Vidya Niketan Institute of Pharmacy and Research Center, Bota.
Immunotherapy has rapidly evolved from a promising research field into a standard treatment option for cancer. As new methods move from laboratory studies to actual patient care, people with cancer are now benefiting from many drugs that have been approved by the U.S. Food and Drug Administration. Cancer occurs when cells in the body grow and develop uncontrollably, and it is one of the leading causes of death worldwide. There are more than 100 different types of cancer, each classified based on the specific tissue or organ affected in the human body. Until recently, the main treatments for cancer were surgery, radiation therapy, chemotherapy, and targeted therapies. In the past ten years, immuno-oncology (IO), which works by helping the immune system attack cancer cells, has become a new and important alternative to traditional cancer treatments. In 2019, the U.S. Food and Drug Administration and the European Medicines Agency sped up the approval process for these newer cancer drugs, which has led to their fast growth and adoption.
Cancer
Cancer is a group of diseases characterized by the uncontrolled growth, invasion, and spread of abnormal cells.
Types of Cancer:
Cancer is a group of diseases where cells grow out of control, spread to other parts of the body, and cause harm. There are several types of cancer, including:
Treatment:
The main treatments for cancer include surgery, chemotherapy, radiation therapy, immunotherapy, and targeted therapy.
Chemotherapy uses drugs to kill cancer cells, while immunotherapy is a newer and increasingly promising approach. Immunotherapy, also called biologic therapy or biotherapy, works by helping the body’s own immune system fight cancer more effectively. It’s a fast-growing and exciting area in oncology that aims to find, create, and deliver safe and effective treatments that can greatly improve the quality of life for patients with cancer.[2]
Immunotherapy:
Immunotherapy, also known as biologic therapy or biotherapy, is a type of cancer treatment that harnesses the body's immune system to recognize, target, and eliminate cancer cells.
Principles:
1.Stimulation: Helping the immune system work better to fight cancer.
2.Targeting: Making immune cells recognize and attack cancer cells directly.
3.Modulation: Controlling immune responses to make them more effective in fighting cancer.[3]
Why Cancer Immunotherapy:
Cancer immunotherapy has several benefits and is a promising treatment option.
Here's why it's used:
1.Targeted approach: Immunotherapy focuses on cancer cells, so it causes less damage to healthy cells.
2.Enhanced precision: It can find and attack cancer cells based on their unique markers.
3.Long-term potential: It might bring long-lasting remission or even a cure in some cases.
4.Combination therapy: It can be used with other treatments to improve results.
5.Minimized side effects: It usually causes fewer side effects compared to traditional chemotherapy.[4]
History:
Ancient Civilizations (3000 BCE - 500 CE)
1.Egyptian Edwin Smith Papyrus (1600 BCE): Describes breast cancer and mentions surgeries for treatment.
2.Hippocratic Oath (400 BCE): Refers to cancer as an imbalance of "black bile."
3.Galen (129-216 CE): Proposed theories about cancer, such as "bad blood" and the use of surgery.
Middle Ages (500 - 1500 CE)
1.Surgical treatments: Amputations and cauterization were common.
2.Herbal remedies: Plant-based treatments like willow bark were used.[5]
Renaissance and Enlightenment (1500 - 1800 CE)
1.Andreas Vesalius (1514-1564): Made detailed descriptions of cancer anatomy.
2.Giovanni Morgagni (1682-1771): Described cancerous tumors.
3.Percivall Pott (1714-1788): Found a link between chimney sweeps' work and scrotal cancer.
Modern Era (1800 - 1900 CE)
1.Wilhelm Conrad Rontgen (1845-1923): Discovered X-rays.
2.Marie Curie (1867-1934): Developed radiation therapy.
3.William Stewart Halsted (1852-1922): Improved the mastectomy procedure.[6]
20th Century (1900 - 2000 CE)
1.Cancer research institutions were started.
2.Chemotherapy was developed (1940s-1950s).
3.Radiation therapy advanced.
4.Immunotherapy began to emerge in the 1970s.
5.Targeted therapies were introduced (1980s-1990s).
Contemporary Era (2000 CE - present)
1.Precision medicine is being used.
2.Immunotherapy is expanding.
3.CAR-T cell therapy is now a treatment option.
4.Gene editing techniques like CRISPR are being used.
5.Liquid biopsies are being used to detect cancer.[7]
Types of Immunotherapies:
There are several types of immunotherapies, which can be classified as:
A) Monoclonal Antibodies
1.Rituximab (Rituxan): Targets CD20 on B cells
2.Trastuzumab (Herceptin): Targets HER2 on breast cancer cells
3.Cetuximab (Erbitux): Targets EGFR on colorectal cancer cells
B) Checkpoint Inhibitors
1.Pembrolizumab (Keytruda): Targets PD-1
2.Nivolumab (Opdivo): Targets PD-1
3.Ipilimumab (Yervoy): Targets CTLA-4[8]
C) Cancer Vaccines
1.Sipuleucel-T (Provenge): Used for prostate cancer
2.Human Papillomavirus (HPV) vaccine: Prevents cervical, anal, and oropharyngeal cancers
3.Personalized neoantigen-based vaccines
D) Adoptive T-Cell Therapy
1.CAR-T cell therapy: T cells are genetically changed
2.Tumor-infiltrating lymphocyte (TIL) therapy
3.Cytokine-induced killer (CIK) cell therapy [9]
E) Immunomodulators
1.Lenalidomide (Revlimid): Boosts T-cell and NK-cell activity
2.Pomalidomide (Pomalyst): Similar to lenalidomide
3.Interferon-alpha (IFN-α): Helps the immune system respond
F) Cytokines
1.Interleukin-2 (IL-2): Encourages T-cell growth
2.Interferon-alpha (IFN-α): Helps the immune system respond
3.Tumor necrosis factor-alpha (TNF-α): Causes cancer cells to die [10]
G) Gene Therapy
1.Gene editing (CRISPR/Cas9)
2.Gene transfer: Adding tumor suppressor genes
3.RNA-based therapies: Silencing cancer-causing genes [11]
Classification of Immunotherapy:
a) Monoclonal antibodies (MABs):
One kind of immunotherapy is monoclonal antibodies. They help the immune system and support it in beating cancer. Some MABs are more focused than others. By blocking certain signals, they can stop cancer cells from dividing. These are proteins in the blood that help fight disease. "Monoclonal" means one type, so a monoclonal antibody is made up of many copies of the same antibody. A monoclonal antibody finds and targets specific proteins on cells. Some are focused on cancer, others on immune cell proteins. Each monoclonal antibody is tailored to a particular protein. Their effects depend on which protein they target. MABs are used in different ways as immunotherapy.[12]
They Can:
* Help the immune system locate and destroy cancerous cells
* Influence other cells to help fight cancer
Even though cancer cells are abnormal, the immune system has a hard time recognizing them because they come from normal cells.
Some MABs stick to cancer cells, making them easier for immune cells to find. This is called antibody-dependent cell-mediated cytotoxicity (ADCC). Other MABs interact with immune system cells. Checkpoint inhibitors are one example of immunotherapy. These work by blocking proteins that stop the immune system from attacking cancer cells.[13]
Side Effects:
* Skin issues such as redness, soreness, or an itchy rash
* Diarrhea
* Fatigue
* Flu-like symptoms such as chills, fever, and dizziness
* Nausea or vomiting[14]
a) CAR T- cell Therapy:
The process of using chimeric antigen receptor T-cells is complex and requires expert care.
During this process, a healthcare professional takes a sample of your T cells, modifies them in a laboratory, and then returns them to your body. Once these modified T cells are back in your bloodstream, they are ready to fight cancer. The CAR T-cells are designed to recognize and[15]
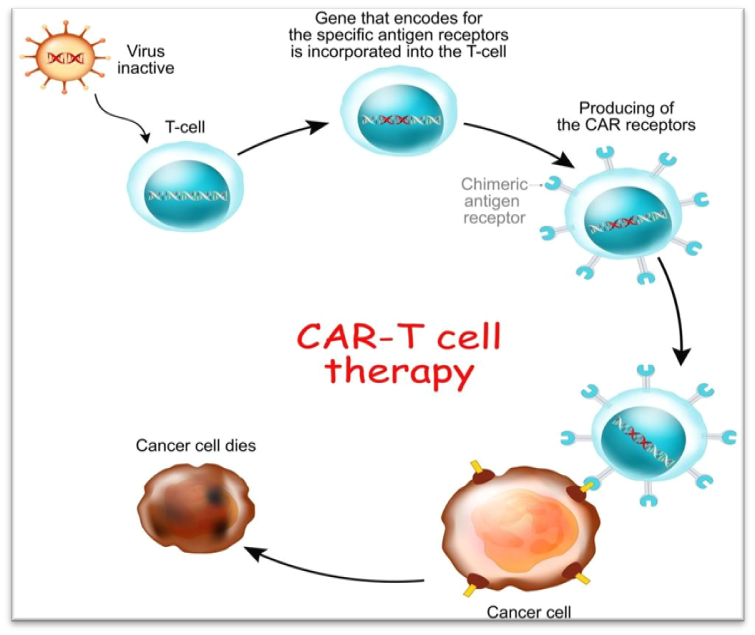
Figure. CAR-T Cell Therapy
Side effects:
- Allergic reactions
- Cytokine-release syndrome
- Brain-related issues (neurological side effects)
- Increased risk of infection
- High levels of uric acid in the blood due to the fast breakdown of cancer cells (tumor lysis)[16] attack a specific protein found on cancer cells.
When T cells are removed from your blood, they are genetically changed in a lab by adding a special gene that creates a synthetic receptor, known as a chimeric antigen receptor (CAR).
This receptor helps the T cells detect certain proteins that are present on cancer cells. After the modification, the CAR T-cells are given back to you. Each CAR T-cell treatment is customized to match the specific protein on the tumor it is meant to attack. For example, some types of lymphoma and leukemia have a protein called CD19, and CAR T-cell treatments for these cancers are designed to target CD19. If CD19 is not present, these treatments won’t work.[15]
Advantages of immunotherapy:
1.Some cancers, like skin cancer, don't respond well to radiation or chemotherapy but may shrink after immunotherapy.
2.Immunotherapy can help other treatments, such as chemotherapy, work more effectively.
3.It often causes fewer side effects because it mainly targets the immune system and no other healthy cells in the body.
Disadvantages of immunotherapy:
1.The treatment area might become painful, itchy, swollen, red, or sore.
2.Some immunotherapies can overstimulate the immune system, causing flu-like symptoms such as fever, shivers, and tiredness.
3.It can lead to problems like swelling, fluid retention, irregular heartbeat, headaches, and diarrhea.[16]
Case study on Immuno-oncology
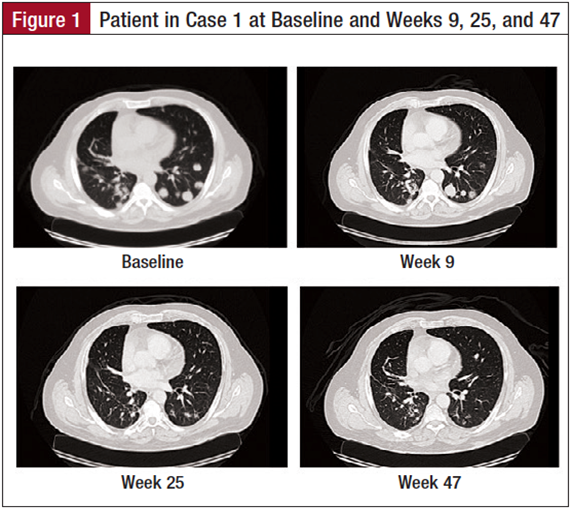
CASE1
The patient is a 60-year-old man with a 5–pack-year smoking history who quit smoking 31 years prior to presentation (Figure 1). He began complaining of right arm pain in November 2011. A chest computed tomography (CT) scan showed a 4.5-cm lesion in the right upper lobe abutting the pleura. A percutaneous needle biopsy of the lung mass was undertaken, which showed sheets of malignant-appearing cells with glandular features and areas of necrosis. The tumor cells were positive for TTF1, napsin A, cytokeratin (CK) 7, and CD56, and negative for CK20, CK5/6, p63, chromogranin, and synaptophysin consistent with primary adenocarcinoma of the lung. Upon review of his case in a multidisciplinary setting, he was offered chemotherapy with cisplatin and pemetrexed as an initial course of therapy. He had an evaluable response to chemotherapy with evidence of tumor shrinkage, enabling him to be referred for a surgical resection. He underwent a right upper lobectomy. Pathology was consistent with high-grade carcinoma with a prominent neuroendocrine pattern. The tumor was 4.0 cm in greatest dimension and approached the perivascular soft tissue. Mediastinal lymph nodes were negative for any evidence of malignancy. He did not receive chemotherapy in the adjuvant setting.
Six months following the patient’s surgery, surveillance CT scans showed evidence of new lesions in the left lung. Percutaneous biopsy of one of the pulmonary lesions was consistent with recurrent TTF1-positive, CK 7-positive, napsin A-negative, and thyroglobulin-negative cells consistent with adenocarcinoma of the lung. He was negative for EGFR and ALK mutations. Because of his prior experience with chemotherapy, the patient was reluctant to undergo further chemotherapy for his now stage IV disease. He opted to participate in a dendritic cell vaccine study to which he initially had a mixed response followed by progression 3 months after enrollment. Upon progression, he was offered treatment with systemic chemotherapy. However, the patient requested to pursue various trial options, ultimately presenting to our clinic for consideration of an immunotherapy trial with a checkpoint inhibitor.
In July 2013, the patient was evaluated for an anti–PD-1 antibody immunotherapy trial and underwent a biopsy of a pulmonary lesion, which was tested for PD-L1 protein expression. The disease was found to express PD-L1. His CT scans prior to enrollment indicated the presence of multiple bilateral pulmonary nodules, the largest of which was 2.5 cm. There was no evidence of pleural effusion, but the patient had a small pericardial effusion. His first scan 9 weeks after initiating therapy indicated stable disease; all subsequent scans have indicated significant tumor shrinkage. The patient has tolerated therapy well with no significant side effects, except for complaint of bilateral buccal mucosal swelling and sensitivity. He has also developed oral ulcers that have been managed well with oral lidocaine and a steroid solution. He has had no other side effects, and continues to do well on the trial 1 year after enrollment.
Case 2: -
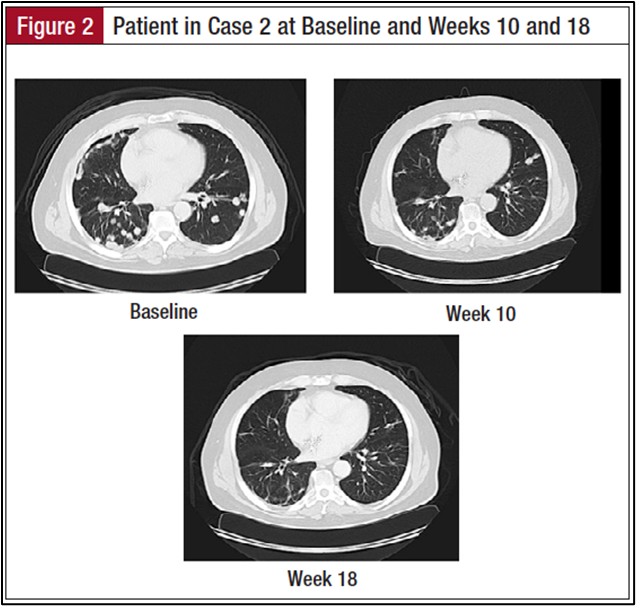
The patient is a 66-year-old man with a medical history of hypertension and a remote smoking history who initially palpated a mass on the left side of his neck in July 2008 (Figure 2). He was referred to an ear, nose, and throat specialist, and was noted to have a mass overlying and possibly involving his left parotid gland. The patient underwent a fine needle aspiration of the lesion, but pathology was nondiagnostic. He subsequently underwent a neck magnetic resonance imaging, which showed the lesion to be localized to the left parotid. In October 2008, he underwent a left total parotidectomy and left modified radical neck dissection. Pathology from the resection was consistent with a 3.7-cm invasive, high-grade, basaloid squamous cell carcinoma involving the parotid gland and periparotid soft tissue. Evidence of malignancy was seen in the deep parotid tissue as well as in 1 of 5 dissected lymph nodes.
There was evidence of perineural invasion by the tumor. The tumor was positive for p63 and KER 5/6, and negative for S100, GFAP, EMA, CEA, and CD117. In the adjuvant setting, the patient received concurrent carboplatin (Paraplatin), docetaxel (Taxotere), and radiation. He completed his course in January 2009, underwent surveillance scans after completion of his concurrent therapy, and did well until February 2011. Surveillance images at that time noted a lesion in the lung and a lytic lesion in the iliac bone. In July 2011, he underwent a percutaneous needle biopsy of the right iliac lesion with pathology again being consistent with metastatic carcinoma consistent with the patient’s history of basaloid squamous cell carcinoma. The tissue was positive for p63, SMA, and pancreatin AE1/AE3, and negative for Vimentin, S100, CD117, CK5/6,andEMA.
Given the stage IV diagnosis, the patient resumed chemotherapy with vinorelbine shortly after the biopsy. After 2 cycles, scans showed disease progression, and therapy was changed to carboplatin and docetaxel with continued progression. He then received bevacizumab and everolimus with no improvement in his disease. Subsequent therapy with cetuximab also did not provide benefit. Upon progression, he was enrolled in a clinical trial with a novel vascular endothelial growth factor inhibitor that provided stabilization of his disease for 4 months, after which his disease began to progress.
In September 2013, the patient presented for consideration of an immunotherapy clinical trial. He was subsequently enrolled in an anti–PD-L1 antibody trial that did not mandate PD-L1 protein expression testing. He underwent a fresh biopsy for the trial, but his PD-L1 protein expression was unknown at the time of his enrollment. Baseline scans prior to initiating the trial indicated evidence of left mastoidectomy and radical left neck surgery. There was evidence of numerous pulmonary nodules and pleural nodularity bilaterally. The largest pulmonary nodule measured 5.1 cm. There was a small right pleural effusion, and there was also evidence of a 5.2-cm lytic and sclerotic lesion involving the right ilium.
The patient began on the anti–PD-L1 antibody with his first infusion in December 2013. His first scans 6 weeks after enrolling into the study indicated evidence of stable disease with minimal shrinkage of his pulmonary lesions. Subsequent scans have shown a dramatic reduction in the size and burden of his pulmonary nodules. His pleural effusion has resolved. The patient has been tolerating the therapy well with no side effects. He is continuing to receive the anti–PD-L1 antibody every 2 weeks with continued evidence of tumorshrinkage9monthsafterenrollinginthestudy.[17]
CONCLUSION: -
IO is changing the treatment of both solid and hematological tumors by taking a completely different approach to cancer therapy. This new therapy approach is still in its early stages, so considerable work needs to be done to optimize the use of these cutting-edge medications, lessen their adverse effects, and figure out how to incorporate them into the current standard of care. It will also be challenging to integrate them into healthcare systems in a way that is both financially viable and increases patient availability, given their high cost. The latest revolution in immunology has been centered on ICPs, as evidenced by the multiple approvals of two important antibodies (pembrolizumab and ipilimumab, respectively) for the inhibition of PD-1/PD-L1 and CTLA-4. Due to their efficacy, IO medications and conventional therapy have been discussed extensively. Some patients experience significant side effects from the ICP is, despite their possible therapeutic value. While they are not the same as those experienced with conventional cancer treatments, these side effects are frequent. Because of this, monitoring long-term results and anticipating and controlling these adverse effects are becoming more and more important aspects of clinical research. This needs to result in management guidelines for these novel medicines and motivate clinicians to incorporate them into treatment regimens as quickly as feasible.
REFERENCES


Sor Sanskruti*, Shete Dipali, Mane Tanishka, Immuno-Oncology Treatment for Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1221-1230 https://doi.org/10.5281/zenodo.17562073
 10.5281/zenodo.17562073
10.5281/zenodo.17562073
