Malla Reddy College of Pharmacy, Maisammaguda, Hyderabad, Telangana, India 500100
Status epilepticus (SE) is a neurological emergency requiring prompt intervention. While multiple benzodiazepines are used for acute management, intravenous (IV) lorazepam and midazolam remain common first-line agents. However, existing literature has largely focused on pediatric populations, intramuscular routes, or comparisons involving alternative drugs such as diazepam. There is a paucity of evidence directly comparing IV lorazepam and midazolam in adults, especially in the context of regional lifestyle and etiological influences. To compare the efficacy of IV lorazepam and IV midazolam in terminating seizures in adults and assess recurrence rates, duration of therapy, and dose patterns, while evaluating contributing etiological and lifestyle factors. This retrospective observational study was conducted involving 500 adult patients presenting with convulsive seizures. Patients were categorized based on treatment received—either IV Lorazepam (4mg) or IV Midazolam (2mg). Data regarding demographics, social habits (alcohol/tobacco use), seizure etiology (e.g., alcohol withdrawal, panic attacks, metabolic causes), dose-response, recurrence, and therapy duration were collected. Statistical analysis included the chi-square test for significance. Among 500 patients, alcohol withdrawal and psychiatric-related episodes were predominant etiological factors, often linked to lifestyle habits. Lorazepam showed greater effectiveness in seizure control, with fewer recurrences and shorter treatment duration compared to midazolam. The chi-square analysis showed significant differences in recurrence and treatment outcomes. Levetiracetam was the most commonly prescribed antiepileptic, used in 90% of patients. This study emphasizes the clinical superiority of IV lorazepam over midazolam in adult seizure emergencies. The findings emphasize the importance of local studies that consider lifestyle and etiological factors, which significantly influence seizure patterns and treatment response. Such region-specific data help bridge the knowledge gap, supporting the development of globally informed yet locally precise treatment guidelines.
The word "seizure" originates from the Latin word meaning 'to take possession of' and describes a sudden event triggered by unusually high or synchronized neural activity in the brain(1). It lasts for less than 5 minutes. Seizures that persist for over half an hour are referred to as status epilepticus (SE), which represents a frequent emergency that requires immediate intervention. The rates of complications and death linked to status epilepticus are affected by its causes and the treatment provided(2). The factors contributing to this condition encompass brain metastases, strokes, subdural hematomas, intracranial and spinal (CNS) infections, degenerative diseases such as Alzheimer's disease, psychiatric disorders, and cancers including malignant gliomas. Additionally, systemic metabolic disorders - alcohol withdrawal, uremia, hypoglycaemia, hyperglycaemia, and hyponatraemia may also lead to these issues(3)(4). Various agents with distinct pharmacokinetic characteristics—such as lorazepam, midazolam, and diazepam—are utilized for managing seizures(5).
Although lorazepam and midazolam are both widely prescribed for the initial treatment of seizures, particularly in status epilepticus, proper comparative studies assessing their intravenous efficacy remain limited. Most available literature supports their individual use but lacks structured, head-to-head evaluations under uniform clinical conditions. This gap restricts clarity in optimal drug selection during acute episodes. Additionally, preventive strategies for recurrent seizures often differ from acute interventions. Understanding seizure patterns based on etiological factors is also critical for guiding both acute and long-term management. Given variations in patient profiles, clinical practices, and healthcare delivery in different regions, there is a clear need for locally relevant data to support evidence-based treatment decisions. Hence, this study was undertaken to compare the intravenous efficacy of midazolam and lorazepam in seizure cessation, identify seizure patterns based on underlying etiologies, and explore preventive options for managing recurrent episodes.
METHODS AND MATERIALS
This study, designed as a prospective observational investigation, was conducted over a duration of six months in the Department of General Medicine at Malla Reddy Hospital. A total of 500 patients who were admitted with different types of seizures were selected for the study based on well-defined inclusion and exclusion parameters. Ethical approval was obtained from the Institutional Ethics Committee (IEC), and informed consent was acquired from each participant using a standardized consent form before enrolment.
Inclusion Criteria
Participants included male and female patients aged between 20 and 80 years who were admitted with various seizure types to the Department of General Medicine. Patients with a history of alcohol use were also included.
Exclusion Criteria
Patients who were below 20 years of age, pregnant or lactating, unable to provide informed consent, or unwilling to participate in the study were excluded.
Data Collection
A structured patient profile form was used to collect information on demographics, clinical history, type of seizure, treatment provided, and therapeutic outcomes. Based on the treating physician’s discretion, patients received either 2 mg of intravenous midazolam or 4 mg of lorazepam. The effectiveness of treatment, seizure cessation, and any recurrence were closely monitored during the hospital stay.
Statistical Analysis
Data analysis was performed using the chi-square test in Microsoft Excel to compare the recurrence of seizures and duration of therapy between the midazolam and lorazepam groups. The chi-square statistic was computed using the formula: χ² = ∑ ((Oi − Ei)² / Ei), where Oi represents the observed frequency and Ei the expected frequency. The degrees of freedom were calculated using the formula: (rows − 1) × (columns − 1).
RESULTS
A total of 500 participants were enrolled in our study, which was conducted in the Department of General Medicine at Malla Reddy Hospital over a period of six months.
Age
The age distribution revealed that the majority of patients (36%) were between 20–29 years, and 22.6% in the 30–39 years age group. The remaining subjects were distributed as follows: 40–49 years (18.4%), 50–59 years (11.8%), 60–69 years (5.2%), and 70–78 years (6%).
Gender and Social Habits
280 patients (56%) were male, and 220 (44%) were female. Analysis of social habits indicated that 23.4% of patients consumed alcohol, 1.6% were smokers, and 2.2% had a history of substance abuse. Additionally, 14.2% reported both alcohol consumption and smoking, and 3% reported alcohol consumption along with substance abuse. A significant portion, 55.6%, reported no social habits.
Table 1: Distribution of Demographic Characteristics, Social Habits (N = 500)
|
|
FREQUENCY |
RATIO % |
|
Age (in Years) |
|
|
|
20 - 29 |
180 |
36 |
|
30 - 39 |
113 |
22.6 |
|
40 - 49 |
92 |
18.4 |
|
50 - 59 |
59 |
11.8 |
|
60 - 69 |
26 |
5.2 |
|
70 - 78 |
30 |
6 |
|
Total |
500 |
100 |
|
Gender |
|
|
|
Male |
280 |
56 |
|
Female |
220 |
44 |
|
Total |
500 |
100 |
|
Social Habits |
|
|
|
Alcohol |
117 |
23.4 |
|
Smoking |
8 |
1.6 |
|
Substance abuse* |
11 |
2.2 |
|
Alcohol, smoking |
71 |
14.2 |
|
Alcohol, substance abuse |
15 |
3 |
|
No habits |
278 |
55.6 |
|
Total |
500 |
100 |
History and frequency of Seizures
When evaluating past seizure occurrence, 196 patients (39.2%) reported previous episodes, whereas 304 (60.8%) had no prior history. Among those with past history, 9.4% had seizures less than one year, 6.4% had a history of seizures for exactly one year, and 17% had a history extending beyond one year. Notably, 6.4% reported congenitally acquired seizures (Figure - 1,2).
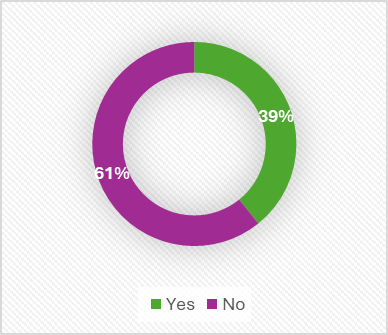
Figure – 1: Distribution of participants based on their history of seizures (N=500)
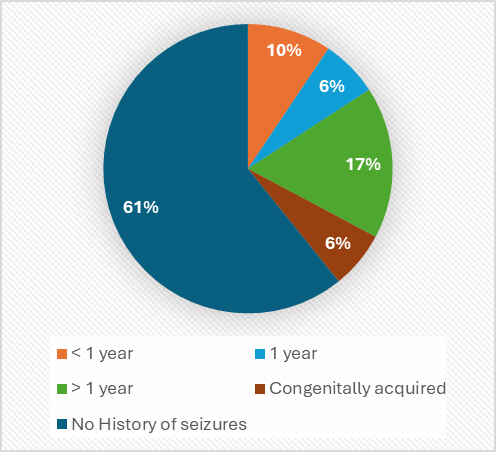
Figure – 2: Distribution of participants based on frequency of seizures (N=500)
Etiology
The most common cause identified was alcohol withdrawal (28%), followed by unknown compound poisoning (7.6%), panic attacks (6.8%), brain infections and hypoglycemia (6% each), and others (burns, fractures, etc.) at 6.2%. Less frequent causes included gliosis and serum electrolyte imbalances (4.8%), ischemic stroke (4%), head injury (4.6%), and a small number involving combination factors (1.2%). Other etiologies included brain tumors, congenital causes, depression, trauma, and insomnia (Figure - 3).
Table – 2: Distribution of participants based on Etiological factors
|
Etiological Factor |
Frequency |
Ratio % |
|
Alcohol withdrawal |
140 |
28 |
|
Brain infection |
30 |
6 |
|
Brain tumour |
13 |
2.6 |
|
Congenital |
29 |
5.8 |
|
Depression |
11 |
2.2 |
|
Gliosis |
24 |
4.8 |
|
Head injury |
23 |
4.6 |
|
Haemorrhagic stroke |
14 |
2.8 |
|
Hypoglycaemia |
30 |
6 |
|
Insomnia |
14 |
2.8 |
|
Ischemic stroke |
20 |
4 |
|
Panic attack |
34 |
6.8 |
|
Trauma |
19 |
3.8 |
|
Unknown compound poisoning |
38 |
7.6 |
|
Serum electrolyte imbalances |
24 |
4.8 |
|
Others (burns, fractures, etc) |
31 |
6.2 |
|
Combination** |
6 |
1.2 |
|
Total |
500 |
100 |
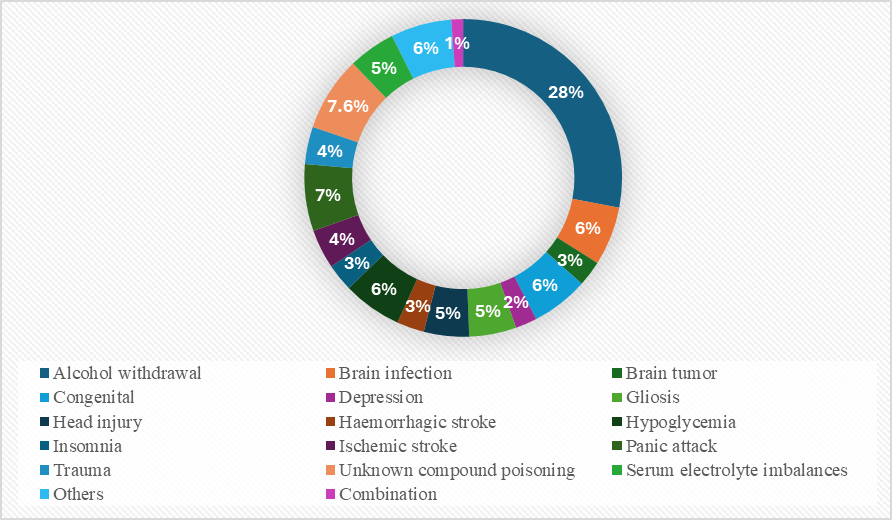
Figure – 3: Distribution of participants based on Etiological factors (N=500)
Choice of Benzodiazepine
Among the 500 subjects, 250 (50%) received Midazolam (2 mg) and 250 (50%) were administered with Lorazepam (4 mg). In the Midazolam group, 130 were males (46.49%) and 120 females (54.55%). In the Lorazepam group, 150 were males (53.51%) and 100 females (45.45%). There was a slightly greater representation of males in the Lorazepam group, whereas females were more prevalent in the Midazolam group.
Table – 3: Distribution of Benzodiazepine Choice by Gender
|
Choice of Benzodiazepine |
Male |
Female |
Total |
Ratio% |
|
Midazolam (2 mg) |
130 (46.49) |
120 (54.55) |
250 |
50 |
|
Lorazepam (4 mg) |
150 (53.51) |
100 (45.45) |
250 |
50 |
|
Total |
280 (100.0) |
220 (100.0) |
500 |
100 |
Recurrence following administration of IV Midazolam (2 mg)
Out of the 250 participants, 187 (74.8%) exhibited recurrence of seizure episodes, whereas 63 (25.2%) of them did not experience any recurrence.
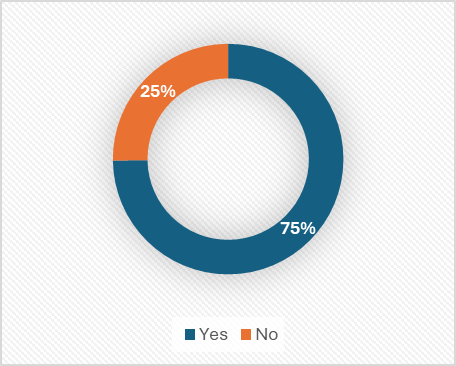
Figure – 4: Seizure Recurrence Among Patients Treated with IV Midazolam (2 mg)
Recurrence following administration of IV Lorazepam (4 mg)
Among the 250 patients treated with IV Lorazepam (4 mg), seizure recurrence was observed in 178 individuals, accounting for 71.2%, while 28.8% (72 patients) did not experience a recurrence.
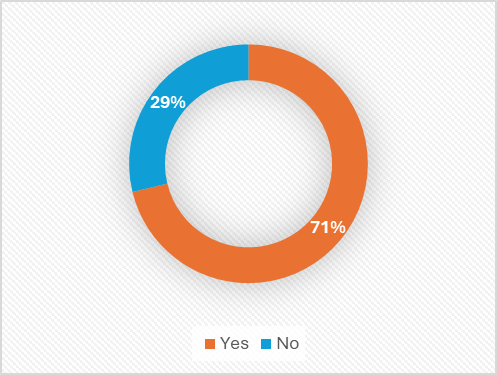
Figure – 5: Seizure Recurrence Among Patients Treated with IV Lorazepam (4 mg)
Although both benzodiazepines showed high recurrence rates, Midazolam was associated with a marginally greater recurrence, suggesting a potential difference in efficacy.
Duration of therapy - Midazolam (Intravenous, 2mg)
Table – 4: Initial Response Post-Control Dose Requirements with IV Midazolam (2 mg)
|
Duration of Therapy (Midazolam) |
No. of cases (Midazolam, IV, 2 mg) |
Ratio % (n=250) |
|
SE* |
63 |
25.2 |
|
SE, 1 dose |
30 |
12 |
|
SE, 2 doses |
37 |
14.8 |
|
SE, 3 doses |
46 |
18.4 |
|
SE, 4 doses |
27 |
10.8 |
|
SE, 5 doses |
25 |
10 |
|
SE, 6 doses |
9 |
3.6 |
|
SE, 7 doses |
13 |
5.2 |
|
Total |
250 |
100 |
*SE – Status epilepticus, SE followed by ‘x’ doses refers to the additional doses administered to manage recurrent episodes after the initial treatment of status epilepticus.
After successful control of status epilepticus (SE) with IV Midazolam at a dose of 2 mg, 63 patients (25.2%) required no further dosing, indicating complete stabilization. However, 187 patients (74.8%) required one or more additional doses to manage subsequent seizure activity. Notably, 30 patients (12%) needed a single extra dose, while a larger proportion, 157 patients (62.8%), required two or more additional doses—including cases where up to seven doses were administered post-initial control.
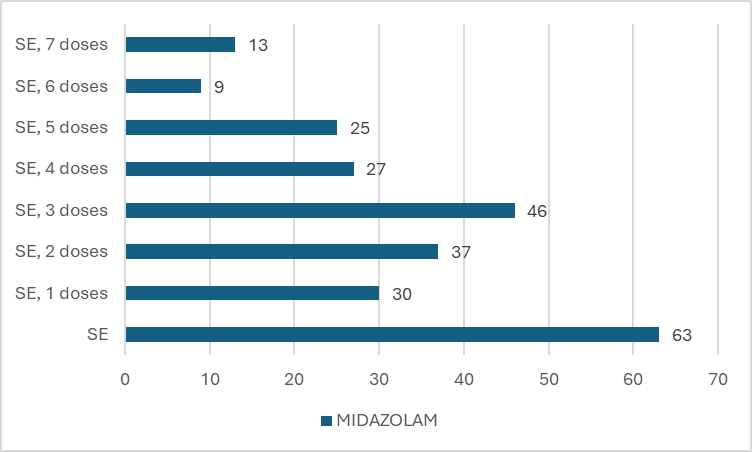
Figure – 6: Initial Response & Post-Control Dose Requirements with IV Midazolam (2mg)
Duration of therapy - Lorazepam (Intravenous, 4mg)
Table – 5: Initial Response and Post-Control Dose Requirements with IV Lorazepam (4 mg)
|
Duration of Therapy (Lorazepam) |
No. of cases (Lorazepam, IV, 4mg) |
Ratio % (n=250) |
|
SE |
72 |
28.8 |
|
SE, 1 dose |
53 |
21.2 |
|
SE, 2 doses |
47 |
18.8 |
|
SE, 3 doses |
38 |
15.2 |
|
SE, 4 doses |
16 |
6.4 |
|
SE, 5 doses |
13 |
5.2 |
|
SE, 6 doses |
5 |
2 |
|
SE, 7 doses |
6 |
2.4 |
|
Total |
250 |
100 |
Among 250 cases treated with IV Lorazepam (4 mg), 28.8% achieved stability without requiring repeated doses. Seizure control with one, two, and three additional doses was observed in 21.2%, 18.8%, and 15.2% of cases, respectively. A smaller proportion required four to seven additional doses (6.4%, 5.2%, 2%, and 2.4%, respectively), indicating that the majority responded within the first three doses, suggesting effective stabilization in most patients with limited recurrence.
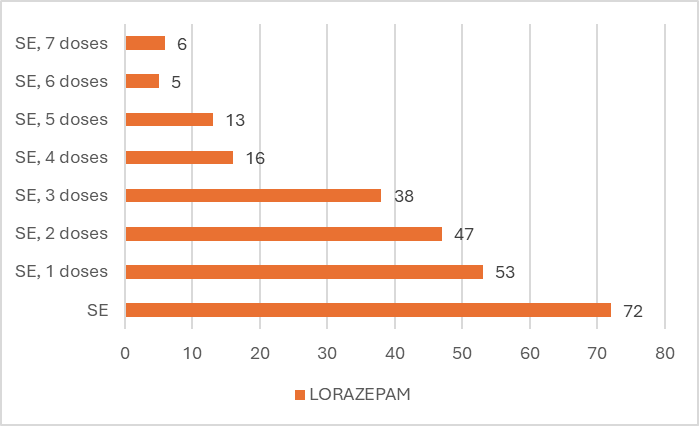
Figure – 7: Initial Response and Post-Control Dose Requirements with IV Lorazepam (4 mg)
The marked decrease in subjects requiring additional doses of Lorazepam compared to Midazolam indicates that Lorazepam exerts a quicker and more sustained therapeutic effect, thereby reducing the need for repeated dosing to achieve seizure control.
CHI-SQUARE TEST
Hypotheses:
Calculation:
Ei or Eij? = Ri?×Cj??/N
Where, Eij?: Expected frequency for a given cell (i.e., category or group).
Ri?: Row total (sum of observed frequencies in a category).
Cj?: Column total (sum of observed frequencies for a group).
N: Grand total (sum of all observed frequencies).
Table – 6: Comparison of Duration of Therapy and Dose Frequencies Between Midazolam (2 mg IV) and Lorazepam (4 mg IV) in Seizure Episodes (N = 500)
|
Duration of therapy |
|
Midazolam (IV, 2mg) |
Lorazepam (IV, 4mg) |
Row total (Ri) |
|
SE |
Oi |
63 |
72 |
135 |
|
Ei |
67.5 |
67.5 |
||
|
SE, 1 doses |
Oi |
30 |
53 |
83 |
|
Ei |
41.5 |
41.5 |
||
|
SE, 2 doses |
Oi |
37 |
47 |
84 |
|
Ei |
42 |
42 |
||
|
SE, 3 doses |
Oi |
46 |
38 |
84 |
|
Ei |
42 |
42 |
||
|
SE, 4 doses |
Oi |
27 |
16 |
43 |
|
Ei |
21.5 |
21.5 |
||
|
SE, 5 doses |
Oi |
25 |
13 |
38 |
|
Ei |
19 |
19 |
||
|
SE, 6 doses |
Oi |
9 |
5 |
14 |
|
Ei |
7 |
7 |
||
|
SE, 7 doses |
Oi |
13 |
6 |
19 |
|
Ei |
9.5 |
9.5 |
||
|
Column total (Cj) |
|
250 |
250 |
500 (N) |
*SE – Status epilepticus, SE followed by ‘x’ doses refers to the additional doses administered to manage recurrent episodes after the initial treatment of status epilepticus. Where, Oi and Ei indicate Observed and Expected values respectively.
2) In the next step, Chi-square values (χ2) were calculated for both the drugs at each dose given to treat SE and recurrent episodes, by using the following formula –
χ2 = (Oi−Ei)2/Ei
where, i indicates position of a value
χ2Midazolam or χ2Lorazepam =∑ χ2i (at each cell)
Table – 7: Chi-Square Analysis of Duration of Therapy for Midazolam (2 mg IV) in Seizure Episodes (n = 250)
|
Duration of therapy (Midazolam) |
Oi |
Ei |
? χ2i |
|
SE |
63 |
67.5 |
0.3 |
|
SE, 1 dose |
30 |
41.5 |
3.1867 |
|
SE, 2 doses |
37 |
42 |
0.5952 |
|
SE, 3 doses |
46 |
42 |
0.381 |
|
SE, 4 doses |
27 |
21.5 |
1.407 |
|
SE, 5 doses |
25 |
19 |
1.8947 |
|
SE, 6 doses |
9 |
7 |
0.5714 |
|
SE, 7 doses |
13 |
9.5 |
1.2895 |
|
|
|
χ2Midazolam = 9.6255 |
|
*SE – Status epilepticus, SE followed by ‘x’ doses refers to the additional doses administered to manage recurrent episodes after the initial treatment of status epilepticus.
Table – 8: Chi-Square Analysis of Duration of Therapy for Lorazepam (4 mg IV) in Seizure Episodes (n = 250)
|
Duration of therapy (Lorazepam) |
Oi |
Ei |
χ2i |
|
SE |
72 |
67.5 |
0.3 |
|
SE, 1 doses |
53 |
41.5 |
3.1867 |
|
SE, 2 doses |
47 |
42 |
0.5952 |
|
SE, 3 doses |
38 |
42 |
0.381 |
|
SE, 4 doses |
16 |
21.5 |
1.407 |
|
SE, 5 doses |
13 |
19 |
1.8947 |
|
SE, 6 doses |
5 |
7 |
0.5714 |
|
SE, 7 doses |
6 |
9.5 |
1.2895 |
|
|
|
χ2Lorazepam = 9.6255 |
|
*SE – Status epilepticus, SE followed by ‘x’ doses refers to the additional doses administered to manage recurrent episodes after the initial treatment of status epilepticus.
? χ2total or χ2calculated = χ2Midazolam ?+ ? χ2Lorazepam
= 9.6255 + 9.6255
χ2total or χ2calculated = 19.251
Df = (number of rows−1) × (number of columns−1)
= (8-1) x (2-1)
= 7 x 1
Df = 7
At Df = 7 and p = 0.05, χ2critical is 14.067.
Finally, χ2calculated ?> χ2critical i.e., 19.251 > 14.067
This indicates that the Null hypothesis (H0) is rejected showing a significant difference in the efficacy distribution between IV Midazolam and IV Lorazepam (χ2calculated ?> χ2critical i.e., 19.251 > 14.067). This supports the alternate hypothesis (Ha?), indicating that the two treatments exhibit distinct distributions across the observed categories i.e., they have a significant difference.
In conclusion, the findings from the chi-square analysis and therapy duration evaluation highlight the superior efficacy of lorazepam over midazolam as evidenced by its requirement for fewer doses to achieve seizure control regardless of the seizure etiology.
Preventive anti-epileptic therapy
Table – 9: Preventive treatment options for seizures
|
Preventive therapy |
Frequency |
Ratio % |
|
Levetiracetam (LevipilBrand) |
450 |
90 |
|
Phenytoin |
37 |
7.4 |
|
Valproate |
13 |
2.6 |
|
Total |
500 |
100 |
Among the 500 patients evaluated for preventive antiepileptic therapy, Levetiracetam (Levipil) was the most commonly administered agent, used in 450 cases (90%). Phenytoin was given to 37 patients (7.4%), while Valproate was used in only 13 cases (2.6%). This data indicates a strong preference for Levetiracetam as the primary choice for seizure prophylaxis, likely due to its favourable seizure stabilization profile and ease of use compared to older antiepileptics.
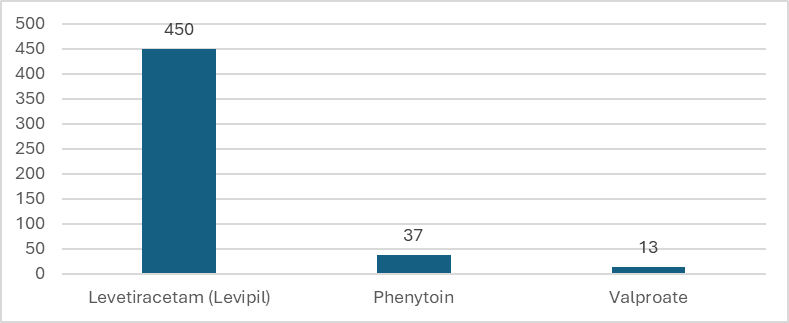
Figure – 8: Distribution of Preventive Antiepileptic Therapy Among Patients (N = 500)
DISCUSSION
This study was conducted as a comparative clinical evaluation to determine the relative efficacy of Midazolam (2 mg IV) and Lorazepam (4 mg IV) in the acute management of seizures. It focused on three critical parameters: dose requirement, duration of therapy, and the pattern of preventive antiepileptic usage. Our data included patients with a wide range of seizure etiologies, thereby strengthening the practical relevance and generalizability of the findings within local clinical settings. In this study, we included nearly all major etiological categories to ensure a comprehensive evaluation of drug efficacy across diverse clinical presentations. Such an approach not only enhanced the representativeness of the study population but also increased the precision of drug selection based on real-world, local healthcare trends. Common factors included alcohol withdrawal, panic attack, unknown compound poisoning, congenitally acquired, burns, fractures, etc — all of which were significantly associated with seizure recurrence and intensity. Importantly, these behavioral factors often influenced the need for repeat dosing and long-term antiepileptic planning.
The results indicated that Lorazepam had greater clinical efficacy in terminating seizures at initial dosing. Specifically, seizure control was achieved in 53 patients with the first dose of Lorazepam, compared to 30 patients in the Midazolam group. This finding supports existing pharmacological evidence that Lorazepam, owing to its higher lipid solubility and longer CNS half-life, provides a more sustained anticonvulsant effect. The chi-square analysis (χ² = 19.251) demonstrated a statistically significant difference in dose distribution patterns between the two groups (p < 0.05), highlighting the superiority of Lorazepam in emergency seizure management. Although Midazolam did show moderate effectiveness when administered in higher doses or repeated schedules, Lorazepam provided faster and more reliable seizure control with fewer interventions. This has important implications for emergency protocols, especially in resource-limited settings where rapid seizure termination is crucial.
The local nature of this study played a critical role in enhancing the clinical applicability of the findings. Our localized data allows for greater accuracy in protocol design and drug prioritization for specific population groups. This supports the need for region-specific studies in developing targeted treatment strategies. While pediatric studies like the PECARN trial (IV lorazepam vs IV diazepam) and network meta-analyses have compared benzodiazepines in children[6], they did not evaluate IV lorazepam vs IV midazolam in adult cohorts. The RAMPART trial compared IM midazolam to IV lorazepam and focused on a mixed population, demonstrating noninferiority of intramuscular midazolam in prehospital settings[7]—but not clarifying fixed IV adult dose comparisons. Thus, our study fills an important gap of the lack of adult-focused study to date compares the IV forms of midazolam and lorazepam directly across diverse etiologies.
Regarding long-term seizure prevention, Levetiracetam emerged as the most frequently prescribed antiepileptic, used in 90% of patients. This trend reflects its favorable tolerability profile. In contrast, traditional agents like Phenytoin and Valproate were used less frequently (7.4% and 2.6%, respectively), indicating a clinical shift toward newer-generation antiepileptics.
CONCLUSION
This study demonstrates that IV Lorazepam offers superior seizure control with fewer doses compared to IV Midazolam, especially in adult patients whose seizures are influenced by social habits such as alcohol use and panic-induced triggers. Early identification of etiological and behavioral contributors is essential for preventing recurrence. Levetiracetam emerged as the preferred agent for post-stabilization prophylaxis, supporting its clinical superiority over phenytoin and valproate in routine practice. Importantly, this research fills a critical knowledge gap by providing evidence-based comparison of IV Lorazepam vs IV Midazolam in adults, an area previously unexplored in literature that largely focuses on drug comparisons between other drugs especially in pediatric groups and between alternate administration routes. Local and regional studies such as this are vital in facilitating globally informed yet context-sensitive therapeutic guidelines, enhancing treatment precision and patient outcomes.
REFERENCES





Shravani Gandla, Pamu Varalaxmi, Mohammad Ghouse, Apoorva Kankanala, Tejaswi Vummarao, M. Satya Pratik, Comparative Study of Midazolam and Lorazepam Efficacy at Tertiary Care Hospital, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 4313-4324. https://doi.org/10.5281/zenodo.16633299
 10.5281/zenodo.16633299
10.5281/zenodo.16633299
