1PES Modern College of Pharmacy, Moshi, Pune Maharashtra, India 412105
2S. B. Patil College of Pharmacy, Vangali, Indapur, Pune, Maharashtra, India 413106
3College of Pharmacy (poly) Akluj, Solapur, Maharashtra, India 413101
4DKSS’s Institute of Pharmaceutical Science and Research (for Girls), Swami-Chincholi, Pune, Maharashtra, India 413130
5Chetana Foundation’s Chetana College of Pharmac, Sardewadi, Indapur, Pune, Maharashtra, India 413106
One of the most prevalent non-communicable diseases in the world is "diabetes mellitus." India has a number of issues with managing diabetes, such as a growing incidence in both urban and rural regions, a lack of public awareness of the condition, a shortage of healthcare facilities, high treatment costs, and poor glycaemic management and the increasing incidence of complications from diabetes. The most popular method of administering insulin therapy for diabetes is subcutaneous injections, which can occur up to four times daily. Because of problems with patient compliance and the intrusive nature of its administration, long-term insulin therapy has a detrimental effect on patient outcomes. Although type 1 diabetes has becoming more common, type 2 diabetes mellitus remains the main causes almost 90% of all cases of diabetes and is a contributing factor to the diabetes epidemic.A hazardous and common chronic illness that arises from a complex interplay between genetics and environment, together with extra risk factors like obesity and inactive lifestyle. Whereas smoking, alcohol consumption, obesity, ageing, and inadequate energy intake are significant risk factors for the development of type 2 diabetes mellitus; yet, the decline in pancreatic cell function over time is evident.
What is Diabetes mellitus?
Define:
Diabetes mellitus is a disorder in which the body does not produce enough or respond normally to insulin, causing blood sugar (glucose) levels to be abnormally high. Diabetes mellitus is a long-term disease affecting the proteins, lipids, and carbs are breaks down. Diabetes mellitus is defined by an inadequate or lack of insulin response, which results in impaired utilisation of carbohydrates (glucose), as well as resulting hyperglycaemias. [1] Diabetes mellitus (DM), also referred to as "sugar," is the most commonly endocrine situation which usually occurs due to an insufficient or insufficient amount of insulin or, sometimes, due increased function of insulin (insulin resistance)[2].
The pancreas secretes the hormones glucagon and insulin. The islets of Langerhans contain beta (ß) cells that release insulin and alpha (α) cells that secrete glucagon. Insulin transports glucose into the skeletal muscles, liver, and adipose tissue while lowering blood glucose levels through glycogenesis. While erythrocytes and neural tissue do not require insulin to use glucose, alpha (α) cells are crucial for blood glucose regulation because they produce glucagon, which raises blood glucose levels by speeding up glycogenolysis. Diabetes mellitus is a chronic illness that alters the metabolism of carbs, fats, and proteins. Another of the symptoms of diabetes mellitus is a low or insufficient insulin secretory response, which results in impaired glucose utilisation and the related hyperglycaemias.[3] Diabetes mellitus, commonly referred to as "sugar," is the more common kind of the disease. Endocrine condition that often manifests as an insulin deficit or deficiency, but on occasion, insulin action can be impeded by insulin resistance [4]. Diabetes mellitus is one of several metabolic diseases that share the symptom of hyperglycemia. Deficits in insulin production, action, or—more commonly—both can result in diabetes-related hyperglycemia. Numerous organ systems may sustain secondary damage as a result of the metabolic dysregulation caused by the persistent hyperglycemia, especially in the kidneys, eyes, nerves, and blood vessels. A lack of insulin, an issue with how insulin functions, or both can cause diabetes mellitus, a group of several diseases that often present with episodes of hyperglycemia and glucose intolerance. The most common endocrine disorder, sometimes called "sugar," is one in which there is either no insulin at all or insufficient insulin, or less commonly, reduced insulin activity (insulin resistance). Since there is currently no treatment for diabetes, the chance of developing long-term problems from the disease can be reduced by managing blood sugar levels with medication, exercise, and a nutritious diet. The following are examples of long-term complications: - kidneys - kidney disease and renal failure - eyes - cataracts and retinopathy (gradual damage of the eye) that may result in blindness - nerves - neuropathy (slow nerve damage) - feet: gangrene, ulcers, infections, etc. cardiovascular system, including heart disease, stroke, and arterial stiffening (Heart Foundation,2003).
In 2014, 8.5 percent of adults over the age of 18 had diabetes. 48 percent of all diabetes-related deaths in 2019 happened before the age of 70, making diabetes the direct cause of 1.5 million deaths. Premature mortality rates (death before age 70) increased by 5% as a result of diabetes between 2000 and 2016. In high-income countries, the premature mortality rate from diabetes decreased between 2000 and 2010, but then increased between 2010 and 2016. Premature mortality from diabetes rose in lower-middle-income countries over both periods. The probability of dying from any of the four main non-communicable diseases (diabetes, cancer, chronic respiratory conditions, or cardiovascular diseases) among people aged 30 to 70 decreased by 18% worldwide between 2000 and 2016.
HISTORY
The distant past "Diabetes mellitus" is a combination of the Greek term "diabetes," which means "to pass through," and the Latin word "mellitus," which means "sweet." The term "diabetes" was first used in 230 BCE by the Greek Apollonius of Memphis, which means "to pass through." According to an Egyptian text from 1500 BCE, diabetes had a "very considerable emptying of the urine" and was one of the first diseases to be given a name. The earliest instances reported are believed to have had type 1 diabetes. At about the same time, Indian physicians identified the illness and called it "honey urine," or madhumeha, after observing that the pee attracted ants. In 400–500 BCE, the Indian physicians Sushruta and Charaka made the first distinction between two types of diabetes as separate illnesses.
CLASSIFICATION:
The classification includes additional types of hyperglycemia as well as the clinical stages and etiological types of diabetes mellitus. Diabetes mellitus is likely a diverse group of disorders with hyperglycemia as a common feature. Diagnosing a person with diabetes frequently depends on the circumstances at the time of diagnosis, and many diabetics do not readily fit into a single class [5].
This form of diabetes mellitus, once referred to as juvenile-onset or ketosis-prone diabetes, is currently categorised as autoimmune diabetes. The individual may also seek assistance from others. IDDM, or insulin-dependent diabetic mellitus, is a term used to describe autoimmune diseases such as Hashimoto's thyroiditis and Graves' Addison's disease, thyroiditis, and a type of diabetes that primarily affects children and young adults. The onset of these conditions is typically unexpected and may be fatal. Type 1 usually One distinguishing property is anti-glutamic acid. Type 1 diabetes, which is caused by the loss of beta-cells, usually results in total insulin insufficiency. Decarboxylase, islet cell, or insulin antibodies are autoimmune reactions that cause beta-cell death. (American Diabetes Association, 2014). varying people experience beta-cell degeneration at varying rates; some experience it rapidly, while others experience it more slowly. or insufficient insulin production due to ß-islet cell destruction in the pancreas. Injections of insulin are required for treatment. [6]
Adult-onset diabetes is another name for type 2 diabetes mellitus. Insulin resistance is the backdrop for the increasing insulin secretary malfunction (American Diabetes Association, 2014) [7]. Insulin resistance is common in patients with this kind of diabetes [8]. Both forms of diabetes have long-term problems with the kidneys, blood vessels, eyes, and nerves, which are the main reasons for morbidity and mortality [9]. Predisposing factors include obesity, sedentary lifestyles, ageing (affecting middle-aged and older individuals), and genetic factors (Ross and Wilson 2010). These factors raise the risk of both macrovascular and microvascular problems in these patients [10,11].
Gestational diabetes mellitus (GDM) is the phrase used to characterise the onset or diagnosis of glucose intolerance during pregnancy. Gestational Type 2 Diabetes (GDM) is the term used to describe women with Type 1 diabetes who develop diabetes mellitus during pregnancy and unexplained Type 2 diabetes mellitus that is asymptomatic during pregnancy. Diabetes is definitely finished for pregnant women with type 1 diabetes (GDM), often known as uncontrolled pregnancy-related diabetes. During pregnancy, diabetes mellitus A number of problems may appear during pregnancy and then go away. Children born to mothers with GDM have a higher chance of acquiring type 2 diabetes and obesity over a prolonged period of time. Exposure to elevated blood sugar levels during pregnancy is associated with the phenomena known as life [12].
Mutations in a hepatic transcription factor called hepatocyte nuclear factor (HNF)-1a on chromosome 12 cause the most prevalent kind of monogenic diabetes.They are also known as beta cell genetic deficiencies. The early onset of hyperglycemia (usually before the age of 25) is a common characteristic of several types of diabetes. Other names for them include: people with exocrine pancreatic diseases like pancreatitis or cystic fibrosis; people with dysfunction linked to other endocrinopathies (like acromegaly); people with pancreatic dysfunction brought on by drugs, chemicals, or infections; and people with maturity-onset diabetes of the young (MODY)[13], maturity-onset diabetes in youth, or defects of insulin action [14].
Certain medications are also used in conjunction with HIV/AIDS treatment or following organ transplantation. A few families have been found to have genetic defects that cause the inability to convert proinsulin to insulin; these features are inherited in an autosomal dominant form. Less than 10% of DM cases involve them [15].
This and other collective evidence have been used to divide diabetes mellitus into four distinct types namely;
• Insulin dependant diabetes,
• Non-insulin dependant diabetes,
• Malnutrition-related diabetes,
• Secondary /other types of diabetes:
It is due to certain pancreatic disesase or certain genetic syndrome or may be drug induced.
PATHOPHYSIOLOGY
Type 1 diabetes mellitus:
once known as juvenile-onset diabetes or diabetes that is prone to ketosis. One may also pursue other autoimmune conditions such as Addison's disease, Hashimoto's thyroiditis, and Graves' disease [16]. Children and young adults are the main populations affected by insulin-dependent diabetes mellitus (IDDM), commonly referred to as type I diabetes. It can be lethal and usually manifests suddenly [17]. Autoimmunity in Type 1 Diabetes is caused by invasive macrophages and CD4+ and CD8+ T lymphocytes attacking the pancreatic cells that produce insulin [18]. The autoimmune loss of pancreatic beta-cells results in insufficient insulin synthesis, which in turn causes the metabolic abnormalities linked to type 1 diabetes. Individuals with type 1 diabetes do not make insulin.
Without insulin, muscle and adipose cells cannot get the glucose they require for energy. Glycogenolysis and gluconeogenesis are triggered when muscle and adipose tissues are starved of glucose, causing an excess of glucagon to be produced. Hyperglycemia decreases glucagon secretion in healthy individuals, however it has no effect on glucagon secretion in T1DM patients [19]. The resulting excessively elevated glucagon levels exacerbate the metabolic problems caused by insulin deficiency. Blood sugar levels rise. The kidneys are unable to absorb the ever-increasing glucose, therefore the excess is excreted in the urine (polyuria). The brain expresses hunger and thirst (polydipsia) as a result of this fluid loss (polyphagia).
The liver will break down stored lipids and produce keto acids if this process persists.Lower pH levels and acidosis are the results of this. A number of other autoimmune diseases, including myasthenia gravis, Addison's disease (primary adrenal insufficiency), coeliac sprue (coeliac disease), pernicious anaemia, vitiligo, Hashimoto's thyroiditis, Graves' disease, and dermatomyo, have been found to be more common in patients with type 1 diabetes in addition to the usual immune-mediated destruction of pancreatic beta-cells [20,21,22,23].
Type 2 diabetes mellitus:
T2DM, also known as non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes. This kind of diabetes is characterised by two main insulin-related abnormalities: insulin resistance and -cell dysfunction. In contrast to type 1 diabetes, no link has been found between disease and immune response-related genes, such as autoimmunity, and hence, there is no immune-mediated pancreatic cell death. [24, 25]
If there are no major physiological stressors in their lives, patients with type 2 diabetes often do not require insulin therapy at the onset of their condition or even later on. (26, 27, 28) T2DM has been more frequently associated with ageing, obesity, a family history of diabetes, physical inactivity, and modern lifestyle choices. Type 2 diabetes develops when the pancreatic beta cells are unable to generate enough insulin to meet metabolic needs.
Additionally, as adipose cells proliferate in the patient's muscle and liver, Type 2 diabetes acquires a significant characteristic of insulin resistance. People with more adipose deposition, who frequently have higher body fat percentages and obese BMIs, are therefore more likely to have type 2 diabetes. Because type 2 diabetes is strongly linked to increased body fat content or obesity (HDLs), patients with the disease often have multiple cardiovascular risk factors, including hypertension and lipoprotein metabolic abnormalities, which are characterised by elevated triglycerides and decreased numbers of high-density lipoproteins.
Gestational diabetes mellitus:
"Gestational diabetes mellitus" is the term used to describe any type 2 diabetes that goes undiagnosed, as well as any level of glucose intolerance or diabetes that may develop during or before pregnancy. (29, 30) When blood glucose levels rise to diabetic levels during the third trimester of pregnancy, it is known as gestational diabetes mellitus (GDM). Both the postprandial and fasting blood glucose levels in the early stages of pregnancy
SIGN AND SYMPTOMS
Because they are unable to properly metabolize glucose, cells with diabetes mellitus essentially starve. Long-term consequences of diabetes mellitus include increased development of specific retinopathy issues with potential blindness, nephropathy and neuropathy that cause renal failure, Charcot joint, and foot ulcer risk, as well as sexual dysfunction and autonomic dysfunction.
I. Gluconeogenesis from amino acids and body protein results in muscle atrophy, tissue degradation, and an increase in blood glucose levels, among other symptoms.
II. Excess ketone body production and the breakdown of body fat, which releases some of its energy [33].
Type 1 diabetes mellitus:
The nausea, vomiting, or stomach discomfort are possible symptoms for those with type 1 diabetes. A few weeks or months can be all it takes for type 1 diabetes symptoms to worsen.
Type 1 diabetes usually appears in children, adolescents, or young adults, while it can occur at any age.
Type 2 diabetes mellitus:
The signs of type 2 diabetes may not appear for years. Others rarely have any symptoms at all. Type 2 diabetes typically impacts adults first, however it is more common in adolescents and teenagers. Identifying the risk factors is crucial because type 2 diabetes has mild signs. Make sure to consult your physician if you encounter any of these symptoms.
The amount of raised blood sugar affects the symptoms of diabetes mellitus. Some people may not always have symptoms, particularly those with non-insulin dependent diabetic mellitus or pre-diabetes.
Symptoms of insulin-dependent diabetes mellitus are often more severe and appear more soon.
High blood sugar (hyperglycemia)
Increased ketones in your urine (diabetic ketoacidosis)
Hyperglycemic hyperosmolar nonketotic syndrome
Low blood sugar (hypoglycemia)
Irritability
Frequent infections, such as gums or skin infections and vaginal infections
Frequent urination
Unexplained weight loss
Polyphagia (excessive hunger)
RISK FACTORS OF DIABETES MELLITUS
The several risk factors have been associated with the developmentof diabetes. The risk factors differ depending on the type of diabetes you ultimately develop.
Physical stress (such as surgery or illness).
Injury to the pancreas (such as by infection, tumor, surgery or accident).
Presence of autoantibodies (antibodies that mistakenly attack your own body’s tissues or organs).
Damage to the pancreas (such as by infection, tumor, surgery or accident).
Exposure to virus-based diseases or Prediabetes
Lack of physical activity
Gestational diabetes, or giving birth to a child who weighs more than 9 pounds are all risk factors.
Being affected by polycystic ovarian syndrome.
Having had a heart attack or a stroke in the past.
Having smoked.
High blood pressure.
Family history (parent or sibling) of type 2 diabetes.
Overweight.
Heart disease or stroke.
Smoking
· Having low levels of HDL cholesterol (the "good" cholesterol) and high triglyceride levels. Being 45 or older and Lack of physical activity.
The overweight before the pregnancy.
Family history (parent or sibling) of type 2 diabetes.
Age above the 25 years.
CAUSES OF DIABETES MILLITEUS
The pancreas (a small gland behind your stomach) usually produces insulin, which transfers any glucose out of your blood and into your cells, where it’s converted to energy.
People with insulin resistance often have a group of conditions including high blood sugar, high blood pressure, and high cholesterol and triglycerides
TREATMENT
The goal of treatment is to address the triggering factor and administer frequent, high doses of insulin. Once the condition is under control, the insulin need returns to normal. The following strategies can help manage diabetes mellitus:
1. To return the diabetic's disrupted metabolism as close to normal as is safe and comfortable.
2. To stop or slow the development of the disease's immediate and long-term risks.
3. To give the patient the information, inspiration, and resources they need to carry out this self-enlightened care.
Hypoglycemic Agent: [46]
They are used to treat Diabeteus mellitus {latin word mellitus means Honey} Diabetus mellitus is characterized by persistant hyperglycemia usually with glycosuria.
They different factors involved in its origin & heredity, immunology, age, stress etc. during which either endogenous insulin secreation is reduced or action of insulin is opposed the lack or deficiency of insulin affects carbohydrates, proteins & lipid metabolism.
As a result different symptoms (manifestation) observed are Hyperglycemia, Glycosuria, Ketonanemia, Ketonuria, Hyperlipidemia, Polyuria, Polydipsia(increased thirst) etc.
Insulin:
It is a harmone produced by β-cells of islets of Langerhans of pancreas. It is polypeptide containing 51 amino acids arranged in 2 chains namely A & B having 21 & 30 amino acids respectively.
These 2 chains are connected by 2 disulphidebridge(-s-s- bonds of cysteine)
Source- Pancreas of Pig or OX
Procine insulin different from human insulin in only one 1 amino acid in ‘B’ chain.
Bovine insulin different from human insulin in 2 amino acids in ‘A’ chain & 1 amino acid in ‘B’ chain.
Human insulin is produced either by enzymetic modification of procaine insulin or by use of DNA recombinant technology in micro-organisms so that amino acid sequence is identical to that of human insulin.
There are four major types of insulin:
1. Rapid-acting
2. Short-acting
Intermediate-acting
Long-acting
There is no standard insulin dose as it depends on factors such as your body weight, when you eat, how often you exercise and how much insulin your body produces.
When oral medication does not manage blood sugar levels in patients with type 1 or type 2 diabetes, insulin injections are administered.
· Short-acting insulin:This type of insulin, often known as normal insulin, begins to function about 30 minutes after injection. It lasts for around 4 to 6 hours, reaching its full effect at 90 to 120 minutes.
· Rapid-acting insulin: This kind of insulin begins to function within 15 minutes. It has a peak effect after 60 minutes and lasts around 4 hours. This kind is frequently taken 15 to 20 minutes prior to meals.
· Intermediate-acting insulin: This form of insulin, also known as NPH insulin, begins to operate within one to three hours. It has its full effect between 6 and 8 hours into its 12- to 24- hour duration.
· Long and Ultra-long acting insulin: This kind of insulin may offer protection for up to 14 to 40 hours.
Properties-
Stability & Storage:
It is sensitive to heat & light & hence it is stored in well closed containers at a temperature not exceeding 200C. It should be stored in refrigerator (2-80C) & used within short time.Insulin injection is stored in multidose containers at a temperature between 20C & 80C & should not be allowed to freeze.
The label on the container should bear:
Hypoglycemic medications are used to treat diabetes mellitus by reducing blood glucose levels. All other hypoglycemic drugs, also known as oral hypoglycemic drugs or oral antihyperglycemic drugs, are taken orally, with the exception of insulin, exenatide, liraglutide, and pramlinited.
Examples.
· Sulfonylurea’s
(Tolbutamide, chlorpropamide, Glibenclamide (Glyburide), Glipizide, Gliclazide, Glimepride ).
· Biguanides
(Phenformin Metformin Meglitinide Analogues Repaglinide Nateglinide).
· Thiazolidinediones (Rosiglitazone Pioglitazone)
· α Glucosidase inhibitors (Acarbose Miglitol).
Due to growing research in traditional medicine, plant-based medications that are eco-friendly, bio-friendly, affordable, and generally safe have emerged from the fringe to the mainstream in recent decades. The review by Atta-ar-Rahman, who has listed over 300 plant species recognised for their hypoglycemic qualities, is the most instructive of the many literature reviews on anti-diabetic herbal compounds written by various writers.The plants in this review have been categorised based on their botanical name, country of origin, parts used, and active agent type. Momordica charantia, a member of the Cucurbitaceae family, is one such plant [31]. 21,000 plants that are used medicinally worldwide have been listed by the WHO. Of these 2500 species, 150 are employed on a reasonably considerable scale for commercial purposes in India. India, known as the botanical garden of the globe, is the world's largest producer of medicinal herbs [32].
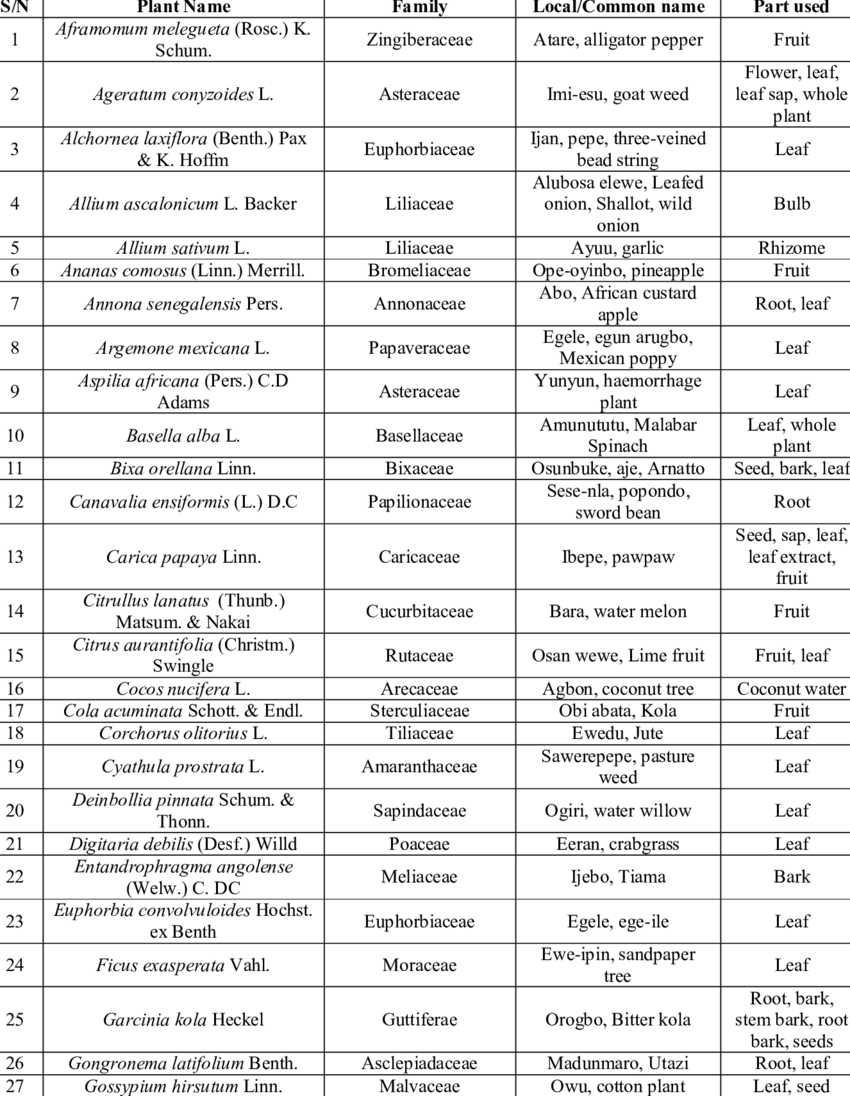
Table. no.1. Plant used for treat diabetic mellitus
DIETARY MANAGEMENT AND PHYSICAL ACTIVITY
The first steps in lowering blood sugar levels for a diabetic patient are usually dietary adjustments and increased physical activity. To educate patients about the nutritional value of food, how to cook healthily, how to exercise, and Consumption of food should be split up into meals of comparable sizes that are spread out regularly. When a diabetic patient's diet of protein, carbohydrates, and lipids is balanced, it is always vital to limit their intake of carbohydrates.
Sufficient calorie content Both diabetic and non-diabetic patients should follow dietary guidelines, such as:
1. Balanced in regard to protein, carbohydrate and fats, in allcases it is necessary to restrict carbohydrate intake.
2. Should conform as closely as possible to normal
3. Food intake should be divided into regularly spaced mealsof similar size
4. Reduce total calorie intake by decreasing both fat andcarbohydrate
5. Patient must be advised to be constant in his dietary habitsfrom day to day.
1. Even if you are feeling well, take your diabetic and other medical medications.
2. Cuts, blisters, red areas, and swelling should all be checked on a daily basis.
3. To keep your mouth, teeth, and gums healthy, brush and floss every day.
4. Please don't smoke.
5. Monitor your blood sugar levels.
NEWER APPROACHES IN TREATMENT OF DIABETES MELLITUS [34]
*Peroxisome proliferator Activated Receptors (PPARs)
*Glucagon like Peptide-1 Hormone
* Liver Selective Glucocorticoid Antagonists
*Β3- Adrenoreceptor Agonist
* Α-Lipoic Acid
* Proteins Tyrosine Phosphatase -1b
* Glycogen Synthase Kinase (GSK-3)
*AMP-Activated Protein Kinase
* Estrogen Receptors: New Players in DM
*Salsalate
*Resveratrol
* L-Arginine
*Gene Therapy
*Anakinra
*Otelixizumab
THERAPY
A. Types of Therapy Involved in Diabetes Mellitus
1. Stem Cell Therapy
Treatment using stem cells Research suggests that monocytes and macrophages may play a significant role in these chronic inflammations and insulin resistance in individuals with type 2 diabetes [35]. teacher for stem cells Therapy is a state-of-the-art method designed to stop or reverse problems with the immune system [36]. The procedure comprises collection, in which patients' blood is circulated in a closed loop, co-cultivation, and purification of lymphocytes from their whole blood using adherent multi-potent stem cells derived from cord blood. In vitro lymphocytes are injected into the patient's circulation to produce educated cells (CB-SCs), but not CB-SC [37].
2. Antioxidant Therapy
Numerous antioxidants, including vitamins, supplements, active ingredients derived from plants, and medications with antioxidant properties, have been utilised to treat oxidative stress in individuals with type 2 diabetes. The best supplements to prevent oxidative stress and its effects are vitamin C, vitamin E, and β-carotene. [38]
Antioxidants are crucial in reducing the chance of getting diabetes and associated complications. Treatment with anti-inflammatory drugs the alterations suggest that inflammation is a key factor in the aetiology of type 2 diabetes and associated consequences. [39, 40].
The number and activation status of various leukocyte populations, increased apoptosis, tissue fibrosis, and changed levels of particular cytokines and chemokines are among the changes that occur in type 2 diabetes, particularly in adipose tissue, pancreatic islets, the liver, the vasculature, and circulating leukocytes [41]. An immunomodulatory medication is offered [41, 42].
B. Dietary Management :
Adequate caloric value Dietary management should be taken properly by the both diabetic and non-diabetic patient such as:
1. Balanced in regard to protein, carbohydrate and fats, in all cases it is necessary to restrict carbohydrate intake.
2. Should conform as closely as possible to normal
3. Food intake should be divided into regularly spaced meals of similar size
4. Reduce total calorie intake by decreasing both fat and carbohydrate
5. Patient must be advised to be constant in his dietary habits from day to day.
C. Newer Insulin Delivery Devices
Many improvements are being made to achieve rigid glycaemia control and to make administering insulin easier and more accurate. These include insulin syringes, pen devices, insulin pumps, implanted pumps, inhaled insulin, and other insulin administration methods.
D. Oral Hypoglycaemic or Antidiabetic Agents
In 1957, phenformin, a biguanide with clinical utility, was manufactured concurrently with sulfonylureas. More recent methods have been continuously investigated and have recently produced α-glucosidase inhibitors, thiazolidinediones, meglitinide analogues, and the most recent, dipeptidyl peptidase-4 (DPP-4) inhibitors [43].
CURRENT STATUS OF DIABETES MELLITUS:[44]
GLOBAL DIABETIC REPORT 2000-2030
|
|
2000 |
2011 |
2021 |
2030 |
|||
|
Diabetes estimates 20-7 0 year |
|||||||
|
People with diabetes in 1,000s |
151000 |
366000 |
536600 |
642800 |
|||
|
Age-adjusted comparative prevalence of diabetes, % |
4.6 |
8.5 |
.8 |
10.8 |
|||
|
People with undiagnosed diabetes, in 1,000s |
-- |
183000 |
-- |
-- |
|||
|
Proportion of people with undiagnosed diabetes, %
|
-- |
50 |
44.7 |
-- |
|||
|
Impaired glucose tolerance (IGT) estimates (20-79 y) |
|||||||
|
People with IGT, in 1,000s |
-- |
280000 |
541 |
622.7 |
|||
|
Age-adjusted comparative prevalence of IGT, % |
-- |
6.5 |
10.2 |
10.8 |
|||
|
Impaired fasting glucose (IFG) estimates (20-79 y) |
|||||||
|
People with IFG, in 1,000s |
-- |
-- |
319 |
369.7 |
|||
|
Age-adjusted comparative prevalence of IFG, % |
-- |
-- |
5.7 |
6 |
|||
|
Mortality attributable to diabetes (20-79 y) |
|||||||
|
Deaths attributable to diabetes |
-- |
4600,000 |
6700,000 |
-- |
|||
|
Proportion of diabetes-related deaths in people under 60 y, % |
-- |
-- |
32.6 |
-- |
|||
|
Type 1 diabetes estimates in children and adolescents |
|||||||
|
New cases of type 1 diabetes (0-14 y), in 1,000s |
-- |
77.8 |
108.3 |
-- |
|||
|
New cases of type 1 diabetes (0-19 y), in 1,000s |
-- |
-- |
149.5 |
-- |
|||
|
Type 1 diabetes (0-14 y), in 1,000s |
-- |
490.1 |
651.2 |
-- |
|||
|
Type 1 diabetes (0-19 y), in 1,000s |
-- |
-- |
1211.9 |
-- |
|||
|
Hyperglycemia in pregnancy (HIP) (20-49 y) |
|||||||
|
Live births affected by HIP |
-- |
-- |
21060499.4 |
-- |
|||
|
Prevalence of gestational diabetes mellitus (GDM), % |
-- |
-- |
16.7 |
-- |
|||
|
Live births affected by other types of diabetes first detected in pregnancy |
-- |
-- |
2112147.5 |
-- |
|||
|
Live births affected by other types of diabetes detected prior to pregnancy |
-- |
-- |
2460477.5 |
-- |
|||
|
Diabetes-related health expenditure |
|||||||
|
Total diabetes-related health expenditure, USD million |
-- |
465000 |
966000 |
1027600 |
|||
|
Total diabetes-related health expenditure, ID million |
-- |
499000 |
1421852 |
1549800 |
|||
|
Diabetes-related health expenditure per person, USD |
-- |
1274 |
1838.4 |
-- |
|||
|
Diabetes-related health expenditure per person, ID |
-- |
1366 |
2706.7 |
-- |
|||
|
Demographics |
|||||||
|
Total adult population (20-79 y), in 1,000s |
3288795 |
4407000 |
51134598 |
5700000 |
|||
|
Population of children (0-14 y), in 1,000s |
1246783.6 |
1900000 |
1991355.7 |
-- |
|||
|
Population of children and adolescents (0-19 y), in 1,000s |
-- |
-- |
|
-- |
|||
Table. No. 2. GLOBAL DIABETIC REPORT 2000-2030
Major drugs interacting in DM prescriptions.
|
Drugs |
Number of Times |
Percentage (%) |
|
Amoxicillin |
4 |
8 |
|
Aspirin |
20 |
40 |
|
Atorvastatin |
5 |
10 |
|
Clopidogrel |
8 |
16 |
|
Digoxin |
7 |
14 |
|
Enoxaparin |
5 |
10 |
|
Heparin |
5 |
10 |
|
Insulin |
4 |
8 |
|
Levofloxacin |
6 |
12 |
|
Nifedipine |
5 |
10 |
|
OHA |
5 |
10 |
|
Pantoprazole |
4 |
8 |
Table No. 3 Major drugs interacting in DM prescriptions.
Drug interactions with anti-diabetic drugs (moderate interactions).
|
S.No |
Drugs |
No. of Times |
Effect |
Alternative/Management |
|
1. |
Glibenclamide + diclofenac |
1 |
Increased effect of glibenclamide |
Use with caution. Monitor blood sugar. |
|
2. |
Glibenclamide + ranitidine |
1 |
Increased effect of glibenclamide |
Use with caution. Monitor blood sugar. |
|
3. |
Glibenclamide + hydrocortisone |
1 |
Reduced effect of glibenclamide |
Use with caution. Monitor blood sugar. |
|
4. |
Glimipride + budesonide |
1
|
Budesonide reduces the effect of glimipride. |
Use with caution. Monitor blood sugar |
|
5. |
Glimipride + aspirin |
1 |
Increased effect of glimipride. |
Use with caution. Monitor blood sugar. |
|
6 |
Metformin + budesonide |
1 |
Reduced effect of metformin |
Use with caution. Monitor blood sugar |
|
7 |
Insulin + aspirin |
2
|
Increased effect of insulin. |
Use with caution. Monitor blood sugar. |
|
8 |
Insulin + levofloxacin |
1 |
Levofloxacin disturbs blood glucose hemostasis |
Monitor blood sugar closely. |
|
9 |
Insulin + metoprolol |
1 |
Increased effect of insulin. |
Use with caution. Monitor blood sugar |
Table No. 4 Drug interactions with anti-diabetic drugs (moderate interactions).
REFERENCES


Srutuja S. Jadhav, Swapnita A. Koli, Namrata S. Kathwate, Pranali A. Tate Deshmukh, Harshada S. Deshmukh*, Priyanka B. Parekar, Emerging Therapeutic Strategies for Diabetes Mellitus: A Literature Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 2, 2110-2124. https://doi.org/10.5281/zenodo.14946705
 10.5281/zenodo.14946705
10.5281/zenodo.14946705
