Department of Pharmaceutical Quality Assurance Ravindra Vidya Prasarak Mandal Institute of Pharmacy, Dwarka Nashik India
The therapeutic potential of Tridax procumbens, a widely recognized medicinal plant, has been evaluated for its anxiolytic and anticonvulsant properties using rodent models. This study aimed to explore the efficacy of Tridax procumbens in managing anxiety and convulsions, both of which are common neurological issues with limited treatment options. The research utilized well-established behavioral tests, including the Elevated Plus Maze (EPM) and Open Field Test (OFT), to assess the anxiolytic effects, while anticonvulsant properties were evaluated through the maximal electroshock and pentylenetetrazol (PTZ)-induced seizure models. In the EPM test, animals treated with Tridax procumbens showed a significant increase in the time spent in the open arms, suggesting a reduction in anxiety-like behaviors. The OFT results further confirmed its anxiolytic potential by demonstrating enhanced locomotor activity and exploration. Additionally, in seizure models, Tridax procumbens exhibited a remarkable dose-dependent reduction in both the frequency and duration of seizures, showcasing promising anticonvulsant effects. Histological analysis revealed that treatment with Tridax procumbens also provided neuroprotection, evident through preserved brain architecture and reduced neuronal damage. These findings indicate that Tridax procumbens possesses significant anxiolytic and anticonvulsant properties, supporting its potential as a novel, natural therapeutic option for anxiety and seizure disorders. Further studies focusing on the plant’s bioactive compounds and mechanistic pathways are warranted to validate its clinical application in neurology.
The human brain is the single most important organ of the human nervous system. Humans and other species are distinguished by the functions of their brain and physiology. Disorders of the brain’s function (anxiety, epilepsy, depression, and dementia) are the major concern of human society. WHO defines “health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”, it is also suggested that there is no health without mental health. Among all the diseases of human being, it is estimated that approximately 12% of psychiatric disorders are the global disease burden in nowadays. It is assumed that it may likely to be increase up to 15% by 2020. Since it is considered as the biggest global health concern. [1]
ANXIETY
1. Anxiety: An Overview
Globally, anxiety-related disorders perturbs one-eighth of the total population. At present, psychopharmacology-related research activities dominate the healthcare sector. Among the psychiatric diseases, anxiety- related disorders elicit paramount stress to individuals, families and society. However, clinical utility of currently available anxiolytics has been limited due to their minimal therapeutic efficacy and noxious effects. [2] Anxiety is a state characterized by the worry and apprehension in response to threat (either actual or potential) to well-being. Anxiety is expressed at behavioral, psychological and physiological levels of the organism. It is suggested that the exposure to aversive stimuli evoke anxiety related behavioral and neurochemical alteration [3]. In the behavioral paradigms rodents often experience novelty which is responsible to evoke the anxiety-related behavioral response in the rodents subjected to these paradigms [4]. Anxiety and depression are extremely dramatic and debilitating multifacetic disorders and it is now becoming clear that without knowledge of clinical and biological aspects of anxiety and depression, it is impossible to offer effective treatment strategies for the patients [5]. Decreased fear, an increased exploratory behaviour and the behavioural disinhibitory effect of the standard anxiolytic. The BZDs are relatively safe and are widely used anxiolytic agents. These agents are known to act through the BZD-GABA receptors; the role of GABA in anxiety is well established [6]
2. Signs and Symptoms A subjective experience of distress with accompanying disturbances of sleep, concentration, social and/or occupational functioning are common symptoms in many of the anxiety disorders. Despite their similarities, these disorders often differ in presentation, course and treatment. Patients often present with complaints of poor physical health as their primary concern. This may temporarily distract from the underlying anxiety symptoms. This is particularly common in panic disorder, which is characterized by a short period of intense fear and a sense of impending, doom, with accompanying physical symptoms, such as chest pain, dizziness and shortness of breath [7].
Figure 1: signs and symptoms of anxiety
3. Epidemiology
Recently, the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) estimated that the anxiety disorders affected 3.6% and depressive disorders affected 4.4% of the global population in the year 2015. As part of the world mental health survey, a large-scale epidemiological survey was conducted in India. [6]The survey also reported a higher prevalence of anxiety disorders among females compared to males (4.42% vs. 2.44%, respectively). The National Mental Health Survey (NMHS) carried out in the year 2015–2016 also reported similar findings [7]. The survey was carried out in 12 states across six regions of India, which included a household sample of 34, 802 adults (≥18 years). The suicide risk was also found to be higher in this age group [8].
Among younger age groups, the most common anxiety disorders are social anxiety disorder, specific phobias, and separation anxiety disorder. If left untreated, anxiety disorders that begin early in life can become chronic and can be associated with a high probability of recurrence in adulthood. There is consistent, strong evidence that people with anxiety disorders have an increased risk for suicidal behaviour. Various studies have reported that approximately 7–12% of suicide attempts were attributable to anxiety disorders [9].
4. Pathophysiology of Anxiety Disorders
The exact mechanism is not entirely known. Anxiety can be a normal phenomenon in children. Stranger anxiety begins at seven to nine months of life. Anxiety symptoms and the resulting disorders are thought to be due to disrupted modulation within the central nervous system. Physical and emotional manifestations of this dysregulation are the result of heightened sympathetic arousal of varying degrees. Several neurotransmitter systems have been implicated to have a role in one or several of the modulatory steps involved. These systems regulate and are regulated by other pathways and neuronal circuits in various regions of the brain, resulting in dysregulation of physiological arousal and the emotional experience of this arousal.
It is, therefore, selective serotonin reuptake inhibitors (SSRI) and serotonin norepinephrine reuptake inhibitors (SNRI) many believe that low serotonin system activity and elevated noradrenergic system activity are responsible for its development. that are the first-line agent for its treatment Disruption of the gamma- aminobutyric acid (GABA) system has also been implicated because of the response of many of the anxiety spectrum disorders to treatment with benzodiazepines. Serotonin and GABA are inhibitory neurotransmitters that quieten the stress response. All of these neurotransmitters have become important targets for therapeutic agents.[7]
5. Treatment Modalities
Currently, serotonin reuptake inhibitors (SSRIs) are the mainstay in the treatment of anxiety-related disorders. Meanwhile, benzodiazepines (BZD) remain an important class of medication for the treatment of anxiety. However, acute administration of benzodiazepines displays cognitive side effects like sedation, impairment in attention, alteration in psychomotor performance and memory scarcity. Apart from the adverse effects, tolerance to side effects occurs after repeated dose of administration.[10]
Treatment of anxiety with BZD prelude to unwanted sedation, but in some instances where sedation is desired (treatment of insomnia), residual daytime sedation can be erratic. Further, it produces lack of ability to concentrate on task or shift attention from one task to another.[11] Moreover, coordination and psychomotor speed were minimized, extension of reaction times are seen in patients. Traffic accidents and workplace injuries are the hallmark of BZD adverse events. While in geriatric patients receiving BZD, ataxia and postural instability are associated with an increased risk of falls and hip fractures.[12]
6. Pharmacological Options
Pharmacotherapy is the most common approach, especially in the developed areas of the world. The different classes of anti-anxiety drugs include anxiolytics, anti- depressants, anticonvulsants, and anti-psychotics.The therapeutic dose for the treatment has to be carefully regulated with all the treatment classes, as patients with anxiety tend to be sensitive to most of the drug side-effects [13].
7. Anti-anxiety drugs
The earliest modern pharmacological treatment of pathologic anxiety was the application of sedating medications, barbiturates, and benzodiazepines, which target the inhibitory GABA receptors. These drugs are usually prescribed for a shorter period as they tend to develop a dependency, especially in people who have abused drugs and alcohol. It has been observed that people face withdrawal symptoms after discontinuation of benzodiazepines.[14]
Barbiturates: At low concentrations barbiturates increase GABA-induced chloride currents; whereas at high concentrations they directly open the channels in the absence of GABA. This blockade of glutamatergic transmission inhibits cationic influx into neurons, thus reducing the frequency of action potentials.
Benzodiazepines: Benzodiazepines were discovered in the early 1960s with the hope for safer and better psychiatric drugs, and subsequently became the most used class of drugs. GABAA receptors possess binding sites for several drugs, including that of anxiolytics, anticonvulsants, barbiturates, general anaesthetics, ethanol, and neurosteroids [11]. They have a rapid onset of effect, which begins soon after oral and/or parenteral applications, and they have long half-lives. Many patients with GAD and panic disorders have been treated with benzodiazepines. However, benzodiazepine usage is associated with adverse effects such as CNS depression, resulting in fatigue, dizziness, increased reaction time, dependency, and impaired cognitive functions. Various studies have reported that benzodiazepines are associated with higher suicide risk, especially in the case of comorbidity between anxiety and depressive [15]. Therefore, current guidelines do not recommend benzodiazepines as first-line treatments due to their potential side effects.
EPILEPSY
Epilepsy is the tendency to have seizures that start in the brain. The brain uses electrical signals to pass messages between brain cells and when these signals are disrupted, it leads to a seizure. According to the WHO, about 450 million people in the entire world have suffered mental, neurological, or behavioral problems out of which 1-2% has had epileptic seizures [16]. The disease can affect people of any age, gender, race, or class where the pain is shared by both affected persons and their caregivers. Apart from the discomfort that individuals with epileptic seizures encounter, their dependents experience social stigma.[17]
1. Epidemiology
Epilepsy has been considered as a public health problem affecting about 50 million people worldwide. A global campaign was launched against a common neurological disorder of epilepsy in 1997 by the World Health Organization (WHO) and the International League against Epilepsy (ILAE).
Antiepileptic drugs (AEDs) are the mainstay for the treatment of epilepsy and generally suppress seizure occurrence. In the past 15 years, newer antiepileptic drugs have effectively replaced the older agents and they possess potential advantages in terms of pharmacokinetics, tolerability and lower risks for drug-drug interactions. [31] According to one estimate, in high income countries, the number of new cases adding up is 30 to 50 per 100,000 people in general population. Epilepsy patients are at a higher risk of dying young. Epilepsy with symptoms might cut life short by up to 19 years. Early death, trauma, homicide, infections, and epileptic seizures are all more common in epilepsy patients than in the general population [18].
TYPES OF EPILEPTIC SEIZURE
When a person experiences at least 2 seizures that are not related to another established medical problem, such as opiate withdrawal or exceptionally low blood sugar, an epilepsy diagnosis is typically made. That part of the brain from which the seizure frequently originates in early phases causes disturbance in functions of the affected part.
he right side of the body is governed by the left half of the brain, while the left side of the body is governed by the right half of the brain. Typically, Doctors determine seizure as either generalized or focal depending on where and how the abnormal activity of the brain starts. Focal seizures are caused by the aberrant activity of the brain in a specific part of the brain, while generalized seizures appear to be involved in the entire brain. Neuro-experts have divided seizures into two main groups, partial and generalized, depending on the signs, as depicted.[19]
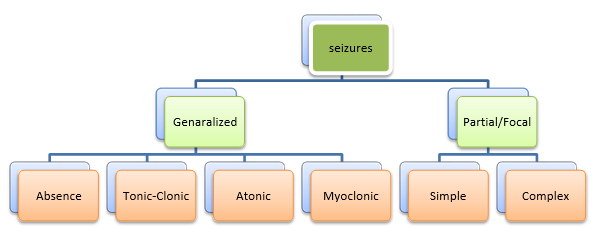
Figure 2: Classification of seizure
SYMPTOMS OF EPILEPTIC SEIZURE
The symptoms of a partial seizure, which are mostly brought on by damage to the cerebral hemisphere, can be utilized to define it. Additionally, there are two basic categories of partial seizures: simple-partial and complex-partial. In simple-partial, the person appears cognizant and can typically speak, whereas, in complex-partial, patients behave erratically, become disoriented, and frequently mumble and chew. A generalized seizure comprises two main components as well.[20]
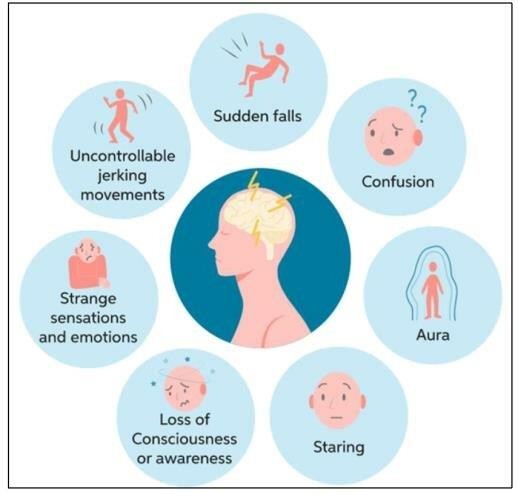
Figure 3: Signs and symptom of epilepsy
Risk Factors in Epilepsy:
Risk factors include age, genetics, family history of epilepsy, history of febrile seizures, alcohol consumption, CNS and other infections, brain trauma, head injury, perinatal stroke, preterm birth, and geographic location. Epilepsy induced by a head injury, central nervous system illnesses, and tumors can strike at any age. The most frequent risk factor in people over 65 is cerebrovascular disease. In adulthood, external non-genetic risk factors such as vascular disease, such as stroke, are increasingly common. Certain types of epilepsy, whether in childhood or adults, may be linked to modifiable risk factors such alcohol use, traumatic brain injuries, or CNS infections Knowing these risk factors could enable for more regular outpatient clinic examinations, warning families about seizures, advising to record video in case of seizure suspicion, and, if necessary, obtaining an early electroencephalogram (EEG).[21]
Pathophysiology of epileptic seizures:
A brief episode of clinical manifestations and pathophysiological changes in the brain caused by abnormally high or synchronised neuronal activity is known as a seizure activity. A transient synchronised discharge of a network of neurons that lasts less than 70 milliseconds and is distinct from a seizure is known as an interictal spike. The paroxysmal surging region can, in fact, be distinguished from the seizure onset zone. Seizures are thought to be triggered by a disruption in the brain's usual balance of excitation and inhibition; however this is now regarded an oversimplification. Communication among dissimilar circuits is required for the brain's function, which is most likely mediated through waves among these circuits. The creation of oscillations in cortical networks is dependent on interneurons, neural transmission (e.g., synaptic transmission), and inherent neuronal properties [22].Greater spread and neuronal recruitment, as a result of a combination of greater connection with neuronal plasticity, increased excitatory transmission, a failure of inhibitory mechanisms, and changes in intrinsic neuronal properties, are thought to be the beginning of the transition from normal to epileptiform behaviour. In human studies, the electroencephalogram (EEG) becomes less chaotic in large areas of the cortex before a seizure, indicating extensive synchronisation [23].
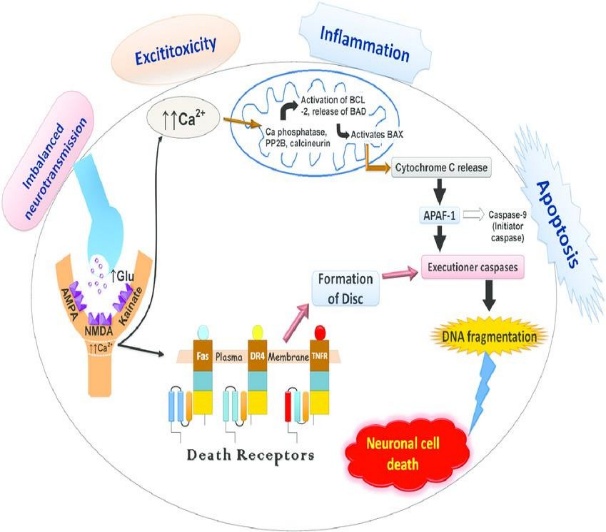
Fig: 4 Basic cascade events of pathophysiology of epilepsy [24]
Few Common Antiepileptic Drugs (AEDs): -
Variety of the anticonvulsant drugs, including carbamazepine, phenytoin, primidone, phenobarbital, clonazepam, valproic acid, and ethosuximide, are available for use in the treatment of patients with seizure disorders [25]. The AEDs used in the management of two major types of seizures namely partial and generalized seizure, are relatively different in their profiles. The phenobarbitone (PBT) was the first synthetic drug accepted as AED. Its effectiveness was limited to generalized tonic-clonic seizures, and to a lesser extent, simple and complex partial seizures and had no effect on absence seizures. The PHT reduced seizures without causing sedative effects. [26].
only six major drugs available in the US for the treatment of patients with epilepsy. These included phenobarbital (PB), phenytoin (PHT), carbamazepine (CBZ), primidone (PRIM), valproic acid/sodium valproate (VPA) and ethosuximide (ESX). Despite these six agents, as well as several secondary drugs, it is estimated that over 30% of patients have inadequate seizure control, while others, whose disease is adequately controlled, suffer from bothersome adverse events (AEs). Since 1993, ten new drugs have entered the worldwide market (not all in the US). Those released include felbamate (FBM), gabapentin (GBP), lamotrigine (LTG), topiramate (TPM), tiagabine (TGB), oxcarbazepine (OXC), levetiracetam (LVT), zonisamide (ZNS), clobazam (CLB) and vigabatrin (VGB). [27].
Mechanism action of antiepileptic drugs[28]
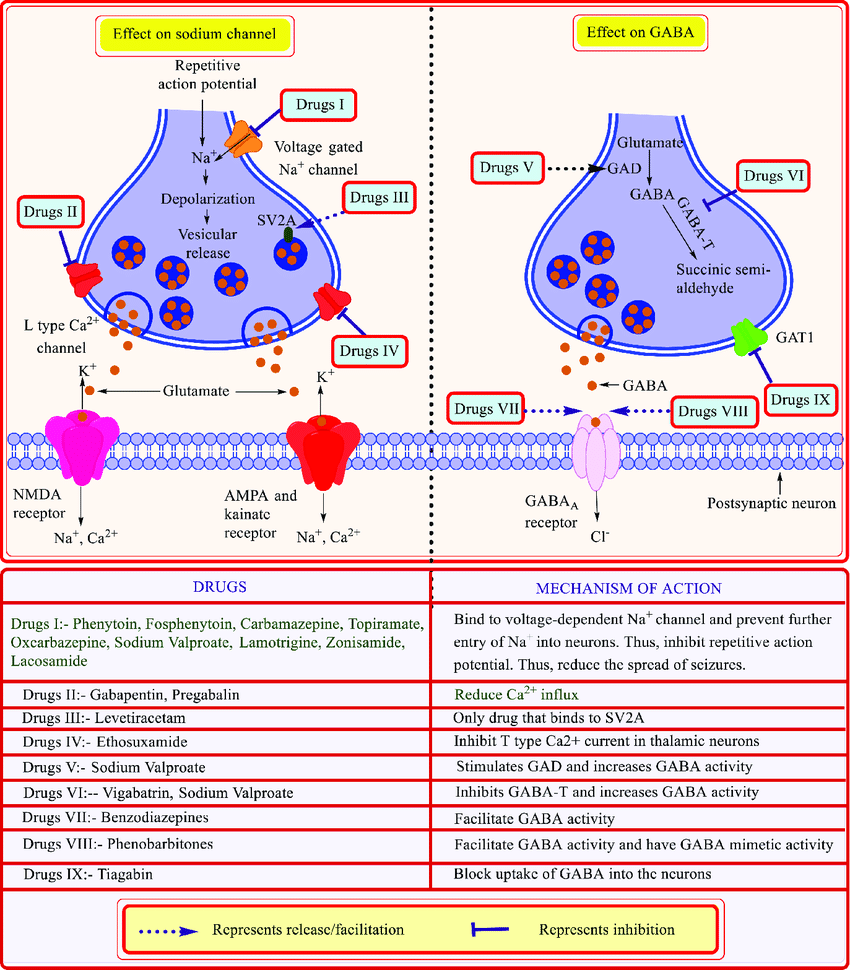
Figure 5: Mechanism action of antiepileptic drugs
TRIDAX PROCUMBEN
Tridax procumben has herbaceous, semi-prostrate habit, and can grow anywhere from 15-40 cm in height. The inflorescence is a capitulum with three-toothed white ligulate ray florets female and disc inner flowers yellow, tubular, bisexual, with corolla 6 mm long. The inflorescence results in abundant production of pappus achenes 2 mm long, obovoid, setaceous, covered with stiff hairs, that can be carried by the wind for long distances, making this species a potential invasive species if not controlled.[47]
Chemical Constituents
The phytochemical study revealed presence of flavonoids, carotenoids, alkaloids, tannins and saponins. The adjacent profile shows that the plant is rich in sodium, potassium and calcium. Leaf of Tridax procumbens mainly contains proteins, fiber, carbohydrates, and calcium oxide. Whereas the fumaric acid and tannin has also been reported in the plant. Oleanolic acid was obtained in good amounts from Tridax and found to be a potential antidiabetic agent when tested against a glucosidase. A number of chemical constituent were reported from the plant that are alkaloids, flavonoids, carotenoids, fumaric acid, lauric acid, tannins etc
A REVIEW: ANXIOLYTIC STUDY
A Review: Antiepileptic Study
CONTRIBUTIONS OF NATURAL PRODUCTS TO CNS DRUG DEVELOPMENT
E. Ngo Bum., et.al. 2011: Many of the plant based medicinal products like St. John’s Wort, ginseng, and ginkgo biloba, have been used in neurological disorders in the last decade. There are also many herbal medicines whose pharmacological activity has been studied in experimental animal models. These studies are the essential basis for the development of new therapies from herbal medicinal plants for use in clinical practice.[29]
Afrormosia laxiflora (A. laxiflora) Chenopodium ambrosioides (C. ambrosioides) Microglossa pyrifolia (M. pyrifolia) Mimosa pudica (M. pudica)
PLANT PROFILE: TRIDAX PROCUMBENS
Overview of Tridax procumbens. (Asteraceae)
Samantha Beck., et.al. 2018:
The species has a diploid number of 36. It has herbaceous, semi-prostrate habit, and can grow anywhere from 15-40 cm in height. The leaves are elongated, opposite, ovate with serrated margins, hirsute on the abaxial and adaxial sides . The inflorescence is a capitulum with three-toothed white ligulate ray florets female and disc inner flowers yellow, tubular, bisexual, with corolla 6 mm long. The inflorescence results in abundant production of pappus achene, 2 mm long, obovoid, setaceous, covered with stiff hairs, that can be carried by the wind for long distances, making this species a potential invasive species if not controlled.[30]
Taxonomical classification:
Kingdom: Plantae Subkingdom: Viridiplantae
Superdivision: Spermatophytina
Class: Magnoliopsida
Superorder: Asteranae
Order: Asterales
Family: Asteraceae
Genus: Tridax L-tridax
Species: Tridax procumbens L


Vernacular names:
Hindi: Ghamra.
Sanskrit: Jayanti Veda.
Marathi: Dagadi Pala and Ghav Pala,
Telugu: Gaddi Chemanthi.
Tamil: Thatapoodu.
Malayalam: Chiravanak.

Origin and geographical distribution:
The plant is native of tropical America and naturalized in tropical Asia, Africa, Australia, and India. It is a wild herb distributed throughout India. It is also found along road sides, waste grounds, dikes, river banks, meadows and dunes.

Figure 6: Tridax procumben plant
Samantha Beck., et.al. 2018:
Traditional uses
Traditionally, Tridax procumbens has been in use in India for wound healing and as an anticoagulant, antifungal, and insect repellent. The juice extracted from the leaves is directly applied on wounds. Its leaf extracts were used for infectious skin diseases in folk medicines. It is used in Ayurvedic medicine for liver disorders, hepatoprotection, gastritis, and heartburn. It is also used as treatment for boils, blisters, and cuts by local healers in parts of India. Traditional and complementary medicine is being increasingly recognized as an integrative approach to health care in many countries (WHO, 2013). The use of plants for medicinal purposes may date back to the Middle Paleolithic age, approximately 60,000 years ago T. procumbens is found throughout the world and it has been used to treat anemia, colds, inflammation, and hepatopathies in Central America. In Guatemala, T. procumbens is used as an antibacterial, antifungal, and antiviral treatment as well for vaginitis, stomach pain, diarrhea, mucosal inflammations, and skin infections. The leaf juice is used to treat wounds and stop bleeding.
Samantha Beck., et.al. 2018:
Chemical Constituents
The phytochemical study revealed presence of flavonoids, carotenoids, alkaloids, tannins and saponins. The adjacent profile shows that the plant is rich in sodium, potassium and calcium. Leaf of Tridax procumbens mainly contains proteins, fiber, carbohydrates, and calcium oxide. Whereas the fumaric acid and tannin has also been reported in the plant. Oleanolic acid was obtained in good amounts from Tridax found to be a potential antidiabetic agent when tested against a glucosidase. A number of chemical constituent were reported from the plant that are alkaloids, flavonoids, carotenoids, fumaric acid, lauric acid, tannins etc.
Primary metabolites: Primary metabolites involved in metabolic pathways present in all plants. There are a few specific primary metabolites that have been extracted from
T. procumbens: Lipids are essential in living organisms; they influence the communication between cells, the cellular makeup, and act as an energy source for the organism. T. procumbens contains common fats found in the Asteraceae family. All these compounds play essential roles in plants and are common to many species.
Secondary Metabolites: Secondary metabolites contain bioactive compounds that often have useful and important medicinal properties. Some of the most important bioactive compounds for medicinal uses are found in compounds such as glycosides, nitrogenous organic compounds, fat-soluble compounds, polyphenolic compounds, and minerals T. procumbens secondary metabolites have been included into six major groups: flavonoids, carotenoids, alkaloids, saponins, tannins, and terpenes.
Flavonoids: Luteolin and Quercetin were also isolated from Tridax, along with the flavonoid Procumbenetin. Lutein, glucoluteolin, and isoquercetin are found in the flowers of T. procumbens. Luteolin has anti-inflammatory and anti-carcinogenic activity probably due to its anti-oxidant activity and its free-radical scavenging ability Luteolin has shown strong inhibition of tumor proliferation by suppressing angiogenesis. In vitro studies indicate that Luteolin has activity against different cancer cell lines including breast, liver cancer hepatoma, colon cancer, human lung squamous carcinoma and uterine cancer. In vivo studies have also shown anti-carcinogenic activity of Luteolin; for example, Quercetin is an antioxidant, protecting against lipid peroxidation, with effective antiulcer activity against ethanol-induced ulcerogenesis it also increases the level of beta-carotene and decreases the level of retinol.
Tannins: Tannins are naturally occurring water-soluble polyphenols found in plants. Tannins have anti-microbial properties, as well as anti-carcinogenic and anti- mutagenic properties, potentially because of their antioxidant capabilities. Several researchers have described the presence of tannins in T. procumbens. Acetone-water or Chloroform-water showed. Tannins are present in the pedicle and buds of T. procumbens.
Carotenoids: Carotenoids are fat-soluble pigments found in the leaves that have three main functions in a plant: light-harvesting, protection from photo oxidative damage, and pigmentation to attract insects. Carotenoids have been postulated to prevent damage to DNA by oxidative stress. Many types of these secondary metabolites have been isolated from T. procumbens including beta-carotene, which can be converted to vitamin A, which is important for maintenance of epithelial tissues. Vitamin A deficiency can result in impairment of immunity and haematopoiesis, night blindness, and Exophthalmia. Carotenoids such as beta-carotene and lutein have shown activity in the reduction of UV-induced erythema.
Alkaloids: Alkaloids are defined as any class of nitrogenous organic compounds of plant origin that have pronounced physiological effects on humans. The presence of some alkaloids has also been reported in T. procumbens. In a phytochemical screening analysis, using aqueous extraction of the leaves, thirty-nine alkaloids were present, mainly Akuamidine (73.91%) and Voacangine (22.33%). Besides alkaloids, the extract contained sterols and tannins. The total amount of alkaloids in the pedicle was 32.25mg/gdw in the pedicles and 92.66mg/gdw in the buds. The presence of these alkaloids point once more to the great potential of this plant.
Saponins: Saponins are steroidal glycosides that contain pharmacological and medicinal properties and have been detected in T. procumbens, specifically a steroidal saponin and pΒ-Sitosterol-3-O-β-D-xylopyranoside in the flowers of the species Another study determined that saponins from an ethanolic extract of T. procumbens could potentially contain antidiabetic properties by inhibiting the sodium glucose co- transporter-1 (S-GLUT-1) in the intestines of male Wistar albino rats. [47]
Reported Pharmacological activities:
The great variety of secondary metabolites in Tridax, show the potential pharmacological properties of this species, however, we have yet to see the use in allopathic medicine. These compounds have been used for their properties in anemia prevention, liver protection, immuno-enhancement, and antioxidant, anticancer, antibacterial, antifungal, antiparasitic, antiplasmodial, and antiviral activities.
Bhati-Kushwaha and Malik., et.al. 2014
Antimicrobial Activity: Antimicrobial screenings have been done, but additional studies are needed to corroborate some of the results. Various species of bacteria and fungi have shown sensitivity to the antimicrobial properties of T. procumbens. More recently, callus of stem and leaf has shown to be useful for the synthesis of silver nanoparticles that showed some antimicrobial activity against E. coli, V. cholerae, A. niger, and A flavus. However, this activity was lower than the activity shown by silver nitrate so these results are not conclusive.[31]
Christudas., et.al. 2012; Manjamalai., et.al. 2012b
Petroleum, ether and ethanolic extracts of leaves of T. procumbens showed antibacterial activity against Bacillus faecalis. This activity was reported to be probably due to the presence of alkaloids. The chloroform extracts showed antibacterial activity against B. faecalis, B. subtilis, E. coli, and Pseudomonas aeruginosa but the experiments need better controls and descriptions of the procedures. Essences from T. procumbens show the presence of alpha and beta pinenes, used in small quantities can help in treating bacterial and fungal infections. There are some contradictory results about the antimicrobial activity of this species.[32,33].
Policegoudra., et.al. 2014
Antifungal Activity: Antifungal activity of T. procumbens has been investigated. Different extraction methods have been used to find the optimum zone of inhibition from different fungal strains including Microsporum fulvum, Microsporum gypseum, Trichophyton mentagrophytes, Trichophyton rubrum, Candida albicans, and Trichosporon beigelii. Extracts of the aerial parts of this plant have shown activity against dermatophytes with zones of inhibition ranging from 17 to 25mm with dichloromethane (DCM) fraction resulting in the best response However, the authors do not describe which ones are the bioactive compounds responsible for the antifungal properties. [34]
Taddei and Rosas-Romero., et.al. 2000; Manjamalai., et.al. 2012b
Antibacterial Activity: Tridax procumbens has shown to have antibacterial activity. It is one of the most common plants for treating bacterial infections in rural parts of the world. Tridax extracts have shown to be effective against a variety of bacteria. N- hexane extracts have activity against Mycobacterium smegmatis, E. coli, Klebsiella sp., Salmonella group C, and Salmonella paratyphi. The ethyl acetate extract was effective against Gram-positive bacteria such as Bacillus cereus, Mycobacterium smegmatis, Staphylococcus aureus, and Gram-negative bacteria such as Klebsiella sp. The essential oil extract of T. procumbens shows significant activity against Gram-positive bacteria: Staphylococcus aureus and Streptococcus pneumoniae. There are some differences in how the studies were conducted so even though there seem to be strong support for the antibacterial activity of this species, more comprehensive research needs to be done.[35,36]
Appiah-Opong., et.al. 2011; Marti?n-Quintal., et.al. 2009
Antiparasitic Activity: Treatment of some diseases caused by protozoal infections like malaria, dysentery, colic, and vaginitis have been assessed with T. procumbens through a bioassay guided fractionation with a methanol extract to isolate an active compound, (3,S)-16,17-Didehydrofalcarinol (an oxylipin). Tridax seemed to have anti-leishmanial activity when using crude extracts from the whole plant. A study done in Ghana tested the antiplasmodial effect of aqueous, chloroform, ethyl acetate, and ethanolic extracts from the flowers, leaves, and stem of T. procumbens. There is evidence that the aqueous and ethanolic extracts from the species have anti-plasmodial properties; a study using the tetrazolium-based colorimetric assay showed that T. procumbens helped protect red blood cells from P. falciparum damage. Tridax shows a great potential against a disease that kills millions of people around the world. [37,38]
Ravikumar., et.al. 2005b,
Antioxidant Activity: Free radicals include reactive hydroxyl radicals (OH), superoxide anion radicals, hydrogen peroxides, reactive oxygen species (ROS), and peroxyl. The instability of these radicals can damage many biologically important molecules like DNA and macromolecules, thus leading to cell damage and homeostatic disturbance. An antioxidant or a free radical scavenger is used to reduce this activity by preventing the oxidation within a biological system. Analysed the antioxidant activity of T. procumbens and found significant activity (comparable to the activity of Ascorbic acid) in the ethyl acetate and n-butanol fractions obtained from methanolic extracts, when using the 1,1-diphenyl-2-picrylhydrazyl (DPPH) method. Also reported a high antioxidant activity of Tridax when using n-butanol and ethyl acetate fractions from methanolic extracts. The strong anti-oxidant activity of T. procumbens is due to the high content of phenols, flavonoids, anthraquinone, carotenoids and vitamins A and C. [39]
Manjamalai, A., 2012
Anticancer Activity: Only until recently has the anticancer activity of T. procumbens been researched. Crude flower aqueous and acetone extracts were tested on prostate epithelial cancerous cells (PC3). Very weak anticancer activity was observed with the aqueous extract. The acetone extract showed an 82.28% activity against cancer cells within 24 hours of treatment. The viability was analyzed using the MTT assay. Significant inhibition of tumor nodule formation in the lungs was observed when using T. procumbens, probably due to the inhibition of formation of new blood vessels in response to monoterpenes (alpha and beta pinenes). There was also an increase of expression with P53 and caspase; indicating that the oils of this plants could induce apoptosis.[40]
Saraf and Dixit., et.al. 1991, Wagh and Shinde., et.al. 2010
Hepatoprotective Activity : Many models have been used to evaluate the effect that
T. procumbens has on reducing oxidative stress in the liver, which leads to liver injury, and the hepatoprotective activity of different extracts. It was determined that when the ethanolic extract from T. procumbens was administered orally at varying dosages, it lowered the levels of serum Aspartate aminotransferase, serum Alanine aminotransferase, serum Alkaline phosphatase, and serum bilirubin, resulting in hepatoprotection. Petroleum ether, methanol, and chloroform water extracts from flowers showed protection against hepatotoxicity in Male Wister Albino Rats, with the methanolic extract showing the best effect. [41,42]
Nwanjo., et.al. 2008, Ravikumar., et.al. 2005a
Aqueous extracts of leaves have shown hepatoprotective activity in rats because of the antioxidant activity of these extracts, due to the active free radical scavenging. An ethanolic extract from leaves of T. procumbens that was fractionated with chloroform showed good hepatoprotective activity in rats that had induced hepatitis by d- Galactosamine Lipopolysaccharide. The study suggests that pretreatment with the plant extract may have caused parenchymal cell regeneration in the liver. The rats that were pretreated also restored their lipid levels to normal after being treated with d- Galactosamine Lipopolysaccharide. Rats that were treated with only the T. procumbens extract showed to no adverse reactions, suggesting that the plant has little to no toxicity in rats. [43,39]
Tiwari., et.al. 2004
Immuno-enhancement Activity: An adaptogen of Tridax procumbens has shown to enhance the body's nonspecific resistance against pathogens. This work compared the Delayed-type hypersensitivity (DTH) in the animals fed with the extracts versus the controls to evaluate cell-mediated immunity. The authors suggest that there was enough evidence for the initiation of clinical trials in immunocompromised patients However, we think that more in-depth studies should be done before clinical trials can be initiated. Even though research has shown that T. procumbens does possess immunostimulators, it is unclear what constituents are immunostimulators, and what constituents are immunosuppressant; different extraction and fractionation methods need to be done and then each solution tested to determine the constituents and their activity.[44]
Petchi., et.al. 2013; Pareek., et.al. 2009
Antidiabetic Properties: Diabetes has become a worldwide epidemic; interestingly,
T. procumbens has shown antidiabetic properties. The study showed that the extract had antidiabetic activity that is comparable to the drug Glibenclamide used to treat diabetes mellitus type 2. The drug works by increasing the amount of insulin produced by the pancreas. This study included proper controls and two different concentrations of whole plant extract of Tridax (250 mg/Kg and 500 mg/Kg). ANOVA and Dennett’s post hoc test showed significant antidiabetic activity compared to the controls. The plant extracts were given to rats in 250 or 500 mg/kg doses, while the Glibenclamide was given at a 10 mg/kg dose. The results showed that either dosage of the plant extract lowered the blood glucose levels in the rats by 10.96%-13.74% better than the conventional drug after 6 hours of treatment. The plants extracts also showed an improvement in the fasting blood glucose levels of the Alloxan-induced diabetic rats.
[45,46]
Bhagwat., et.al. 2008; Sonawane, A., et.al. 2014: In a study oral administration of aqueous and alcoholic extracts from the leaves of T. procumbens significantly decreased blood sugar levels in Alloxan-induced Wistar T. procumbens slowed the rate of both alpha amylase and alpha glucosidase enzymes with ether, methanol, and chloroform extracts showing a significant reduction, enough to resemble common drugs used to slow the enzymes in diabetes treatment (Alpha-amylase and the Alpha-glucosidase enzymes are responsible for the breakdown of carbohydrate molecules, by slowing their breakdown rate, allowing the body to digest these carbohydrates in lower doses and therefore slowing the need for insulin, which is the main chemical affected in diabetes mellitus. All these studies demonstrate the great pharmacological potential of Tridax against diabetes and the importance of further research and clinical studies that could evaluate the effect in humans. [47,48]
Salami., et.al. 2017
Antihypertensive Activity: For adults over 20, hypertension, or high blood pressure, is any measurement where the systolic number is above 140 mmHg, and the diastolic reading is above 90 mmHg. The CDC also characterized people who were taking medications to lower their pressure as individuals with hypertension. From 2009-2012, 30% of Americans, over the age of 20, had high blood pressure (National Center for Health Statistics). In Benin and other countries, Tridax procumbens has been traditionally used for the treatment of hypertension. Because of its traditional history, a study was done looking into its antihypertensive activity. The aerial parts of the plant were used to make cyclohexane, micellar, dichloromethane, and ethyl acetate fractions from a crude aqueous extract. [49]
Table 1: Pharmacological properties of Tridax procumbens
|
Plant part |
extract |
Biological activity |
Phytochemi cal |
Reference |
|
Whole plant |
Methanol and aqueous |
Antioxidant and antibacterial activities |
Phenolic and flavonoids compounds |
Bera and Banerjee (2023) |
|
Leaves |
Dichlorometh ane, butanol, ethyl acetate and methanol |
Antidiabetic and antioxidant activities |
Flavonoids, phenols, terpenes, sterols and alkaloids |
Nandi et al. (2022) |
|
Leaves |
Methanol, ethanol, aqueous, chloroform, acetone and ethyl acetate |
Anticancer, Antioxidant and antibacterial activities |
Alkaloids, polyphenols and tannins |
Syed et al. (2020) |
|
Whole plant |
Hydroalcohol ic extract and fractions |
Antioxidant and antimicrobial activities |
Flavonoids, phenols, terpenes, sterols and alkaloids |
Jalalpure and Patil (2022) |
|
Whole plant |
Aqueous |
Wound-heali ng and antibleeding activities |
Phenols |
Gubbiveeran na et al.(2019) |
MATERIALS AND METHODOLOGY
STERILIZATION OF GLASSWARE
Glassware were soaked overnight in cleaning solution and washed thoroughly with running tap water. They were then cleaned with detergent solution and rinsed several times with tap water and finally in distilled water and air dried. The glassware and media were sterilized in an autoclave at 15psi for 20 minutes, at 120oC.
COLLECTION OF PLANT MATERIAL
Plant material were collected from medicinal garden of DCS's Annasaheb Ramesh Ajmera College of Pharmacy and authenticated by Dr. S.R. Kshirsagar (Assistant professor). Head of the Department of Botany, Dhule. The authenticated plant materials were washed firstly with tap water followed by distilled water. Leaves stem and flowers separated from the plant, dried completely under shade and pulverized into coarse powder. The powder was kept in air tight container for further use.
About 1 kg of the Tridax procumben was freshly obtained washed with running tap water and dried at room temperature to a constant weight. The dried plant samples were grinded into powder form using mortar and pestle and the powdered samples were stored in clean polythene bags until required for use.
DRUGS AND CHEMICALS
Diazepam (Zepose 5 mg, Cipla Limited, Mumbai). Pentylenetetrazole (SRL Pvt Ltd Mumbai)
Solvents:
Various solvents were used for extraction of selected plant material
Table 2: Equipments and their source
|
Materials/Equipments |
Sources/Model |
|
Electronic Balance/ Analytical balance |
Phoenix |
|
Sonicator |
Lab Man Scientifoc Instrument |
|
Ultra-violet Spectrophotometer |
SHIMADZU UV 1900I |
|
Water Bath |
B.R. Instrument |
|
Vaccum filter |
B.R. Instrument |
|
Distillation setup |
B.R. Instrument |
PHYTOCHEMICAL STUDIES
Preparation of Extract
Fresh leaves of Tridax procumben were properly rinsed and air-dried thereafter until constant weight was obtained (about 3 weeks). The dried leaves (99 g) were blended and then macerated in 1500 ml hydroethanol (1: 1) for 48 h. afterwards; the extract was decanted and filtered. The residue was further macerated in 1000 ml hydro ethanol for another 48 h to ensure exhaustive extraction (x 2). The combined filtrate after that distillation was carried out and later on evaporated under reduced pressure at 40°C. The dried extract, with a yield of 35.62%, was reconstituted in distilled water to obtain appropriate concentrations before administration to experimental animals.[50]
The Aqueous extract of Tridax procumben (TPE) was prepared by maceration method using distilled water solvent for 72 hrs at room temperature. A suspension of EECAL in 5% (w/v) Carboxy Methyl Cellulose was prepared for oral administration.


Figure 8: Hydroalcoholic maceration
Preliminary Phytochemical Investigation
The preliminary phytochemical investigations were carried out with Tridax procumben for qualitative identification of phytochemical constituents. [51]
Table 3: Preliminary phytochemical investigations of Tridax procumben
|
Reagents/Solutions |
Composition |
Observation |
|
Test for tannins and phenolic compounds
Ferric chloride test
Bromine water test |
5 mL of 5% ferric chloride solution was added to 0.5 g of Tridax procumben.
0.5 g of Tridax procumben was added to 5 mL of bromine water. |
Appearance of deep blue-black color.
the decoloration of bromine water. |
|
Test for alkaloids Mayer’s test
Wagner’s test
Dragendorff’s test |
5 mL of Mayer’s reagent was added to 0.5 g of Tridax procumben.
5 mL of Wagner’s reagent was added to 0.5 g of Tridax procumben
5 mL of Dragendorff’s reagent was added to 0.5 g of Tridax procumben. |
Appearance of a cream colored precipitated.
Formation of reddish brown precipitated.
Appearance of orange- brown precipitate |
|
Test for flavonoids Lead acetate test
Shinoda test |
0.5 g of Tridax procumben was added to 5 mL of lead acetate solution.
5 mL of 95% ethanol, few drops of concentrated hydrochloride and 0.5 g of magnesium turnings were added to 0.5 g of Tridax procumben. |
Formation of yellow colored precipitated.
formation of a pink color |
|
Test for tannins and phenolic compounds
Ferric chloride test
Bromine water test |
5 mL of 5% ferric chloride solution was added to 0.5 g of Tridax procumben.
0.5 g of Tridax procumben was added to 5 mL of bromine water. |
Appearance of deep blue-black color.
The decoloration of bromine water. |
|
Test for carbohydrates Molish’s test |
5 mL of ?-naphthol solution in alcohol was shaken with 0.5g of Tridax procumben and then 0.5 mL of concentrated sulphuric acid was added carefully down the side of the test tube. |
The formation of a violet ring at the junction of the two solutions indicated the presence of carbohydrates. |
|
Fehling’s test
Benedict’s test |
5 mL each of Fehling’s solution A and B were added to the test tube and boiled for 1 min. 5 g of Tridax procumben was added to this and heated in a boiling water bath for 5- 10 min.
5 mL of Benedict’s reagent and 0.5 g of Tridax procumben were mixed in a test tube and heated in boiling water bath for 5-10 min. |
Appearance of yellow and then brick red precipitate indicated the presence of reducing sugars.
Change in color to yellow, green or red indicated the presence of reducing sugars. |
|
Test for proteins Biuret test
Million’s test |
5 mL of 4% sodium hydroxide and 1% copper sulphate were added to 0.5 g of Tridax procumben.
5 mL of Million’s reagent was added to 0.5 g of Tridax procumben. |
The change in color of solution to violet or pink indicated the presence of proteins.
The appearance of white precipitate changing to brick red on heating indicated the presence of proteins |
|
Test for fixed oil and fats Stain test |
One drop of extract (30% solution in water) was pressed between filter paper. |
Permanent stain in the filter paper indicated the presence of fixed oil. |
|
Test for steroids Salkowski test |
3 mL Chloroform and 1 mL sulphuric acid were added to 0.5 g of Tridax procumben and shaken well. |
Change in color of chloroform layer to red and acid layer to greenish yellow fluorescence. |
The aqueous extract Tridax procumben revealed the presence of alkaloid, flavanoids, tannins, and saponins. Same as aqueous extract the Hydroalcoholic extract Tridax procumben is presence of alkaloid, flavanoids, tannins, and saponins.
THIN LAYER CHROMATOGRAPHY
Samples were eulted with column using silica gel 120 mesh with Chloroform: ethylacetate (10:2) and TLC performed on precoated TLC plates (silica gel 60F-254). Chloroform- methanol-ethylacetate-hexane and acetic acid (10:2:5:1:1) is used as mobile phase. Samples were placed on TLC using capillary tube at the bottom of plate and allowed to dry. The plate is kept under mobile phase and separation of compounds permitted until the solvent reached ¾ the distance and exposed under UV at 365 and 254 nm. [52]
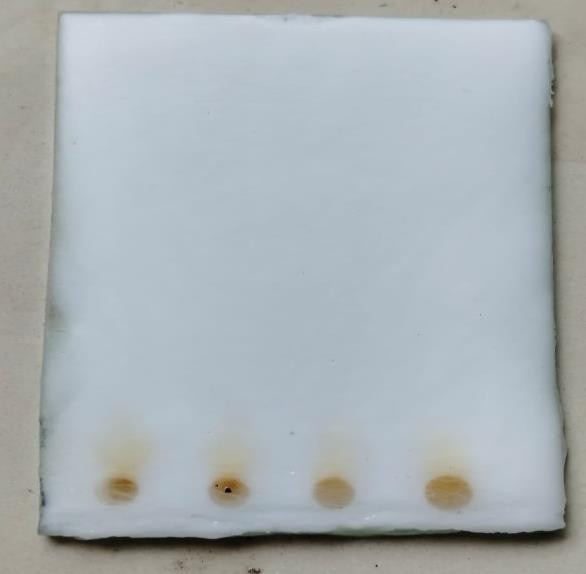
Figure 9: Silica gel TLC Plate
UV–Visible (UV-Vis) spectroscopic analysis
The Hydroalcoholic plant extract of Tridax procumben was examined under UV Visible spectral analysis. The sample was diluted to 1:10 with the same solvent. The extract was scanned in the wavelength ranging from 200-800nm using Perkin Elmer Spectrophotometer and the characteristic peaks were detected. [52]
Figure 10: Digital UV meter
ACUTE ORAL TOXICITY TEST
The acute oral toxicity of Tridax procumben was performed according to Organization for Economic Co-operation and Development (OECD) – 425 guideline (2011) using female, nulliparous and non-pregnant rat weighing 180 – 220 g. Before the experiment animals were fasted for 3hr. Animals was administered a single dose of Tridax procumben and observed for its mortality during 48 h study period (short term toxicity). Different doses of the extract were administered to rat. The dose progression was 2000 mg/kg. The dose, at which mortality was observed in two out of three rats, was considered as toxic dose. The LD50 of the Tridax procumben was calculated using acute oral toxicity (AOT) 425. [53]

Figure 11: Oral dosing of toxicity
4.8. Animals
Swiss albino and Wistar albino rats weighing between 180 – 200 g were procured from Bioneeds, DCS's Annasaheb Ramesh Ajmera College of Pharmacy Nagaon, Dhule for experimental purposes. All the animals were acclimatized for seven days under standard husbandry conditions: room temperature (24 ± 1 oC), relative humidity (45-55%) and a 12:12 h light / dark cycle. Each experimental group had separate set of animals and care was taken to ensure that animals used for one response were not employed elsewhere. Animals were habituated to laboratory conditions for 48 h prior to experimental protocol to minimize any nonspecific stresses. All the experiments were conducted in strict compliance, according to ethical principles and guidelines provided by the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA).
IN VIVO PHARMACOLOGICAL STUDIES:
Elevated Plus Maze (EPM)

Figure 12: Elevated Plus Maze Model
Test The apparatus consists of two open arms (35 × 5 cm) and two closed arms (30 × 5 × 15 cm) that extend from a common central platform (5 × 5 cm). The floor and walls of the closed arms is wooden and painted with white coloured. The entire maze is elevated to a height of 50 cm above the floor level to observe anxiolytic behaviour in rats (number of entries in open arm and time spent in open arm) (Figure 12). Rats were housed in pairs for 10 days prior to testing in the apparatus. During this time the rats were handled alternate days to reduce stress. The animals were treated with control (3% Tween 80, p.o.), diazepam (3 mg/kg, p.o.) and test drug (100, 200 and 400 mg/kg, p.o.). One hour after the treatment, each mouse was placed in the centre of the maze facing one of the enclosed arms. During a five- minute session, the following parameters were noted. Number of entries into open arm and time spent in the open arm. Every time before placing the animal, the arena was cleaned with 5% alcohol to eliminate the possible bias due to the odor left by the previous animal [54, 55,56]. The above procedure was conducted preferably in a sound attenuated room.
Table 4: Grouping of animals for evaluation of anxiolytic activity in EPM
|
Group |
Treatment |
|
I |
Vehicle control: 0.9% saline p.o. |
|
II |
Standard (Diazepam 3 mg/kg i.p.) |
|
III |
Tridax procumben (100 mg/kg p.o.) |
|
IV |
Tridax procumben (200 mg/kg p.o.) |
|
V |
Tridax procumben (400 mg/kg p.o.) |
4.9.2 Pentylenetetrazole (PTZ) Induced Convulsion
Pentylenetetrazole (PTZ) Induced Convulsion
For evaluation of the anticonvulsant activity of Tridax procumben plant, Rats were divided into five groups of six each as follows: Group I received control (3% Tween 80, p.o.), Group II received standard (Diazepam 3 mg/kg, p.o.) Group III, IV, and V received crude extract of Tridax procumben at the dose levels of 100, 200 and 400 mg/kg, p.o. respectively. Thirty minutes after Tridax procumben administration, the rats were injected with PTZ (80 mg/kg). Rats were observed for onset of clonus, tonic and mortality for one hour. Six groups of six mice each were pretreated with Tridax procumben (once daily for 4 days) After 4 days pretreatment with varying doses of Tridax procumben, control (n=6, 3 % Tween 80) and Diazepam (n=6, single dose 3 mg/kg, p.o.). After one hour of the last dose, all the animals were received a Intraperitonial injection of PTZ (80 mg/kg).[57,58,59] Each rats was placed in an individual plastic cage and was observed for 30 min. Rats failing to show clonic seizures lasting longer than 5 s were scored as protected. Protection against mortality was calculated by the following formula

Figure 13: Pentylenetetrazole (PTZ) Induced Convulsion Method
Table 5: Grouping of animals for evaluation of anticonvulsant activity in PTZ
|
Group |
Treatment |
|
I |
Vehicle control: 0.9% saline p.o. |
|
II |
Standard (Diazepam 3 mg/kg i.p.) |
|
III |
Tridax procumben (100 mg/kg p.o.) |
|
IV |
Tridax procumben (200 mg/kg p.o.) |
|
V |
Tridax procumben (400 mg/kg p.o.) |
STATISTICAL ANALYSIS
One way ANOVA followed by Tukey – Kramer’s post hoc test was used for the calculation of statistical significance. The data was represented as mean ± s. e. m. values and n = 6 per group (s. e. m. = standard error of mean)
RESULTS
PHYTOCHEMICAL INVESTIGATIONS
Phytochemical analysis
Results of preliminary phytochemical analysis are given in table 6. It shows that aqueous and Hydrolalcoholic extract of whole plant of Tridax procumben. Aqueous extract Tridax procumben revealed the presence of alkaloid, flavanoids, tannins, and saponins. Same as aqueous extract the Hydroalcoholic extract Tridax procumben is presence of alkaloid, flavanoids, tannins, and saponins.
Table 6: Result of Phytochemical screening of Aqueous and Hydroalcoholic extract of Tridax procumbens
|
Category |
Name of the test |
Aqueous Extract |
Hydroalcoholic Extract |
|
Alkaloids |
a) Mayer’s test |
+ |
+ |
|
b) Wagner’s test |
+ |
+ |
|
|
c) Dragendorff’s test |
+ |
+ |
|
|
Flavonoids |
a) Sulphuric acid test |
+ |
+ |
|
b) Zinc +HCL+T.S |
+ |
+ |
|
|
Phenolics &Tannins |
a) Ferric chloride test |
+ |
+ |
|
b) Dil.iodine solution |
+ |
+ |
|
|
Carbohydrates |
a) Molish’s test |
-- |
-- |
|
b) Fehling’s test |
-- |
-- |
|
|
c) Benedict’s test |
-- |
-- |
|
|
Fixed oil and Fats |
a) Stain test |
-- |
-- |
|
Saponins |
a) Froth test |
+ |
+ |
|
Steroids |
a) Salkowski test |
-- |
-- |
|
b) Liebermann Burchard test |
-- |
-- |
-- = Negative (absent) + = Positive (present)
CHROMATOGRAPHIC ANALYSIS
6.2.1: Thin Layer Chromatography
Thin layer chromatogram of Hydroalcoholic extract of Tridax procumbens was given in plate and TLC of Hydroalcoholic extract of Tridax procumbens revealed the presence of a spot having Rf value of 0.70-0.72 when a solvent phase of Chloroform, ethanol, ethylacetate, hexane and acetic acid in the ratio of (10:2:5:1:1) a solvent system was used.
The TLC analyses took 25 min to complete the 12 cm run of the solvent.while the solute Tridax procumben run about 7 cm. Spots of Tridax procumben appeared.The spots had dark bluish-violet color on a yellow-light brown background, with Rf in the range 0.70-0.72 (Figure 13).
Rf value = Distance travel by solute Distance travel by solven

Figure: 14 TLC plate of hydroalcoholic extract of Tridax procumbens
6.3. UV – Visible Spectroscopy of Tridax procumbens
UV spectroscopy is a form of absorption spectroscopy, in which the molecule absorbs light from the ultra-violet region (200-800 nm).
UV-VIS analysis preformed for identification of phyto-chemicals found in Hydroalcoholic extract of Tridax procumben. In Hydroalcoholic, the UV absorbance of the isolated chemical was measured throughout a scanning range of 200-800 nm. To acquire the desired concentration, the chemical was dissolved in Hydroalcoholic and the spectra were recorded. The UV spectra of the isolated F3 elute showed spectral maxima at 360 nm. The typical UV Vis spectra of elute include single absorbance band. Band lies in the 250-360 nm range for Flavonoids. Thus, the UV spectra showed that the compound may belong to Flavonoids category. The UV/Vis spectrum obtained was also in agreement with published UV spectrum of Flavonoids.
Figure 1: UV Spectral analysis of Hydroalcoholic extract of Tridax procumbens
6.4 Acute Toxicity Studies
The acute oral toxicity of Tridax procumben was performed according to Organization for Economic Co-operation and Development (OECD) – 425 guideline (2011). In the first phase of the acute toxicity studies, there were no remarkable signs of toxicity observed at 100 mg/kg dosage, while at 2000 and 1000 mg dosages, there were however salivation, rubbing at site of application, nose and mouth on the floor of the cage and restlessness. In the second phase of the study, the signs of toxicity observed were same and more severe than those observed at the phase one. all animal survived at 2000 dose was calculated to be 2000mg/kg dosage as geometric means on the doses for which there is zero mortality (0/3) and total mortality (0/3).
PHARMACOLOGICAL STUDIES
Elevated Plus Maze (EPM) Model
Test Anxiolytic effect of Hydroalcoholic extract of Tridax procumben using Elevated Plus Maze test (EPM)
In the EPM, control 3 % Tween 80 vehicle treated rats had a tendency to prefer to stay in the closed arm for a longer period of time than in the open arm. Treatment with diazepam (3 mg/kg) increased the number of open arm entries, and time spent in the open arm suggests that diazepam produces anxiolytic activity, which is in accordance with the earlier findings. [73]
Tridax procumben produced a dose dependent increase in time spent in open arm along with an increase in number of open arm entries. Tridax procumben at a dose of 200 and 400 mg/kg significantly (p<0.001) increased the number of entries (11.67+0.45 and 14.5+0.45) and time spent into the open arm (38.67+0.44 and 50.67+9.85). The magnitude of the anxiolytic effects of 200 mg/kg and 400 mg/kg of Tridax procumben was comparable to that of diazepam 3mg/kg (Table: 7).
Table 7: Effect of Tridax procumbens. on elevated plus maze test
|
Drug |
Number of open arms (sec) entries |
Number of total arm entries |
Percentage ratio of open/total arm entries |
Time spent in open arms (Sec) |
Time spent in closed arms (Sec) |
|
control |
5 ± 0.32 |
8 ± 0.34 |
8.20% |
21.22± 0.137 |
56+0.67 |
|
Standard (Diazepam 3 mg/kg i.p.) |
18.17 ± 0.965 |
21.17 ± 0.65 |
42.26% |
57.67 ± 1.410 |
24.83 ± 1 |
|
TP (100 mg/kg p.o) |
8 ± 0.327 |
10 ± 0.81 |
17.27% |
27.33 ± 1.252 |
38.33 ± 1.20 |
|
TP (200 mg/kg p.o) |
11.67 ± 0.45 |
14.33 ± 0.38 |
25.83% |
38.67 ± 0.44 |
33.5 ± 1.14 |
|
TP (400 mg/kg p.o) |
14.5 ± 0.45 |
53.83 ± 0.99 |
37.93% |
50.67 ± 9.85 |
23.67 ± 0.51 |
values are expressed as mean r SEM from 6 mice. Significant at **P < 0.01 and ***P < 0.001 as compared to control group using one way ANOVA followed by Tukey – Kramer’s post hoc test.
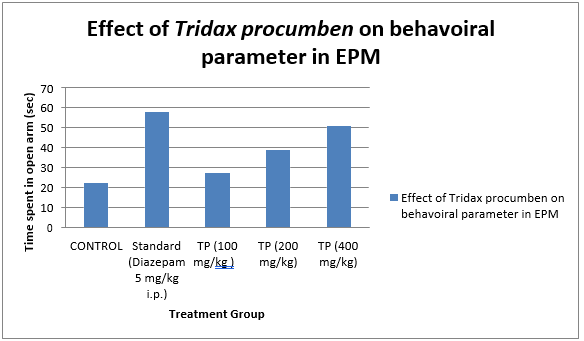
Figure 2: Effect of Tridax procumben on behavioural parameter in EPM
EVALUATION OF ANTICONVULSANT ACTIVITY
Pentylenetetrazole (PTZ) Induced Convulsion
Tridax procumben at the doses of 100, 200 and 400 mg/kg showed alteration in the onset of tonic – clonic seizures compared to control group animals and also showed protection against PTZ induced mortality in a dose dependent manner (Table: 8 and Figure 15). The convulsions were completely abolished by Diazepam (3 mg/kg).
Table 8: Effect of TP on pentylenetetrazole induced convulsion
|
Treatment |
Onset of Clonus (Sec) |
Onset of Tonic (Sec) |
% Protection against mortality |
|
Vehicle control: 0.1% Na CMC or 0.9% saline |
46.33 ± 0.416 |
363.33 ± 1.05 |
0 |
|
Standard (Diazepam 3 mg/kg i.p.) |
Not observed |
Not observed |
100 |
|
TP (100 mg/kg p.o ) |
166.83 ± 1.184 |
386.83 ± 1.184 |
51% |
|
TP (200 mg/kg p.o ) |
246.33 ± 0.416 |
546.33 ± 3.82 |
20% |
|
TP (400 mg/kg p.o ) |
279.83 ± 0.823 |
665.67 ± 0.796 |
100 |
Values are expressed as mean r SEM from 6 rats. Significant at **P < 0.01 and ***P < 0.001 as compared to control group using one way ANOVA followed by Tukey – Kramer’s post hoc test.
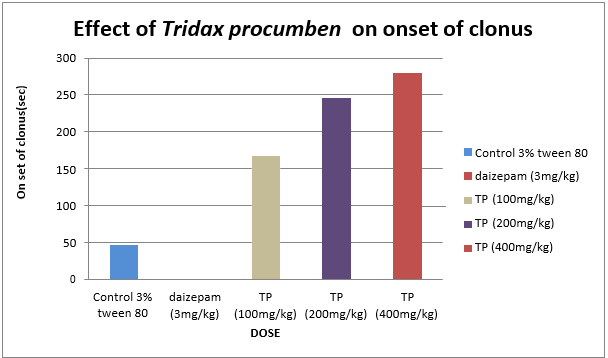
Figure: 3 Effect of Tridax procumben on onset of clonus
It is well documented that PTZ induced convulsions are produced due to diminution of GABA level in brain. Pentylenetetrazole is a central nervous system stimulant. It produces a jerky type of clonic convulsions in rats. The convulsive effect of this drug is considered to be analogous to petit mal type of convulsions in man. The PTZ test is assumed to identify anticonvulsant drugs effective against generalized clonic seizures [58,60].
BZ receptors may be primarily involved in the convulsant action of PTZ. Hence, there may be a possible predominant involvement of ?2-containing GABAA receptors in the convulsant action of PTZ. Tridax procumben was able to effectively inhibit the convulsion against PTZ induced convulsion model with ED50 value of 81.04 suggesting TP may be effectively inhibit the petit mal type of convulsion and generalized seizure.[61]
DISCUSSION
Behavioral response is related to the actions or reactions of an animal or humans usually in relation to the environment. In mammal this behavior is controlled by endocrine and central nervous system whereby complexity of behaviour of mammals is a function of complexity of its nervous system. Neuropsychiatric diseases like depression and anxiety represents aberrations from normal behaviour. Abnormal emotion is also frequently seen in other neuropsychiatric and neurological diseases like epilepsy and Alzheimers disease.
Phytochemical screening revealed the presence, in both extracts, of phytosterols, proteins, reducing sugars, carbohydrate, tannins, phenols, saponins, free amino acids and arginine except flavonoids which were present only in the water extract.
Our findings demonstrated that Tridax procumben leaf extracts have anticonvulsant effects on PTZ model of epilepsy in rats. Tridax procumben extract at a dose of 400 mg/kg decreased seizure latency, while the Hydroalcoholic extract significantly reduced the severity of seizures. Pretreatment with Tridax procumben extracts protected the animals against PTZ induced death seizures with the percentage of seizure protection highest at 400 mg/kg. The medicinal value of plants lies in some chemical substances (phytochemicals) that have a definite physiological action on the human body. [62] The observed anticonvulsant activity in this study can be attributed to Tridax procumben extract. PTZ exerts its convulsant effects by inhibiting the activity of gamma amino butyric acid (GABA) at GABA-A receptors. [63] GABA is a major inhibitory neurotransmitter, which is implicated in epilepsy. The enhancement of GABA neurotransmission attenuates convulsions while inhibition of the neurotransmission of GABA enhances convulsions.[64] Diazepam is a known conventional antiepileptic agent that generally inhibits sodium currents and enhances GABA transmission. As expected, diazepam (3 mg/kg, i.p.) pretreated rats did not have any convulsive episode or show any mortality when treated with PTZ. Since the extracts showed anticonvulsant effect against PTZ induced seizures, it is probable that they may be interfering with GABA transmission to exert their anticonvulsant effect. This is in agreement with findings of studies carried out by who found out that alkaloids, flavonoids, terpenoids, saponins, and coumarins enhance GABA transmission.[65] Therefore, flavonoids and saponins may be responsible for the anticonvulsant activity observed in this study. The elevated plus maze is considered to be an etiologically valid animal model of anxiety. The number of entries and time spent in the open arms have been found to be increased and it reduced by anxiogenic agents. The elevated plus maze is considered to be an etiologically valid animal model of anxiety. The number of entries and time spent in the open arms have been found to be to be increased and it reduced by anxiogenic agents. The elevated plus maze is considered to be an etiologically valid animal model of anxiety. The number of entries and time spent in the open arms have been found to be increased by anxiolytics and reduced by anxiogenic agents. Tridax procumben showed anxiolytic activity at a higher dose of 400 mg/kg however, such activity was not observed at lower doses (100 and 200 mg/kg) compared to the control. Animals spent more time in the closed arms and made fewer entries into the open arms compared to the control, at lower doses, as locomotor activity could have been impaired following after Tridax procumben extract administration.[66] Available literature reports describe the action of benzodiazepines, such as diazepam, as anxiolytics (at low doses) and as anticonvulsants, also producing sedation and myorelaxant effects at higher doses.[67] Reduction in the locomotor activity by Tridax procumben in the elevated plus maze test may be correlated with central nervous depression. This was probably because the dose of diazepam used in this study (3 mg/kg) was higher than that of (1 1mg/kg).In various studies, flavonoids have been shown to have antianxiety activity.[68]
The anxiolytic effect of flavonoids has been attributed to its effect on benzodiazepine receptors and central nervous system Therefore, [69] flavonoids may be responsible for the anti-anxiety activity observed in this study. This study provides experimental support for the traditional medicinal use of this plant for the management of epilepsy and anxiety. showed anxiolytic activity at a higher dose of 400 mg/kg however, such activity was not observed at lowered doses (100 and 200 mg/kg) compared to the control. Animals spent more time in the closed arms and made fewer entries into the open arms compared to the control, at lower doses, as locomotor activity could have been impaired following after Tridax procumben extract administration.
CONCLUSION
The present research aimed to establish a new principle for treating anxiety and convulsions. To achieve this, approximately 130 plants were reviewed, and Tridax procumben was selected due to its traditional use as a brain tonic, despite lacking scientific validation. This study aimed to provide scientific documentation and pharmacological validation to support the traditional practice of indigenous medicines.
The present work deals with Pharmacognostic, phytochemical and pharmacological investigation for anxiolytics and Antiepileptic activity of plant belongs to Asteraceae family i.e. Tridax procumben Literature review reveals that traditionally these plants are being used in the treatment of CNS disorder. The hydroalcoholic and aqueous extracts of Tridax procumben were prepared and subjected to phytochemical screening. The results revealed the presence of various bioactive compounds, including flavonoids, carbohydrates, proteins, fixed oil, fats, saponins, phytosterols, triterpenoids, phenolic compounds, and tannins.
The LD50 value of TP was found to be 2000 mg/kg whereas, TP did not produce any mortality even at 2000 mg/kg till 14 days. Besides, the extract could have few quantities of toxic substances which could have caused the death of the animals. Purification could have removed those toxic substances making the compound to be safer.
By investigating the pharmacological potential of Tridax procumben, this study provides a scientific basis for its traditional use, potentially leading to the development of new treatments for anxiety and convulsions. Examined for anxiolytic and anticonvulsant activities, Tridax procumben was subjected to the elevated plus maze test for determination of anxiolytic activity and pentylenetetrazole induced convulsion for screening the anticonvulsant activity. It showed a promising result for both activities. Hence, it was decided to proceed with the detailed study by isolating the major compound from TP. The LD50 value of TP was found to be 2000 mg/kg whereas, TP did not produce any mortality even at 2000 mg/kg till 14 days. Besides, the extract could have few Purification could have removed those toxic substances making the compound to be safer.
Bioactivity directed isolation and characterization of the anxiolytic constituent from the ethanolic extract of heart wood of Tridax procumben could be an inspiration of new prototypes for drug development. quantities of toxic substances which could have caused the death of the animals.
REFERENCES


Priyanka Gaikwad, Utkarsh Mandage, Evaluation Of Anxiolytic and Anticonvulsant Effects of Tridax Procumbens in Rodent Models, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 556-590. https://doi.org/10.5281/zenodo.14994631
 10.5281/zenodo.14994631
10.5281/zenodo.14994631
