting the soluble Aβ protofibrils—basically skipping over the monomers and fully formed fibrils. This specificity minimizes neurotoxic effects at an earlier stage of AD development.
Clearance of Amyloid Deposits: Following binding to protofibrils, lecanemab enables their clearance via the immune system's microglial-mediated phagocytosis. Microglia identify the antibody-protofibril complex and clear it from the brain, lowering the overall amyloid burden.
Prevention of Plaque Formation: By inactivating soluble protofibril, lecanemab inhibits additional aggregation into fibrils and insoluble amyloid plaques. This is different from other monoclonal antibodies that act mainly by degrading already existing plaques.
Binding Affinity and Selectivity: Lecanemab binds to small protofibrils with 100 times the affinity of aducanumab, and to larger protofibrils with 25 times the affinity. It has significantly lower binding affinity for Aβ monomers, reducing potential off-target effects and toxicity [12].
Through its mechanism of action, lecanemab contributes to:
Lecanemab represents a forward-thinking strategy by acting against soluble amyloid species before they turn into permanent plaques, thus being among the most developed second-generation anti-amyloid treatments [13].
SYNTHESIS:
Lecanemab is a humanised monoclonal antibody developed to treat amyloid?beta (Aβ) protofibrils of Alzheimer's disease. It is manufactured by several established biotechnological steps, like other therapeutic monoclonal antibodies [11-14].
Antigen Recognition and Production of Antibody:
Aβ protofibrils are targeted as antigens. Mice are immunised with the antigen to create antibodies that are secreted by mice for binding specifically onto Aβ protofibrils [12].
Humanisation of Murine Antibodies:
To lower the risk of triggering an immune response in humans, mouse antibodies are modified to be more human-like. This is typically achieved by grafting the murine complementarity-determining regions (CDRs) onto the framework of a human antibody. The resulting chimeric antibody keeps the original mouse antibody’s ability to recognise its target but is less likely to trigger an immune response in humans [12]
Gene Cloning and Expression:
The vectors are transfected into host cells—Chinese Hamster Ovary (CHO) cells in most cases. CHO cells are commonly used since they can produce complex proteins and carry out the necessary post-translational modifications to ensure the proteins work properly [11].
Cell Culture and Fermentation:
Transfected CHO cells are grown in bioreactors under highly controlled conditions (pH, temperature, nutrient feed, and oxygen level) to achieve optimal cell growth and antibody yield. Advanced bioprocessing technologies, including three-dimensional culture systems and optimised fermentation regimens, are frequently used to achieve optimal yield [14].
Purification:
When synthesized, the antibody is secreted into culture medium and purified by different chromatographic methods. Some of these common methods are [14]:
Characterisation and Quality Control:
The antibody is purified extensively to validate structure, binding activity, and biological function. Quality control is utilised to guarantee consistency between lots of manufacture, conforming to regulatory requirements for clinical use [13].
MEDICINAL USES:
A humanised monoclonal antibody called lecanemab has demonstrated great promise in the management of Alzheimer's disease in its early stages. Based on clinical and regulatory data, the following are its primary medicinal uses [13-17]:
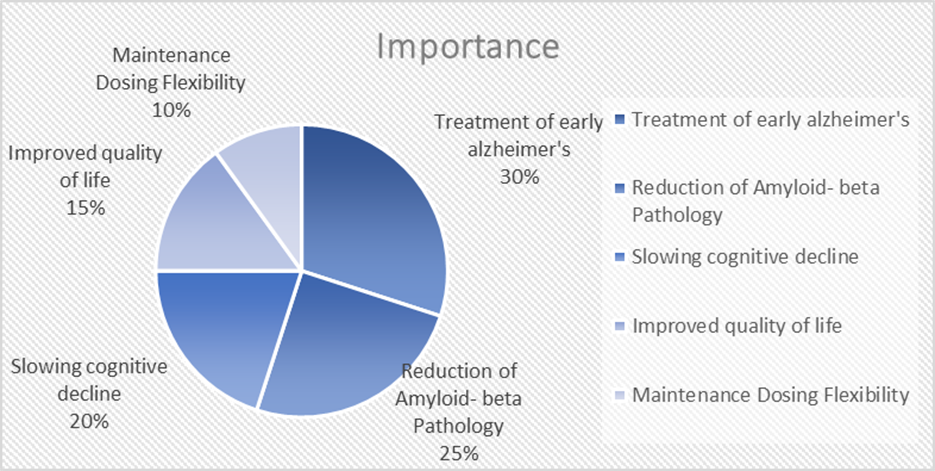
Figure 1.2 Medicinal uses of Lecanemab
Management of Alzheimer's Disease in Its Early Stages:
People in the early stages of Alzheimer’s, such as those with mild memory problems or early dementia, may benefit from taking lecanemab. The goal of early intervention is to halt the progression of the disease before significant neuronal damage happens [16].
Decrease in Amyloid-Beta Disease:
By focusing on soluble amyloid-beta protofibrils, it helps remove them from the brain and lessens the buildup of amyloid plaque, which is a defining feature of Alzheimer's disease pathology [14].
Decrease in Cognitive and Functional Abilities:
Lecanemab considerably slowed the decline in cognitive and functional abilities as assessed by the Clinical Dementia Scale in the Phase 3 CLARITY-AD trial [17].
Enhanced Life Quality:
Lecanemab's role in improving daily functioning and managing symptoms is demonstrated by the improved health-related quality-of-life ratings reported by patients [15].
Maintenance Dosing Availability:
Following the initial biweekly regimen, a once-monthly maintenance dosing option has been approved, increasing treatment flexibility and adherence [13].
ADVERSE EFFECTS:
Lecanemab has demonstrated several clinical benefits in treating early Alzheimer's disease. However, it’s use is also associated with a wide range of side effects based upon post-marketing and clinical data [17,18].
Table 1.5 Summary of Reported Adverse Effects of Lecanemab [17]
|
Category |
Source |
Adverse Effects |
|
Clinical trial data |
Clarity - AD Trial |
|
|
Post-marketing data |
FAERS Pharmacovigilance Study (2024) |
|
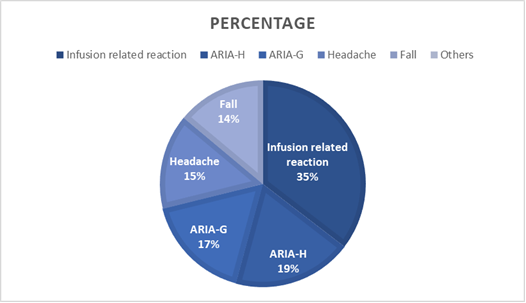
Figure 1.3 Distribution of common adverse effects [18]
TREATMENT OF OVERDOSE:
Lecanemab is a recently developed antibody therapy aimed at helping people in the early stages of Alzheimer’s. It acts by inhibiting amyloid-beta protofibrils to slow cognitive decline and alter disease course. Although its clinical efficacy is impressive, the risk of overdose, particularly with newer modes of administration, makes safety and proper management a concern. An appreciation of the effects of overdose by different routes of administration is important for maintaining patient safety and informing healthcare practice in approved and hypothetical contexts alike [13].
Intravenous (IV) overdose:
Most probable scenario, since IV is the sole approved route.
1. Possible Consequences:
Table 1.6 Dosing recommendations for patients with ARIA-E
|
Clinical Symptom Severity |
ARIA-E Severity on MRI |
||
|
Mild |
Moderate |
Severe |
|
|
Asymptomatic |
May continue dosing. |
Suspend dosing. |
Suspend dosing. |
|
Mild |
Further dosing may be guided by the clinical’s discretion. |
Suspend dosing. |
|
|
Moderate or severe |
Suspend dosing. |
|
|
Table 1.7 Dosing recommendation for patients with ARIA-H
|
Clinical symptom severity |
ARIA-H Severity on MRI |
||
|
Mild |
Moderate |
Severe |
|
|
Asymptomatic |
May continue dosing. |
Suspend dosing. |
Suspend dosing. |
|
Symptomatic |
Suspend dosing. |
Suspend dosing. |
|
2. Treatment Approach:
Subcutaneous (SC) overdose:
Not approved, but if SC forms become available and overdosed:
1. Possible Consequences
2. Treatment Approach
Intramuscular (IM) Overdose:
Unlikely and not licensed, but potentially so theoretically.
1. Possible Consequences:
2. Treatment Approach:
Intrathecal (Spinal) Overdose:
Extremely risky and never done.
1. Possible Consequences:
2. Treatment Approach:
Oral Overdose:
Monoclonal antibodies are biologically ineffective when administered orally, as they are degraded in the gastrointestinal tract
1.Possible Consequences
2. Treatment Approach:
No MRI or monitoring is required, unless patient has inadvertently ingested another toxic drug.
Inhalational or Nasal Overdose:
Still experimental and theoretical.
1. Possible Consequences:
2. Treatment Approach:
CONTRAINDICATIONS:
Lecanemab, known by its brand name Leqembi, is a humanised IgG1 monoclonal antibody that acts on soluble aggregated amyloid-beta protofibrils. It was approved on an expedited basis by the U.S. FDA in January 2023 as a treatment for early Alzheimer's disease, mild cognitive impairment, or mild dementia stage with positive amyloid pathology confirmation. Although it is a milestone in disease-modifying treatments, its application must be preceded by a definite knowledge of its contraindications and safety profile in differing comorbidities [19-21].
Hypersensitivity to lecanemab: Do not use lecanemab in patients with known allergies to the drug or its ingredients. The reactions can be in the form of anaphylaxis, angioedema, urticaria, or bronchospasm [19].
Cerebrovascular Disease and Amyloid-Related Imaging Abnormalities (ARIA): Lecanemab has been linked with Amyloid-Related Imaging Abnormalities (ARIA), specifically [19]:
Relative contraindications are:
Use of Antithrombotic or Anticoagulant Therapy: Chronic anticoagulation patients (e.g., warfarin, apixaban, rivaroxaban) are at greater risk of intracranial haemorrhage on Lecanemab therapy, particularly if ARIA-H is present. Although not entirely contraindicated, use with anticoagulants should be undertaken with utmost caution and risk vs. benefit evaluation [20].
Uncontrolled Hypertension: Hypertension is an intracranial haemorrhage risk factor. The treatment with Lecanemab should not be started in those uncontrolled with high blood pressure. Blood pressure should be monitored throughout treatment [20].
Advanced Alzheimer's Disease: Lecanemab is indicated only for use in early-stage Alzheimer's disease and is not approved for advanced stages. Use in moderate or severe phases is not evidence supported and could risk increasing the chances of adverse effects without demonstrated benefit [20].
Active Seizure Disorders: While not contraindicated per se, caution is exercised in epilepsy or recent seizure history because ARIA-E could worsen neurological symptoms and reduce seizure threshold [20].
Pregnancy and Lactation: There are insufficient human data on the use of Lecanemab in pregnant or breastfeeding women. Monoclonal antibodies can cross the placenta—most notably in the third trimester of pregnancy—and may also be excreted into breast milk. Use during pregnancy is not advised unless the potential benefits clearly outweigh the risks [20].
Immunocompromised Conditions: Although Lecanemab is not widely immunosuppressive, patients with pre-existing immunodeficiency or on immunosuppressants need to be closely monitored because immune reactions to ARIA or other adverse effects can be compromised [20].
Lecanemab is an attractive treatment option for incipient Alzheimer's disease but has important risks, especially among patients with predisposing cerebrovascular disease, APOE ε4 homozygotes, or those on anticoagulation. Careful selection of patients, MRI screening, and regular monitoring are required to maximize therapeutic benefit with minimal risk.
INTERACTION –
Alzheimer’s disease is the most common neurodegenerative disorder with huge currency in elderly population. The clinical condition is characterised by slow progressive impairment of intellectual function, psychiatric and different behavioural symptoms. Delusion or hallucination appears 30 -50 % in Alzheimer patient and as many as 70% of them exhibit aggressive behaviour. Additionally, antipsychotics are known to interact with various pharmacological agents, notably antiarrhythmic drugs and acetylcholinesterase inhibitors. This review highlights the most frequent drug - drug interaction which are capable of harming in Alzheimer diseases [22].
The most common drug – drug interaction is pharmacokinetic and pharmacodynamic interaction .
Pharmacokinetic drug interaction: The pharmacokinetic property of drug is affected by several conditions related to patient, such as genetic determination and age-related alteration. Drug behaviour in the body can differ in Alzheimer patient, due to reduce muscle mass and alter liver and kidney function.
The memantine and AChEL are the frequently used agents for Alzheimer’s treatment. According to definition pharmacokinetic interaction mainly includes alteration in plasma concentration of drug by other agents that affect absorption , metabolism, distribution, and excretion phage [22].
According to pharmacology, AChEL have relatively few pharmacokinetic interactions. The donepezil and galantamine are metabolised in liver through CYP2D6 and CYP3A4 , their hepatic metabolism is affected by specific substrate and inhibitor. Several drugs such as amiodarone, bupropion, cimetidine, citalopram, donepezil, duloxetine, galantamine, haloperidol, pergolide, propranolol, thioridazine etc can be interrelated with donepezil and galantamine at specified level with different mechanism.
However, given that donepezil may be metabolised by two cytochromes (CYP3A4 and CYP2D6), competitive inhibition with other CYP2D6 and CYP3A4 drug substrate , such as antidepressant may not be clinically applicable. The interaction of galantamine with ketoconazole or paroxetine leads to 30 – 40 % of galantamine vulnerability, compared to alone galantamine.
Urine PH is the major factor for excretion of alkaline drug such as memantine, the renal excretion of memantine may have relevant impact on the pharmacokinetic profile. Alteration in urine PH might leads to toxic effect and suppress renal function. The increase in plasma level of memantine may arise if co administered with agents using same renal cationic transport system as amantadine, cimetidine, ranitidine, quinidine, quinine, and nicotine.
Other pharmacokinetic drug – drug interaction that may occur in Alzheimer patient are related to psychiatric drugs such as benzodiazepine, antidepressant, and antipsychotic agents that are largely used for behavioural alteration in patients. The major drug – drug interaction is related to hepatic metabolism . For example – hepatic CYP enzyme of phase 1 metabolism are most liable, regarding the pharmacokinetic interaction of antipsychotic drug. Among the multiple enzymes in the liver, CYP1A2 , CYP2C19, CYP2D6 and CYP3A4 are practically relevant for the degradation of antipsychotic drugs . Several drugs, such as amiodarone, bupropion, cimetidine, citalopram, duloxetine, haloperidol, pergolide, propranolol, and thioridazine, may exhibit pharmacokinetic or pharmacodynamic interactions with acetylcholinesterase inhibitors like donepezil and galantamine, each via distinct mechanisms.
Pharmacodynamic drug interaction:
The pharmacodynamic drug – drug interaction may result from a synergistic mechanism. There are many CNS drug which may interact directly at receptor level or indirectly effect one or more neurotransmitter. The risk developed an ADR related to negative drug – drug interaction is increased due to CNS aging alteration and can be more relevant to Alzheimer patient. When these medications are used properly, they may slow down cognition and functional impairment associated with Alzheimer diseases [22].
The effect of anticholinergic is a feature of several drugs such as antidepressant, anti-histamine, bronchodilator, and drugs for antipsychotic. The use of these classes of drugs even in non – Alzheimer elderly individual is considered potentially inappropriate. The use of anticholinergic drugs by those with dementia can cause trouble for these individual because they can be more prone to develop medication induced cognitive impairment. By the analysis of recent reports ADRs related to AchEL in France up to 2006, found that most frequently reported ADRs are due to drug - drug interaction, in patients who are treated with ACHELs and were associated with bradycardia (54.5%) and anticholinergic (31.4%) drugs via pharmacodynamic mechanism.
Parasympathetic nervous system is stimulated by most of the cardiovascular ADRs. This system can affect heart as well as brain function. The inhibition of cholinesterase by ACHELs retars acetylcholine degradation. The cardiovascular effect reported for ACHELs underlines that the molecular mechanism may be responsible for the most negative drug – drug interaction with other drugs that have cardiac activity.
According to drug – drug interaction, the memantine shows a weak dopaminergic agonist effect with atropine. Concurrent use of memantine and other NMDA receptor modulators can potentially lead to pharmacotoxic psychosis, so such combinations should be avoided.
CONVENTIONAL MARKETED FORMULATION:
According to recent conventional treatment of Alzheimer's disease, it mainly includes cholinesterase inhibitors such as donepezil, rivastigmine, galantamine and also NMDA receptor antagonist. These drugs help to manage symptoms by enhancing neurotransmitter functions but do not affect disease progression. Lecanemab is a monoclonal antibody which is developed to target amyloid - beta protofibrils who’s aim is to slow Alzheimer progression [23].
Table 1.8 Conventional marketed formulation
|
Sr. No. |
Types |
Brand name |
Company |
Dose |
Price (Approx) |
|
1 |
Tablet |
Aricept |
Eisai/ Pfizer |
5mg/10mg |
$300/month USA |
|
2 |
Tablet |
Exelon |
Novartis |
1.5mg – 6mg |
$200 -$250 /month |
|
3 |
Capsule |
Namenda |
Allergan |
5mg/10mg |
$150 -$250/month |
|
4 |
Oral solution |
Donepezil hydrochloride |
Various generics |
1mg/ml |
$100 -$150/month |
|
5 |
Patch |
Exelon patch |
Novartis |
4.6mg/13.3mgper 24 hrs |
$300/month |
|
6 |
Tablet |
Galantamine |
Janssen pharmaceuticals |
4mg/12mg |
$200/month |
|
7 |
Extended-release capsule |
Memantine ER |
Allergan |
7mg – 28mg |
$250/month |
|
8 |
Combination tablet |
Namzaric (donepezil &memantine) |
Allergan |
10mg/28mg |
$400/month |
|
9 |
Tablet |
Rivamer |
Sun pharma |
3mg/6mg |
$20 - $50/month (India) |
|
10 |
Tablet |
Donetaz |
Intas pharmaceuticals |
5mg/10mg |
$15 - $40/month (India) |
NOVEL MARKETED FORMULATION:
Novel marketed formulation shows the recent advancements in Alzheimer treatment which have introduced modified therapies according to pathology of disease. It is noteworthy that monoclonal antibodies such as Lecanemab and Aducanumab have been developed to decrease amyloid beta plaques in the brain and slow down the disease progression [24].
Table 1.9 novel marketed formulation
|
Sr. No. |
Types |
Brand Name |
Company |
Dose |
Price (Approx) |
|
1 |
Nasal spray |
Aduhelm (Aducanumab) |
Biogen & Eisai |
IV Infusion 100mg/ml |
$28,000/year |
|
2 |
Intravenous infusion |
Leqembi (Lecanemab) |
Eisai & Biogen |
200-500mg IV every 2 weeks |
$26,500/year |
|
3 |
Subcutaneous injection |
Donanemab |
Eli Lilly |
Varies per protocol |
Expected $25,000 – 30,000/year |
|
4 |
Transdermal patch |
Rivastigmine patch |
Novartis |
4.6/13.3mg/ 24hrs |
$300 / month |
|
5 |
Extended-release capsule |
Namenda XR |
Allergan |
7mg – 28mg |
$250 / month |
|
6 |
Combination capsule |
Namzaric (Donepezil &memantine) |
Allergan |
10mg/28mg |
$400 / month |
PATENTS:
There is numerous patent which have been focusing on therapeutic strategies and treatment of Alzheimer by using Lecanemab drug. There are basically two types of patents which is based on Lecanemab specified patent and other is Broader Alzheimer's treatment patent. These patents highlight the innovative approaches for being pursued in Alzheimer's disease treatment [25-32].
Table 1.10 patents
|
Sr. No. |
Inventor |
Invention |
Patent no. &Year of grant |
Year of expiry |
Remarks |
|
1. |
Dennis Selkoe et al. |
Monoclonal antibodies for Alzheimer treatment |
US6355245B1 (2002) |
2022 |
Targeting amyloid-beta plaques. [25] |
|
2. |
Lars Lannfelt et al. |
BAN2401 (Lecanemab) |
US8986693B2 (2015) |
2032 |
Targets alpha beta protofibrils. |
|
3. |
Dale Schenk et al. |
Amyloid-beta immunotherapy |
US5849695A (1998) |
2015 |
Early immunotherapy approach.[26] |
|
4. |
Elan Pharmaceutical |
Beta-amyloid vaccine |
US6663883B1 (2003) |
2023 |
Vaccine based approach for AD [27] |
|
5. |
Genentech Inc. |
Anti-alpha beta antibodies |
US7537797B2 (2009) |
2029 |
Broad alpha beta binding strategy.[28] |
|
6. |
Wyeth LLC. |
Bapineuzumab (anti-alpha beta antibody) |
US7604811B2 (2009) |
2029 |
Failed in trials but foundational |
|
7. |
Biogen Inc. |
Aducanumab antibody |
US9463216B2 (2016) |
2036 |
First FDA approved antibody for AD. [29] |
|
8. |
Merck sharp &Dohme |
BACE inhibitor for Alzheimer’s |
US8501738B2 (2013) |
2033 |
Targeting beta secretase enzyme[30] |
|
9. |
Eli Lilly &co. |
Solanezumab Antibody |
US7767226B2 (2010) |
2030 |
Binds to soluble alpha beta monomers.[31] |
|
10. |
Eisai co., Ltd. |
Combination Alzheimer’s therapy |
US10772818B2 (2020) |
2040 |
Combination of antibody and inhibitor.[32] |
CONCLUSION:
Lecanemab ushers in a new era of disease-modifying treatments and is a major advancement in the treatment of Alzheimer's disease. Lecanemab, in contrast to conventional symptomatic therapies, targets the underlying pathology by attaching itself to amyloid-beta protofibrils, which are believed to be essential for the advancement of the disease. Its effectiveness in delaying cognitive and functional decline in patients with early-stage Alzheimer's disease is supported by clinical evidence, particularly from the CLARITY-AD Phase III trial. Despite being mild, this delay has a significant impact on the patient's autonomy and standard of living.
Lecanemab's promise is accompanied by several negative side effects, though. Neuropsychiatric symptoms, infusion-related reactions, and amyloid-related imaging abnormalities (ARIA-E and ARIA-H) were significant in both real-world data and clinical trials. Post-marketing surveillance, including data from the FDA Adverse Event Reporting System (FAERS), has reported 203 serious adverse events and 22 deaths, underlining the need for rigorous patient selection and ongoing monitoring during treatment. The presence of the ApoE ε4 gene variant appears to increase the risk of ARIA, further emphasizing the need for personalized approaches.
Notwithstanding its drawbacks, lecanemab represents a significant advancement in the creation of Alzheimer's medications. It promotes the search for earlier diagnosis and intervention and establishes the groundwork for future studies into immunotherapies that target neurodegenerative diseases. Lecanemab may change treatment guidelines as more information about its long-term safety and effectiveness becomes available. Millions of people afflicted by this crippling illness will eventually have hope thanks to ongoing innovation, regulatory monitoring, and clinical vigilance that will maximize its therapeutic potential while lowering risk.
REFERENCES




Arpita Lad, Ishi Kumari, Harsha Jagtap, Mansi Matkar, Lecanemab: A Breakthrough in Alzheimer’s Treatment and Therapeutics, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 4076-4091. https://doi.org/10.5281/zenodo.16608582
 10.5281/zenodo.16608582
10.5281/zenodo.16608582
