Swamy Vivekanandha college of pharmacy, Namakkal, India.
Acute poisoning and drug overdose continue to contribute significantly to global morbidity and mortality, laying a high burden on emergency and critical care services. Whereas the mainstay of early management is supportive care, many poisonings require specific antidotes targeting the underlying toxic mechanisms. Over the past decade, advances have increased the breadth of antidotal therapy, including high-dose insulin euglycemia therapy, lipid emulsion therapy, monoclonal antibody-based anticoagulant reversal agents, and investigations into supramolecular antidotes. Recent advancements in diagnostic tools, extracorporeal treatments, and precision medicine have significantly transformed the practice of emergency toxicology. This review synthesizes the latest updates on both established and emerging antidotes, highlights current evidence and its evolution, examines barriers to real-world application, and suggests future directions in research and clinical care. Keeping up with these advances is key to giving patients the best possible chance of recovery during acute toxicologic emergencies.
Poisoning persists as a global health issue, with millions of exposures each year. The American Association of Poison Control Centers reports a continuing rise in serious and fatal poisonings, particularly involving opioids, cardiovascular medications, and new psychoactive substances (NPS)(1). In many countries, pesticide poisoning is still the leading cause of mortality, especially in rural and farming communities. The surge of synthetic opioids—such as fentanyl analogs—and extremely cardiotoxic agents in the environment has led to an increase in complicated toxicology emergencies that require rapid and targeted management in the emergency setting(2). Supportive care—airway stabilization, ventilation support, hemodynamic support, and all of the aspects of care necessary to correct metabolic derangements—remains the pinnacle of care; however, they do not reverse toxin-receptor interactions, enzyme inhibition, or specific organ toxicodynamics(3). Therefore, antidotal therapy is an important adjunctive therapy when supportive care is inadequate. The advancements in pharmacology, molecular chemistry, and biomedical engineering have suggested several promising antidotes with better efficacy and safety(4).
BASIC CONCEPTS OF ANTIDOTE TREATMENT
Antidotes work to neutralize dangerous exposures by utilizing a variety of different critical mechanisms that target the underlying pathophysiology of toxicity. Some act through receptor antagonism, which removes the toxin from its binding site, as illustrated by naloxone for opioids and flumazenil for benzodiazepines. Certain strategies depend on chelation or direct neutralization methods, such as hydroxocobalamin binding to cyanide to produce a nontoxic complex(5). Certain antidotes reconstitute the activity of inhibited enzymes, such as pralidoxime, reactivating acetylcholinesterase in cases of organophosphate poisoning. Certain treatments create metabolic barriers; for example, fomepizole inhibits alcohol dehydrogenase to prevent the formation of toxic metabolites in cases of methanol or ethylene glycol poisoning. Antidotes can also facilitate detoxification, as N-acetylcysteine stimulates glutathione synthesis to neutralize toxic reactive metabolites of paracetamol. Direct reversal agent such as andexanet alfa for the factor Xa inhibitors rapidly counteract the effect of specific drugs. And lastly, physical sequestration approaches-such as lipid emulsion therapy and novel supramolecular compounds-bind to or sequester lipophilic toxins, reducing their bioavailability and clinical toxicity(6).
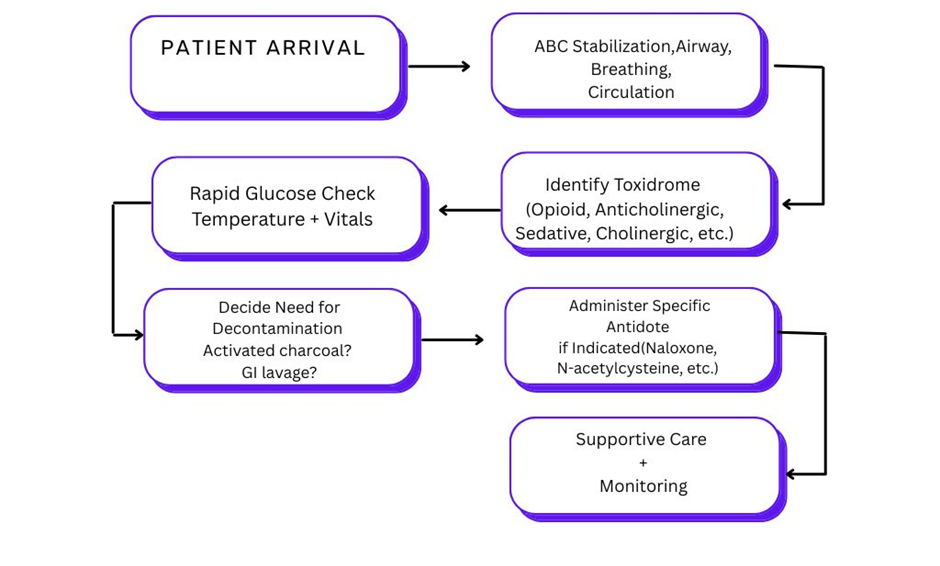
Figure 1 – Algorithm for Emergency Toxicology management
Initial detection and syndromic approach
The main assessment addresses airway, breathing, circulation, temperature control, and neurological status, as emphasized in standard toxicology practice and poison center guidelines(3).
Modern research examines:
Supramolecular antidotes such as cyclodextrins and cucurbiturils have potential binding ability to xenobiotics(4).
Antidotes in Clinical Toxicology.
High-dose insulin therapy for calcium channel blocker and β-blocker toxicity is strongly recommended in the AHA 2023 guidelines(7).
EMERGING AND RECENTLY UPDATED ANTIDOTES
Initially developed as a parenteral nutrition supplement, lipid emulsion therapy (LET) has powerful effects on lipophilic drug toxicity, notably local anaesthetic systemic toxicity (LAST)(8).
Mechanism
Sequestration of lipophilic poisons via a "lipid sink
↓
Restore myocardial free fatty acid supply.
↓
Membrane stabilization(26).
LET is suggested in refractory cardiotoxicity because of the Local anaesthesia (bupivacaine) effect, Tricyclic Antidepressants, β-blockers, and calcium channel blockers.
The 2023 AHA update recognizes LET as a life-saving treatment in LAST(9).
HIET is now the preferred therapy for Severe β-blocker toxicity and Severe calcium channel blocker poisoning
Mechanism :
Enhances myocardial carbohydrate utilization
↓
Improves inotropy independent of β-receptors
↓
Restores systemic perfusion.(10)
AHA strongly recommends the early initiation of HIET in life-threatening cardiotoxicity.(11)
An important advancement in the treatment of methanol and ethylene glycol intoxication.(12)
Mechanism :
Process Blocks alcohol dehydrogenase → inhibits toxic metabolite production.(13)
Advantages include:
No adverse events associated with ethanol infusion. Reproducible pharmacokinetics. More favorable safety profile.
Fomepizole is now the mainstay antidote in the clinical management of toxic alcohol ingestion. (14)
Idarucizumab:
Monoclonal antibody fragment
Mechanism :
Works within minutes to neutralize dabigatran. Superior recovery when compared to dialysis(15)
Recombinant altered FXa decoy agent.(16) Used as an Antidote for apixaban, rivaroxaban, and edoxaban. It plays a vital and Critical role in the management of trauma and emergency bleeding(17).
The best antidote for cyanide poisoning, especially in smoke inhalation cases.
According to AHA 2023, hydroxocobalamin should not be delayed in cases of suspected cyanide toxicity, even if laboratories have not confirmed.(18)(19)
Extremely proficient in counteracting digoxin-induced Ventricular arrhythmias, Elevated potassium levels, and Critical bradyarrhythmia.(20) It is highlighted prominently in the 2023 AHA guidelines
Recent research shows promise for the treatment of Toxicity from neuromuscular blockers (sugammadex).Toxicity involving new medication overdoses, including Cyclodextrins, Cucurbiturils, Pillararenes(21)
Table 1. Novel Antidotes and Their Therapeutic Applications
|
COUNTERACTING AGENT |
TARGET TOXICITY |
MECHANISM |
PROOF |
|
Lipid emulsion, LAST |
hydrophobic medications |
Lipid reservoir, metabolic assistance |
Strong;AHA 2023
|
|
Elevated insulin dosage |
CCB/β-blocker poisoning |
Metabolic assistance + inotropic support |
Strong AHA endorsement
|
|
Fomepizole |
Poisonous Alcohol |
Inhibition of ADH |
Widely recognised |
|
Idarucizumab |
Dabigatran |
Antibody |
Quick , total reversal |
|
Andexanet Alfa |
FXa Inhibitor |
Decoy receptor |
Robust evidence in hemorrhage |
|
Hydroxocobalamin |
Cyanide |
Unites with cyanide → Cyanocobalamin |
Rapid effect; AHA focus |
|
Digoxin Fab |
Digoxin |
Antibody interaction |
Critical Arrhythmias |
These compounds exhibit high-affinity molecular encapsulation and present future opportunities for use as antidotes.
EVIDENCE-BASED EMERGENCY USE
The 2023 AHA update on toxicology has clear recommendations for toxicants that have antidotes that need to be given immediately for life-threatening toxicity, which include Naloxone, Hydroxocobalamin , Digoxin Fab, Sodium bicarbonate (TCA/cocaine toxicity), Lipid emulsion therapy , High-dose insulin.
Similar to worldwide toxicology reviews, there is often inadequate availability of antidotes, and stocking plans should be developed for emergency systems(22)
Table 2: Critical Antidotes for Emergency Rooms
|
IMPORTANCE RANK |
REMEDY |
JUSTIFICATION |
|
Prompt Accessibility |
Naloxone |
Frequent opioid overdoses |
|
Activated charcoal |
Wide ranging initial decontaminant |
|
|
Hydroxocobalamin |
Cyanide crises |
|
|
Atropine + Pralidoxime |
Poisoning from Organophosphates |
|
|
Idarucizumab |
Bleeding associated with NOAC |
|
|
In 1 Hour |
Digoxin |
Heart toxicity |
|
Fomepizole |
Ingestion of toxic alcohol |
|
|
Glucagon |
Overdose of beta blockers |
|
|
Fat emulsion |
Intense Cardiotoxicity |
CONSTRAINTS OF CONVENTIONAL ANTIDOTES AND DEMAND FOR NOVEL AGENTS
Traditional antidotes have some limitations which include Latency in effect in Generic mechanisms, Significant adverse effects (e.g., seizures from flumazenil), Supply chain disruption , inconsistent stock control and Inadequate for modern toxins (e.g., NOACs, new opioids)
New antidotes are being developed with improved affinity, specificity and lower toxicity.(23)
ANTIDOTE INVENTORY AND READINESS
global consensus suggests 44 critical antidotes, with 23 required to be readable in emergency departments. Readiness deficiencies encompass Insufficient inventory, Delays in the supply chain, and a Lack of national strategic plans(24) (24)
The WHO endorses antidote banking, particularly for expensive, infrequently used antidotes
CLINICAL SIGNIFICANCE OF NEW ANTIDOTES
The emerging antidotes and tailored reversal agents have revolutionized toxicology by making it possible to receive results much faster in critical situations. These advancements enhanced survival rates and reduced side effects. (6) These innovations support the previously untreatable or high-mortality toxic exposure and thus enhance treatment in emergency care and patient outcomes.
These novel antidotes and reversal agents play an important role in the setting of mass chemical exposure, where rapid, concentrated efforts may prevent many illnesses. They play a vital role in mitigating toxic injuries among workers exposed to dangerous substances promptly. In clinical practice, next-generation reversal agents are now essential for controlling bleeding associated with anticoagulant therapy, providing rapid and reliable hemostatic correction. Additional critical roles include the management of overdoses of cardiovascular medications???, whereby timely stabilization significantly reduces life-threatening complications and improves patient outcomes.
PROSPECTIVE AVENUES AND RESEARCH REQUIREMENTS
Future development in toxicology is generating a broad spectrum of supramolecular countermeasures capable of effectively neutralizing a wide range of specificities. Advances in molecular medicine are gene-targeted or enzyme-targeted treatments for nerve agents. The advent of nanotechnology-enabled toxin sequestration?²?? enables fast attachment and elimination of hazardous materials at the nanoscale. There is an increasing demand to advance clinical studies on lipid rescue therapies to further establish their efficacy and improve their practice. Improving global supply and stocking of antidote formulations is essential to ensure timely availability for emergencies or mass exposures. Finally, the introduction of AI-driven predictive toxicology for specific antidote administration?²?? is expected to revolutionize personalized and immediate management of poisoning incidents.
PHARMACOECONOMIC CONSIDERATION :
The economic structure of modern toxicology is increasingly dictated by the value for money of novel antidotes, such as the consideration of andexanet alfa versus standard PCCs, raising key questions about value with regard to affordability. Antidote shortages can be financially burdensome, leading to longer delays in treatment, extended hospital stays, and increased overall healthcare costs. Healthcare systems must, therefore, focus on sound financial planning and diligent procurement strategies that ensure adequate supplies of antidotes, thus assuring affordable care while remaining ready for any toxicological emergency.
WORLDWIDE INEQUALITIES IN ANTIDOTE AVAILABILITY
An urgent worldwide health issue is the imbalanced access to antidotes. Typically, high-income nations have sufficient resources; however, low- and middle-income nations often struggle to purchase enough quantities and may lack the necessary supply chains or production capabilities. This disparity is greater in rural and agricultural regions, where barriers to swift treatment involve long travel distances, inadequate public transport, and inferior medical facilities. Bridging these gaps is essential for providing communities everywhere with an equitable opportunity for successful toxicological interventions.
IMPROVEMENTS IN DIAGNOSTICS ENHANCING ANTIDOTE APPLICATIONS
The speed and precision of antidote delivery are being significantly improved by advances in diagnostic capabilities. Bedside toxicology panels eliminate delays in commencing targeted treatment by offering quick toxin testing at the patient's site.Similarly, early diagnosis of toxic alcohol consumption has been transformed by quick lactate and anion-gap diagnostics, which allow medical practitioners to start life-saving treatments like fomepizole without waiting for laboratory confirmation. Bedside ultrasound offers instant information about heart function in cases of cardiotoxic poisoning, which informs treatment decisions about high-dose insulin or lipid emulsion. This diagnostic field is further enhanced by new biomarkers for early toxicity identification, which ensure prompt and precise antidote delivery that can greatly improve clinical outcomes.
PROGRAMS FOR MANAGING ANTIDOTES
Successful antidote formulation depends on organized efforts to enhance hospital and community reactions to toxicological crises. Evaluation of antidotes includes sufficient inventory and analyse usage trends. regular training simulations and simulated emergency circumstances for healthcare providers and first responders strengthen preparation, enhance coordination, and guarantee that antidotes are administered quickly and efficiently during actual emergencies
TOXICOLOGICAL INFORMATICS AND INTEGRATION OF AI
Clinical toxicology is a result of the combination of artificial intelligence and advanced informatics. Machine-learning models can predict the level of poisoning, assisting medical personnel in anticipating problems and prioritizing actions. AI-driven solutions provide antidote dosage modifications by optimizing treatment accuracy based on patient details and real-time physiological data. Also, intelligent decision-support tools are becoming increasingly beneficial in toxicological crises, assisting clinicians in navigating complex situations, accelerating triage, and improving the overall efficacy and safety of antidote administration.
CONCLUSION
Acute poisoning and drug overdose persist as challenges in contemporary emergency medicine, requiring swift diagnosis, stabilization, and precise treatment measures. Though supportive care continues to be the foundation of toxicological treatment, the past ten years have seen a significant change with the emergence of highly specialized and mechanism-targeted antidotes. New interventions such as high-dose insulin euglycemia therapy, lipid emulsion therapy, and monoclonal antibody–based reversal agents have greatly improved outcomes in previously lethal toxicities. Advances in supramolecular chemistry, nanotechnology-based sequestration systems, and precision diagnostics further expand treatment options, marking a shift away from generalized, nonspecific therapies toward highly individualized, targeted therapies.
REFERENCES


Anushya, R. R. Redlin Jani, Sri Vaishnavi P, Susmitha S, Swasamathi S, Thejasree S, Vidhyasri S, Emerging Antidotes and Reversal Agents in Emergency Toxicology: Recent Advances and Clinical Relevance, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1903-1910. https://doi.org/10.5281/zenodo.17883769
 10.5281/zenodo.17883769
10.5281/zenodo.17883769
