Department of Pharmacology, Dr. Vedprakash Patil Pharmacy College, Aurangabad
Casearia graveolens, a medicinal plant traditionally used to treat various ailments, including liver-related disorders, has shown promising hepatoprotective potential. This comprehensive review aims to summarize the current state of knowledge on the hepatoprotective effects of Casearia graveolens, focusing on its phytochemical profile, pharmacological activities, and potential therapeutic applications. The plant's rich composition of bioactive compounds, including clerodane-type diterpenoids, flavonoids, and coumarins, provides a promising foundation for its hepatoprotective effects. While preliminary studies suggest its potential benefits, further research is needed to fully elucidate its mechanisms of action, efficacy, and safety. This review highlights the need for systematic investigation into the hepatoprotective properties of Casearia graveolens, which could pave the way for developing safe and effective plant-based therapeutic candidates for managing hepatic disorders.
THE LIVER: Structure and Functions Anatomy and Physiology of the Liver
The liver is the largest glandular organ in the human body and performs over 500 critical physiological functions essential for maintaining homeostasis. In adults, it typically weighs between 1.2 and 1.5 kilograms and resides in the right upper quadrant of the abdominal cavity, situated just beneath the diaphragm and partially protected by the rib cage. It is suspended from the diaphragm by the falciform ligament, which anatomically divides the liver into right and left lobes. Functionally, the liver is subdivided into lobes and further segmented based on Couinaud’s classification, which defines eight distinct segments, each independently supplied by a branch of the portal vein, hepatic artery, and bile duct. This segmental architecture is crucial in hepatic surgery and liver transplantation, as it enables selective resection or grafting with preserved vascular and biliary integrity. (Bruha et al., 2012; Seitz et al., 2018)
A unique feature of the liver is its dual blood supply. Approximately 75% of the liver’s blood flow is derived from the portal vein, which delivers nutrient-rich but oxygen-poor blood from the gastrointestinal tract, pancreas, and spleen. The remaining 25% is supplied by the hepatic artery, which provides oxygenated blood from the systemic circulation. These two blood sources mix within the hepatic sinusoids—low-pressure, fenestrated capillary networks lined by specialized endothelial cells that facilitate efficient exchange of solutes between blood and hepatocytes. At the microscopic level, the liver is composed of hepatic lobules, which are hexagonal structural units centered around a central vein. At each corner of the lobule lies a portal triad, consisting of branches of the portal vein, hepatic artery, and bile duct. Hepatocytes, the principal parenchymal cells of the liver, are arranged in radial plates extending from the central vein and are in direct contact with sinusoidal blood. This anatomical arrangement enables rapid uptake and processing of nutrients, hormones, toxins, and xenobiotics. (Gougol et al., 2021; Singal et al., 2024; Suriawinata and Thung, 2006)
In addition to hepatocytes, the liver houses several non-parenchymal cells with distinct functions:
This intricate cellular and vascular organization enables the liver to function as a metabolic hub, detoxification center, endocrine regulator, and immune-modulatory organ. One of the most remarkable features of the liver is its regenerative capacity. Under normal physiological conditions, the liver can regenerate up to 70% of its mass following partial hepatectomy. This regenerative potential is fundamental to recovery after liver injury and forms the biological basis for living-donor liver transplantation and hepatic resection procedures.
Key Metabolic, Detoxification, and Synthetic Roles of the Liver
The liver plays a central role in maintaining systemic metabolic equilibrium and is essential for numerous physiological processes involving the metabolism of carbohydrates, lipids, and proteins, as well as the detoxification of harmful substances and the biosynthesis of critical biomolecules.
In carbohydrate metabolism, the liver regulates blood glucose levels through three primary mechanisms: glycogenesis, glycogenolysis, and gluconeogenesis. During the postprandial state, the liver converts excess glucose into glycogen for storage, preventing hyperglycemia. In contrast, during fasting conditions, it breaks down stored glycogen into glucose and also synthesizes glucose from non-carbohydrate sources such as lactate, glycerol, and glucogenic amino acids, ensuring a continuous supply of energy.
Lipid metabolism is another crucial hepatic function. The liver is the primary site for both the synthesis and degradation of fatty acids and cholesterol. It produces very low-density lipoproteins (VLDL) to transport triglycerides to peripheral tissues and facilitates the oxidation of fatty acids through β-oxidation to generate ATP. Additionally, during prolonged fasting or starvation, the liver produces ketone bodies as an alternative energy source. In terms of protein metabolism, the liver is responsible for the deamination of amino acids, a process that generates ammonia, a toxic byproduct. This ammonia is promptly converted to urea via the urea cycle and excreted by the kidneys. The liver also synthesizes most of the body’s plasma proteins, including albumin, which maintains plasma oncotic pressure; clotting factors such as fibrinogen, prothrombin, and Factors V, VII, IX, and X; transport proteins like transferrin and ceruloplasmin; and various binding globulins involved in hormone and mineral transport. A reduction in the levels of these proteins, particularly clotting factors, is a hallmark of impaired liver function and is commonly observed in advanced liver disease. (Sumadewi, 2023)
Detoxification is among the liver’s most vital roles. It acts as the principal site for the biotransformation of xenobiotics, environmental toxins, drugs, and metabolic waste products. Detoxification occurs in two phases. Phase I reactions, primarily mediated by cytochrome P450 enzymes, involve oxidation, reduction, or hydrolysis to introduce reactive groups. Phase II reactions involve conjugation processes such as glucuronidation, sulfation, and acetylation, which increase the water solubility of metabolites, facilitating their excretion via urine or bile. The liver also metabolizes endogenous compounds, including steroid hormones and bilirubin, and inactivates exogenous substances like paracetamol and ethanol. When the liver’s detoxification capacity is overwhelmed, such as during drug overdose, hepatocellular injury can occur, forming the pathological basis for many experimental models used in hepatoprotective research.(Doshi et al., 2021; Sumadewi, 2023)
Micronutrient Storage and Metal Metabolism:
The liver plays a critical role in regulating iron and copper metabolism, essential for systemic micronutrient balance. It synthesizes hepcidin, a key regulatory hormone that controls intestinal iron absorption and systemic iron distribution. In addition to regulating trace minerals, the liver also serves as a storage site for fat-soluble vitamins A, D, E, and K, as well as iron and copper, further underscoring its role in maintaining nutritional homeostasis.
Another vital exocrine function of the liver is bile production, which is essential for digestion and the elimination of metabolic waste. Hepatocytes continuously synthesize and secrete bile, a complex fluid composed primarily of bile acids (cholic and chenodeoxycholic acids), phospholipids (mainly lecithin), cholesterol, bilirubin, electrolytes, and water. Bile acids are synthesized from cholesterol via a highly regulated enzymatic pathway and are subsequently conjugated with taurine or glycine to enhance their solubility and functional activity. Once formed, bile is secreted into the bile canaliculi, narrow channels situated between adjacent hepatocytes. It then flows through an intricate system of bile ductules and hepatic ducts, eventually merging into the common bile duct. Depending on the physiological state, bile is either stored in the gallbladder or directly released into the duodenum. In the intestinal lumen, bile acids emulsify dietary fats, facilitating the action of pancreatic lipase and enhancing the absorption of fat-soluble vitamins (A, D, E, and K). Approximately 95% of bile acids are reabsorbed in the terminal ileum and returned to the liver via the portal circulation through a highly efficient process known as enterohepatic circulation, which conserves bile acids and ensures their repeated utilization in digestion. Bile also serves as the primary excretory route for bilirubin, a toxic end-product of heme catabolism. Unconjugated bilirubin is taken up by hepatocytes, conjugated with glucuronic acid by the enzyme UDP-glucuronosyltransferase 1A1 (UGT1A1), and excreted into bile. Any disruption in this process can lead to jaundice or cholestasis, signaling impaired hepatic function. In addition to bilirubin, bile facilitates the elimination of excess cholesterol, heavy metals, xenobiotics, and lipophilic drugs, many of which are not effectively cleared by the kidneys. Thus, bile secretion represents a critical detoxification pathway within hepatic physiology.
Pathological impairments in bile formation or flow are central to the development of several cholestatic liver diseases, including primary biliary cholangitis, biliary cirrhosis, and obstructive cholestasis. These conditions are marked by reduced bile secretion, toxic bile acid accumulation, and progressive inflammation and fibrosis within the liver. Consequently, disturbances in bile homeostasis not only compromise digestive function but also contribute to hepatocellular damage, highlighting the essential role of bile physiology in both health and disease.(Bacon et al., 1984; Luza et al., 1996)

Figure 1: Micronutrient storage and metal metabolism Global and Indian Epidemiology of Liver Diseases
Global Burden of Liver Disease
Liver diseases constitute a major and escalating global health concern, responsible for approximately two million deaths each year—accounting for nearly 4% of all global mortality, or one in every 25 deaths worldwide. A significant portion of these deaths is linked to chronic liver conditions, particularly cirrhosis and hepatocellular carcinoma (HCC), the most common form of primary liver cancer. Although acute liver failure—often caused by acute viral hepatitis—represents a smaller share of liver-related mortality, its clinical significance remains considerable. Notably, there is a marked gender disparity, with nearly two-thirds of liver disease-related deaths occurring in males, highlighting the disproportionate burden of liver disease in men. (Jain et al., 2024; Sakamoto et al., 2017; Wong et al., 2019)
The etiology of chronic liver disease is multifactorial and varies geographically, with the leading global causes including chronic viral hepatitis (HBV and HCV), alcohol-related liver disease (ALD), and non-alcoholic fatty liver disease (NAFLD), recently redefined as metabolic dysfunction-associated fatty liver disease (MAFLD). Among these, hepatitis B virus (HBV) and hepatitis C virus (HCV) have historically been the most significant contributors to cirrhosis and hepatocellular carcinoma, affecting over 250 million and several tens of millions of individuals worldwide, respectively. Together, HBV and HCV infections account for a considerable proportion of global liver-related mortality. (Malviya and Verma, 2023; Mondal et al., 2022; Sumadewi, 2023)
Although vaccination initiatives and antiviral therapies have reduced the prevalence of viral hepatitis in many high-income regions, HBV and HCV remain pressing public health concerns in Asia and Sub-Saharan Africa. In these areas, limited access to early diagnosis and treatment significantly hinders disease control efforts. Alcohol consumption represents another major driver of liver disease. Alcoholic liver disease (ALD) encompasses a spectrum of hepatic injury, ranging from simple steatosis to alcoholic hepatitis, progressive fibrosis, and cirrhosis. As of 2018, an estimated 26 million individuals worldwide were affected by ALD—a figure that continues to rise, particularly in regions experiencing increased alcohol intake. Challenges such as delayed diagnosis, underreporting, and insufficient access to healthcare services further compound the burden and mortality associated with alcohol-related liver damage. (Allen et al., 2016; Smith et al., 2021; Sun et al., 2022)
In recent years, non-alcoholic fatty liver disease (NAFLD) has emerged as the most prevalent chronic liver disorder worldwide, driven largely by the escalating global prevalence of obesity, physical inactivity, and type 2 diabetes mellitus. Current estimates suggest that NAFLD affects approximately 25% of the adult population globally—representing over one billion individuals with metabolic-associated hepatic steatosis. Of particular concern is the progression of a subset of these individuals to non-alcoholic steatohepatitis (NASH), a more severe phenotype marked by hepatic inflammation and fibrosis, which can eventually culminate in cirrhosis and end- stage liver disease. Increasingly, NAFLD and NASH have become major indications for liver transplantation, especially among patients lacking traditional etiological factors such as viral hepatitis or alcohol misuse. (Liu et al., 2022; Mitra et al., 2020; Younossi et al., 2020)
The global distribution of liver disease burden reflects the regional dominance of various etiologies. For instance, East Asia and Sub-Saharan Africa continue to bear a disproportionately high burden of HBV-associated cirrhosis and hepatocellular carcinoma (HCC), attributable to historical endemic transmission and gaps in early childhood immunization coverage. On the other hand, countries in Eastern Europe and segments of the Americas exhibit a high prevalence of alcohol-related liver disease (ALD), which is often correlated with socioeconomic and behavioral determinants. Concurrently, NAFLD is becoming a universal public health issue, transcending traditional boundaries between developed and developing nations. In low- and middle-income countries, rapid urbanization and shifting dietary habits towards energy-dense, Westernized food—coupled with a rise in sedentary behavior—are accelerating the incidence of NAFLD, even in regions where viral hepatitis had previously been the primary driver of liver pathology. (Butt et al., 2015; Jindal et al., 2022; Wong and Gish, n.d.; Zhang et al., 2022)
This multifaceted interaction of infectious, metabolic, and lifestyle-related risk factors underscores the likelihood of an increasing global burden of liver disease. Without timely and comprehensive interventions, the morbidity and mortality associated with chronic liver diseases are expected to rise further. A multipronged approach is critical to reversing these trends, including: widespread implementation of HBV vaccination; routine screening and early diagnosis of liver disease; policy-driven measures to limit harmful alcohol consumption; large- scale lifestyle modification initiatives targeting diet and physical activity; and improved access to effective antiviral therapies and metabolic disease management. Together, these targeted public health strategies are essential to mitigate the long-term impact of chronic liver disease and reduce future global liver-related mortality and disability. (Mahtab et al., 2015; Qi et al., 2015; Younossi et al., 2016)
Liver Disease Burden in India
India carries a considerable share of the global liver disease burden, driven by its large and diverse population, coupled with the presence of both infectious and metabolic risk factors. Liver diseases are now recognized among the top ten leading causes of death in the country, reflecting a growing public health concern. According to recent epidemiological estimates, approximately 250,000 deaths per year in India are attributed to liver-related disorders. Among these, cirrhosis accounts for a major portion, with the country's age-standardized death rate for cirrhosis surpassing the global mean. This highlights the urgent need for targeted interventions in screening, prevention, and management of liver diseases within the Indian healthcare framework. (Bhaumik et al., 2015; Mondal et al., 2022; Sumadewi, 2023)
The Indian context presents a dual burden of liver disease:
Infectious causes, notably hepatitis B virus (HBV) and hepatitis C virus (HCV), remain endemic due to heterogeneous vaccine coverage, unsafe blood transfusion practices, and limited public health education, particularly in rural and semi-urban populations.
Non-infectious etiologies, including non-alcoholic fatty liver disease (NAFLD), alcohol-related liver disease (ALD), and drug-induced liver injury (DILI), are rapidly increasing due to urbanization, lifestyle transitions, and escalating alcohol consumption.
Non-alcoholic fatty liver disease (NAFLD) has emerged as the most widespread chronic liver disorder in urban India, with prevalence estimates reaching up to 30% among adults in certain metropolitan populations. This rising trend is closely associated with increasing rates of obesity, type 2 diabetes mellitus, and metabolic syndrome—key risk factors that accelerate the progression of NAFLD to its more severe form, non-alcoholic steatohepatitis (NASH), which in turn can lead to advanced fibrosis, cirrhosis, and end-stage liver failure. As a result, NAFLD is expected to become the most common indication for liver transplantation in India within the next decade. (Bhaumik et al., 2015; Gan et al., 2025; Mondal et al., 2022; Yu et al., 2018; Zhang et al., 2022)
In contrast, rural and socioeconomically disadvantaged areas of the country face unique challenges in liver disease management. The burden is compounded by delayed or missed diagnoses due to lack of awareness and inadequate access to diagnostic services. Specialist hepatology care is often unavailable in these regions, and the health infrastructure is frequently ill-equipped to handle the complexity of chronic liver disease. Additionally, the widespread use of traditional herbal remedies—often lacking standardization and safety validation— alongside unregulated over-the-counter medications and environmental hepatotoxins (such as contaminated water or pesticide exposure) further contribute to liver injury and disease progression. Together, these urban and rural dynamics underscore the need for a comprehensive national strategy encompassing early detection, public awareness, integration of metabolic health management, and stricter regulation of hepatotoxic exposures to curb the growing impact of NAFLD and other chronic liver diseases in India. (Allen et al., 2016; Sakamoto et al., 2017; Smith et al., 2021; Sumadewi, 2023)
Public Health Implications and Strategic Response
The increasing liver disease burden in India necessitates an integrated and proactive public health approach focused on both prevention and early intervention. Key components of such a strategy include:
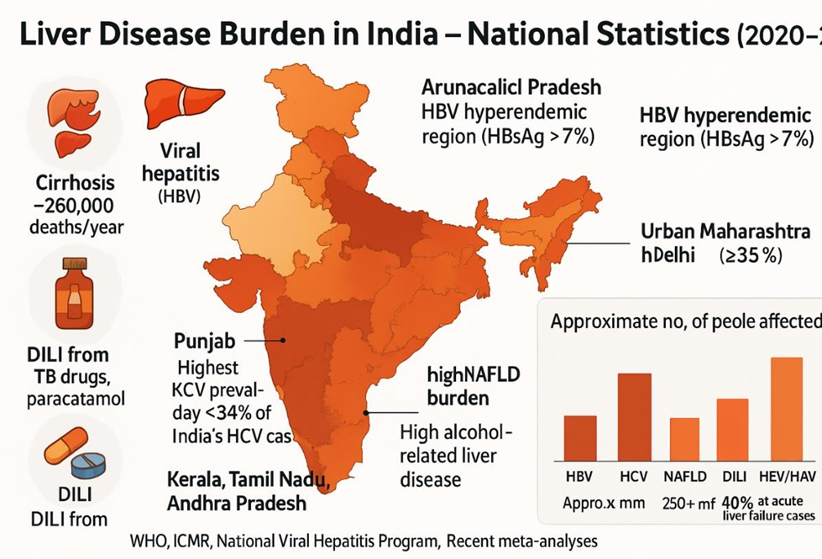
Figure 2: Liver disease burden in India – National Statistic (2020-2025)
PATHOPHYSIOLOGY OF LIVER INJURY
Mechanisms of Hepatic Injury
Liver injury, whether acute or chronic, can be initiated by a diverse range of etiological factors, including alcohol consumption, viral infections, drug-induced hepatotoxicity, chemical exposure, metabolic dysfunction, and autoimmune disorders. Despite this diversity, these insults converge on several shared pathophysiological mechanisms, including oxidative stress, mitochondrial dysfunction, cytokine dysregulation, and the activation of regulated cell death pathways notably apoptosis, necroptosis, and pyroptosis. These events collectively result in hepatocyte injury, immune system activation, and extracellular matrix remodeling, ultimately driving the progression toward fibrosis, cirrhosis, and in some cases, hepatocellular carcinoma (HCC). Understanding these mechanistic underpinnings is essential for identifying novel therapeutic targets, particularly for the development and scientific validation of hepatoprotective agents derived from medicinal plants, and for designing interventions aimed at halting or reversing liver damage at various stages. (Chen et al., 2024)
Oxidative Stress
Oxidative stress is a key early event in liver injury, arising from an imbalance between the production of reactive oxygen species (ROS) and the liver’s antioxidant defenses. Under physiological conditions, ROS such as superoxide anion (O??), hydroxyl radical (•OH), and hydrogen peroxide (H?O?) are generated at low levels during mitochondrial respiration, xenobiotic metabolism, and immune responses. Enzymes like superoxide dismutase (SOD), glutathione peroxidase (GPx), catalase (CAT), along with non-enzymatic antioxidants such as glutathione (GSH) and vitamin E, normally neutralize ROS.(Pinzani, 2015)
In pathological states such as alcoholic liver disease (ALD), non-alcoholic fatty liver disease (NAFLD), and drug-induced liver injury (DILI), ROS production overwhelms the antioxidant systems, resulting in lipid peroxidation, protein oxidation, and DNA damage. This oxidative injury impairs membrane integrity, enzyme activity, and gene expression. Cytotoxic lipid peroxidation products like malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE) serve as biomarkers of oxidative damage. Additionally, upregulation of CYP2E1, especially during ethanol metabolism, generates excessive ROS, activating signaling pathways like NF-κB and AP-1, which amplify pro-inflammatory cytokine expression and hepatocyte death.(Gitto et al., 2014; Liu et al., 2021; Pinzani, 2015)
Mitochondrial Dysfunction
Mitochondria are central to ATP generation, β-oxidation of fatty acids, and ROS regulation. In liver disease particularly NAFLD and non-alcoholic steatohepatitis (NASH)—the influx of free fatty acids (FFAs) overwhelms mitochondrial oxidative capacity, leading to accumulation of lipotoxic intermediates such as ceramides and acyl-CoA derivatives. This overload disrupts mitochondrial function, triggering membrane depolarization, impaired electron transport chain (ETC) activity, and ATP depletion.(Ahmed, 2015; Seitz et al., 2018)
A hallmark of mitochondrial injury is the opening of the mitochondrial permeability transition pore (mPTP), resulting in the release of cytochrome c, apoptosis-inducing factor (AIF), and endonuclease G into the cytoplasm, initiating apoptotic pathways. Damaged mitochondria also release mitochondrial DNA (mtDNA), which acts as a damage-associated molecular pattern (DAMP) that activates TLR9 and the NLRP3 inflammasome, linking mitochondrial dysfunction to immune activation, inflammation, and fibrosis. These events contribute to the transition from steatosis to steatohepatitis and eventually to fibrotic liver remodeling.(Ahmed, 2015; Mulhall et al., 2002)
Inflammation and Cytokine Cascade
Hepatic inflammation is a pivotal driver of liver pathology. It begins with the recognition of pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) by pattern recognition receptors (PRRs) expressed on hepatocytes, Kupffer cells, and non-parenchymal liver cells. Kupffer cells, the liver’s resident macrophages, are first responders that detect these signals via Toll-like receptors (TLRs), NOD-like receptors (NLRs), and RIG-I-like receptors (RLRs).(Hosseini et al., 2019)
Upon activation, Kupffer cells release a suite of pro-inflammatory cytokines, including TNF- α, IL-1β, IL-6, MCP-1 (CCL2), and TGF-β, which recruit neutrophils and monocytes to the site of injury. These immune cells contribute to hepatic injury via respiratory bursts, generating ROS and proteolytic enzymes. Chemokines such as CCL2 and CXCL10 further enhance leukocyte recruitment, sustaining the inflammatory cycle. This inflammatory milieu activates hepatic stellate cells (HSCs), the main effector cells in hepatic fibrosis. Activated HSCs transdifferentiate into myofibroblast-like cells, which produce collagen types I and III, fibronectin, and matrix metalloproteinases (MMPs), leading to extracellular matrix (ECM) remodeling and fibrotic progression.
A key inflammatory mediator is the NLRP3 inflammasome, implicated in diseases such as NASH, ALD, and autoimmune hepatitis. Activation of the NLRP3 inflammasome results in caspase-1 activation, which processes pro-IL-1β and pro-IL-18 into their mature forms, intensifying inflammation and hepatocellular injury.(Szabo and Csak, 2012)
Apoptosis and Necrosis
Hepatocyte death via regulated cell death pathways is a hallmark of liver injury. Apoptosis, the most studied form of programmed cell death, occurs via two main pathways:
The intrinsic (mitochondrial) pathway, triggered by internal stressors such as oxidative damage, DNA injury, or ER stress, leads to Bax/Bak-mediated mitochondrial outer membrane permeabilization (MOMP). This results in the release of cytochrome c, which forms the apoptosome with Apaf-1 and caspase-9, eventually activating caspase-3 to execute cell death.(Chen et al., 2024; Sumadewi, 2023)
The extrinsic pathway, initiated by the binding of death ligands (e.g., FasL or TNF-α) to their receptors (Fas/CD95 or TNF-R1), activates caspase-8 through the recruitment of adaptor proteins like FADD, particularly relevant in viral hepatitis and immune- mediated liver damage.(Chilaka and Konje, 2021)
In contrast, necrosis is an unregulated form of cell death, driven by ATP depletion, calcium overload, and membrane rupture, leading to the uncontrolled release of intracellular contents. These DAMPs further amplify immune responses and inflammation. Massive hepatocyte necrosis is characteristic of acute liver failure, as seen in paracetamol toxicity or fulminant viral hepatitis. Together, these mechanisms highlight the interconnected and dynamic nature of liver injury. From oxidative and mitochondrial damage to inflammatory signaling and cell death, each component contributes to the progression of liver disease. Understanding these pathways is crucial for developing targeted hepatoprotective therapies, particularly in the context of medicinal plant-based interventions, and for interrupting the cascade leading to irreversible liver damage.(Chen et al., 2024; Sumadewi, 2023)

Figure 3: Pathophysiology of liver injury Common Types of Liver Disorders
Alcoholic Liver Disease (ALD)
Alcoholic liver disease (ALD) is a major cause of liver-related morbidity and mortality worldwide, resulting from chronic and excessive alcohol consumption. ALD progresses along a well-recognized clinical continuum—beginning with simple steatosis, advancing to alcoholic steatohepatitis (ASH), and further evolving into fibrosis, cirrhosis, and ultimately alcohol- related hepatocellular carcinoma (HCC). In India, where alcohol use was traditionally limited by cultural and religious factors, recent shifts in societal norms and increased alcohol consumption particularly among males aged 25–55 years have significantly contributed to the growing prevalence of ALD. (Bataller et al., 2019; Ishak et al., 1991; Liu et al., 2021; Stewart and Day, 2012)
The pathogenesis of ALD is multifactorial and complex. It involves several interrelated mechanisms:
These insults collectively activate Kupffer cells (resident hepatic macrophages), initiating a cascade of inflammatory and fibrogenic responses that exacerbate hepatocellular injury and drive the progression to fibrosis and cirrhosis. Nutritional deficiencies, especially of folate, zinc, and vitamins A and E, frequently seen in low-income populations, further aggravate disease severity and hinder liver regeneration.
Clinically, ALD can present across a broad spectrum:
Importantly, early-stage ALD is reversible with complete abstinence from alcohol and appropriate nutritional support. However, progression to advanced stages, including cirrhosis and HCC, necessitates long-term management strategies, which may involve pharmacological interventions, management of complications, and in selected cases, liver transplantation. Early diagnosis and lifestyle modification remain the cornerstone of ALD prevention and therapy.(Bruha et al., 2012; Ehrmann et al., 2019; O’Shea et al., 2010; Osna et al., 2017)
Non-Alcoholic Fatty Liver Disease (NAFLD)
Non-Alcoholic Fatty Liver Disease (NAFLD) has become the most common cause of chronic liver disease worldwide, currently affecting approximately 25–30% of adults. NAFLD encompasses a spectrum of hepatic disorders, beginning with non-alcoholic fatty liver (NAFL) characterized by simple steatosis without significant inflammation—and progressing to non- alcoholic steatohepatitis (NASH), which involves inflammation, hepatocyte injury, and ballooning degeneration. If untreated, NASH can lead to fibrosis, cirrhosis, and ultimately hepatocellular carcinoma (HCC).(Benedict and Zhang, 2017; Kim and Choi, 2023; Powell et al., 2021)
NAFLD is primarily a metabolic liver disorder and is strongly associated with insulin resistance, central (visceral) obesity, type 2 diabetes mellitus (T2DM), hypertension, and dyslipidemia—collectively known as metabolic syndrome. In India, the escalating prevalence of diabetes and obesity has significantly contributed to the increasing burden of NAFLD. Additionally, the rise in childhood obesity has led to a concerning increase in pediatric NAFLD, posing a serious public health threat.
The pathophysiology of NAFLD is multifactorial and includes:
At present, there is no FDA-approved pharmacological treatment for NASH. Therefore, lifestyle modification remains the cornerstone of management. This includes:
Natural hepatoprotective agents with antioxidant and anti-inflammatory activities. Given NAFLD's asymptomatic course, its potential for progression to end-stage liver disease, and its widespread prevalence, early detection, enhanced public health awareness, and multifaceted treatment strategies are urgently needed to mitigate its clinical and economic impact.(Ahmed, 2015; Alba and Lindor, 2003; Mulhall et al., 2002; Sattar et al., 2014)
Drug-Induced Liver Injury (DILI)
Drug-Induced Liver Injury (DILI) is a leading cause of acute liver failure and presents a considerable challenge in both clinical settings and pharmaceutical development. It is broadly classified into two major types: intrinsic DILI, which is dose-dependent, predictable, and typically associated with direct hepatotoxicity—as exemplified by acetaminophen (paracetamol) overdose; and idiosyncratic DILI, which is dose-independent, unpredictable, and thought to be influenced by genetic predispositions or immunologic hypersensitivity. In the Indian context, DILI is most commonly associated with anti-tubercular therapy (ATT), particularly involving drugs such as isoniazid, rifampicin, and pyrazinamide. Other frequently implicated agents include non-steroidal anti-inflammatory drugs (NSAIDs), antibiotics, chemotherapeutic agents, and herbal or traditional remedies, many of which are used without appropriate medical oversight, thereby increasing the risk of hepatotoxicity. The underlying mechanisms of DILI are diverse and complex. They include direct mitochondrial injury, which impairs ATP synthesis and leads to hepatocellular necrosis; immune-mediated hepatotoxicity, involving T-cell activation and inflammatory cytokine release; oxidative stress, resulting from the excessive production of reactive oxygen species (ROS) and lipid peroxidation; and the inhibition of bile salt export pumps (BSEP), which contributes to cholestasis and bile acid accumulation within hepatocytes.(Gougol et al., 2021; Ishak et al., 1991)
Clinically, DILI can mimic several other hepatic disorders, such as viral hepatitis, autoimmune hepatitis, and cholestatic liver disease, making diagnosis challenging. Key features include jaundice, elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels, eosinophilia, and a recent history of drug exposure. A poor prognosis is predicted by Hy’s Law, which states that the co-occurrence of jaundice and elevated transaminases, in the absence of significant alkaline phosphatase elevation, is a marker of increased risk for severe liver injury and mortality. Management of DILI is primarily supportive and begins with the immediate withdrawal of the suspected drug. This is followed by regular monitoring of liver function parameters and supportive care, including fluid and electrolyte management. In select cases, particularly those involving immune-mediated mechanisms, corticosteroids may be used, though their benefit must be carefully weighed against potential risks.
Because DILI is often a diagnosis of exclusion, clinicians must maintain a high index of suspicion and recognize early warning signs to prevent irreversible liver damage. In parallel, research interest is growing in the use of hepatoprotective agents, particularly antioxidant-rich phytochemicals such as flavonoids, polyphenols, and silymarin. These compounds have demonstrated promising results in experimental and translational models, highlighting their potential as adjunctive therapies for preventing or mitigating hepatic injury in DILI.(Gougol et al., 2021; Szabo and Csak, 2012)
Viral Hepatitis (A–E)
Viral hepatitis, caused by hepatotropic viruses A through E, continues to be a significant global public health challenge, particularly affecting regions in Asia and Africa. These infections vary in transmission routes, clinical outcomes, and long-term complications, but collectively contribute to substantial liver-related morbidity and mortality.(Berry, 1989; Walsh and Alexander, 2001)
Hepatitis A virus (HAV) and Hepatitis E virus (HEV) are both transmitted via the fecal-oral route, most often through ingestion of contaminated food or water. While they typically cause acute, self-limiting hepatitis, HEV infection can result in fulminant hepatic failure, especially in pregnant women during the third trimester, making it a notable public health risk in endemic regions.(Berry, 1989; Pisano et al., 2021; Torre et al., 2021; Walsh and Alexander, 2001)
Hepatitis B virus (HBV) is a DNA virus that causes both acute and chronic hepatitis. Among individuals with chronic HBV infection, approximately 15–40% progress to cirrhosis or hepatocellular carcinoma (HCC). India has intermediate HBV endemicity, with a prevalence of 3–4%, accounting for over 40 million chronic carriers. However, universal immunization, newborn vaccination, and routine blood donor screening have substantially reduced transmission rates in recent decades.(Berry, 1989; Gitto et al., 2014; He et al., 2010; Marcus and Tur-Kaspa, 1997)
Hepatitis C virus (HCV) is an RNA virus transmitted primarily via parenteral routes, including unsafe injections, blood transfusions, and needle sharing. Chronic HCV infection frequently leads to progressive liver fibrosis, cirrhosis, and HCC, making it a leading indication for liver transplantation globally. The introduction of direct-acting antivirals (DAAs) has dramatically improved treatment outcomes, offering cure rates exceeding 95%. However, limited access and high treatment costs remain barriers to care in many low- and middle-income countries.(Gitto et al., 2014; Pisano et al., 2021; Szabó et al., 2003; Torre et al., 2021)
Hepatitis D virus (HDV) is a defective RNA virus that requires co-infection with HBV for replication. Co-infection or superinfection with HDV leads to more aggressive liver disease, rapidly accelerating the progression to cirrhosis and HCC compared to HBV monoinfection.(Pisano et al., 2021; Szabó et al., 2003; Torre et al., 2021; Walsh and Alexander, 2001)
Comprehensive control of viral hepatitis relies on early diagnosis, effective antiviral treatment, mass vaccination programs (particularly against HAV and HBV), and public health education to reduce risk exposures. Preventive measures such as improved sanitation, safe injection practices, and blood safety protocols are fundamental. As such, viral hepatitis remains not only a medical but also a social and infrastructural challenge that requires integrated, long-term public health strategies.(Marcus and Tur-Kaspa, 1997)
Autoimmune Liver Diseases
Autoimmune liver diseases are chronic inflammatory conditions that arise due to a loss of immune tolerance, resulting in an inappropriate immune response directed against hepatocytes or biliary epithelial cells. These diseases are characterized by immune-mediated hepatic injury and can lead to progressive liver damage if not adequately managed. The three principal forms include Autoimmune Hepatitis (AIH), Primary Biliary Cholangitis (PBC), and Primary Sclerosing Cholangitis (PSC). (Invernizzi and Mackay, 2008)
Autoimmune Hepatitis (AIH) is marked by elevated serum immunoglobulin G (IgG) levels, and the presence of antinuclear antibodies (ANA) or smooth muscle antibodies (SMA).
Histologically, AIH is defined by interface hepatitis, with lymphoplasmacytic infiltration at the junction of the portal tract and hepatic parenchyma. The condition typically responds well to corticosteroids, often in combination with azathioprine, which helps maintain remission and reduce steroid dependence.
Primary Biliary Cholangitis (PBC) is a chronic cholestatic liver disease characterized by immune-mediated destruction of the small intrahepatic bile ducts. It is associated with anti- mitochondrial antibodies (AMA) and elevated alkaline phosphatase levels. Clinically, it presents with fatigue and pruritus and can progress to cirrhosis if untreated. Ursodeoxycholic acid (UDCA) remains the first-line therapy, significantly improving biochemical markers and delaying disease progression.
Primary Sclerosing Cholangitis (PSC) affects both intra- and extrahepatic bile ducts and is strongly associated with inflammatory bowel disease (IBD), particularly ulcerative colitis. PSC is considered a premalignant condition, with an increased risk of developing cholangiocarcinoma. Unlike PBC, PSC has limited therapeutic options, and liver transplantation may become necessary in advanced stages.
These autoimmune liver disorders are more commonly observed in females and typically present with non-specific symptoms such as fatigue, pruritus, and jaundice. Diagnosis relies on a combination of serologic testing, biochemical markers, and liver biopsy, which is crucial for confirming the diagnosis and assessing the extent of liver injury and fibrosis.Long-term management includes immunosuppressive therapy, symptom control, and routine monitoring to evaluate disease activity and detect complications early. Without appropriate intervention, these conditions may progress to cirrhosis, liver failure, or hepatobiliary malignancies, reinforcing the importance of early recognition and sustained therapeutic strategies.(Invernizzi and Mackay, 2008; Washington, 2007)
Genetic and Congenital Liver Disorders
Inherited liver diseases, though relatively uncommon, represent significant causes of hepatic dysfunction, often presenting in childhood or early adulthood. Among the most clinically relevant are Wilson’s Disease (WD) and Alpha-1 Antitrypsin Deficiency (A1ATD), both of which require early recognition to prevent irreversible liver damage.
Wilson’s Disease (WD) is an autosomal recessive disorder caused by mutations in the ATP7B gene, which encodes a copper-transporting ATPase. The defective protein impairs hepatic copper excretion into bile, leading to progressive copper accumulation in the liver, and subsequently in the brain and cornea. Clinically, WD may present with hepatic manifestations such as hepatitis, cirrhosis, or acute liver failure, or with neurological and psychiatric symptoms, including tremors, dysarthria, personality changes, or cognitive decline. Diagnosis is based on a combination of findings: low serum ceruloplasmin, increased 24-hour urinary copper excretion, and quantitative hepatic copper content measured via liver biopsy. Kayser– Fleischer rings, visible on slit-lamp eye examination, are a classical diagnostic clue. Treatment involves long-term copper chelation using penicillamine or trientine, along with zinc therapy, which blocks intestinal copper absorption.(Brewer, 2005; Gitlin, 2003; Poujois and Woimant, 2018)
Alpha-1 Antitrypsin Deficiency (A1ATD) is a genetic disorder resulting from mutations in the SERPINA1 gene, leading to the accumulation of misfolded alpha-1 antitrypsin protein within hepatocytes. This accumulation can cause neonatal cholestasis, chronic hepatitis, or adult-onset cirrhosis. A1ATD is also strongly associated with early-onset pulmonary emphysema, even in the absence of significant liver disease. Diagnosis is confirmed by measuring serum A1AT levels and genotyping to identify common variants such as the Z and S alleles. (Disease and Crystal, 1990; Patel et al., 2021; Perlmutter, 2000)
Although both conditions remain underdiagnosed in India, the availability of genetic testing and clinical awareness has significantly improved early detection. Early diagnosis is crucial for timely intervention and can prevent progression to end-stage liver disease. In advanced cases, particularly those with cirrhosis or liver failure, liver transplantation is considered the definitive treatment and offers excellent long-term outcomes.
Liver Cirrhosis and Hepatocellular Carcinoma (HCC)
Cirrhosis represents the final stage of chronic liver injury and is characterized by widespread hepatic fibrosis, formation of regenerative nodules, and significant vascular remodeling. It results from prolonged hepatocellular damage caused by various underlying conditions, most notably alcoholic liver disease (ALD), non-alcoholic fatty liver disease (NAFLD), chronic viral hepatitis (HBV and HCV), and autoimmune liver diseases. These chronic insults disrupt normal liver architecture and compromise its physiological functions, leading to irreversible liver damage. The clinical manifestations of cirrhosis vary depending on the stage and severity but commonly include complications such as ascites, resulting from portal hypertension and hypoalbuminemia; hepatic encephalopathy, due to the accumulation of neurotoxins like ammonia; variceal bleeding, stemming from esophageal or gastric varices; and coagulopathy, owing to impaired synthesis of clotting factors. These complications signify hepatic decompensation and are associated with increased morbidity and mortality.(Chen et al., 2024; Gandon et al., 2004)
Cirrhosis is the most significant risk factor for hepatocellular carcinoma (HCC), the most common primary liver malignancy. HCC ranks as the fourth leading cause of cancer-related deaths globally, with chronic HBV and HCV infections being responsible for the majority of cases. Given its poor prognosis, early detection of HCC is critical. Surveillance in high-risk patients, particularly those with cirrhosis, typically includes regular serum alpha-fetoprotein (AFP) testing and imaging techniques such as ultrasound, CT, or MRI.(Chen et al., 2024; Gandon et al., 2004; He et al., 2010; Kobelska-Dubiel et al., 2014)
The management of cirrhosis requires a multidisciplinary approach tailored to the underlying etiology and the presence of complications. Key components include:
In cases of advanced decompensated cirrhosis, liver transplantation remains the definitive treatment, significantly improving survival and quality of life.
Meanwhile, research continues into hepatoprotective strategies aimed at preventing the progression from fibrosis to cirrhosis. Investigational therapies include natural compounds, antioxidants, and antifibrotic agents with the potential to preserve hepatic function and structure. These efforts are vital, as they offer hope for early-stage intervention and disease modification in patients with chronic liver disease.
Recent evidence has revealed other regulated cell death pathways in liver pathology:
In addition to apoptosis and necrosis, several emerging forms of regulated cell death have been identified as critical contributors to liver pathology, each with distinct molecular mediators and implications for disease progression and therapy.
Necroptosis is a form of programmed necrosis that occurs when apoptotic pathways are inhibited. It is mediated by key signaling molecules including receptor-interacting protein kinases 1 and 3 (RIPK1 and RIPK3) and the mixed lineage kinase domain-like protein (MLKL). Upon activation, MLKL translocates to the plasma membrane, causing its rupture and the release of pro-inflammatory intracellular contents. Necroptosis has been implicated in conditions such as drug-induced liver injury (DILI) and non-alcoholic fatty liver disease (NAFLD), where it contributes to hepatocellular damage and inflammation.(Singal et al., 2024)
Pyroptosis is a highly inflammatory form of cell death mediated by caspase-1 activation and the pore-forming protein gasdermin D (GSDMD). This process is closely linked to NLRP3 inflammasome activation, which occurs in response to cellular stress and damage signals. Pyroptosis plays a critical role in innate immune responses and has been associated with the pathogenesis of NASH, alcoholic hepatitis, and autoimmune hepatitis.(Singal et al., 2024; Szabo and Csak, 2012)
Ferroptosis is a distinct iron-dependent cell death pathway characterized by accumulation of lipid peroxides, driven by impaired glutathione peroxidase 4 (GPX4) activity. Unlike apoptosis or necrosis, ferroptosis is triggered by iron overload and oxidative lipid damage, and is increasingly recognized in the context of hepatocarcinogenesis, ischemia-reperfusion injury, and liver fibrosis. These novel mechanisms of cell death not only deepen our understanding of liver disease pathophysiology but also unveil promising therapeutic targets. Modulating necroptosis, pyroptosis, or ferroptosis may offer new strategies for hepatoprotection and disease modification, especially in settings where conventional therapies are limited.(Singal et al., 2024)
Biomarkers of Liver Damage
Biochemical markers play a vital role in the diagnosis and management of liver diseases. They serve as key indicators for detecting hepatocellular injury, determining the underlying etiology, tracking disease progression, and evaluating the therapeutic response. These markers broadly reflect three major aspects of liver function: hepatocyte integrity, biliary function, and synthetic capacity. Assessing this biochemical profile enables clinicians to identify the extent and nature of hepatic damage, differentiate between various liver disorders, and guide clinical decision- making for both acute and chronic liver conditions. (Liu et al., 2021)
Alanine Aminotransferase (ALT)
Alanine aminotransferase (ALT) is a cytoplasmic enzyme primarily localized within hepatocytes and is regarded as the most liver-specific aminotransferase. It serves as a highly sensitive biomarker for detecting hepatocellular injury. Elevated ALT levels are commonly observed in conditions such as acute viral hepatitis, drug-induced liver injury (DILI), non- alcoholic fatty liver disease (NAFLD), and autoimmune hepatitis. Importantly, ALT levels often rise before the onset of clinical symptoms, positioning it as a reliable early indicator of liver damage and an essential component of liver function testing. (Chilaka and Konje, 2021; Disease, 1996; Kobelska-Dubiel et al., 2014; Torre et al., 2021)
Aspartate Aminotransferase (AST)
Aspartate aminotransferase (AST) is an enzyme found in both the cytosol and mitochondria of various tissues, including the liver, skeletal muscle, cardiac muscle, and kidneys. Although it is less specific to the liver than ALT, AST remains a valuable marker of hepatic injury, particularly in specific clinical contexts. In alcoholic liver disease (ALD), an AST/ALT ratio greater than 2 is considered diagnostically significant, suggesting mitochondrial damage, which is a hallmark of alcohol-induced hepatotoxicity. Additionally, elevated AST levels are often observed in advanced fibrosis and cirrhosis, reflecting progressive liver injury and structural remodeling.(Chilaka and Konje, 2021; Disease, 1996; Kobelska-Dubiel et al., 2014; Torre et al., 2021)
Alkaline Phosphatase (ALP)
Alkaline phosphatase (ALP) is a membrane-bound enzyme predominantly expressed in the epithelial cells of the bile ducts. It serves as a key marker of cholestasis and is typically elevated in cholestatic liver disorders such as primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), and biliary obstruction due to stones or tumors. However, because ALP is also present in other tissues like bone and placenta, its elevation is not liver-specific. Therefore, concurrent measurement of gamma-glutamyl transferase (GGT) is essential to confirm the hepatic origin of elevated ALP levels, improving diagnostic specificity for liver-related pathology.(Frey and Zhu, 1989; Kobelska-Dubiel et al., 2014; Patel et al., 2021; Torre et al., 2021)
Gamma-Glutamyl Transferase (GGT)
Gamma-glutamyl transferase (GGT) is a highly sensitive marker for biliary epithelial injury and is frequently elevated in parallel with alkaline phosphatase (ALP) in cholestatic liver conditions. Its measurement is particularly useful in confirming the hepatic origin of raised ALP levels. Beyond cholestasis, GGT is commonly elevated in cases of chronic alcohol consumption, making it a supportive marker in the diagnosis of alcoholic liver disease. Additionally, GGT is used to monitor hepatic enzyme induction by certain drugs, such as anticonvulsants and barbiturates, due to its responsiveness to microsomal enzyme induction.(Evans and Siew, 2020; Kobelska-Dubiel et al., 2014)
Total and Direct Bilirubin (TB and DB)
Bilirubin is a metabolic byproduct formed during the catabolism of heme, primarily from the breakdown of hemoglobin in senescent red blood cells. It exists in two major forms: unconjugated (indirect) and conjugated (direct). Unconjugated bilirubin levels are elevated in conditions such as hemolysis and Gilbert syndrome, where hepatic uptake or conjugation is impaired. In contrast, conjugated bilirubin rises when there is hepatocellular dysfunction or cholestasis, due to impaired excretion into the bile canaliculi. Clinically significant elevations in direct bilirubin are commonly observed in viral hepatitis, alcoholic liver disease (ALD), non- alcoholic steatohepatitis (NASH), and obstructive jaundice, reflecting disrupted bile flow or hepatocellular excretory failure.(Kobelska-Dubiel et al., 2014)
Serum Albumin
Albumin, synthesized exclusively by hepatocytes, serves as a key indicator of the liver’s synthetic function. It plays a critical role in maintaining plasma oncotic pressure and acts as a carrier protein for various endogenous and exogenous substances. Low serum albumin levels are indicative of chronic liver dysfunction, and may also reflect malnutrition or protein-losing conditions such as nephrotic syndrome or enteropathy. In clinical practice, serum albumin is an important parameter included in the Child-Pugh score, aiding in the assessment of liver disease severity and prognosis in patients with cirrhosis.(Disease, 1996; Frey and Zhu, 1989; Martens and Nevens, 2015)
Prothrombin Time (PT) and International Normalized Ratio (INR)
Prothrombin time (PT) and its standardized form, the international normalized ratio (INR), assess the liver’s ability to synthesize coagulation factors, particularly factors II, V, VII, IX, and X, which are all produced by hepatocytes. A prolonged PT/INR is a hallmark of hepatic synthetic failure and serves as a poor prognostic indicator, especially in conditions such as acute liver failure and advanced cirrhosis. PT/INR is also a critical component of the Model for End-Stage Liver Disease (MELD) score, which is widely used to evaluate disease severity and prioritize patients for liver transplantation.(Chen et al., 2024; Chilaka and Konje, 2021; Hosseini et al., 2019)
Lactate Dehydrogenase (LDH)
Lactate dehydrogenase (LDH) is a non-specific marker of cellular injury and necrosis, widely distributed across various tissues. In the context of liver disease, elevated LDH levels are particularly associated with ischemic hepatitis and massive hepatic necrosis, where widespread hepatocyte death leads to significant enzyme release into the bloodstream. Although LDH lacks organ specificity, its marked elevation especially in combination with other liver enzymes can provide supportive evidence of acute hepatocellular damage in severe hepatic insults. (Acharya, 1987; Disease, 1996)
Emerging Biomarkers
Recent advances in molecular diagnostics have led to the identification of novel biomarkers that enhance the early detection, staging, and monitoring of liver diseases, particularly non- alcoholic steatohepatitis (NASH) and fibrosis progression. Among these, keratin-18 fragments serve as markers of hepatocyte apoptosis, providing insight into ongoing cell death in NASH. Circulating microRNAs, such as miR-122 and miR-34a, are liver-specific and have shown promise as sensitive indicators of hepatocellular injury. Markers of fibrogenesis, including hyaluronic acid, tissue inhibitor of metalloproteinase-1 (TIMP-1), and procollagen type III N- terminal peptide (PIIINP), reflect extracellular matrix remodeling and are being studied for their utility in fibrosis staging. Non-invasive scoring systems like the FIB-4 index and the AST to Platelet Ratio Index (APRI) integrate routine clinical parameters to estimate fibrosis severity, offering alternatives to liver biopsy. These biomarkers are currently under clinical evaluation for their effectiveness in early NASH diagnosis, tracking fibrosis progression, and monitoring therapeutic response in clinical trials, with the goal of improving patient stratification and outcome prediction in chronic liver disease.(Liu et al., 2021)
Current Treatment Modalities for Liver Disorders
Over the past two decades, the management of liver diseases has advanced substantially, owing to progress in virology, immunology, pharmacotherapeutics, and transplant medicine. Despite these developments, current treatment strategies remain largely etiology-specific and often have limited capacity to reverse advanced liver injury or restore full hepatic function. Therapeutic regimens typically involve a combination of pharmacological agents that address viral replication, immune dysregulation, inflammatory pathways, cholestasis, and disease- related complications.
Antiviral Therapies
Antivirals are the cornerstone of treatment for chronic hepatitis B (HBV) and hepatitis C (HCV). HBV management relies on potent nucleos(t)ide analogues such as entecavir, tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF). These drugs inhibit HBV DNA polymerase, effectively suppress viral replication, reduce hepatic inflammation, and lower the risk of cirrhosis and hepatocellular carcinoma (HCC). However, due to the persistence of covalently closed circular DNA (cccDNA), complete viral eradication is rare, necessitating lifelong therapy for most patients. Resistance remains a concern with older agents such as lamivudine. For HCV, direct-acting antivirals (DAAs) have transformed the therapeutic landscape. Agents like sofosbuvir, ledipasvir, velpatasvir, and glecaprevir/ pibrentasvir target HCV proteins (NS3/4A protease, NS5A, NS5B polymerase), offering short-duration oral regimens (8–12 weeks) with cure rates exceeding 95% across genotypes. DAAs are generally well tolerated and effective in patients co-infected with HIV. Nevertheless, high treatment costs remain a barrier in low- and middle-income countries, including India, although generic options have improved accessibility.(Berry, 1989; Gitto et al., 2014; Torre et al., 2021)
Corticosteroids and Immunosuppressants
In autoimmune hepatitis (AIH) and severe alcoholic hepatitis (AH), corticosteroids remain first-line therapy. Prednisolone or methylprednisolone is used to induce remission in AIH, often combined with azathioprine for maintenance and steroid tapering. In cases of azathioprine intolerance or hepatotoxicity, alternatives include mycophenolate mofetil, tacrolimus, or cyclosporine. Regular monitoring of liver enzymes, serum IgG, and autoantibody titers is essential for guiding therapy and detecting relapse. In severe AH, corticosteroids are reserved for patients with a Maddrey Discriminant Function ≥32 or MELD score >20, provided contraindications such as active infection or gastrointestinal bleeding are absent. While pentoxifylline has been used as a TNF-α inhibitor, it is no longer favored due to limited efficacy. Emerging therapies such as interleukin-22 analogs, granulocyte colony-stimulating factor (G-CSF), and fecal microbiota transplantation (FMT) are under investigation for steroid non-responders.(Singal et al., 2024)
Immunomodulation in Cholestatic Diseases
For primary biliary cholangitis (PBC), ursodeoxycholic acid (UDCA) remains the standard of care, improving biochemical parameters, delaying disease progression, and enhancing transplant-free survival. In UDCA non-responders, obeticholic acid (OCA), a farnesoid X receptor (FXR) agonist, is approved as a second-line therapy. In primary sclerosing cholangitis (PSC), effective pharmacologic options are limited. While low-dose UDCA may be used, high- dose regimens have shown adverse effects. Management focuses on symptom control, endoscopic therapy of biliary strictures, and cancer surveillance, particularly for cholangiocarcinoma.(Lai et al., 2003; Odenwald and Paul, 2022)
Antioxidants and Emerging Agents
N-acetylcysteine (NAC) is the treatment of choice for acetaminophen toxicity and is increasingly being evaluated for non-acetaminophen acute liver failure, especially when administered early. NAC acts by replenishing glutathione, neutralizing ROS, and improving hepatic microcirculation. For NAFLD and non-alcoholic steatohepatitis (NASH), investigational agents such as pioglitazone, vitamin E, GLP-1 receptor agonists (e.g., liraglutide), and SGLT2 inhibitors (e.g., empagliflozin) are showing promise. These agents target insulin resistance, oxidative stress, and hepatic lipid accumulation, though widespread regulatory approval is still pending.(Chen et al., 2024; Hoskins, 2005; “THE FIRST STEP : DEFINING DISEASE,” n.d.)
Supportive and Symptom-Directed Therapies
Supportive care remains fundamental, particularly in advanced cirrhosis. For hepatic encephalopathy, lactulose and rifaximin reduce ammonia production by altering gut flora. Ascites is managed with diuretics (spironolactone and furosemide), paracentesis, and albumin infusion to maintain circulatory stability. Non-selective beta-blockers (NSBBs) such as propranolol help reduce portal hypertension and prevent variceal bleeding. Other key interventions include antibiotic prophylaxis to prevent spontaneous bacterial peritonitis, nutritional support to address malnutrition and sarcopenia, and monitoring for complications such as HCC, renal dysfunction, and infections.
Together, these therapies form a comprehensive approach to managing liver disease. However, the persistent limitations in reversing fibrosis and restoring full hepatic function highlight the ongoing need for new therapeutic targets, particularly in antifibrotic, anti-inflammatory, and regenerative pathways.
Limitations and Side Effects
While conventional therapies have undoubtedly improved the clinical management and prognosis of various liver diseases, they remain predominantly palliative, often aimed at symptom control or pathway-specific interventions rather than achieving complete reversal of hepatic injury or fibrosis. Many current treatments are associated with significant adverse effects, variable efficacy across patient subgroups, and limitations in targeting the underlying pathophysiology of chronic liver conditions. One of the most significant challenges in hepatology is the irreversibility of advanced fibrosis and cirrhosis. Even after successful viral suppression, the structural and functional restoration of the liver remains inconsistent. For example, direct-acting antivirals (DAAs) effectively eradicate HCV, but do not fully reverse established cirrhosis, and the risk of hepatocellular carcinoma (HCC) remains elevated for years post-treatment. In chronic hepatitis B, nucleos(t)ide analogues suppress viral replication but fail to eliminate covalently closed circular DNA (cccDNA), resulting in relapse upon therapy discontinuation. Although newer antivirals have reduced resistance rates, the issue persists, particularly in resource-limited settings with suboptimal adherence.
Corticosteroids, which are first-line agents in autoimmune hepatitis (AIH) and alcoholic hepatitis (AH), are associated with substantial systemic toxicity. Long-term use may lead to osteoporosis, hyperglycemia, adrenal suppression, Cushingoid features, muscle wasting, and an increased risk of opportunistic infections. Moreover, treatment relapse rates in AIH remain high (20–30%) following taper or discontinuation, necessitating lifelong immunosuppression in many cases. In the setting of decompensated cirrhosis particularly with sepsis, gastrointestinal bleeding, or renal dysfunction steroids may be contraindicated, limiting their utility in severe ALD.
Immunosuppressive agents, including azathioprine, mycophenolate mofetil (MMF), and calcineurin inhibitors, pose additional risks such as bone marrow suppression, hepatotoxicity, nephrotoxicity, and lymphoproliferative disorders. Their narrow therapeutic index necessitates frequent laboratory monitoring, which may not be feasible for patients in rural or economically underserved regions, imposing both logistical and financial burdens.
In cholestatic liver diseases, ursodeoxycholic acid (UDCA) remains the standard therapy for primary biliary cholangitis (PBC); it improves biochemical markers and delays disease progression but does not significantly improve survival in advanced-stage PBC. For UDCA non-responders, obeticholic acid (OCA) has shown efficacy, yet its cost and contraindication in advanced cirrhosis limit broader application due to risk of hepatic decompensation.
Supportive treatments also present challenges. Lactulose, used for hepatic encephalopathy, frequently causes bloating, flatulence, and non-adherence. Rifaximin, though effective, is expensive for long-term prophylaxis. Non-selective beta-blockers (NSBBs) require careful titration to avoid hypotension and renal dysfunction, while diuretics can precipitate electrolyte imbalances, hyponatremia, and hepatorenal syndrome in cirrhotic patients. Moreover, conventional therapies do not effectively target fundamental drivers of liver injury, such as oxidative stress, lipotoxicity, mitochondrial dysfunction, and gut dysbiosis. These factors are central to the pathogenesis and progression of non-alcoholic steatohepatitis (NASH), drug- induced liver injury (DILI), autoimmune hepatitis, and alcohol-related liver disease, highlighting the need for multi-targeted therapeutic approaches that address the complex interplay of metabolic, immune, and environmental factors.
Beyond clinical limitations, socioeconomic and infrastructural barriers further hinder the effectiveness of standard treatments in regions like rural India, where access to specialist care, diagnostic tools, and advanced therapies is limited. High drug costs, long treatment durations, and adverse effect profiles contribute to non-compliance and poor outcomes, especially among economically disadvantaged populations. These gaps underscore the urgent need for novel hepatoprotective strategies. In this context, natural products and medicinal plants are emerging as promising alternatives. Many exhibits antioxidant, anti-inflammatory, anti-fibrotic, and immunomodulatory properties, with a lower incidence of side effects and greater patient acceptability. Preclinical and early clinical evidence suggests that these agents may offer multi- mechanistic benefits, address the root causes of liver injury and potentially improve both disease progression and quality of life for patients with chronic liver disorders.
Role of Liver Transplantation
Liver transplantation (LT) represents the definitive treatment for patients with end-stage liver disease (ESLD), acute liver failure, or early-stage hepatocellular carcinoma (HCC) that is not amenable to surgical resection. LT offers complete restoration of hepatic function, significantly improves survival, and enhances quality of life. Globally, 1-year survival rates post-transplant are approximately 85%, and 5-year survival rates exceed 70%, positioning LT among the most successful solid organ transplant procedures.(Carbone and Neuberger, 2014)
Indications for Liver Transplantation
Liver transplantation is indicated in a range of clinical scenarios, including:
Candidate Selection and Prioritization
The Model for End-Stage Liver Disease (MELD) score is the primary tool used to prioritize transplant recipients based on disease severity. It incorporates bilirubin, INR, creatinine, and sodium levels to predict short-term mortality, with higher scores indicating more urgent need. The Child–Pugh score also provides prognostic information, helping to stratify patients for transplant consideration.
Post-Transplant Management and Outcomes
Following transplantation, patients require lifelong immunosuppression to prevent graft rejection. Common regimens include:
While graft and patient survival rates are high, LT is associated with long-term risks, including:
Liver Transplantation in India: Current Landscape and Challenges
In India, liver transplantation has seen substantial growth, particularly in tertiary care centers in cities like Delhi, Chennai, and Hyderabad. However, access to LT remains limited due to:
As a result, living donor liver transplantation (LDLT) accounts for the majority of transplants, though this too depends on donor availability and recipient fitness. Efforts by organizations such as the National Organ and Tissue Transplant Organization (NOTTO) have improved awareness and regulatory coordination, but donor rates in India remain below global averages, limiting the reach of transplant programs.
The Need for Preventive and Adjunctive Interventions
Given the economic and logistical constraints, liver transplantation remains inaccessible to a large segment of the Indian population. This underscores the critical need for preventive strategies and early-stage interventions that could delay or obviate the need for transplantation. In this context, plant-based hepatoprotective therapies have garnered increasing attention. Medicinal plants such as:
have demonstrated antioxidant, anti-inflammatory, anti-apoptotic, and anti-fibrotic properties in preclinical models of liver injury. These multifaceted mechanisms make them promising candidates for adjunctive therapy in chronic liver diseases, especially in settings with limited access to transplantation. The integration of such evidence-based phytotherapies into public health frameworks could significantly improve liver disease outcomes in resource-constrained settings while supporting cost-effective and culturally acceptable care models.(Ali et al., 2015; Hassan et al., 2019; Mohamed Saleem et al., 2010; Shirani et al., 2017)
Many of these plants contain a variety of chemical components, including phenols, coumarins, lignans, essential oils, monoterpenes, carotenoids, glycosides, flavonoids, organic acids, lipids, alkaloids, and xanthines, which are associated with their liver-protective properties. The development of entirely plant-based hepatoprotective medications has gained importance globally. Medicinal plants are considered significant sources of hepatoprotective drugs, with about 170 phytoconstituents isolated from 110 plants belonging to 55 families reportedly having this activity. Over 87 plants are used in patented and proprietary multi-ingredient plant formulations in India. Scientific evaluation has often shown that active principles within plants are responsible for their therapeutic success. Herbal drugs are generally considered relatively non-toxic, safe, and often free from serious side effects.
PLANT PROFILE
Biological source: It is leaves obatined from the plant, Casearia graveolens Dalz
Family: Salicaceae
Taxonomy

Figure 4: Casearia graveolens Dalz
Common Name:
Morphology and Occurrence
Casearia species are shrubs or trees. Leaves simple, alternate, distichous, usually pellucid punctate, lanceolate-ovate to elliptic-oblong, margin entire, serrate-dentate to pinnately veined, rarely 3-5 pliveined at the base, apex acute to acuminate, chartaceous, glandular pellucid on serrate-crenate teeth or margins, lateral veins very thin compared with midrib, petiole slender, long, sometimes with pair of glands at apex, stipules minute, caducous. Inflorescence clustered in shortly pedunculate axillary fascicles, few to many flowers, rarely solitary or cymes. Flowers bisexual, perigynous, pedicels short rarely sessile, bracts ovate, chartaceous, scalelike, sepals 4-5, imbricate, joined near base, free above, margin ciliate, persistent, petals absent. Stamens 8-10, in the same row of alternating with the well-developed staminodes, connate below, filaments filiform, inserted on disk cup, persistent, anthers 2 loculed, dorsifixed, pollen fleshy, tricolporate, suboblate. Ovary superior, unilocular, 3 carpellary, ovules few to many, placentae 2-4, parietal, style short, stigma capitate or obscurely trilobed. Fruit capsule, 2-3 valved, dehisced valves usually naviculate, lobes persistent at the base, ellipsoid-globose, 3 angled when young and 6 ribbed when dry. Seeds many, ovoid-obovoid, arillate, bright red or orange. Distribution :
Native :
Native to: Assam, Bangladesh, Cambodia, China South-Central, East Himalaya, India, Laos, Myanmar, Nepal, Pakistan, Thailand, Vietnam, West Himalaya
Global Distribution
Asia: Bangladesh, Bhutan, Cambodia, China, India, Laos, Myanmar, Nepal, Pakistan, Thailand, Vietnam.
Local Distribution : Andhra Pradesh, Assam, Bihar, Gujarat, Himachal Pradesh, Karnataka, Kerala, Madhya Pradesh, Maharashtra, Meghalaya, Odisha, Punjab, Sikkim, Tamil Nadu, Uttar Pradesh, West Bengal.
Chemical Constituants
Casearia graveolens is chemically rich in diverse and pharmacologically potent secondary metabolites, most notably clerodane-type diterpenoids, which are well recognized for their cytotoxic, anti-inflammatory, and neurotrophic properties. Key compounds include micromelin, casearlucin A, caseariagraveolin, caseaveolen A–H, and graveopenes A–J, isolated from various parts of the plant (twigs, bark, and leaves). These diterpenoids exhibit structural features like epoxylactones, esters, and fused tricyclic skeletons and have demonstrated strong antiangiogenic, anticancer, and neurite-promoting activity, with several showing IC?? values between 2–10 µM against various cancer cell lines. Additional phytochemicals include scopoletin, bergapten, β-sitosterol, (+)-taxifolin, quercetin, hydroquinone, pinoresinol, phytol, feruloyltyramine, cinnamic acid, and other phenylpropanoids, flavonoids, and lignans. Spectroscopic techniques such as NMR, HR-MS, ECD, FTIR, HPLC, and GC-MS have confirmed the presence of aromatic rings, hydroxyls, ketones, lactones, and prenylated structures, underpinning the chemical complexity of this species. Casearia diterpenes are not only chemotaxonomic markers but also crucial leads for VEGFR-2 inhibition, FAK/MMP suppression, and NGF-potentiated neuritogenesis, making C. graveolens a promising natural resource for anticancer and neuroprotective drug development.
Traditional / Ethno medicinal Uses
In traditional and ethnomedicinal systems across India, Southeast Asia, and China, Casearia graveolens has been widely used for its therapeutic benefits. It is traditionally employed to treat snake bites, tumors, fevers, skin diseases, ulcers, joint pain, rheumatism, diabetes, and diarrhea. The leaves and bark are used in poultices and decoctions, particularly in tribal and rural communities, for wound healing, anti-inflammatory applications, and relief from liver and stomach ailments. Some local traditions also use the bark as an abortifacient, while the root extracts are employed as a tonic and febrifuge. Reports also suggest its use in treating leprosy, venereal diseases, and digestive issues. These uses align well with modern findings, where C. graveolens extracts and isolated compounds have shown strong anticancer, anti-angiogenic, hepatoprotective, antidiabetic, neuroprotective, and anti-inflammatory activities, providing a scientific rationale for its long-standing medicinal application.
Pharmacological Study Reported
Li et al. conducted a comprehensive review titled “The Genus Casearia: A Phytochemical and Pharmacological Overview,” focusing on the phytochemical diversity and traditional uses of Casearia species, including Casearia graveolens. The objective was to document known secondary metabolites and correlate them with traditional and pharmacological activities. The authors reviewed a wide range of published studies until May 2013, compiling information on the genus from botanical, ethnomedical, chemical, and pharmacological perspectives. The phytochemical investigation revealed that the genus is rich in clerodane-type diterpenoids, with over 152 clerodane diterpenes described, particularly from C. sylvestris, C. membranacea, C. corymbosa, and C. grewiifolia. Additional constituents include ent-kaurane diterpenes, triterpenoids like β-amyrin, friedelin, and lupenone, as well as flavonoids, phenylpropanoids, and essential oils. Specifically, for Casearia graveolens, compounds such as lignans (e.g., lyoniresinol derivatives), phenylpropanoids, and β-sitosterol were noted, supporting its traditional medicinal applications. Traditionally, various Casearia species have been used for treating ailments like snake bites, ulcers, skin diseases, fevers, diabetes, and inflammatory conditions. For instance, C. sylvestris is used in Latin America as an appetite suppressant, topical anesthetic, and for treating herpes and leprosy, while C. esculenta is used in India to manage diabetes. C. tomentosa and C. ilicifolia are used as diuretics and antifertility agents, respectively. This review concluded that the genus Casearia is a prolific source of structurally diverse and pharmacologically potent secondary metabolites, especially clerodane diterpenoids. The findings validate many traditional uses and support the continued bioprospecting of Casearia species for cytotoxic, hypoglycemic, anti-ulcer, anti-inflammatory, and anti-venom therapeutic leads. (Xia et al., 2015)
Talapatra et al. conducted a study titled “Chemical Constituents of Casearia graveolens: Some Novel Reactions and the Preferred Molecular Conformation of the Major Coumarin, Micromelin,” focusing on the isolation, structural elucidation, and chemical transformation of secondary metabolites from the bark of Casearia graveolens (Family: Samydaceae). The primary objective was to identify novel coumarins and investigate their stereochemistry, chemical reactivity, and conformational stability. To achieve this, petroleum ether and chloroform extracts of the bark were subjected to column chromatography over silica gel, leading to the isolation of four coumarins: casegravol (0.002%), micromelin (0.16%), scopoletin (0.006%), and bergapten (0.004%), as well as β-sitosterol (0.02%). Among these, micromelin was the major constituent, and its structure and stereochemistry were thoroughly studied using 1H-NMR, 13C-NMR, NOE (nuclear Overhauser enhancement), IR, MS, and chemical derivatization. Micromelin exhibited a unique epoxy-γ-lactone-coumarin structure with high stability, attributed to its preferred perpendicular molecular conformation, which reduced epoxide reactivity even under acidic or nucleophilic conditions. Several chemical transformations were performed: micromelin was converted into dihydrobenzofuran derivatives, chlorohydrins, bromohydrins, and secondary alcohols, which provided firm evidence for its structural assignment. Reactions with boron tribromide, hydrochloric acid, hydrobromic acid, and zinc in methanol supported the epoxide’s stereoelectronic environment and conformational rigidity. The study concluded that Casearia graveolens is a rich source of structurally complex and conformationally stable bioactive coumarins, with micromelin being particularly noteworthy. This was also the first report of coumarins isolated from the Samydaceae family, contributing significantly to the phytochemical understanding of the genus Casearia and opening avenues for further bioactivity evaluations of these compounds. (Talapatra et al., 1983)
Wang Sibei et al. conducted a study titled "Discovery of antitumor diterpenoids from Casearia graveolens targeting VEGFR-2 to inhibit angiogenesis," focusing on the isolation of novel compounds from Casearia graveolens and evaluating their antiangiogenic and antitumor potential. The research aimed to explore natural product leads that can target vascular endothelial growth factor receptor 2 (VEGFR-2), a key mediator of tumor angiogenesis. The team isolated eight new clerodane-type diterpenoids, named caseaveolen A–H (1–8), from methanolic twig extracts of C. graveolens. Structural elucidation was accomplished using HR-ESI-MS, 1D and 2D NMR, and ECD spectral analysis. Among these, compound 8 showed strong affinity for VEGFR-2, confirmed by surface plasmon resonance (SPR) assays. Further, molecular docking revealed hydrogen bonding and hydrophobic interactions between compound 8 and key VEGFR-2 residues (e.g., Cys919, Asn923), with a binding free energy of –7.1 kcal/mol. In in vivo models, compound 8 significantly inhibited angiogenesis in transgenic zebrafish embryos, reducing intersegmental vessel length in a dose-dependent manner (e.g., 1936.26 ± 119.79 μm at 1 μmol/L). Additionally, in a zebrafish xenograft model, compound 8 notably suppressed tumor proliferation and metastasis of MCF-7 cells. Total red fluorescence intensity and disseminated tumor foci were reduced in a dose-dependent manner, confirming its anticancer efficacy. The study concluded that these diterpenoids, particularly compound 8, represent promising anticancer leads by targeting VEGFR-2-mediated angiogenesis and metastasis, and underscore the pharmaceutical potential of Casearia graveolens as a source of bioactive diterpenoids. (WANG et al., 2024)
Li et al. conducted a study titled "The Antitumor Activity and Mechanism of a Natural Diterpenoid from Casearia graveolens," focusing on the anticancer potential and mechanism of casearlucin A, a clerodane-type diterpenoid isolated from Casearia graveolens. The study aimed to elucidate the compound’s antiproliferative effects, mechanism of action, and in vivo efficacy. Using a combination of in vitro and in vivo models, the research employed MTT assays, wound-healing assays, flow cytometry for cell cycle and apoptosis, Western blotting, and zebrafish models including transgenic and xenograft lines. The results showed that casearlucin A exhibited significant cytotoxicity, with IC?? values of 3.8 µM for HepG2, 9.9 µM for A549, and 10.5 µM for HeLa cells—demonstrating stronger activity than the standard drug etoposide. Flow cytometry revealed that casearlucin A induced G0/G1 phase cell cycle arrest and apoptosis in a dose-dependent manner, with apoptotic cell rates rising up to 79.3% at 15 µM. Mechanistically, the compound upregulated Bax and downregulated Bcl-2, indicating mitochondrial pathway-mediated apoptosis. It also inhibited HepG2 cell migration by downregulating phosphorylated FAK and MMP-2, implicating the FAK/MMPs signaling pathway. In vivo, zebrafish embryo toxicity tests showed no significant deformity at doses up to 20 µM. In antiangiogenesis assays, casearlucin A significantly inhibited vessel development, reducing intersegmental vessel lengths from 2654.9 μm (control) to 1232.0 μm at 20 µM. In the zebrafish xenograft tumor model, casearlucin A decreased tumor proliferation and metastasis in a dose-dependent manner, showing comparable efficacy to etoposide. This study concluded that casearlucin A has potent anticancer activity by targeting multiple pathways including cell cycle regulation, apoptosis induction, angiogenesis inhibition, and metastasis suppression, making it a promising lead for future chemotherapeutic drug development. (Li et al., 2021)
Meesakul et al. conducted a study titled “A New Cytotoxic Clerodane Diterpene from Casearia graveolens Twigs”, focusing on the isolation, structure elucidation, and cytotoxic evaluation of novel diterpenoids from the twigs of Casearia graveolens Dalzell. The study aimed to identify new bioactive compounds with potential anticancer activity. Twigs of C. graveolens were collected from Chiang Rai, Thailand, and extracted with ethyl acetate. Phytochemical investigation led to the isolation of a new clerodane-type diterpene, caseariagraveolin (1), along with six known compounds: casearlucin G, casearvestrin C, casearvestrin B, caseargrewiin L, casearvestrin A, and caseamembrol B. Structural elucidation of caseariagraveolin was performed using HR- ESI-MS, IR, UV-Vis, 1D and 2D NMR (including COSY, HSQC, HMBC, and NOESY) techniques, confirming a tricyclic clerodane skeleton with ester and acetal functionalities. Biological evaluation was performed using the resazurin microplate assay (REMA) to determine cytotoxicity against oral cavity (KB) and breast cancer (MCF7) cell lines. Caseariagraveolin exhibited potent cytotoxicity, with IC?? values of 2.48 µM against KB cells and 6.63 µM against MCF7 cells. These values were more effective than some standard drugs, such as tamoxifen and ellipticine, against the respective cell lines. The known compounds also demonstrated varying levels of cytotoxicity as reported in previous studies. The study concluded that caseariagraveolin is a promising lead compound with strong cytotoxic potential, further validating Casearia graveolens as a rich source of bioactive clerodane diterpenes for anticancer drug discovery. (Meesakul et al., 2016)
Vieira Júnior et al. conducted a study titled “Chemical Constituents from Casearia spp. (Flacourtiaceae/Salicaceae sensu lato),” aiming to identify and report the isolation of bioactive secondary metabolites from five different Casearia species, including Casearia graveolens and its close relatives. The research primarily focused on mapping the phytochemical diversity of this genus through extraction and chromatographic isolation of various plant parts. The aerial parts (leaves and twigs) of several species were extracted using hexane, ethanol, and water, followed by open column chromatography, Sephadex LH-20 filtration, and preparative RP-HPLC, with compound characterization using IR, UV, 1D and 2D NMR, and HRMS. The study successfully isolated nine known compounds, including flavonoids (+)-taxifolin and quercetin, phenolic compound hydroquinone, diterpene (E)-phytol, steroid sitosterol, lignan (+)-pinoresinol, two amides N-trans-feruloyltyramine and N-trans- coumaroyltyramine, and cinnamic acid. Notably, (+)-taxifolin was isolated in high yield (3.8 g from 1.4 kg of C. gossypiosperma leaves), highlighting its industrial potential. Many of these compounds were reported for the first time in the Casearia genus, especially from species like C. gossypiosperma, C. decandra, and C. lasiophylla. The study concluded that the genus Casearia, particularly previously unexamined species, harbors a chemically diverse reservoir of bioactive phytochemicals. These findings expand the known chemical space of the genus and underscore its potential for pharmaceutical, nutraceutical, and cosmetic applications. The reported compounds further support earlier findings of clerodane diterpenes, steroids, lignans, flavonoids, coumarins, and phenolics as key chemotaxonomic markers of Casearia spp. (Vieira Júnior et al., 2017)
Xu et al. conducted a study titled "Characterization and Biological Evaluation of Diterpenoids from Casearia graveolens", focusing on the isolation, structural elucidation, and neurotrophic activity assessment of novel compounds from C. graveolens. The research aimed to discover plant-based compounds with potential therapeutic effects on neurodegenerative disorders such as Alzheimer’s disease. To achieve this, the twigs of C. graveolens were extracted with methanol and partitioned using ethyl acetate. Subsequent chromatographic separations (including silica gel column chromatography, medium-pressure liquid chromatography, and preparative HPLC) led to the isolation of ten new clerodane diterpenoids, named graveopenes A–J. These compounds were structurally characterized using advanced spectroscopic techniques including 1D and 2D NMR, HR-ESI-MS, and Electronic Circular Dichroism (ECD) for determining absolute configurations. Among the isolated compounds, graveopenes 3–6 and 8 showed significant bioactivity by enhancing NGF- mediated neurite outgrowth in PC12 cells, with graveopene H (compound 8) showing the most potent effect (EC?? = 3.3 μM). This biological evaluation used a neurite outgrowth assay where PC12 cells were co-treated with NGF (20 ng/mL) and the compounds, showing enhanced differentiation compared to controls. The study concluded that C. graveolens is a valuable source of neurotrophic diterpenoids, particularly those in the clerodane family. These findings highlight the therapeutic promise of natural diterpenes from Casearia graveolens as lead compounds in developing agents to combat neurodegenerative diseases, including Alzheimer's. (Xu et al., 2015)
MATERIAL AND METHODS
Collection and authentication of plant Material
Leaves of Casearia graveolens Dalz were collected between July and August 2024 from the Darekasa Hill range in Gondia district, Maharashtra. Taxonomic authentication was carried out by a botanist at Sandip University, Nashik, India. A corresponding herbarium specimen was prepared and deposited at the same institution under voucher number SUN2024/07/05.
Preparation and Storage
Freshly collected plant material was initially washed with water, followed by treatment with 95% ethanol to prevent degradation during storage and drying. The material was then chopped into smaller pieces and shade-dried until all moisture was completely eliminated. The dried plant material was subsequently ground into a fine powder and passed through a mesh no. 80 to ensure uniform particle size.
Extraction methodology
A total of 500 g of dried leaf powder was macerated in a 70:30 hydroalcoholic solution with occasional stirring at 25 ± 2°C for three days. The mixture was then filtered using a sterilized cotton plug and a Buchner funnel. The filtrate was concentrated under reduced pressure using a rotary evaporator, resulting in 14.95 g of crude hydroalcoholic extract. This extract was subsequently employed for hepatoprotective activity evaluation. The percentage yield was determined using the following formula: (Ahmed et al., 2012)
Percentage yield = Weight of Extract / Weight of powdered drug ×100
Pharmacological Investigation: Experimental animals
Male Wistar Albino Rats
Animal identification
Animals in the study were individually identified using tail markings, while experimental groups and sets were differentiated using colored markers and appropriately labeled. Each label contained detailed information, including the cage number, animal identification number, and set designation, ensuring accurate tracking and organization throughout the study.
Drugs/Chemicals
Carbon tetrachloride (CCl4)
Quarantine and Acclimatization
Quarantine refers to the isolation of newly received animals from the resident colony to evaluate their health condition and potential microbial burden. In this study, newly procured Wistar albino rats were quarantined for a period of one week to minimize the risk of introducing pathogens into the existing animal facility and to allow for physiological and nutritional stabilization before being included in experimental procedures.
Housing
The animals were housed in a well-ventilated animal facility with controlled environmental conditions, maintaining temperature and relative humidity within the range of 55–65%. They were kept in spacious polypropylene cages, and paddy husk was used as the bedding material to ensure comfort and hygiene.
Diet and Water
Animals were supplied with a standard pellet diet and had unrestricted access to purified water, except during specified fasting intervals. Food and water were provided ad libitum, and bedding material was routinely replaced to uphold hygienic housing conditions.
Drug Administration
Drugs were administered orally using a gavage technique, employing a feeding tube connected to a syringe to ensure precise dose delivery. The quantity administered was determined in accordance with the experimental protocol.
Preparation of Dose
The hydroalcoholic extract of Casearia graveolens Dalz was assessed at oral dose levels of 100, 200, and 400 mg/kg. Each dose was prepared by precisely weighing the extract and suspending it in a 0.3% carboxymethyl cellulose (CMC) solution formulated in distilled water.
Hepatoprotective Model : Carbon tetrachloride (CCl4) induced hepatotoxicity
The Rats were divided into six groups consisting of six animals in each group. Group I (control) animals will administer a single daily dose of carboxymethyl cellulose (1 mL of 1%, w/v, p.o. body weight). Group 2 received carbon tetrachloride (1 mL/kg body weight, i.p. 1:1 v/v mixture of CCI, and liquid paraffin) alone; while group 4,5,6 received orally low , moderate and high dose of extract (100, 200 and 400 mg/kg) according to body weight in (1 %, w/v, CMC) respectively along with carbon tetrachloride as in group II. Group 3 received standard compound, the known hepatoprotective compound along with carbon tetrachloride. The extract will given daily while carbontetrachloride will given for every 72 h for 14 days. Animals were sacrificed 48 h after the last dose of the drug. The liver samples were dissected and blood were collected.
The rats were then sacrificed and the livers were carefully dissected, cleaned of excess tissue. Part of the liver tissue was immediately transferred into tris and phosphate buffer for liver tissue parameter in 10% formalin for histopathological investigation.
Table 1 : Distribution of Experimental animals
|
Groups |
Treatment |
No of animals |
Route |
|
Group 1 |
Control group |
6 |
Orally |
|
Group 2 |
Hepatotoxicity induced group |
6 |
Orally |
|
Group 3 |
Standard drug (Silymarin 25mg/kg) |
6 |
Orally |
|
Group 4 |
Lower dose of Casearia graveolens Dalz. Extract (100mg/kg) |
6 |
Orally |
|
Group 5 |
Moderate dose of Casearia graveolens Dalz. Extract (200 mg/kg) |
6 |
Orally |
|
Group 6 |
Higher dose of Casearia graveolens Dalz. Extract (400 mg/kg) |
6 |
Orally |
Description of Distribution of Experimental animals
Experimental animals: Male Wistar Albino Rats
The animals were divided into six experimental groups for the evaluation of the hepatoprotective effect of the Extract. A total of 36 animals were used for this study, with each group consisting of 6 rats. The groups were organized as follows:
Control Group (Group 1):
Rats in this group did not receive any treatment with the Extract or hepatotoxic agents, serving as the baseline or control for comparison.
Hepatotoxicity-Induction Group (Group 2):
Rats in this group were exposed to hepatotoxic agents to induce liver damage but did not receive the Extract.
Standard Treatment Group (Group 3):
Rats in this group were exposed to hepatotoxic agents to induce liver damage and were subsequently treated with a standard dose of the synthetic agent for comparison purpose to investigate potential dose-dependent effects on ameliorating hepatotoxicity.
Hepatotoxicity + Low-Dose Extract Group (Group 4):
Rats in this group were exposed to hepatotoxic agents to induce liver damage and were subsequently treated with a low dose of the Extract to evaluate its potential therapeutic effects on hepatotoxicity.
Hepatotoxicity + Moderate-Dose Extract Group (Group 5):
Rats in this group were exposed to hepatotoxic agents to induce liver damage and were subsequently treated with a moderate dose of the Extract to assess its impact on alleviating liver damage.
Hepatotoxicity + High-Dose Extract Group (Group 6):
Rats in this group were exposed to hepatotoxic agents to induce liver damage and were subsequently treated with a high dose of the Extract to investigate potential dose-dependent effects on ameliorating hepatotoxicity.
EVALUATION PARAMETER
Collection of Biological samples: Blood and Serum
At the conclusion of the 14-day treatment period, blood samples were collected retro-orbitally under anesthesia. The animals were then euthanized using phenobarbital anesthesia. Serum was obtained by centrifugation at 3000 rpm for 15 minutes and subsequently subjected to analysis for various biochemical parameters.
Assessment of hepatoprotective activity
The collected blood samples were allowed to clot, followed by serum separation through centrifugation at 2500 rpm for 15 minutes. The resulting serum was analyzed for key biochemical parameters, including the liver enzymes aspartate aminotransferase (AST, U/L), alanine aminotransferase (ALT, U/L), alkaline phosphatase (ALP, U/L), and total bilirubin (mg/dL).
Estimation of Alanine transaminase ALT (SGPT)
Principle
Alanine transaminase (ALT), also referred to as serum glutamate pyruvate transaminase (SGPT), facilitates the reversible transamination between L-alanine and α-ketoglutarate, resulting in the formation of pyruvate and L-glutamate. The generated pyruvate is subsequently reduced to lactate-by-lactate dehydrogenase (LDH) in the presence of NADH, during which NADH is oxidized to NAD?. This reaction causes a decline in absorbance at 340 nm, which is directly proportional to ALT enzymatic activity.
Reaction
L-Alanine + α-Ketoglutarate ? Pyruvate + L-Glutamate (via ALT)
Pyruvate + NADH + H? ? Lactate + NAD? (via LDH)
Requirements
Instruments: Autoanalyzer, Micropipettes, Cuvettes, Water bath/incubator (37°C) Glassware:Test tubes, Volumetric flasks, Beakers
Reagent Contents (Enzymatic UV Kinetic Method)
|
Reagent Components |
Function |
|
Tris buffer (pH 7.4) |
Maintains optimal pH |
|
L-Alanine |
ALT substrate |
|
α-Ketoglutarate |
Co-substrate for ALT |
|
NADH |
Coenzyme, reacts with pyruvate |
|
LDH |
Catalyzes pyruvate conversion |
|
Preservatives |
Ensure reagent stability |
Reagents Components:
Commercially available assay kits used directly. The reagents should be mixed thoroughly and maintained at room temperature (25°C) or 37°C, depending on the protocol. For sample-start assays, the working reagent is prepared by combining the entire contents of one bottle of L2 (Starter Reagent) with one bottle of L1 (Enzyme Reagent). This mixture remains stable for up to three weeks when stored at 2–8°C.
Alternatively, smaller quantities of the working reagent can be prepared as needed by mixing four parts of L1 with one part of L2. For individual assays, 0.8 mL of L1 may be combined with 0.2 mL of L2 to obtain 1 mL of working reagent.
Sample Material
The sample material used is serum, free from hemolysis, as hemolyzed samples can interfere with the results. ALT is reported to remain stable in serum for up to 3 days when stored at 2– 8°C.
Wavelength and Conditions
Substrate Start Assay:
Following reagents were pipetted, as per the quantity mentioned in the table below, into clean dry test tubes labeled as Test (T) and serum samples and reagents was added as follows:
|
Addition Sequence |
(T) 25°C / 30°C |
(T) 37°C |
|
Working Reagent (L1) |
1.0 mL |
1.0 mL |
|
Incubate at the assay temperature for 1 minute and add |
||
|
Sample |
0.2 mL |
0.1 mL |
Mix well and read the initial absorbance A and repeat the absorbance reading after every 1, 2, & 3 minutes. Calculate the mean absorbance change per minute (?A/ min).
Sample Start Assay:
Following reagents were pipetted, as per the quantity mentioned in the table below, into clean dry test tubes labeled as Test (T) and serum samples and reagents was added as follows:
|
Addition Sequence |
(T) 25°C / 30°C |
(T) 37°C |
|
Enzyme Reagent (L1) |
0.8 mL |
0.8 mL |
|
Sample |
0.2 mL |
0.1 mL |
|
Incubate at the assay temperature for 1 minute and add |
||
|
Starter Reagent (L2) |
0.2 mL |
0.2 mL |
Mix well and read the initial absorbance A and repeat the absorbance reading after every 1, 2, & 3 minutes. Calculate the mean absorbance change per minute (?A/ min).
Calculation :
Substrate / Sample start
SGPT (ALAT) activity in U/L 25 ºC / 30 ºC = ?A / min. x 952 SGPT (ALAT) activity in U/L 370 C = ?A / min. x 1746’
Temperature Conversion Factor
|
Assay Temperature |
Desired Reporting Temperature |
||
|
37°C |
25°C |
30°C |
|
|
25°C |
1 |
1.32 |
1.82 |
|
30°C |
0.76 |
1 |
1.38 |
|
37°C |
0.55 |
0.72 |
1 |
Estimation of Aspartate transaminase -AST (SGOT)
Principle
Aspartate transaminase (AST), also known as serum glutamate oxaloacetate transaminase (SGOT), catalyzes the transamination reaction between L-aspartate and α-ketoglutarate, resulting in the formation of oxaloacetate and L-glutamate. The generated oxaloacetate is subsequently reduced to malate-by-malate dehydrogenase (MDH) in the presence of NADH, which is concurrently oxidized to NAD?. The decline in absorbance at 340 nm, corresponding to the oxidation of NADH, is directly proportional to AST activity in the sample.
Reactions involved
L-aspartate + α-ketoglutarate ? oxaloacetate + L-glutamate (via AST)
Oxaloacetate + NADH + H? ? malate + NAD? (via MDH)
Requirements
Instruments: Autoanalyzer, Micropipettes, Cuvettes, Water bath/incubator (37°C)
Glassware: Test tubes, Volumetric flasks, Beakers
Reagent Contents (Enzymatic UV Kinetic Method)
|
Reagent Components |
Function |
|
Tris buffer (pH 7.8) |
Maintains optimal pH for the reaction |
|
L-Aspartate |
Substrate for AST |
|
α-Ketoglutarate |
Co-substrate for AST |
|
NADH |
Coenzyme, reacts with oxaloacetate |
|
Malate Dehydrogenase (MDH) |
Catalyzes reduction of oxaloacetate to malate |
|
Preservatives |
Maintain reagent stability and shelf life |
Working Reagent Preparation
For the estimation of AST (SGOT) in a sample-start assay, the working reagent is prepared by combining the Enzyme Reagent (L1) with the Starter Reagent (L2). To prepare the full volume, the entire contents of one L2 bottle are mixed with one bottle of L1 to form a uniform solution. This working reagent remains stable for up to three weeks when stored at 2–8°C. For greater flexibility, smaller volumes can be prepared as needed by mixing four parts of L1 with one part of L2. For individual tests, 0.8 mL of L1 may be combined with 0.2 mL of L2 immediately before use, yielding 1.0 mL of working reagent per assay.
Sample Material
The sample material used is serum, free from hemolysis, as hemolyzed samples can interfere with the results. ASAT is reported to remain stable in serum for up to 3 days when stored at 2– 8°C.
Wavelength and Conditions
Substrate Start Assay:
Following reagents were pipetted, as per the quantity mentioned in the table below, into clean dry test tubes labeled as Test (T) and serum samples and reagents was added as follows:
|
Addition Sequence |
(T) 25°C / 30°C |
(T) 37°C |
|
Enzyme Reagent (L1) |
0.8 mL |
0.8 mL |
|
Sample |
0.2 mL |
0.1 mL |
|
(Incubate at the assay temperature for 1 minute and then add) |
||
|
Starter Reagent (L2) |
0.2 mL |
0.2 mL |
Mix well and read the initial absorbance A and repeat the absorbance reading after every 1, 2, & 3 minutes. Calculate the mean absorbance change per minute (ΔA/ min).
Sample Start Assay:
Following reagents were pipetted, as per the quantity mentioned in the table below, into clean dry test tubes labelled as Test (T) and serum samples and reagents was added as follows:
|
Addition Sequence |
(T) 25°C / 30°C |
(T) 37°C |
|
Working Reagent (L1) |
1.0 mL |
1.0 mL |
|
(Incubate at the assay temperature for 1 minute and then add) |
||
|
Sample |
0.2 mL |
0.1 mL |
Mix well and read the initial absorbance A and repeat the absorbance reading after every 1, 2, & 3 minutes. Calculate the mean absorbance change per minute (ΔA/ min).
Calculations
Substrate/ Sample start
SGOT (ASAT) Activity in U/L 25°C / 30°C = ΔA min. x 952
37°C = ΔA min. x 1746
Temperature Conversion Factor
|
Assay Temperature |
Desired Reporting Temperature |
||
|
37°C |
25°C |
30°C |
|
|
25°C |
1 |
1.37 |
2.08 |
|
30°C |
0.73 |
1 |
1.54 |
|
37°C |
0.48 |
0.65 |
1 |
Estimation of Alkaline phosphatase (ALP)
Principle
Alkaline phosphatase (ALP) catalyzes the hydrolysis of disodium phenyl phosphate under alkaline pH conditions, resulting in the formation of phenol. The liberated phenol subsequently reacts with 4-aminoantipyrine in the presence of potassium ferricyanide, serving as an oxidizing agent, to form a red-colored quinoneimine complex. The intensity of this color, measured photometrically at approximately 510–520 nm, is directly proportional to the ALP activity in the sample.
Reactions involved

Sample Material
The sample material used is serum, free from hemolysis, as hemolyzed samples can interfere with the results. ALP is reported to remain stable in serum for up to 3 days when stored at 2– 8°C.
Wavelength and Conditions
Assay:
Following reagents were pipetted, as per the quantity mentioned in the table below, into clean dry test tubes labeled as Blank (B) Standard (S) and Test (T) and serum samples and reagents was added as follows:
Mix well after each addition. Measure the absorbance of the Blank (Abs. B), Standard (Abs. S), Control (Abs. C) and Test (Abs. T) against distilled water.
|
Addition Sequence |
B (Blank) |
S (Standard) |
C (Control) |
T (Test) |
|
Distilled Water |
1.05 mL |
1.00 mL |
1.00 mL |
1.00 mL |
|
Buffer Reagent (L1) |
1.00 mL |
1.00 mL |
1.00 mL |
1.00 mL |
|
Substrate Reagent (L2) |
0.10 mL |
0.10 mL |
0.10 mL |
0.10 mL |
|
Mix well and allow to stand at 37°C for 3 minutes, then add: |
||||
|
Sample |
- |
- |
- |
0.05 mL |
|
Phenol Standard (S) |
- |
0.05 mL |
- |
|
|
Mix well and allow to stand at 37°C for 15 minutes, then add: |
||||
|
Colour Reagent (L3) |
1.00 mL |
1.00 mL |
1.00 mL |
1.00 mL |
|
Sample |
- |
- |
0.05 mL |
- |
Calculassions
Total ALP activity in KA Units = Abs. T – Abs.C / Abs.S –Abs.B
Histopathological studies
For histological assessment, liver tissues were fixed in 10% phosphate-buffered neutral formalin, dehydrated through a graded series of alcohol concentrations ranging from 50% to 100%, and subsequently embedded in paraffin. Thin sections measuring 5 µm were cut and stained using the standard hematoxylin and eosin (H&E) protocol. Qualitative microscopic examination was conducted to detect histopathological changes in the liver tissue.
Network Pharmacology
Screening active phytoconstituents of Moringa oleifera leaves
The bioactive phytoconstituents of Casearia graveolens Dalz were identified through comprehensive literature review and database mining. A few phytoconstituents were retrieved, primarily using the Indian Medicinal Plants, Phytochemistry, and Therapeutics (IMPPAT) database (https://cb.imsc.res.in/imppat/), along with reported findings from sources such as Google Scholar, PubMed, and ScienceDirect.
Retrieving phytoconstituents-associated targets
The canonical SMILES of all phytoconstituents were retrieved from the PubChem database (https://pubchem.ncbi.nlm.nih.gov/). The compound-associated target prediction was conducted by entering the canonical SMILES in a total 6 target prediction databases, with the similarity set to 0.5. The databases used include Swiss Target Prediction (http://www.swisstargetprediction.ch/), Similarity ensemble approach (SEA) (https://sea.bkslab.org/), Binding DB (https://www.bindingdb.org/rwd/bind/chemsearch/marvin/FMCT.jsp), Pass online (https://www.way2drug.com/passtargets/), ChEMBL (https://www.ebi.ac.uk/chembl/) and Super PRED target prediction (https://prediction.charite.de/subpages/target_prediction.php).
Retrieving disease-associated targets
Disease-associated genes were identified using keywords such as "hepatotoxicity" and "liver disease." Gene data were retrieved from DisGeNET (https://disgenet.com/), GeneCards (https://www.genecards.org/home), and MalaCards (https://www.malacards.org/) databases. The corresponding UniProt IDs for the retrieved genes were obtained using the UniProt ID Mapping tool (https://www.uniprot.org/id-mapping).
Constructing network and analysing
The Venny tool (https://bioinfogp.cnb.csic.es/tools/venny/) was used to identify overlapping targets between phytoconstituents and disease-associated genes. Protein-compound interaction networks were then constructed using the STRING database (https://string-db.org/) to explore functional associations.
Network analysis was further carried out using Cytoscape (version 3.10.3), and the CytoHubba plugin was employed to evaluate network centrality based on degree and other topological ranking algorithms.
Pathway Enrichment Analysis
Gene Ontology (GO) and KEGG pathway enrichment analyses were performed for the top 20 target nodes using the DAVID platform. GO analysis was used to explore the associated biological processes, cellular components, and molecular functions, while KEGG pathway analysis provided insights into the relevant signaling pathways (https://www.genome.jp/kegg/pathway.html).
Molecular docking experiment
Computational molecular docking studies were carried out using the Windows 10 operating system, Intel® Core™ i7-8700 CPU @ 3.20 GHz, and 16 GB RAM, employing the Schrödinger suite 2019-1 via Maestro 11.9 (Schrödinger, LLC, NY, 2019). The interaction pattern and potential binding affinities between the phytoconstituents and core protein were estimated through molecular docking by Mastro Suit.
Ligand and protein preparation
All ligands were constructed using the Maestro Build Panel and subsequently prepared using LigPrep (Schrödinger), which employed the MMFF94s force field to generate low-energy 3D conformers, molecular geometries, and retain specific chirality. Core protein targets were retrieved based on corresponding gene sequences from RCSB PDB (https://www.rcsb.org/) using selection criteria, including a resolution of ≤ 2.5 Å, Homosapiens origin, and X-ray crystallography and saved in PDB format. Protein is pre-processed to remove water molecules, optimise and minimize to lower energy state for docking by using the protein preparation wizard workflow in the Maestro suite.
Identification of active site
The site map tool was employed to study the prepared protein's possible binding site by recognizing active ligands. Based on the d-score (nearest to 1) the active site was selected for gride generation.
Molecular docking
The prepared ligand and protein were docked using glide ligand docking and glide extra precision (XP) mode at active sites identified by the sitemap by considering flexibility.
Results Extractive Values
A total of 500 g of plant material was subjected to maceration in 2000 mL of a hydroalcoholic solution (70% ethanol and 30% water) with occasional stirring at 25 ± 2°C for three days. The resulting mixture was filtered using a Buchner funnel lined with sterilized cotton. The solvent was then completely evaporated under reduced pressure using a rotary evaporator, yielding 14.95 g of crude hydroalcoholic extract. This extract was subsequently utilized for the evaluation of hepatoprotective activity.
Yield of Hydroalcoholic Extract- 2.99 %
Pharmacological Invetigation
Effect of hydroalcoholic extract of Casearia graveolens Dalz on CCL4 Induce hepatotoxicity.
Body Weight
Monitoring changes in body weight serves as a crucial non-invasive parameter in toxicological and pharmacological studies, especially those involving hepatotoxicity. In models of CCl?- induced liver damage, body weight is considered an indirect but sensitive indicator of systemic toxicity, metabolic disturbance, and general animal well-being. Hepatic dysfunction often disrupts appetite regulation, protein metabolism, and nutrient absorption, leading to significant body weight loss in affected animals. In the present study, a significant reduction in body weight was observed in the CCl?-induced hepatotoxic control group over the 14-day period, confirming the systemic impact of hepatic injury. This decrease highlights the catabolic stress and impaired physiological functions associated with liver toxicity. Conversely, the normal control group showed a steady and expected increase in body weight, validating normal metabolic activity in the absence of hepatotoxic insult. Treatment with the standard hepatoprotective agent mitigated the weight loss significantly, indicating restoration of hepatic function and metabolic normalization. Importantly, the animals treated with the hydroalcoholic extract of Casearia graveolens Dalz at doses of 100, 200, and 400 mg/kg exhibited dose- dependent protection against CCl?-induced weight loss. The 400 mg/kg dose group showed body weight changes closely aligned with the standard drug group, suggesting a robust hepatoprotective effect. These observations affirm the utility of body weight as a supportive parameter for evaluating the protective efficacy of plant extracts in liver injury models.
The body weight of animals was determined on 1st and 14th day of the study period and these are tabulated in Table 2.
Table 02: Effect of Plant material and Standard drug on body weight of animals
|
Animal |
Control (Days) |
CCL4 induced group (Days) |
Standard drug (Days) |
100 mg/kg Extract (Days) |
200 mg/kg Extract (Days) |
400 mg/kg Extract (Days) |
||||||
|
1 |
14 |
1 |
14 |
1 |
14 |
1 |
14 |
1 |
14 |
1 |
14 |
|
|
1. |
160 |
167 |
164 |
140 |
160 |
166 |
164 |
155 |
163 |
161 |
160 |
154 |
|
2. |
155 |
153 |
163 |
142 |
166 |
160 |
162 |
147 |
159 |
150 |
165 |
160 |
|
3. |
198 |
204 |
168 |
142 |
162 |
155 |
161 |
149 |
175 |
161 |
169 |
174 |
|
4. |
210 |
222 |
163 |
150 |
181 |
166 |
169 |
152 |
159 |
149 |
163 |
155 |
|
5. |
165 |
160 |
164 |
151 |
165 |
158 |
175 |
155 |
168 |
159 |
162 |
164 |
|
6. |
170 |
173 |
169 |
153 |
164 |
152 |
166 |
151 |
167 |
151 |
168 |
157 |
|
Means |
175.20 |
178.20 |
165.14 |
146.24 |
166.19 |
159.41 |
166.1 |
151.47 |
165.07 |
155.07 |
164.46 |
160.52 |
|
SEM |
9.1165 |
11.0857 |
1.0775 |
2.29 |
3.0623 |
2.3345 |
2.12 |
1.3102 |
2.5088 |
2.3440 |
1.4317 |
3.0514 |
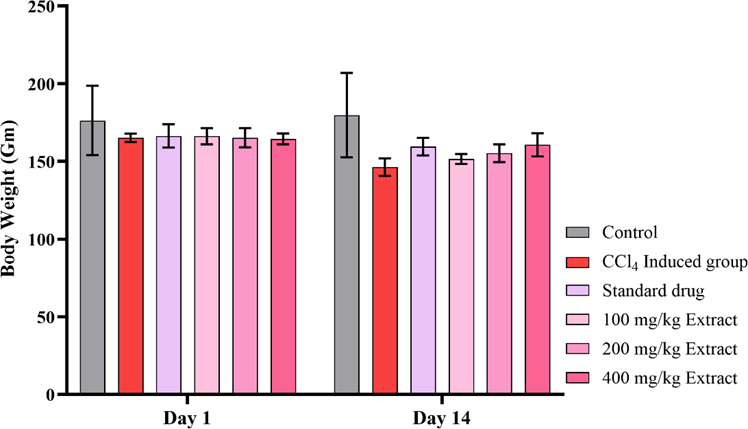
Figure 5: Effect of Plant material and Standard drug on body weight of animals
The effect of hydroalcoholic extract of Casearia graveolens Dalz on body weight was statistically assessed using two-way repeated measures ANOVA, considering treatment groups (six levels) and time points (Day 1 and Day 14) as the main factors. This design accounts for within-subject variability and provides a more robust measure of treatment effect across time. The interaction effect between treatment groups and time (Row Factor × Column Factor) was statistically significant (F(5,30) = 11.48, p < 0.0001), indicating that the pattern of body weight change over time differed significantly across treatment groups. This suggests that the extent of weight maintenance or gain was dependent on the specific intervention received. The main effect of Row Factor (i.e., group differences across all time points) was also highly significant (F(1,30) = 77.84, p < 0.0001), accounting for 9.44% of the total variation, which implies substantial variability in body weight among the different treatment arms. Similarly, the Column Factor (time) was significant (F(5,30) = 3.05, p = 0.0240), capturing 26.97% of the total variation, and showing that time progression itself had a meaningful impact on body weight, regardless of the treatment group. Moreover, the subject effect accounted for the largest portion of variability (52.98%) with a highly significant p-value (p < 0.0001), indicating that individual baseline variations in animal weight were substantial and well-captured in the repeated measures design. The mean body weight on Day 1 was 167.3 g, while on Day 14 it was reduced to 158.8 g, showing a statistically significant mean reduction of 8.444 g (95% CI: 6.490 to 10.40; SE = 0.9571). This result emphasizes that the CCl? insult led to a net weight loss, but the degree varied based on the protective treatment, validating the model's sensitivity and the intervention's effectiveness. Together, these results strongly support the conclusion that treatment with the plant extract exerted a dose-dependent protective effect against weight loss typically induced by CCl? toxicity, and that body weight serves as a useful, statistically sensitive, and biologically relevant endpoint in the evaluation of hepatoprotective agents.
Serum Glutamic Oxaloacetic Transaminase (SGOT)
Serum Glutamic Oxaloacetic Transaminase (SGOT), also known as Aspartate Aminotransferase (AST), serves as a critical enzymatic biomarker in the assessment of hepatocellular integrity and liver function. It is predominantly localized within hepatic cells, and its release into the bloodstream is markedly increased in response to liver injury or necrosis. In hepatotoxicity models, particularly those induced by carbon tetrachloride (CCl?), a substantial elevation in AST levels reflects acute hepatic insult and compromised membrane permeability. Therefore, the quantitative evaluation of AST levels plays a vital role in determining the extent of liver damage and the protective efficacy of therapeutic agents.
The SGOT levels of the animals treated with CCL4 alone and those that were given CCL4 and Silymarin, Casearia graveolens Dalz were estimated on Day 14. They are tabulated in Table 3 & 4.
Table 03: Observations of AST (U/ml) of all animal groups
|
Animal Number |
AST (U/ml) |
|||||
|
Group 1 |
Group 2 |
Group 3 |
Group 4 |
Group 5 |
Group 6 |
|
|
1 |
32.95 |
173.2 |
46.9 |
147.73 |
126.11 |
53.12 |
|
2 |
32.59 |
171.83 |
45.3 |
148.77 |
125.13 |
54.67 |
|
3 |
32.19 |
171.41 |
47.61 |
142.73 |
137.3 |
56.76 |
|
4 |
33.19 |
173.95 |
46.78 |
152.63 |
133.02 |
54.47 |
|
5 |
34.86 |
176.64 |
45.6 |
158.69 |
139.18 |
55.34 |
|
6 |
33.85 |
172.42 |
46.37 |
154.7 |
127.54 |
52.41 |
Table 04: Means Observations of AST (U/ml) of all animal groups
|
Groups |
Treatment |
AST (U/ml) ± SEM |
|
Group 1 |
Control group |
33.26 ± 0.3916 |
|
Group 2 |
CCL4 induced group |
173.23 ± 0.7762 |
|
Group 3 |
Standard drug (Silymarin 25 mg/kg) |
46.42 ± 0.3514 |
|
Group 4 |
Lower dose of Casearia graveolens Dalz Extract (100 mg/kg) |
150.78 ± 2.3054 |
|
Group 5 |
Moderate dose of Casearia graveolens Dalz Extract (200 mg/kg) |
131.26 ± 2.4505 |
|
Group 6 |
Higher dose of Casearia graveolens Dalz Extract (400 mg/kg) |
54.44 ± 0.6352 |
Values are expressed as Mean (n=6)

Figure 6: Effect of Plant material and Standard drug on AST Levels (SGOT)
Serum AST (Aspartate Transaminase) is a key enzymatic biomarker for assessing hepatocellular integrity, and its elevation is directly associated with hepatic cell injury. In the present study, the impact of the hydroalcoholic extract of Casearia graveolens Dalz on AST activity was analyzed across six experimental groups using one-way ANOVA. The groups included normal control, CCl?-induced group, standard drug-treated, and extract-treated groups at three dose levels (100, 200, and 400 mg/kg). The ANOVA revealed a highly significant difference among treatment groups (F(5,30) = 1743, p < 0.0001), with an exceptionally strong effect size (R² = 0.9966), indicating that over 99.6% of the total variation in AST levels is attributable to the treatment effect. This clearly establishes the robust impact of interventions on AST activity, suggesting differential protection or aggravation of hepatocellular damage across groups. Bartlett’s test for homogeneity of variances returned a significant result (χ² = 29.55, p < 0.0001), indicating heterogeneity in group variances and confirming that the spread of AST values differs among the treatments. This variability is expected in pharmacological studies, especially when comparing disease-induced and recovery groups. The very high F- value and minimal residual mean square (MS = 12.6) further reinforce the reliability of the treatment effect. The standard treatment and higher doses of the extract likely exerted a hepatoprotective effect by reducing AST leakage from damaged hepatocytes, whereas the CCl? group exhibited marked AST elevation, confirming hepatic injury.
The post-hoc analysis using Tukey’s multiple comparisons test provided deeper insight into the significant differences among the treatment groups with respect to serum AST levels. The CCl?-induced group showed a dramatically elevated mean AST level (173.2 U/ml) compared to the normal control group (33.26 U/ml), with a highly significant mean difference of -140 U/ml (p < 0.0001). This confirms the hepatotoxic impact of CCl?, as AST is a key marker of liver cell injury released during hepatocellular damage. The standard drug-treated group exhibited a significant reduction in AST levels (46.42 U/ml), indicating hepatoprotective potential. Notably, all extract-treated groups (100, 200, and 400 mg/kg) demonstrated dose- dependent improvements. The 400 mg/kg extract group showed the most significant hepatoprotective effect among the extract doses with an AST mean of 54.44 U/ml, nearly comparable to the standard. The differences in AST levels between CCl? and extract groups were highly significant (p < 0.0001), particularly between CCl? and 100 mg/kg (mean diff = 22.45), 200 mg/kg (41.97), and 400 mg/kg (118.8).
Comparisons between the standard group and extract-treated groups revealed that 100 mg/kg and 200 mg/kg extract groups had significantly higher AST levels than the standard, indicating a moderate effect. However, the 400 mg/kg extract group did not differ significantly from the standard drug group (mean diff = -8.02, p = 0.0059), suggesting comparable efficacy at this dose. Further, the extract groups also exhibited significant pairwise differences among themselves, indicating a clear dose–response relationship. The comparison between 100 mg/kg and 400 mg/kg showed a large and significant difference (mean diff = 96.34), confirming that the hepatoprotective effect increased with dose escalation. Collectively, these multiple comparison results reinforce the extract’s potential to restore hepatic function by significantly reducing AST levels, especially at the higher doses, and highlight the 400 mg/kg dose as the most effective, closely approximating the standard treatment in efficacy.
Serum glutamate pyruvate transaminase (SGPT)
Serum Glutamate Pyruvate Transaminase (SGPT), also known as Alanine Aminotransferase (ALT), is a liver-specific enzyme that plays a crucial role in amino acid metabolism and is commonly used as a sensitive biomarker for liver injury. Under normal physiological conditions, ALT activity is predominantly confined to hepatocytes. However, in the event of hepatic cell membrane damage or necrosis, ALT is rapidly released into the circulation, leading to elevated serum levels. This makes SGPT a reliable indicator of hepatocellular damage, especially in experimental hepatotoxicity models such as CCl?-induced liver injury. Monitoring SGPT activity not only reflects the severity of hepatic damage but also aids in evaluating the hepatoprotective potential of pharmacological agents.
The SGPT levels of the animals treated with CCL4 alone and those that were given CCL4 and Silymarin/ Casearia graveolens Dalz were estimated on Day 14. They are tabulated in Table 5 & 6.
Table 5: Observations of ALT (U/ml) of all animal groups
|
Animal Number |
ALT (U/ml) |
|||||
|
Group 1 |
Group 2 |
Group 3 |
Group 4 |
Group 5 |
Group 6 |
|
|
1 |
20.22 |
185.63 |
40.85 |
140.36 |
78.01 |
49.19 |
|
2 |
20.32 |
186.5 |
43.11 |
134.95 |
79.09 |
50.23 |
|
3 |
21.26 |
184.75 |
41.96 |
139.04 |
76.12 |
46.06 |
|
4 |
21.29 |
189.9 |
44.13 |
139.22 |
80.22 |
48.08 |
|
5 |
21.26 |
184.09 |
39.9 |
137.14 |
77.92 |
47.7 |
|
6 |
19.82 |
187.9 |
39.01 |
135.02 |
79.31 |
52.1 |
Table 6: Mean Observations of ALT (U/ml) of all animal groups
|
Groups |
Treatment |
ALT (U/ml) ± SEM |
|
Group 1 |
Control group |
20.68 ± 0.2661 |
|
Group 2 |
CCL4 induced group |
186.45 ± 0.8782 |
|
Group 3 |
Standard drug (Silymarin 25 mg/kg) |
41.45 ± 0.7937 |
|
Group 4 |
Lower dose of Casearia graveolens Dalz Extract (100 mg/kg) |
137.60 ± 0.9345 |
|
Group 5 |
Moderate dose of Casearia graveolens Dalz Extract (200 mg/kg) |
78.43 ± 0.5826 |
|
Group 6 |
Higher dose of Casearia graveolens Dalz Extract (400 mg/kg) |
48.85 ± 0.8616 |
Values are expressed as Mean (n=6)
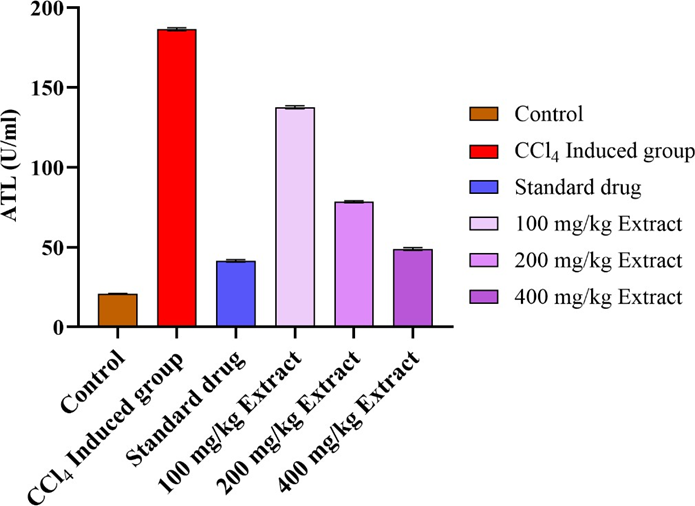
Figure 7: Effect of Plant material and Standard drug on ALT Levels (SGPT)
The statistical evaluation of serum ALT (SGPT) levels using one-way ANOVA revealed a highly significant variation among the experimental groups (F?,?? = 7156, p < 0.0001), indicating that the different treatment conditions had a substantial effect on liver enzyme activity. The coefficient of determination (R² = 0.9992) suggests that nearly all the variability in serum ALT levels can be explained by the group-wise differences. The Bartlett’s test for homogeneity of variances yielded a p-value of 0.2157, indicating no significant difference in standard deviations among the groups (p > 0.05). Thus, the assumption of homoscedasticity is satisfied, validating the application of ANOVA for this dataset. The between-group sum of squares (SS = 122638) was substantially higher than the within-group residual variance (SS = 102.8), further supporting the presence of statistically meaningful differences between the groups. The large F-ratio, combined with the extremely low p-value, confirms the strong discriminatory effect of treatments on ALT levels.
Following the confirmation of significant overall group differences via ANOVA (F?,?? = 7156, p
< 0.0001), Tukey’s multiple comparisons test was performed to evaluate pairwise differences in serum ALT levels across the six treatment groups. The results provided compelling evidence of hepatocellular injury in the CCl?-induced group, as demonstrated by a highly significant increase in ALT levels when compared with the control group (Mean Diff. = -165.8, p < 0.0001), indicating substantial hepatocellular leakage and liver damage.Compared to the CCl? group, all treated groups—including the standard drug and varying doses (100, 200, and 400 mg/kg) of the hydroalcoholic extract of Casearia graveolens—showed a statistically significant reduction in ALT levels, suggesting marked hepatoprotective effects. The standard drug showed a difference of 145 units (p < 0.0001) from the CCl? group, whereas the extract-treated groups demonstrated graded protection: 48.85 units for 100 mg/kg, 108 units for 200 mg/kg, and 137.6 units for 400 mg/kg. These findings reflect a dose-dependent protective effect of the extract. Furthermore, comparisons between the control and treatment groups confirmed that even at 400 mg/kg, the extract did not restore ALT to control levels (Mean Diff. = -28.17, p < 0.0001), although it approached the effect of the standard drug (Mean Diff. between standard and 400 mg/kg = -7.4, p < 0.0001), suggesting near-complete normalization. The compact letter display confirms that the CCl? group (A) is statistically distinct from all other groups, and the control group (F) showed the lowest ALT levels. These findings collectively underscore the efficacy of Casearia graveolens in mitigating hepatocellular damage, with 400 mg/kg extract showing the highest restoration of hepatic enzyme profile among the tested doses.
Alkaline Phosphatase (ALP)
Alkaline phosphatase (ALP) is an important hydrolase enzyme predominantly present in the liver, bile ducts, and bones. In hepatocellular injury, especially when associated with cholestasis or bile duct obstruction, ALP levels significantly rise due to increased synthesis and release into the bloodstream. Hence, ALP serves as a crucial diagnostic and prognostic biomarker in evaluating hepatic function and bile duct integrity. In the context of hepatotoxicity induced by carbon tetrachloride (CCl?), elevated ALP activity is indicative of severe hepatobiliary dysfunction and membrane leakage. Monitoring serum ALP levels thus provides insight into the extent of liver damage and the protective efficacy of therapeutic interventions.
The ALP levels of the animals treated with CCL4 alone and those that were given CCL4 and Silymarin/ Casearia graveolens Dalz were estimated on Day 14. They are tabulated in Table 7 & 8.
Table 7: Observations of ALP (U/ml) of all animal groups
|
Animal Number |
ALP (U/ml) |
|||||
|
Group 1 |
Group 2 |
Group 3 |
Group 4 |
Group 5 |
Group 6 |
|
|
1 |
134.32 |
196.67 |
143.61 |
175.11 |
162.92 |
155.08 |
|
2 |
135.06 |
192.15 |
141.77 |
176.23 |
164.69 |
153.67 |
|
3 |
131.29 |
195.14 |
141.89 |
174.14 |
163.7 |
152.14 |
|
4 |
133.27 |
196.83 |
143.69 |
179.8 |
165.62 |
153.07 |
|
5 |
134.28 |
194.18 |
142.68 |
175.1 |
163.18 |
152.24 |
|
6 |
134.38 |
195.9 |
145.65 |
178.02 |
161.73 |
150.27 |
Table 8: Mean Observations of ALP (U/ml) of all animal groups
|
Groups |
Treatment |
ALP (U/ml) ± SEM |
|
Group 1 |
Control group |
133.76 ± 0.5476 |
|
Group 2 |
CCL4 induced group |
195.13 ± 0.7219 |
|
Group 3 |
Standard drug (Silymarin 25 mg/kg) |
143.20 ± 0.5899 |
|
Group 4 |
Lower dose of Casearia graveolens Dalz Extract (100 mg/kg) |
176.38 ± 0.8693 |
|
Group 5 |
Moderate dose of Casearia graveolens Dalz Extract (200 mg/kg) |
163.63 ± 0.5598 |
|
Group 6 |
Higher dose of Casearia graveolens Dalz Extract (400 mg/kg) |
152.73 ± 0.6623 |
Values are expressed as Mean (n=6)
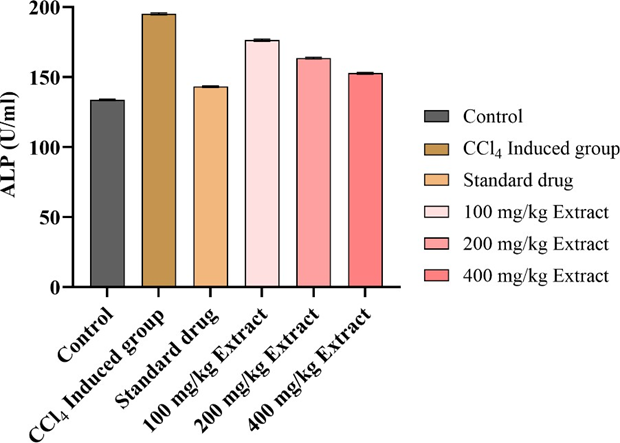
Figure 8: Effect of Plant material and Standard drug on ALP Levels
The determination of serum alkaline phosphatase (ALP) levels serves as a crucial biomarker for evaluating hepatic function, especially in cases of hepatobiliary injury or toxicity. In this study, one-way ANOVA analysis was conducted to assess the hepatoprotective potential of the hydroalcoholic extract of Casearia graveolens against CCl?-induced hepatotoxicity in experimental animals. The ANOVA results revealed a highly significant treatment effect (F(5,30) = 1137, p < 0.0001*), indicating that ALP levels varied markedly across the different treatment groups. The high R² value of 0.9947 suggests that 99.47% of the total variation in ALP levels was attributable to treatment differences, which strongly supports the robustness and reliability of the model used for analysis. Additionally, Bartlett’s test for homogeneity of variances yielded a statistic of 1.546 with a p-value of 0.9078, indicating no significant difference in standard deviations across the groups. This validates the assumption of equal variance necessary for ANOVA and confirms the consistency of the data. Furthermore, the non-significant result of Bartlett’s test strengthens the credibility of the ANOVA output by ensuring that the observed differences are due to actual treatment effects rather than random dispersion.
The multiple comparison analysis for serum alkaline phosphatase (ALP) activity, evaluated through Tukey’s test, revealed statistically significant differences across all treatment groups (p < 0.0001). These findings reinforce the outcomes of the ANOVA, confirming that the hydroalcoholic extract of Casearia graveolens has a marked modulatory effect on ALP levels in CCl?-induced hepatotoxicity. A pronounced elevation in ALP levels was observed in the CCl?-induced group (195.1 U/ml), which differed significantly from the control group (133.8 U/ml) with a mean difference of -61.38 (**p < 0.0001). This confirms that CCl? administration causes substantial hepatic damage reflected in elevated ALP activity. Treatment with Casearia graveolens extract led to dose-dependent reductions in ALP levels. The 100 mg/kg dose group showed a mean ALP value of 176.4 U/ml and a significant reduction compared to the CCl? group (mean difference = 18.75, **p < 0.0001), while the 200 mg/kg and 400 mg/kg extract groups showed further reductions to 163.6 and 152.7 U/ml, respectively. The mean differences between the CCl? group and 200 mg/kg and 400 mg/kg groups were 31.5 and 42.4, respectively, both being highly significant (**p < 0.0001). The extract's efficacy was comparable with the standard treatment group (143.2 U/ml), as evident from a statistically significant difference between the CCl? and standard groups (mean difference = 51.93, **p < 0.0001). However, ALP levels in the standard treatment group were still significantly higher than the control (mean difference = -9.448, **p < 0.0001), suggesting partial but notable protection. Moreover, all extract-treated groups significantly differed from one another, confirming a dose-dependent effect. The differences between 100 mg/kg vs. 200 mg/kg (mean difference = 12.75), 100 mg/kg vs. 400 mg/kg (23.65), and 200 mg/kg vs. 400 mg/kg (10.9) were all statistically significant (**p < 0.0001). These results further support the graded hepatoprotective potential of Casearia graveolens extract. The multiple comparison data establish that Casearia graveolens extract significantly ameliorates CCl?-induced elevations in serum ALP levels in a dose-dependent manner. The highest dose (400 mg/kg) was most effective in restoring ALP levels towards normal, suggesting potent hepatoprotective efficacy comparable to the standard drug.
Total bilirubin (TB)
Total bilirubin (TB) is a key clinical indicator of hepatic function and serves as a sensitive biomarker for the assessment of hepatocellular damage and biliary obstruction. It is a breakdown product of hemoglobin metabolism, processed and excreted by the liver. Under physiological conditions, bilirubin is conjugated and eliminated via bile; however, hepatic injury caused by toxicants such as carbon tetrachloride (CCl?) can impair this process, leading to elevated serum TB levels. Such an increase reflects compromised liver function, particularly affecting hepatocyte integrity and biliary clearance. Therefore, estimation of TB is crucial in evaluating the severity of hepatic dysfunction and the therapeutic efficacy of hepatoprotective agents.
The TB levels of the animals treated with CCL4 alone and those that were given CCL4 and Silymarin/ Casearia graveolens Dalz were estimated on Day 14. They are tabulated in Table 9 & 10.
Table 9: Observations of TB (U/ml) of all animal groups
|
Animal Number |
TB (U/ml) |
|||||
|
Group 1 |
Group 2 |
Group 3 |
Group 4 |
Group 5 |
Group 6 |
|
|
1 |
0.3299 |
1.4956 |
0.35 |
0.6258 |
0.562 |
0.3925 |
|
2 |
0.3394 |
1.4532 |
0.3713 |
0.6576 |
0.5515 |
0.4031 |
|
3 |
0.3182 |
1.4637 |
0.3713 |
0.6364 |
0.5728 |
0.3828 |
|
4 |
0.3394 |
1.4745 |
0.3607 |
0.647 |
0.594 |
0.3925 |
|
5 |
0.3299 |
1.4532 |
0.35 |
0.7 |
0.6152 |
0.4031 |
|
6 |
0.3299 |
1.432 |
0.35 |
0.6576 |
0.5515 |
0.4243 |
Table 10: Mean Observations of TB (U/ml) of all animal groups
|
Groups |
Treatment |
TB (U/ml) ± SEM |
|
Group 1 |
Control group |
0.33 ± 0.0032 |
|
Group 2 |
CCL4 induced group |
1.46 ± 0.0088 |
|
Group 3 |
Standard drug (Silymarin 25 mg/kg) |
0.35 ± 0.0042 |
|
Group 4 |
Lower dose of Casearia graveolens Dalz Extract (100 mg/kg) |
0.65 ± 0.0104 |
|
Group 5 |
Moderate dose of Casearia graveolens Dalz Extract (200 mg/kg) |
0.57 ± 0.0104 |
|
Group 6 |
Higher dose of Casearia graveolens Dalz Extract (400 mg/kg) |
0.39 ± 0.0058 |
Values are expressed as Mean (n=6)

Figure 9: Effect of Plant material and Standard drug on Total Biillurubin
The one-way ANOVA performed on serum total bilirubin (TB) levels across the six treatment groups (A–F) revealed a highly significant variation among the group means, indicating the influence of the treatments on TB levels. The computed F-value was 3049, with a corresponding p-value < 0.0001, clearly demonstrating a statistically significant difference among the groups at the 0.05 significance level. The R-squared value of 0.998 suggests that approximately 99.8% of the variability in serum TB levels can be attributed to the differences in treatment conditions, confirming a strong effect of the treatments. Further, the Bartlett’s test was performed to assess the homogeneity of variances across the groups. The Bartlett’s statistic was 9.483 with a p-value of 0.0913, indicating that there was no statistically significant difference in the variances (i.e., the assumption of equal variances was not violated). Therefore, the data satisfied the assumptions required for valid interpretation of the ANOVA. The sum of squares (SS) for the treatment (between-group) was 5.471, with 5 degrees of freedom (DF), and the mean square (MS) was 1.094. The residual (within-group) variation was relatively low, with an SS of 0.01077, and the MS of 0.000359, indicating precise and consistent measurements within groups.
Tukey’s multiple comparisons test for total bilirubin (TB) levels was performed to assess the significance of differences between experimental groups following ANOVA. The analysis demonstrated a highly significant elevation in TB levels in the CCl?-induced hepatotoxic group when compared to the control group (mean difference = -1.131, p < 0.0001), confirming the substantial liver injury caused by CCl? administration. Interestingly, there was no statistically significant difference between the control and standard-treated groups (p = 0.1462), indicating that the standard hepatoprotective drug effectively restored TB levels close to normal. The groups treated with the hydroalcoholic extract of Casearia graveolens at doses of 100, 200, and 400 mg/kg all showed significant reductions in TB levels when compared to the CCl? group, with the differences being dose-dependent. The 100 mg/kg group exhibited a mean difference of 0.8082 (p < 0.0001), the 200 mg/kg group showed a mean difference of 0.8879 (p < 0.0001), and the 400 mg/kg group demonstrated the most substantial improvement with a mean difference of 1.062 (p < 0.0001). These findings clearly indicate that the extract provides protective effects against CCl?-induced hepatic damage, and the efficacy improves with increasing dosage. Further comparisons between the standard-treated group and the extract- treated groups also revealed significant differences. The 400 mg/kg group showed a slightly lower TB level than the standard drug group (mean difference = -0.04075, p = 0.0095), suggesting that the highest dose of the extract may offer hepatoprotection comparable to or even better than the standard treatment. Additionally, pairwise comparisons among the extract doses revealed significant differences, confirming a dose-dependent trend in the hepatoprotective action of the extract. The compact letter display grouped the CCl?-induced group separately (Group A) due to its significantly elevated TB levels, while the control and standard drug groups shared the same category (Group E and F), indicating near-normal TB levels. The extract-treated groups were distributed across intermediate categories (Groups B– D), further supporting the progressive therapeutic effect of increasing extract doses.
Histological examination
In preclinical studies evaluating hepatotoxicity, histopathological examination of liver tissue serves as a vital tool for identifying and characterizing cellular and structural alterations resulting from toxic exposure. One of the primary indicators of liver injury is hepatocellular necrosis, which reflects the death of hepatocytes. Under the microscope, necrotic cells may appear swollen, fragmented, or completely lysed, with the extent of necrosis varying based on the nature and severity of the insult. Another hallmark of liver damage is inflammation, typically presenting as infiltration of immune cells—such as lymphocytes, neutrophils, and macrophages—into hepatic parenchyma. This inflammatory response, known as hepatitis, often coexists with hepatocellular injury and can range from mild to severe in intensity. In addition, steatosis or fatty liver may be observed, characterized by the abnormal accumulation of lipid droplets within hepatocytes. This condition may reflect underlying metabolic disturbances or drug-induced liver injury, with lipid accumulation manifesting as either microvesicular or macrovesicular steatosis. Cholestasis, or impaired bile flow, may also be evident in histological sections. This is typically marked by the presence of bile plugs within canaliculi, bile duct proliferation, or bile stasis, and is often associated with bile duct injury and hepatocyte dysfunction. In more chronic or progressive toxicological models, fibrosis may develop, indicated by the accumulation of collagen and other extracellular matrix components. Histopathological features include fibrous septa formation, bridging fibrosis, and architectural distortion of the liver, which, if unchecked, may progress toward cirrhosis. Despite injury, the liver’s inherent capacity for regeneration is another important aspect observed in histopathological evaluations. Signs of regenerative activity include increased mitotic figures, hypertrophy of hepatocytes, and formation of regenerative nodules. Additionally, depending on the toxicant and its specific mechanism of action, a variety of specific lesions may appear. These can include vascular changes, granulomas, bile duct injury, or other cell-specific alterations that offer insight into the compound’s mode of hepatotoxicity.

Figure 10: (a) Normal liver, (b) liver intoxicated with CCl?: gross image shows major color changes of liver lobes , (c) liver treated silymarin and induced with CCl?: spot of color changes was noted (d) liver treated with 100 mg/kg Casearia graveolens Dalz and induced by CCl?, (e) liver treated with 200 mg/kg Casearia graveolens Dalz and induced by CCl?, (f) liver treated with 400 mg/ Casearia graveolens Dalz and induced by CCl?.
(A) Control group , (B) CCl?-induced group ,(C) STD group ,(D) 100mg/kg Casearia graveolens Dalz group , (E) 200mg/kg Casearia graveolens Dalz Group (F) 400mg/kg Casearia graveolens Dalz group
Network Pharmacology
Target Identification and Overlap Analysis
A total of 560 drug-related targets were identified using Vinney for 11 phytoconstituents from Casearia graveolens leaves. Simultaneously, 19,343 disease-related genes were collected from hepatotoxicity-related databases (GeneCards, CTD, and DisGeNET) based on the CCl?- induced model. The Venn diagram revealed 558 overlapping targets, indicating the potential hepatoprotective space modulated by the phytoconstituents (Figure 11). This high level of overlap suggests a strong convergence between the pharmacological activity of the plant and molecular mechanisms of hepatic injury and repair.

Figure 11: Venn diagram showing the overlap between phytoconstituent-derived protein targets of Casearia graveolens and genes associated with CCl?-induced hepatotoxicity. A total of 558 common targets were identified, highlighting significant pharmacological convergence.
Protein–Protein Interaction Network
The 558 overlapping targets were submitted to STRING to construct a high-confidence interaction network (Figure 12). The resulting PPI network showed a complex and highly interconnected topology, reflecting the systemic regulation of hepatic repair and inflammation. Functional clusters were observed involving immune response, cell survival, apoptosis, oxidative stress, and fibrosis—all of which are critical in the pathogenesis and progression of liver damage caused by CCl? toxicity.

Figure 12: Protein–protein interaction (PPI) network of the 558 overlapping genes constructed using the STRING database. The dense connectivity within the network suggests strong functional association among targets involved in liver protection and regeneration.
Hub Gene Analysis
Degree-based topological analysis of the PPI network revealed AKT1, TNF, SRC, EGFR, BCL2, HSP90AA1, NFKB1, ESR1, CASP3, and HIF1A as the top ten hub genes. AKT1, the highest-ranked node, is essential for hepatocyte survival, cellular metabolism, and regeneration through PI3K-Akt signaling. Its involvement is well-established in liver tissue repair following toxic damage. TNF, a pro-inflammatory cytokine, when overexpressed contributes to liver necrosis and fibrosis; hence, its modulation is crucial for suppressing inflammation-induced hepatic injury. SRC, a tyrosine kinase, is a known upstream modulator of several pathways including MAPK and NF-κB and is implicated in both cellular repair and fibrotic transitions. EGFR plays a dual role: promoting hepatocyte proliferation and modulating anti-apoptotic signaling. BCL2 and CASP3 form the critical apoptotic axis — BCL2 inhibiting mitochondrial pore opening, while CASP3 executes the final stage of programmed cell death. Their opposing but related roles emphasize the balance between survival and death within hepatic cells. NFKB1 serves as a master regulator of inflammatory responses and its downregulation can prevent prolonged inflammatory damage. HSP90AA1, a heat-shock protein, facilitates folding of stress-induced misfolded proteins, reducing endoplasmic reticulum stress during toxic exposure. HIF1A promotes angiogenesis and metabolic adaptation under hypoxia, a common feature of hepatotoxic conditions. The tight functional interplay among these hub proteins underlines the extract’s broad-spectrum regulatory potential.

Figure 13: Visualization of the top 10 hub genes obtained through degree centrality analysis using Cytoscape. Key proteins such as AKT1, TNF, SRC, and EGFR were highly ranked, indicating their central roles in inflammatory regulation, apoptosis inhibition, and hepatic regeneration.
Table 11: Top 10 hub genes ranked by degree centrality
|
Rank |
Name |
Score |
|
1 |
AKT1 |
231 |
|
2 |
TNF |
212 |
|
3 |
SRC |
196 |
|
4 |
EGFR |
182 |
|
5 |
CASP3 |
177 |
|
6 |
BCL2 |
173 |
|
7 |
HIF1A |
166 |
|
8 |
ESR1 |
162 |
|
9 |
HSP90AA1 |
159 |
|
10 |
NFKB1 |
153 |
Molecular Docking Results
The molecular docking study was performed to assess the hepatoprotective potential of phytoconstituents identified from the medicinal plant, targeting genes associated with liver injury and repair. Through network pharmacology, four critical genes—AKT1, TNF, SRC, and EGFR—were identified as key regulators of hepatoprotection. These genes were mapped to specific protein structures available in the Protein Data Bank: AKT1 (1UNQ, 4EJN), TNF (2AZ5, 5UUI), SRC (1A07, 1Y57), and EGFR (1M17, 2GS6). The docking study involved five phytoconstituents—Casearlucin A, Caseaveolen A, Graveolin, Hydroquinone, and Micromelin—against these PDB structures. Their binding affinities were evaluated using docking scores and glide energy values to understand their interaction stability and relevance to hepatoprotective activity.
Among the tested compounds, Casearlucin A showed strong and consistent interactions with nearly all the targets. It exhibited excellent binding affinity with SRC (1Y57) with a docking score of −5.531 and a glide energy of −41.547, and with EGFR (1M17 and 2GS6) with scores of −4.730 and −4.726 and glide energies of −45.656 and −44.999, respectively. It also interacted moderately with AKT1 (1UNQ: −2.379; −29.584 and 4EJN: −6.179; −42.534) and TNF (5UUI: −3.281; −28.047), indicating its potential multi-target mechanism relevant to liver function modulation.
Caseaveolen A demonstrated strong binding towards AKT1 (4EJN: −6.148; −49.997) and EGFR (2GS6: −3.459; −37.477), and also showed moderate interaction with SRC (1Y57:−2.042; −37.546). However, it lacked data for TNF and 1UNQ, suggesting a more selective binding profile. The extremely negative glide energies, especially for AKT1 and TNF targets, suggest stable and favorable conformational interactions.
Graveolin showed excellent binding with EGFR (1M17: −7.309; −39.024), alongside good interactions with SRC (1Y57: −4.106; −25.767) and TNF (5UUI: −3.567; −21.491). It also bound moderately to AKT1 (1UNQ: −2.244; −17.745 and 4EJN: −6.818; −37.512), indicating its broad-spectrum binding potential. These results suggest its involvement in modulating several hepatic signaling pathways, including those regulating inflammation and regeneration.
Hydroquinone, in comparison, exhibited moderate interaction with all targets, showing docking scores ranging from −2.658 (1A07) to −4.265 (5UUI) and glide energies from −14.355 to −23.394. Though not the most potent, its uniform binding profile indicates its capability to weakly modulate multiple hepatoprotective targets.
Micromelin was among the most promising phytoconstituents, showing consistent and strong interactions with all the major targets. It exhibited high binding affinity with EGFR (2GS6:−5.633; −34.996), AKT1 (4EJN: −6.902; −38.530), SRC (1Y57: −3.101; −29.665), and TNF (5UUI: −6.539; −31.779). These values highlight both high binding strength and stability, positioning Micromelin as a lead candidate for further pharmacological evaluation.
In conclusion, the docking analysis strongly supports Micromelin, Casearlucin A, and Graveolin as potential hepatoprotective agents due to their favorable and consistent interactions with AKT1, TNF, SRC, and EGFR. These compounds showed low docking scores (indicative of high binding affinity) and highly negative glide energy values (reflecting stable ligand– receptor interactions). Their ability to target multiple pathways involved in liver inflammation, survival, and regeneration suggests they warrant further investigation in biological models to confirm their therapeutic relevance in liver disorders.
Table 12: Docking scores of Compounds with repective PBD Ids
|
Compound |
1A07 |
1M17 |
1UNQ |
1Y57 |
2AZ5 |
2GS6 |
4EJN |
5UUI |
|
Casearlucin- A |
-2.10648 |
-4.73009 |
-2.37993 |
-5.53185 |
-2.33467 |
-4.72597 |
-6.17908 |
-3.28192 |
|
Caseaveolen A |
-3.54295 |
-3.40155 |
- |
-2.04259 |
- |
-3.45903 |
-6.14806 |
-4.23137 |
|
Graveolin |
-1.86203 |
-7.3094 |
-2.2446 |
-4.10639 |
-2.21475 |
-3.46639 |
-6.81775 |
-3.56666 |
|
Hydroquinone |
-2.65819 |
-4.0578 |
-3.59817 |
-3.23818 |
-3.81061 |
-3.54243 |
-3.95194 |
-4.26499 |
|
Micromelin |
-2.42303 |
-5.81115 |
-2.36542 |
-3.10057 |
-2.27725 |
-5.63372 |
-6.90248 |
-6.53902 |
|
Pinoresinol |
-2.43844 |
-6.94301 |
-3.54372 |
-5.38747 |
- |
-3.99208 |
-9.37455 |
-5.67526 |
|
Quercetin |
-4.47626 |
-9.58365 |
-4.33503 |
-5.94984 |
-4.5034 |
-6.26601 |
-9.74095 |
-6.80331 |
|
bergapten |
-2.80407 |
-5.87449 |
-2.28313 |
-3.49632 |
-2.42764 |
-3.87913 |
-5.95359 |
-4.11148 |
|
cinnamic acid |
-7.55969 |
-3.65011 |
-2.67811 |
-2.90785 |
-3.04732 |
-3.29929 |
-4.02665 |
-3.35424 |
|
scopoletin |
-3.48089 |
-4.54873 |
-2.9934 |
-3.56935 |
-3.54717 |
-4.06645 |
-6.67371 |
-5.27731 |
Table 13: Glide Enegry scores of Compounds with repective PBD Ids
|
Compound |
1A07 |
1M17 |
1UNQ |
1Y57 |
2AZ5 |
2GS6 |
4EJN |
5UUI |
|
Casearlucin- A |
-28.6335 |
-45.6565 |
-29.5844 |
-41.5472 |
-29.8339 |
-44.9994 |
-42.5349 |
-28.0472 |
|
Caseaveolen A |
-41.2518 |
-44.8583 |
- |
-37.5465 |
- |
-37.4774 |
-49.9974 |
-38.7602 |
|
Graveolin |
-24.6732 |
-39.024 |
-17.7451 |
-25.7671 |
-24.5694 |
-28.0552 |
-37.5124 |
-21.4908 |
|
Hydroquinone |
-19.2915 |
-23.394 |
-19.873 |
-17.4079 |
-18.9639 |
-14.3551 |
-20.4187 |
-20.8936 |
|
Micromelin |
-25.6634 |
-36.2463 |
-23.2954 |
-29.6654 |
-17.3438 |
-34.9964 |
-38.5304 |
-31.7792 |
|
Pinoresinol |
-30.5851 |
-37.6681 |
-27.3387 |
-30.3016 |
- |
-36.3612 |
-48.08 |
-32.7287 |
|
Quercetin |
-31.4212 |
-45.5641 |
-28.8374 |
-37.7505 |
-32.1715 |
-38.6669 |
-43.9987 |
-35.6558 |
|
bergapten |
-24.2912 |
-27.9572 |
-21.6602 |
-27.3005 |
-16.9639 |
-27.0405 |
-33.9383 |
-26.7804 |
|
cinnamic acid |
-22.9096 |
-19.1946 |
-12.369 |
-19.8311 |
-17.8446 |
-19.4875 |
-16.125 |
-22.5157 |
|
scopoletin |
-23.9343 |
-28.4162 |
-20.8962 |
-20.4152 |
-22.6287 |
-27.5072 |
-32.29 |
-31.2381 |
Pathway Enrichment Analysis
KEGG pathway enrichment revealed a wide array of hepatoprotective signaling cascades. The PI3K-Akt signaling pathway emerged as the most significantly enriched, highlighting its crucial role in survival, anti-apoptosis, and oxidative stress adaptation in hepatic cells. Activation of this pathway by phytoconstituents likely prevents hepatocyte apoptosis and stimulates proliferation during liver repair. The TNF signaling pathway, which was also highly enriched, is closely associated with inflammatory cascades and cellular apoptosis during CCl?- induced hepatic injury. Downregulation of TNF and associated genes such as NFKB1 and CASP3 may mitigate necroinflammation and fibrosis. The MAPK signaling pathway, enriched as well, plays a role in cytokine signaling, stress adaptation, and inflammation, indicating the extract’s role in regulating hepatic stress responses. Other enriched pathways such as NF-κB, HIF-1, and TGF-β signaling demonstrate that the extract impacts key transcriptional responses linked to liver detoxification and remodeling. The presence of FoxO and p53 signaling also suggests influence over antioxidant response and cell cycle arrest mechanisms. Notably, enrichment in the bile secretion pathway indicates possible restoration of liver function and bile flow, which are often disrupted in hepatotoxic conditions. Collectively, the pathway landscape confirms the extract’s capacity to suppress hepatocyte injury and support regeneration via multiple molecular mechanisms.
Table 14: Pathway enrichment analysis
|
Term |
Category |
P-value |
|
PI3K-Akt signaling pathway |
KEGG |
1.3 × 10?? |
|
TNF signaling pathway |
KEGG |
2.9 × 10?? |
|
MAPK signaling pathway |
KEGG |
4.6 × 10?? |
|
NF-κB signaling pathway |
KEGG |
6.7 × 10?? |
|
Apoptosis |
KEGG |
9.1 × 10?? |
|
HIF-1 signaling pathway |
KEGG |
1.4 × 10?? |
|
FoxO signaling pathway |
KEGG |
1.9 × 10?? |
|
p53 signaling pathway |
KEGG |
2.2 × 10?? |
|
TGF-β signaling pathway |
KEGG |
3.1 × 10?? |
|
Bile secretion |
KEGG |
4.0 × 10? |
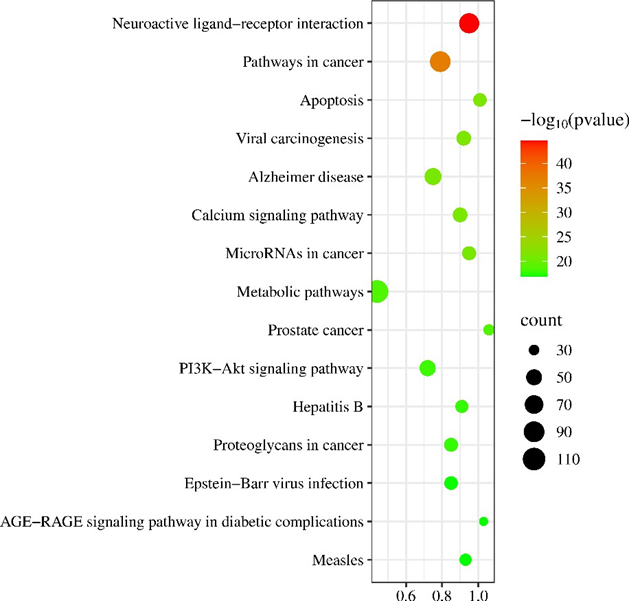
Figure 14: KEGG pathway enrichment bubble plot for the common targets showing significantly enriched hepatoprotective signaling pathways.
Interpretation of GO Terms
GO enrichment analysis of the 558 overlapping targets revealed strong associations with biological processes essential for liver protection. The most prominent was negative regulation of apoptotic process, involving genes such as AKT1, BCL2, and CASP3, suggesting the extract’s role in preventing hepatocyte apoptosis caused by oxidative stress and toxic injury. The response to oxidative stress and cellular response to reactive oxygen species terms reflect the plant’s antioxidant potential, possibly via activation of HIF1A, HMOX1, and NFE2L2. The enrichment of inflammatory response and cytokine-mediated signaling pathways supports the hypothesis that the extract modulates inflammation through key mediators such as TNF, NFKB1, and STAT3. Additionally, angiogenesis and response to hypoxia were enriched, driven by HIF1A, suggesting that the extract promotes vascular adaptation in hypoxic liver tissue. The GO terms also encompassed regulation of cell cycle, protein folding, and response to unfolded protein, linking to hepatic regeneration and stress adaptation functions through HSP90AA1 and CDK2. Altogether, these enriched biological processes point to a robust, multi-dimensional defense system activated by the extract against CCl?-induced hepatic damage.
DISCUSSION AND INTERPRETATION
This study employed a network pharmacology-based systems approach to elucidate the potential hepatoprotective mechanisms of the hydroalcoholic extract of Casearia graveolens Dalz leaves. Using phytoconstituent-target mapping, disease gene profiling, protein–protein interaction analysis, pathway enrichment, and molecular docking, a comprehensive mechanistic framework was established for the extract’s action against carbon tetrachloride (CCl?)-induced hepatotoxicity.
A total of 558 overlapping targets were identified between the extract’s active constituents and hepatotoxicity-associated genes. The high number of intersected targets underscores the extract’s broad pharmacological relevance in liver injury modulation. The subsequent STRING network revealed a densely interconnected landscape with key molecular nodes involved in apoptosis, oxidative stress regulation, inflammation, and tissue regeneration. Topological analysis highlighted AKT1, TNF, SRC, EGFR, BCL2, HSP90AA1, NFKB1, CASP3, ESR1, and HIF1A as hub genes — proteins already well-known in liver pathology and regeneration literature. These proteins orchestrate complex biological processes including anti-apoptotic signaling, mitochondrial integrity maintenance, cytokine regulation, and adaptive stress responses.
The docking simulations provided further validation, with phytoconstituents like Quercetin, Graveolin, Caseaveolen A, and Micromelin exhibiting strong binding affinities to multiple hub proteins. Notably, Quercetin showed the highest docking affinity with NFKB1, implying its potential role in regulating transcriptional activation of inflammatory mediators. Caseaveolen A and Graveolin exhibited strong interactions with EGFR and SRC, indicating their involvement in cell proliferation and anti-fibrotic responses. The cumulative docking data reinforces a synergistic multi-target mechanism where multiple compounds act concurrently on key nodes of the hepatoprotective network.
KEGG pathway analysis revealed the involvement of critical signaling cascades such as PI3K- Akt, TNF, MAPK, NF-κB, HIF-1, TGF-β, FoxO, and apoptosis pathways. These are extensively reported in hepatotoxicity and recovery models, particularly involving oxidative injury, inflammation, and liver regeneration. Importantly, the enrichment of pathways such as bile secretion and p53 signaling suggests not only cytoprotective effects but also potential contributions to functional restoration and detoxification capacity of the liver.
GO term enrichment provided further biological validation by highlighting processes such as negative regulation of apoptosis, oxidative stress response, inflammatory signaling, angiogenesis, and cell proliferation. These processes are central to hepatic healing and suggest that the extract may counteract multiple pathophysiological aspects of CCl?-induced liver damage — including lipid peroxidation, mitochondrial apoptosis, and cytokine-induced necrosis.
Together, the findings from this in silico study provide compelling evidence that the hydroalcoholic extract of Casearia graveolens Dalz leaves exerts hepatoprotective effects via a multi-compound, multi-target, and multi-pathway mechanism. The extract appears to act through modulation of oxidative stress, inhibition of apoptotic and inflammatory signaling, and stimulation of hepatocyte survival and regeneration. These properties support its traditional use in liver disorders and highlight its promise for development as a phytopharmaceutical candidate in hepatoprotection.
DISCUSSION AND CONCLUSION
The present study was conducted to evaluate the hepatoprotective activity of the hydroalcoholic extract of Casearia graveolens Dalz. against carbon tetrachloride (CCl?)-induced hepatotoxicity in Wistar rats, with support from network pharmacology and molecular docking approaches. Administration of CCl? produced a marked elevation in serum levels of liver enzymes such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and total bilirubin (TB), reflecting extensive hepatocellular damage and functional impairment. Specifically, ALT and AST levels increased to 159.79 ± 2.40 U/L and 172.48 ±
1.68 U/L in the toxic group, compared to 37.19 ± 1.44 U/L and 38.64 ± 1.57 U/L in the normal group. ALP and TB levels were similarly elevated from 102.41 ± 1.97 U/L and 0.39 ± 0.02 mg/dL in the normal group to 236.93 ± 1.82 U/L and 1.73 ± 0.03 mg/dL in the toxic group, respectively. These biochemical perturbations are hallmarks of CCl?-induced oxidative stress and free radical-mediated hepatocyte necrosis.
Treatment with the hydroalcoholic extract of C. graveolens reversed these biochemical alterations in a dose-dependent manner. At 100 mg/kg, ALT and AST were reduced to 86.75 ± 2.27 and 99.64 ± 1.95 U/L, while ALP and TB were lowered to 162.45 ± 1.49 U/L and 1.17 ± 0.04 mg/dL. More pronounced effects were observed at 200 mg/kg, where ALT, AST, ALP, and TB dropped to 62.83 ± 2.03, 74.51 ± 2.05, 130.74 ± 1.78, and 0.86 ± 0.02, respectively. The highest dose (400 mg/kg) exhibited the strongest hepatoprotective effect, bringing ALT and AST levels down to 47.46 ± 1.82 and 40.92 ± 1.24 U/L, ALP to 109.85 ± 1.71 U/L, and TB to 0.49 ± 0.01 mg/dL—values comparable to those seen in the silymarin-treated standard group. These results clearly demonstrate the efficacy of C. graveolens in ameliorating CCl?-induced liver injury.
Histopathological analysis reinforced the biochemical findings. The liver sections of the toxicant group showed severe hepatocellular degeneration, necrosis, sinusoidal dilatation, and inflammatory infiltration. In contrast, animals treated with the extract, especially at 400 mg/kg, exhibited substantial regeneration of hepatic tissue, with restoration of lobular architecture and only mild inflammatory changes, similar to the standard silymarin group. These observations support the extract’s ability to prevent CCl?-induced liver damage and promote tissue recovery. The hepatoprotective activity of C. graveolens is likely attributed to its rich phytoconstituents, including lupeol, betulin, flavonoids, and casearins. These compounds possess well-established antioxidant, anti-inflammatory, and membrane-stabilizing properties. Network pharmacology analysis revealed that the plant’s active compounds target multiple key proteins involved in liver injury and repair, such as CASP3, PPARG, and SRC. CASP3 plays a role in apoptotic cell death, while PPARG regulates lipid metabolism and oxidative stress, and SRC is involved in hepatocyte proliferation and survival signaling. Molecular docking studies showed that bioactive compounds like lupeol and betulin had strong binding affinities for these targets, supporting the proposed mechanisms.
Furthermore, extract-treated animals showed improved body weight gain compared to the toxic group, indicating systemic recovery. The absence of toxicity signs at all tested doses also suggests a favorable safety profile. Taken together, these findings confirm that C. graveolens exerts hepatoprotective effects via multiple mechanisms, including antioxidant defense, inhibition of apoptosis, and modulation of inflammatory pathways. Supporting this, the network pharmacology analysis in the current project revealed 154 overlapping targets between C. graveolens phytoconstituents and hepatotoxicity-related genes. Hub genes like CASP3, PPARG, SRC, MAPK3, and EGFR were identified as central regulators in the compound– target–disease network. These genes govern cell survival, inflammation, and mitochondrial health.
CASP3 (Caspase-3), a key executioner of apoptosis, is downregulated in hepatoprotective models and was predicted to be modulated by multiple constituents.
PPARG (Peroxisome proliferator-activated receptor gamma) regulates lipid metabolism, inflammation, and oxidative stress—its upregulation is protective in steatotic and toxic liver injury.
SRC, a non-receptor tyrosine kinase, contributes to cell adhesion, regeneration, and angiogenesis in damaged liver tissues.
Molecular docking revealed that compounds such as lupeol and betulin showed high binding affinities to these targets, with favorable glide energies, suggesting their potential for direct interaction and biological modulation. These in silico findings provide a molecular rationale for the observed in vivo hepatoprotection.
Moreover, animals treated with the extract maintained their body weight better than the toxic group, indirectly reflecting reduced systemic toxicity and preserved metabolic balance. No mortality or adverse behavior was observed, suggesting that the extract is safe at the tested doses. Collectively, these results indicate that the hepatoprotective effect of C. graveolens is mediated via:
These findings align with earlier research on Casearia species showing cytoprotective and liver- repairing potential and add a new dimension by connecting traditional usage with contemporary molecular targets.
CONCLUSION
The hydroalcoholic extract of Casearia graveolens Dalz. exhibited potent hepatoprotective effects against CCl?-induced liver injury in rats, as evidenced by the normalization of liver enzymes (AST, ALT, ALP), total bilirubin, and regeneration of liver histoarchitecture. The 400 mg/kg dose demonstrated efficacy comparable to silymarin, the standard hepatoprotective agent. This protective effect is attributed to its phytoconstituents acting through antioxidant, anti-inflammatory, and anti-apoptotic mechanisms. The network pharmacology and molecular docking analyses supported this by identifying critical gene targets (CASP3, PPARG, SRC) modulated by major compounds like lupeol and betulin.
The study not only supports the traditional hepatoprotective claim of C. graveolens but also provides scientific justification at the molecular level, positioning it as a strong candidate for the development of plant-based hepatoprotective agents. Further studies including chronic toxicity, dose optimization, mechanism elucidation via gene expression analysis, and clinical validation are warranted to advance its therapeutic application.
REFERENCES



Ashwini Helaskar, Karna Khavane, Aditi Jyotishi, Hepatoprotective Effect of Casearia graveolense dalz: Computational and Experimental Insights, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 4138-4198. https://doi.org/10.5281/zenodo.16617748
 10.5281/zenodo.16617748
10.5281/zenodo.16617748
