Shri Sarvajanik Pharmacy College, Near Arvind Baug, Mehsana-384001, Gujarat, India.
Floating drug delivery systems have garnered significant attention in recent decades as a potential solution to overcome the limitations of traditional drug delivery systems, such as frequent dosing and limited bioavailability. An ideal floating system remains in the stomach for an extended period, releasing the active medication continuously and maintaining its pharmacological effects. This review aims to consolidate recent research on gastroretentive and floating tablets, highlighting their principles, advantages, classification, preparation, and evaluation methods. Additionally, it provides an overview of marketed floating tablets and explores the formulation and evaluation aspects of effervescent floating drug delivery systems. The review also discusses factors influencing gastric retention and offers insights into the pharmaceutical formulation of these systems, providing a comprehensive understanding of this promising drug delivery approach.
The oral route has become increasingly popular for delivering therapeutic agents due to its simplicity and high patient compliance, making it a preferred choice for pharmaceutical companies and patients alike. Gastro-retentive drug delivery systems are designed to remain in the stomach for an extended period, enhancing the bioavailability of drugs absorbed in the upper gastrointestinal tract, such as antibiotics, antifungal agents, and anti-diabetic drugs. These systems offer several benefits, including improved bioavailability, reduced drug waste, and enhanced solubility for drugs poorly soluble in high pH environments, thereby reducing the frequency of dosing and associated side effects. They also enable localized delivery to the stomach and proximal small intestine, making them suitable for treating various diseases, including gastric ulcers, gastro-esophageal reflux disease (GERD), and Helicobacter pylori infections.
Moreover, gastro-retentive systems can be tailored to release drugs in a controlled manner, maintaining optimal drug concentrations and minimizing fluctuations, which can lead to improved therapeutic outcomes and patient compliance. Various approaches, such as hydrodynamically balanced systems, floating drug delivery systems, raft systems, bioadhesive systems, superporous hydrogels, and magnetic systems, have been explored to achieve prolonged gastric retention. These systems have been evaluated in vitro and in vivo to assess their efficacy and potential applications, with some formulations showing promising results in clinical trials. Overall, gastro-retentive drug delivery systems hold great promise for improving the treatment of various diseases and disorders, and ongoing research is focused on developing more efficient and effective systems.
Physiology of the stomach3
The stomach is anatomically divided into three regions: the fundus, body, and antrum (pylorus). The fundus and body act as a reservoir for undigested food, while the antrum is responsible for mixing and propelling food into the small intestine through its pumping actions. Gastric emptying occurs in both fasting and fed states, with distinct motility patterns. During fasting, the interdigestive myloelectric cycle (MMC) takes place, cycling through the stomach and intestine every 2-3 hours. The MMC consists of four phases, as described by Wilson and Washington, which regulate the movement of food through the digestive system.
After a meal, gastric motility shifts from a fasted to a fed state, characterized by continuous contractions that break down food particles into smaller sizes (<1 mm) and propel them towards the pylorus. This digestive motility pattern delays the onset of the migrating myoelectric cycle (MMC), resulting in a slower gastric emptying rate. However, orally administered controlled-release dosage forms are subject to two major complications: short gastric residence time and unpredictable gastric emptying rate, which can impact their efficacy. Understanding these physiological processes is crucial for designing effective gastroretentive drug delivery systems.
Strategies for Gastroretention3-4
Various approaches have been explored to prolong gastric retention, including mucoadhesive systems, high-density systems, modified-shape systems, floating dosage forms (gas-generating and swelling/expanding systems), and co-administration of gastric emptying delaying agents. These strategies aim to extend the retention of medication in the stomach, improving bioavailability and efficacy. However, the success of these approaches depends on several factors that influence the gastroretentive mechanism.
Density: Buoyancy-dependent, influencing dosage form retention.
Size: Larger dosage forms (>7.5 mm) exhibit longer GRT.
Shape: Tetrahedron and ring-shaped devices show better GRT (90-100% retention at 24 hours).
Formulation: Multiple unit formulations offer predictable release profiles, safety, and reduced risk of dosage form failure.
Fed or unfed state: GRT is influenced by GI motility, with longer retention in the fed state and shorter retention in the unfed state due to the migrating myoelectric complex (MMC).
Caloric content: High-protein and high-fat meals can increase GRT by 4-10 hours.
Frequency of feed: Successive meals can prolong GRT by over 400 minutes due to reduced MMC frequency.
Gender: Females tend to have longer GRT (4.6±1.2 hours) compared to males (3.4±0.6 hours), regardless of weight, height, or body surface area.
Age: Elderly individuals (>70 years) experience significantly longer GRT.
Posture: GRT varies between supine and upright positions.
Concomitant drug administration: Certain medications, such as anticholinergics, opiates, and prokinetic agents, can alter GRT.
Biological factors: Conditions like diabetes and Crohn’s disease can also influence GRT.
Polymers are used in floating system5
|
Polymer |
Sub Type |
Examples |
|
Natural |
Proteins |
Albumin, Gelatin, Collagen |
|
Carbohydrates |
Agarose, Carragenan, Chitosan, Starch |
|
|
Chemically modified carbohydrates |
Poly dextran, Poly starch |
|
|
Synthetic Polymer |
Biodegradable |
Lactides, Glycosides, and their copolymers. Poly alkyl Cyanoacrylates, Polyanhydrides |
|
Non-biodegradable |
Polymethyl methacrylate, Glycidyl, methacrylate, and Epoxy polymers, |
Rationale for Floating Drug Delivery Systems5-6
Certain medications exhibit optimal absorption at specific sites in the gastrointestinal tract, necessitating targeted delivery to maximize therapeutic efficacy. Site-specific drug delivery has become a prominent focus in the pharmaceutical industry, driven by the need to enhance bioavailability and reduce systemic side effects. Gastro-retentive drug delivery systems, including floating dosage forms, offer a promising approach to achieve this goal. By prolonging the residence time of the dosage form in the stomach or upper gastrointestinal tract, these systems enable controlled release of the medication, thereby increasing the amount of drug that reaches the target site. This approach is particularly beneficial for drugs with:
By retaining the dosage form in the stomach or upper gastrointestinal tract, floating drug delivery systems can improve the bioavailability and therapeutic efficacy of these medications, while minimizing side effects and enhancing patient outcomes.
Ideal Candidates for Floating Drug Delivery Systems (FDDS)7
FDDS is particularly suitable for medications with specific characteristics, including:
Advantages of Floating Drug Delivery Systems (FDDS)8
Disadvantages of Floating Drug Delivery Systems (FDDS)8
Applications of Floating Drug Delivery Systems (FDDS)9-10
Methods for Preparing Floating Dosage Forms11
Floating dosage forms can be prepared using various techniques, including the use of hydrocolloids that gel, such as cellulose derivatives, gelatin, hydrophilic gums, and alginates. Low-density enteric materials like cellulose acetate phthalate and methacrylic polymers can also be employed. Additionally, floating dosage forms can be prepared by packing the drug inside a capsule and reducing the particle size, generating gaseous carbon dioxide that gets trapped within the gel network, creating hollow micro-balloons made of acrylic polymer filled with the drug, or incorporating an inflatable chamber that expands in the stomach due to the vaporization of a liquid at body temperature. These methods enable the design of floating dosage forms that can prolong gastric residence time and improve therapeutic efficacy.
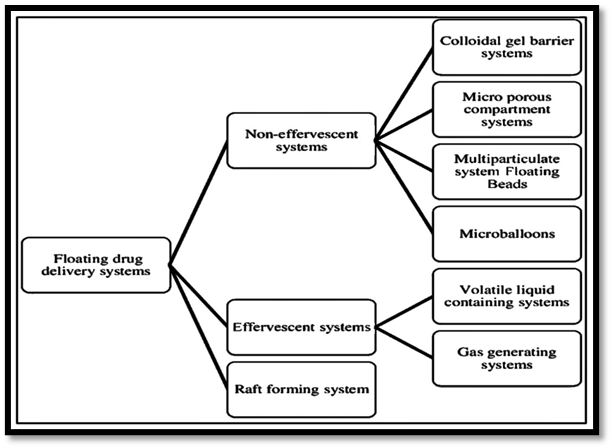
Effervescent systems utilize a combination of carbonates (e.g., sodium bicarbonate) and organic acids (e.g., citric acid, tartaric acid) to generate CO? gas, reducing the system’s density and enabling it to float on gastric fluid. This gas generation can be facilitated by incorporating a volatile liquid that evaporates at body temperature, further enhancing buoyancy. This approach allows for a sustained release of the drug in the stomach, improving its absorption and therapeutic efficacy.
These systems involve incorporating CO2-generating agents into a matrix tablet, reducing its bulk density and allowing it to float on gastric fluids. This prolongs gastric residence time, slowing down gastric emptying and enabling sustained drug release.
This system features a floatation chamber, either vacuum-sealed or filled with air or a harmless gas, which enables it to float in the stomach. The drug reservoir is encapsulated within a microporous compartment, allowing for controlled release as the volatile liquid evaporates or diffuses out, achieving sustained drug delivery.
Non-effervescent FDDS involves swelling upon contact with gastric fluids, forming a gel-like barrier that prevents rapid exit from the stomach. These plug-type systems rely on swelling and bending to stay near the pyloric valve, releasing the drug slowly. Typically, the drug is mixed with a hydrophilic polymer that swells, trapping air and providing buoyancy. This approach is widely used due to its simplicity and effectiveness, with common excipients enabling sustained release and improved bioavailability.
This system uses hydrocolloids like polyacrylate, polystyrene, or polycarbophil to form a gel barrier upon contact with gastric fluid. The gel floats on stomach contents, prolonging gastric retention and releasing the drug in solution form, enhancing absorption. Hydration of the hydrocolloid creates a colloid gel barrier, controlling drug release and improving bioavailability.
This system features a microporous compartment encapsulating a drug reservoir, with pores on the top and bottom walls. An air-filled flotation chamber enables the system to float on gastric contents, allowing controlled drug release through the pores, and enhancing gastric retention and bioavailability.
Hollow microspheres, or micro balloons, are highly efficient buoyant materials with a central hollow core. Prepared using a solvent diffusion emulsion technique, they consist of a polymer shell loaded with the drug. This design enables them to float on gastric contents, releasing the drug slowly and improving bioavailability.
Calcium alginate beads, prepared by freeze-drying, form porous floating dosage forms that sustain buoyancy for over 12 hours. Created by injecting sodium alginate into calcium chloride solution, these beads have a diameter of ~2.5 mm and provide a gastric residence time of >5 hours, significantly longer than non-floating beads (1 hour). The porous structure enables prolonged drug release, making alginate beads a promising approach for gastroretentive delivery. Studies have shown improved bioavailability and therapeutic efficacy with these floating beads, highlighting their potential for various pharmaceutical applications.
Raft-forming systems are gaining attention for delivering antacids and treating GI infections and disorders. Upon contact with gastric fluid, a gel-forming solution expands, creating a viscous raft that releases the drug slowly. This approach provides localized action, prolonged gastric retention, and improved bioavailability. Raft-forming systems often incorporate alginates, pectin, or other polymers, and can be formulated as liquids or tablets. They offer a promising approach for treating conditions like gastro-esophageal reflux disease (GERD) and Helicobacter pylori infections, with potential for tailored release profiles and enhanced therapeutic outcomes.
Evaluation of gastro-retentive dosage forms19-21
Weigh 20 tablets individually and calculate the mean weight. Compare each tablet’s weight to the mean, checking if any deviate by more than twice the percentage limit (as per USP standards). The batch passes if no tablet exceeds this limit and no more than two tablets are outside the specified range. This test ensures dosage uniformity, typically applied to tablets with active ingredients ≥50mg. For low-dose tablets, content uniformity testing is often required additionally. USP and other pharmacopoeial standards provide specific limits for different tablet types and weights.
Tablet hardness is assessed using testers like Monsanto, Strong-Cobb, Pfizer, Erweka, and Schleuniger to ensure they withstand manufacturing, packing, transportation, and patient handling stresses. The test measures the force required to break the tablet, typically expressed in kg/cm² or Newtons. Optimal hardness balances durability and disintegration; too hard may delay dissolution, while too soft may lead to breakage. Hardness ranges vary depending on tablet size, shape, and formulation, influencing patient compliance and therapeutic efficacy.
Tablet thickness is determined using a vernier caliper, available with digital or manual readings, providing measurements in mm. This straightforward test ensures uniformity and compliance with specifications, influencing packaging, coating, and patient acceptability. Consistent thickness also indicates proper compression and formulation consistency.
Friability is evaluated using a Roche friabilator, rotating 20 tablets at 25 rpm for 100 revolutions. Tablets are weighed before and after, with acceptable weight loss typically ≤0.5-1.0%. This test ensures tablets can withstand handling and transportation stresses, maintaining integrity during use. High friability may indicate inadequate binding or compression, impacting patient safety and efficacy.
Buoyancy lag time measures the time taken by a dosage form to float on the dissolution medium’s surface. This parameter, often assessed during dissolution testing, indicates the formulation’s floating ability, influencing gastric retention and drug release. A shorter lag time typically enhances floating efficacy and therapeutic outcomes.
Floating time, a key parameter for gastroretentive formulations, is assessed in Simulated Gastric Fluid (SGF) at 37°C. It measures the duration a dosage form remains buoyant on the dissolution medium, influencing drug release and bioavailability. Longer floating times often enhance therapeutic efficacy by prolonging gastric retention.
Density is determined using the displacement method, with benzene as a displacement medium. This parameter is critical for floating dosage forms, as lower density (≤1 g/cm³) enables buoyancy in gastric fluid, influencing gastric retention and drug release profiles. Accurate density measurement ensures formulation efficacy.
While bulk density and floating time describe buoyancy, resultant weight better represents a dosage form’s floating behaviour, as it accounts for changes over time. For example, gas generation and matrix erosion alter the weight, impacting buoyancy. Resultant weight integrates these dynamic changes, providing a more accurate measure of floating performance and gastric retention.
Swelling Index and Water Uptake
Swelling index, an indicator of a matrix’s swelling capacity, is assessed by measuring dimensional changes (thickness/diameter) or weight gain over time in Simulated Gastric Fluid (SGF) at 37°C. This indirect measurement reflects the dosage form’s hydration and swelling behaviour, influencing drug release kinetics and gastric retention.
Swelling index= Wt -Wowo* 100

Where, Wt = weight of dosage form at time t.
Wo = initial weight of dosage form.
In-vitro drug release was evaluated using a USP Type II (paddle) apparatus at 37°C ± 0.5°C, 50 rpm, in 900 mL 0.1N HCl. Samples were withdrawn at intervals over 6 hours, filtered (0.45 µm), and analysed using a Shimadzu UV-1800 spectrophotometer at the API’s λmax. Cumulative percentage release (CPR) was calculated using a calibration curve equation, providing insights into the formulation’s release kinetics.
Fourier Transform Infrared (FTIR) spectroscopy evaluated physical and chemical interactions between the drug and excipients. Spectra of the pure drug and floating tablet were recorded using a Shimadzu FTIR-1700 analyser (KBr disc method), identifying potential drug-excipient compatibility and structural changes.
Differential Scanning Calorimetry (DSC) assessed drug-excipient interactions using a Shimadzu DSC-60 instrument. Thermograms of pure drug and drug composite mixtures were recorded, identifying potential incompatibilities or changes in thermal properties, ensuring formulation stability and compatibility.
Stability testing, as per ICH Q1A (R2) guidelines, evaluated the impact of environmental factors (temperature, humidity, light) on the drug product’s quality. Short-term stability studies (40°C, 75% RH) assessed changes in the in vitro dissolution profile of the optimized batch over 1 month, ensuring the product’s shelf life and storage conditions.
Floating formulations for GRDDS Research done by some listed researchers in the last 5 years.
|
Drug name |
Disease |
Preparation methods |
References |
|
Lovastatin |
Hypercholesterolemia |
Floating Tablet |
(Kumar V., et al, 2025)22 |
|
Curcumin |
Peptic Ulcer |
Floating Tablet |
(Gupta C., et al, 2025)23 |
|
Atenolol |
Hypertension |
Floating Tablet |
(Patel S et al., 2025)24 |
|
Capsaicin |
Peptic ulcers |
Nanofiber films |
(Karavasili C., et al, 2024)25 |
|
Dihydromyricetin |
Parasite infections, liver diseases, and hangovers |
Compression coating technique, |
(Hao liu., et al, 2023)26 |
|
Brivacetam |
Epilepsy |
Direct compression, Floating tab |
(Jinsong Ding., et al, 2023)27 |
|
Propranolol Hydrochloride |
Hypertension and cardiovascular disorders |
3d-printed |
(Mohammed AA.,et al, 2023)28 |
|
Ciprofloxacin Hydrochloride |
Broad-spectrum fluoroquinolone antibiotics |
Sfgrdds direct compression method |
(Sheu M-T., et al, 2023)29 |
|
Niclosamide |
Antiparasitic drug being repositioned for helicobacter pylori |
3D Printed Nanocrystals by the Melting Solidification Printing Process. |
(Real JP, Real DA., et al, 2023)30 |
|
Flavonolignan Silymarin |
Treat acute and chronic hepatic diseases. |
Direct compression, Floating tab |
(Khan JA., et al, 2023)31 |
|
Metformin Hydrochloride |
Diabetes type ii |
Three-dimensional printing (3DP) |
(Millán-Jiménez M., et al, 2023)32 |
|
Gabapentin |
Treat overactive bladder |
3d-printed |
(Ghori MU., et al, 2023)33 |
|
Famotidine |
Treat gastric and duodenal ulcers, zollinger-ellison syndrome, and reflux esophagitis |
Semisolid extrusion 3d printing |
(Kim DW., et al, 2023)34 |
|
Clarithromycin And Pantoprazole |
Treating ulcers and lower and upper git bacterial infections. |
Bilayer with direct compression |
(Nawaz A., et al, 2023)35 |
|
Drotaverine hydrochloride |
An antispasmodic drug used for smooth muscle spasms and pain associated with gastrointestinal colics, renal colics, biliary colics, irritable bowel syndrome, postsurgical spasm, and uterine neck. spasm |
Direct compression, Floating mini-tablets |
(Louis MM., et al, 2023)36 |
|
Domperidone |
Used to stop feeling or being sick (nausea or vomiting) |
3D-printed |
(Patrojanasophon P., et al, 2023)37 |
|
Ofloxacin |
Treat bacterial infections of the skin, lungs, prostate, or urinary tract |
HBS floating capsules |
(Nayak AK., et al, 2023)38 |
|
Esomeprazole And Clarithromycin |
Management of gastroesophageal reflux disease (GERD), broad-spectrum antibiotic |
Effervescent floating bilayer tablets direct compression. |
(Muzammal M, Alamri AS., et al, 2022)39 |
|
Metronidazole |
Abdominal discomfort, weight loss, diarrhea, constipation |
Direct compression |
(Elkomy MH., et al, 2022)40 |
|
Ciprofloxacin |
Antiulcer therapeutic potential due to composed dietary fibers psyllium-moringa gum-alginate. |
Beads using alginate-gelatin for cefadroxil drug encapsulation |
(Singh B., et al, 2022)41 |
|
Sildenafil Citrate |
Treatment of pah |
Direct compression |
(Diniz A., et al, 2022)42 |
|
Neratinib |
Breast cancer treatment |
Effervescent floating matrix NTB |
(Alshahrani S., et al, 2021)43 |
|
Metformin HCl |
Diabetes type ii |
Direct compression floating tab |
(Huh HW., et al, 2021)44 |
|
Dipyridamole |
Widely used to prevent angina and inhibit thromboembolic complications |
Acrylamide-based hydrogels are neutral hydrogels |
(Salama AH., et al, 2021)45 |
|
Amoxicillin Trihydrate |
Treatment of Helicobacter pylori |
Floating-alginate based beads |
(Raafat Al., et al, 2021)46 |
|
Losartan Potassium |
Used to treat hypertension |
Effervescent floating matrix tablets |
(Rahamathuila M., et al, 2021)47 |
CONCLUSION
Floating drug delivery systems (FDDS) offer a promising approach to enhance bioavailability, sustain release, and minimize side effects. By prolonging gastric retention, FDDS improves absorption of drugs absorbed in the upper GI tract. Growing understanding of physiochemical and pharmacological aspects drives future advancements in FDDS design, making it a viable strategy for gastric retention and optimized drug delivery.
REFERENCES

Unnati Patel, Dhanvi Patel, Mona Gupta, Nisha Patel, Pankaj Prajapati, Floating Drug Delivery Systems: A Promising Approach to Enhance Bioavailability and Therapeutic Efficacy, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1914-1927. https://doi.org/10.5281/zenodo.19073247
 10.5281/zenodo.19073247
10.5281/zenodo.19073247
