Shri K R Pandav Institute of Pharmacy
The treatment of vitiligo, a long-term depigmenting skin condition, is still quite difficult. Particularly with traditional oral or topical regimens, current treatments frequently encounter challenges such low Patient adherence, unfavourable side effects, and limited efficacy. This abstract investigates a new method of treating vitiligo by combining herbal remedies with transdermal drug delivery devices (tdds). Herbal compounds are attractive possibilities for vitiligo treatment because they provide a wealth of Naturally occurring bioactive chemicals with proven melanogenic, immunomodulatory, and antioxidant Qualities. However, poor skin penetration, degradation, and uneven bioavailability are common problems with topical administration. Patches, gels, microneedles, and nanoparticles are examples of transdermal. Drug delivery systems that offer a non-invasive, regulated, and targeted delivery platform that can get Over these restrictions. Herbal extracts can be formulated or encapsulated within tdds to improve Patient compliance, prolong therapeutic effects, decrease systemic toxicity, and increase percutaneous absorption. This synergistic approach has the potential to greatly increase the therapeutic efficacy of herbal remedies for vitiligo, providing a more secure, efficient, and patient-friendly therapy option. To thoroughly assess the pharmacokinetics, pharmacodynamics, safety, and clinical results of such integrated systems, more investigation is necessary.
Vitiligo
Vitiligo is a prevalent, chronic autoimmune disorder of the skin characterized by the loss or malfunction of melanocytes—the cells responsible for producing pigment in the skin, hair, and mucous membranes. Affecting approximately 0.5–2% of the global population, the disease manifests as distinct white or hypopigmented macules, sometimes accompanied by leukotrichi[1]. It can emerge at any age and affect individuals of all ethnicities, sexes, and skin tones, with common early lesions appearing on areas such as the fingertips, knuckles, lips, eyelids, toes, and genital regions. According to the 2011 consensus, vitiligo is clinically divided into two major types: nonsegmental vitiligo (NSV) and segmental vitiligo (SV) [2]. NSV typically shows symmetrical patterns and encompasses generalized, universal, acrofacial, mucosal, and mixed subtypes. SV, on the other hand, usually presents as asymmetrical patches that follow specific dermatomal distributions, commonly arise in childhood or early adulthood, and tend to stabilize after one to two years of progression [3].
The etiopathogenesis of vitiligo is intricate and multifaceted. It involves a combination of genetic susceptibility linked to immune-regulatory genes, intrinsic melanocyte defects that heighten vulnerability to chemical and oxidative stress, and environmental factors that trigger immune activation, primarily T-cell–mediated. Heat shock protein 70 (HSP70) plays a pivotal role in the initiation of depigmentation, with mutant variants demonstrating repigmenting potential in experimental models. Besides melanocytes, structural and functional changes have also been detected in keratinocytes, Merkel cells, and in physiological processes such as sweating and vascular responses[4].Accurate differential diagnosis from other hypopigmented or depigmented disorders— such as nevus depigmentosus and café-au-lait macules—is essential. Beyond being a cosmetic issue, vitiligo imposes a significant psychological and social burden, leading to distress, low self-esteem, and social withdrawal due to stigmatization[5] .The major therapeutic aims are to halt progression and achieve complete repigmentation.
Current standard treatments include phototherapy, topical corticosteroids, and topical calcineurin inhibitors, with combination therapies—such as afamelanotide with narrowband UVB—showing encouraging outcomes. In stable cases, especially SV, surgical interventions like non-cultured epidermal cell suspension (NCES) transplantation are gaining prominence as first-line options[6].
Hair follicle melanocytes, with their distinctive antigenic makeup, along with dermal stem cells, are being investigated for their contributions to repigmentation and disease stabilization.Ongoing advances in understanding vitiligo’s molecular and cellular mechanisms are guiding the development of more precise and effective therapies [7].
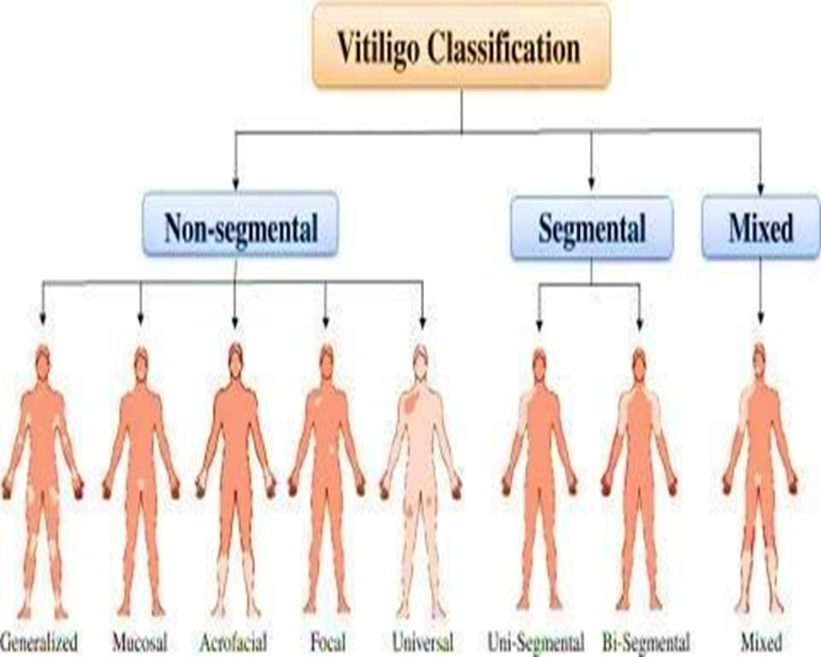
Fig 1: Classification of Vitiligo
Pathophysiology
Defective melanocyte adhesion to the basal epidermis, metabolic disruption linked to oxidative stress, genetic susceptibility, and dysregulated innate and adaptive immune responses are all components of its intricate and multifactorial pathogenesis, which culminates in the targeted destruction of melanocytes[8]. Even though there are many therapeutic modalities available, the effectiveness of the current corrective options is frequently limited, and they are linked to high rates of relapse[9]. To enhance patients' quality of life, new, secure, and more efficient therapeutic approaches are still desperately needed. Since the majority of vitiligo triggers center on inflammatory and autoimmune pathways that target melanocytes, there is mounting evidence that the immune system plays a critical role in the onset and progression of the condition[10].
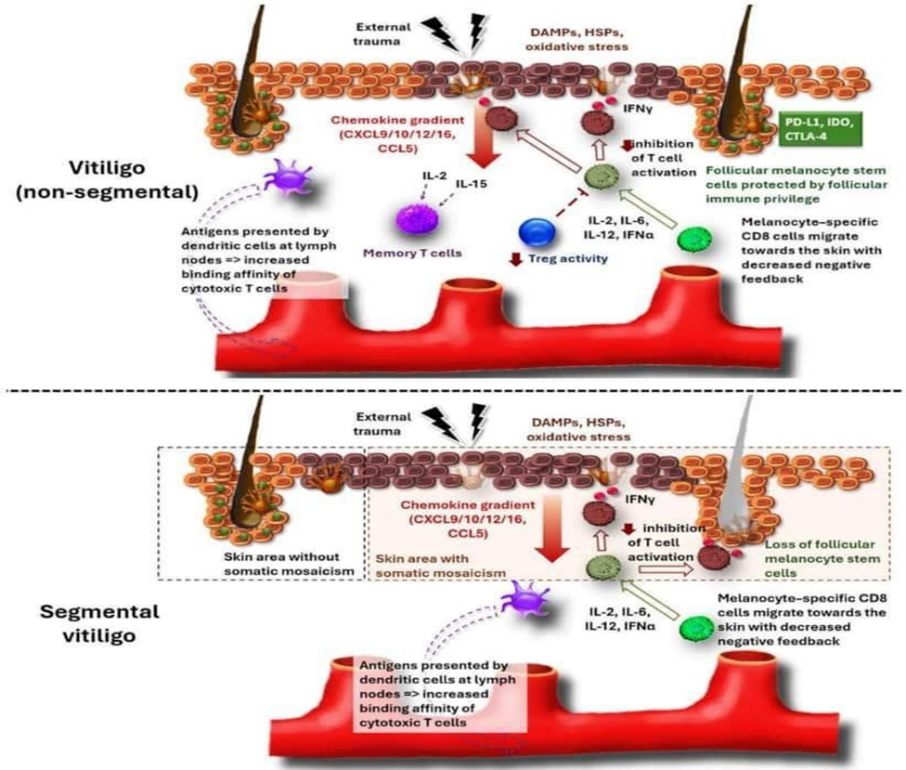
Fig 2: Pathophysiology of vitiligo
Transdermal drug delivery system
The goal of the transdermal drug delivery system (TDDS), which falls under the category of controlled drug delivery, is to administer the medication via the skin at a predefined and regulated rate[11].Transdermal drug delivery systems (TDDS), also known as “patches,” are dosage forms designed to deliver a therapeutically effective amount of drug across a patient’s skin. In order to deliver therapeutic agents through the human skin for systemic effects, the comprehensive morphological, biophysical and physicochemical properties of the skin are to be considered[12]. Transdermal delivery provides a leading edge over injectables and oral routes by increasing patient compliance and avoiding first pass metabolism respectively[13].
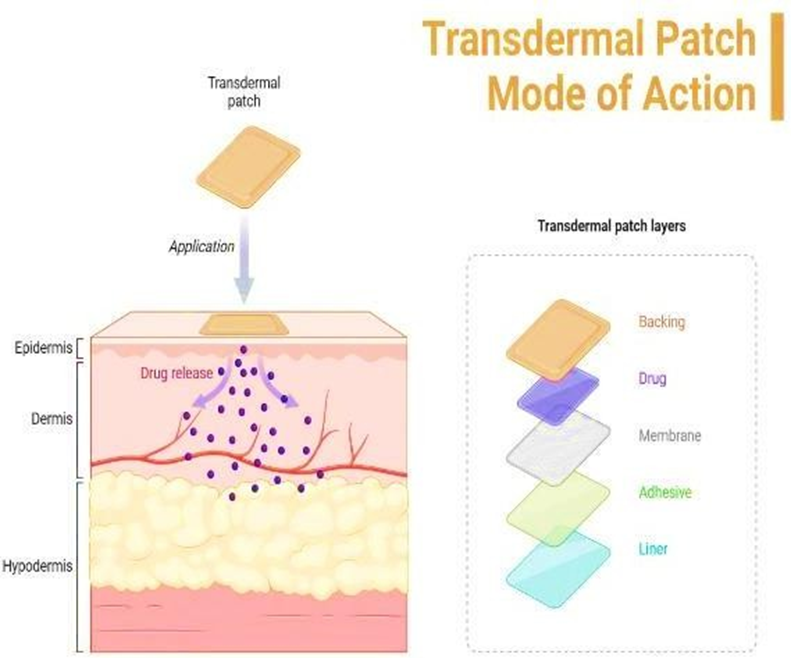
Fig 3: Mode of Action of Transdermal Patch
Method for Preparation of TDDS
Plant Profile
|
Sr. no. |
Natural components |
Biological source And family |
Chemical Constituents |
Mechanism Of Action |
|
1 |
Psoralea corylifolia (Babchi) |
Dried ripe fruits and seeds of Psoralea corylifolia Linn / Fabaceae (Leguminosae) [15]. |
coumarins, flavonoids, mero terpenes [22]. |
1. Making skin sensitive to sunlight increasing melanin production 2. Activating and multiplying melanocytes 3. Protecting melanocytes through antioxidant and anti-inflammatory actions 4. Supporting repigmentation when combined with UV exposure. |
|
2 |
Gingko Biloba |
Dried ripe fruits and seeds of Psoralea corylifolia Linn / Fabaceae (Leguminosae) [16]. |
terpene trilactones (ginkgolides), acylated flavonol glycosides (ginkgoghrelins), biflavones (ginkgetin), ginkgotides and ginkgolic acids. |
1. Reducing oxidative stress (antioxidant) 2. Modulating the immune system (anti-inflammatory) 3. Preventing melanocyte death 4. Supporting melanocyte regeneration & repigmentation 5. Improving skin microcirculation. |
|
3 |
Turmeric (curcuma) |
Dried rhizome of Curcuma longa Linn / Zingiberaceae [17]. |
curcuminoids phenolic acid, flavonoids. |
1.Turmeric helps in vitiligo by reducing oxidative stress, lowering autoimmune inflammation, protecting melanocytes from apoptosis, and creating a supportive environment for repigmentation. |
|
4 |
Aloe vera |
Dried juice/latex from the leaves of Aloe barbadensis Miller / Asphodelaceae (formerly Liliaceae/Xanthorrhoeaceae) [18]. |
Ascorbic acid, Catalase, Lipase, Aloetic acid, Mannose, Glucose, Xylan, Pure mannan, Cholesterol. |
1.Aloe vera helps in vitiligo by reducing oxidative stress, lowering inflammation, modulating immune responses, and supporting skin healing, which together protect melanocytes and aid repigmentation indirectly. |
|
5 |
Nigella sativa (Black Seed, Kalonji) |
Seeds and oil of Nigella sativa plant / Ranunculaceae (buttercup family) [19]. |
oils, proteins, carbohydrates, alkaloids, saponins, and essential oils [23]. |
1.Nigella sativa helps vitiligo by reducing oxidative stress, lowering inflammatory and autoimmune damage, protecting melanocytes from apoptosis, and promoting melanocyte proliferation, which together aid repigmentation. |
|
6 |
Cassia tora (Chakramarda) |
Annual herb, Senna tora (L.) Roxb. (syn. Cassia tora Linn.) / Fabaceae (Leguminosae) [20]. |
Anthraquinone glycosides, Flavonoids, emodin, chrysophanol, physion, rubrofusarine, methionine, tryptophan [24]. |
1.Cassia tora helps in vitiligo by reducing oxidative stress and inflammation, protecting melanocytes from damage, mildly enhancing melanin production, and supporting skin healing to encourage repigmentation. |
|
7 |
Neem (Azadirachta indica) |
All aerial parts: leaves, bark, fruit, seeds, oil / Meliaceae [21]. |
Nimbidin, Sodium nimbidate, Gedunin, Polysaccharide, Polysaccharide, Azadirachtin [25]. |
1.Neem helps in vitiligo by modulating autoimmune activity, reducing inflammation, protecting melanocytes from oxidative and apoptotic damage, and improving overall skin healing thereby supporting repigmentation. |
FUTURE SCOPE
The combination of herbal remedies with transdermal drug delivery systems (TDDS) presents a number of encouraging avenues for further study and clinical use in the treatment of vitiligo. It is anticipated that the development of more efficient and patient-friendly treatments will quicken as scientific knowledge of skin biology, herbal pharmacology, and nanotechnology advances. Important prospects for the future include:
CONCLUSION
An inventive and promising method of treating vitiligo is the combination of transdermal drug delivery systems and herbal remedies. Although herbal remedies like Aloe vera, Psoralea corylifolia, Curcuma longa, and Ginkgo biloba have beneficial therapeutic qualities like immunomodulation, antioxidant activity, and melanocyte regeneration stimulation, their clinical efficacy is frequently restricted by poor skin penetration and uneven bioavailability.
Overall, this review shows that a new, efficient, and patient-friendly approach to treating vitiligo may be possible by combining herbal remedies with contemporary transdermal drug delivery technologies. Such integrated systems may greatly enhance therapeutic results and broaden the future scope of dermatological care with further study and technological advancement.
REFERENCES







Punam Karande, Samyak Nannaware, Aniket Katkar, Mohd Wasim Vakeel Sheikh, Rameshwar Patil, Ahfaz Shah, Anchal Bajpayee, Aachal Kanekar, Integrating Herbal Medicine with Transdermal Drug Delivery: A Novel Approach to Vitiligo Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 4022-4029. https://doi.org/10.5281/zenodo.19339393
 10.5281/zenodo.19339393
10.5281/zenodo.19339393
