Central India College of Pharmacy, Lonara, Nagpur.
Early-onset Alzheimer’s disease (EOAD), defined by symptom onset before the age of 65, represents a rare but clinically significant subset of Alzheimer’s disease (AD). EOAD is marked by greater genetic influence, rapid progression, and frequent atypical variants including posterior cortical atrophy, logopenic primary progressive aphasia, frontal variant, and corticobasal presentations. These forms often present with non-amnestic symptoms such as visuospatial, language, or executive dysfunction, complicating diagnosis and management. Standard pharmacological treatments, including cholinesterase inhibitors and memantine, provide only symptomatic relief without altering disease course. In recent years, herbal and nutraceutical interventions have gained attention as adjunctive strategies due to their neuroprotective, antioxidant, anti-amyloid, and anti-inflammatory properties. Prominent candidates include Ginkgo biloba, curcumin, Bacopa monnieri, Withania somnifera (ashwagandha), and huperzine A, each with mechanistic plausibility and varying levels of preclinical and clinical evidence. While some clinical studies suggest modest cognitive benefits, trial heterogeneity, small sample sizes, and issues of standardization limit strong conclusions. This review outlines the epidemiology, clinical heterogeneity, and pathophysiology of EOAD, highlighting its atypical variants, and critically evaluates the current evidence for herbal managerial tools. Despite encouraging findings, rigorous clinical trials are urgently required to validate efficacy, establish safety, and define the role of herbal medicines as adjuncts in the comprehensive management of EOAD.
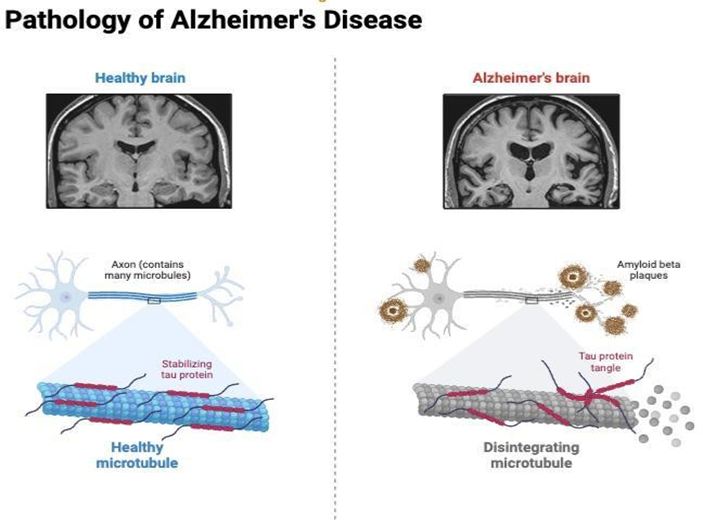
Alzheimer’s disease (AD) is the most common cause of dementia worldwide, affecting millions of people and posing a major global health burden. It is characterized by progressive cognitive decline, behavioral disturbances, and functional impairment, underpinned by neuropathological hallmarks such as extracellular amyloid-β plaques and intraneuronal tau neurofibrillary tangles. [1,5,]While most cases manifest after the age of 65 years (late-onset Alzheimer’s disease, LOAD), a significant minority—approximately 5–10% of cases—develop symptoms earlier, defined as early-onset Alzheimer’s disease (EOAD). EOAD is clinically important for several reasons. Firstly, its age of onset affects individuals in their most productive years, leading to profound personal, social, and economic consequences. Secondly, EOAD often presents with non-amnestic and atypical symptoms, including visuospatial deficits, language dysfunction, executive impairment, or behavioral changes, unlike the predominantly memory-led presentation seen in LOAD. [4]These atypical forms are categorized into distinct variants such as posterior cortical atrophy (PCA), logopenic primary progressive aphasia (lvPPA), frontal-behavioral variant, and corticobasal syndrome (CBS). This clinical heterogeneity complicates early recognition and often delays diagnosis.

From a pathophysiological perspective, EOAD differs from LOAD in its stronger genetic contribution. Mutations in the amyloid precursor protein (APP) and the presenilin genes (PSEN1 and PSEN2) account for a substantial proportion of familial EOAD cases, leading to abnormal amyloid processing and early, aggressive disease onset.[6]Beyond genetics, EOAD involves mitochondrial dysfunction, oxidative stress, neuroinflammation, synaptic failure, and cholinergic deficits, making it a complex, multi-factorial disorder. Advances in biomarkers— including cerebrospinal fluid (CSF) assays of amyloid and tau, plasma phosphorylated tau, and neurofilament light chain, as well as neuroimaging modalities (FDG-PET, amyloid PET, tau PET)—have improved diagnostic precision and facilitated earlier detection.Despite progress, treatment options remain limited. [13] Current pharmacological therapies such as cholinesterase inhibitors (donepezil, rivastigmine, galantamine) and NMDA receptor antagonist (memantine) provide symptomatic relief but do not halt disease progression.
Recently approved anti-amyloid monoclonal antibodies (aducanumab, lecanemab, donanemab) offer disease-modifying potential, but accessibility, cost, and safety concerns limit their widespread use. Consequently, there is growing interest in complementary and adjunctive therapies, particularly herbal medicines and nutraceuticals, that target oxidative stress, neuroinflammation, and synaptic dysfunction through multi-modal mechanisms.
Several herbal agents have been investigated for their neuroprotective roles. Ginkgo biloba extract has shown modest cognitive benefits and microcirculatory effects; curcumin, derived from turmeric, exerts anti-amyloid, anti-tau, and anti- inflammatory activity, particularly with novel bioavailability-enhanced formulations; Bacopa monnieri improves memory and synaptic plasticity; Withania somnifera (ashwagandha) demonstrates adaptogenic and neuroregenerative potential; and huperzine A, a natural cholinesterase inhibitor, offers cognitive improvements similar to synthetic drugs. While preclinical evidence is strong, clinical trials often yield inconsistent results due to small sample sizes, heterogeneous methodologies, and variability in herbal product standardization. Given the clinical heterogeneity of EOAD, limitations of existing therapies, and growing scientific interest in herbal interventions, a comprehensive review of EOAD and its herbal managerial tools is timely. This article aims to (i) summarize the epidemiology, clinical variants, and pathophysiology of EOAD; (ii) review current diagnostic and therapeutic approaches; and (iii) critically evaluate the evidence for herbal and nutraceutical strategies as adjunctive management tools in EOAD.
Early-Onset Alzheimer’s Disease (EOAD) :
Definition: EOAD is Alzheimer’s disease with clinical symptom onset before age 65. It represents a minority of AD cases but causes disproportionate social, economic and caregiving burdens because it affects people in their working years.
Epidemiology : EOAD accounts for roughly 5–10% of all AD cases, with prevalence estimates varying by age band and population; some studies report ~24 per 100,000 in mid-life age ranges and higher in certain cohorts. EOAD may be underrecognized because atypical, non-memory presentations lead to delayed diagnosis. [11,15]
Genetic architecture
Variants of Alzheimer’s Disease
Alzheimer’s disease (AD) is not a uniform clinical entity but a spectrum of syndromes. While the majority of patients present with the typical amnestic variant, a substantial subset—especially those with early-onset AD (EOAD) develop atypical presentations involving visual, language, behavioral, or motor symptoms. Recognizing these variants is crucial for accurate diagnosis and management, as they are frequently misdiagnosed as other dementias or psychiatric conditions.

Typical Amnestic Alzheimer’s Disease :
Posterior Cortical Atrophy (PCA)
Logopenic Variant Primary Progressive Aphasia (lvPPA)
Frontal/Behavioral Variant Alzheimer’s Disease
Corticobasal Syndrome (CBS) Associated with AD
Other Less Common Variants
Management of Early-Onset Alzheimer’s Disease
1. Pharmacological Management :
a. Symptomatic Therapies :
b. Disease-Modifying Therapies (Emerging)
2. Non-Pharmacological Management
3. Genetic Counseling and Risk Management :
4. Multidisciplinary & Holistic Care :
EOAD requires a multidisciplinary approach:
Herbal managerial tools
1. Ginkgo biloba (EGb 761)
Mechanisms : Antioxidant and free-radical scavenging. Anti-inflammatory effects and modulation of microglial activation.Improves cerebral microcirculation and mitochondrial function; may modulate neurotransmission (serotonergic/dopaminergic/cholinergic).
Evidence : Multiple meta-analyses and RCTs report modest cognitive and functional benefits in cognitive impairment and dementia when using the standardized extract EGb 761 at 120–240 mg/day; benefits are most consistent for stabilization or slowing of decline in short-to-medium term (weeks–months) but effect sizes vary.
Safety / Caveats : Generally well tolerated in trials of standardized extracts; bleeding risk and interactions with antiplatelet/anticoagulant drugs remain important concerns. Product variability is a major limitation — only well- standardized extracts (EGb 761) have reproducible evidence.
Research gaps : Need for long-term, biomarker-guided RCTs in well- characterized EOAD populations; combination with standard therapy (and monitoring for interactions) requires study.[45,46]
2. Curcumin (Curcuma longa) and novel formulations
Mechanisms : Anti-amyloid and anti-tau actions (direct binding/aggregation inhibition), strong antioxidant and anti-inflammatory activities, metal chelation, inhibition of microglial pro-inflammatory signaling, modulation of autophagy.Native curcumin has poor oral bioavailability; nanoformulations and carrier systems (liposomes, ferritin nanocages, polymeric nanoparticles) markedly increase BBB penetration and plasma/tissue exposure.
Evidence : Extensive preclinical evidence for anti-amyloid/tau and neuroprotective effects. Human trials with conventional curcumin formulations were largely negative or inconsistent, but newer pharmacokinetic-enhanced formulations show promising biomarker signals and small clinical improvements in early studies; definitive large RCTs are still lacking. Reviews of nanocarrier strategies highlight translational potential for AD.
Safety / Caveats : Safe at commonly used doses; GI side effects reported rarely. Clinical benefit depends heavily on formulation and dosing trials must report pharmacokinetic data.
Research gaps : Well-powered RCTs using standardized, bioavailability- enhanced curcumin with biomarker endpoints (plasma/CSF p-tau, amyloid, imaging) are needed.[43.44]
3. Bacopa monnieri (Brahmi)
Mechanisms : Bacosides and other constituents show antioxidant, anti- apoptotic, cholinergic modulation, enhancement of synaptic plasticity and BDNF signaling, and anti-inflammatory effects.
Evidence : Multiple RCTs in healthy older adults and MCI show improvements in memory, attention, and some cognitive domains; systematic reviews/meta-analyses support cognitive benefits but note heterogeneity in extracts, doses, and outcomes. A few longer trials (including an RCT vs donepezil in small cohorts) suggest comparable effects in some measures, but sample sizes are small.
Safety / Caveats : Generally well tolerated; common mild GI complaints. Standardization of bacoside content is necessary for reproducible results.
Research gaps : Larger, longer trials in MCI/early AD (including EOAD subsets) with standardized extracts and biomarker outcomes.[47]
4. Withania somnifera (Ashwagandha)
Mechanisms : Adaptogenic and anti-inflammatory actions; animal studies indicate reduced amyloid-β, lowered pro-inflammatory cytokines, antioxidant effects, and promotion of neurite outgrowth / synaptic recovery. Clinical mechanisms likely include modulation of neuroinflammation and support of neuroplasticity.
Evidence : Preclinical models (including 5xFAD mice) show improvement in cognition and neuropathology. Small human trials report improvements in memory and attention measures; systematic reviews indicate potential but emphasise small trials and mixed quality. Recent human supplementation studies report benefit on some cognitive endpoints.
Safety / Caveats : Generally safe at typical doses used in trials (e.g., 225– 600 mg standardized extracts), but quality and standardization vary across commercial products.
Research gaps : Need RCTs in early AD/EOAD using standardized extracts, with dose-finding, PK, and biomarker endpoints.[48]
5. Huperzine A
Mechanisms : Reversible acetylcholinesterase inhibition (cholinergic augmentation) and possible neuroprotective effects (anti-apoptotic, NMDA antagonism reported in preclinical work).
Evidence : Several RCTs (many conducted in China) and meta-analyses report short-term cognitive improvement (8–16 weeks) vs placebo; however, methodological limitations, small sample sizes, and inconsistent longer-term benefits limit conclusions. Larger multicenter trials have reported mixed results.
Safety / Caveats : Side effects overlap with cholinesterase inhibitors (nausea, diarrhea, sweating, bradycardia); interactions with other cholinergic agents must be monitored.
Research gaps : Larger, rigorously designed, longer trials to confirm efficacy and safety; studies in EOAD specifically are lacking.[49]
6. Other candidates & multi-component approaches
Omega-3 fatty acids, resveratrol, citicoline, Panax ginseng, sage and rosemary: mixed evidence; some promising biomarker or small clinical signals but inconsistent across trials. Recent reviews highlight potential of combinations and multi-target strategies rather than single-agent “silver bullets.” [50]
Role of NDDS in Herbal Management of Early-Onset Alzheimer’s Disease
Herbal compounds (curcumin, bacosides, resveratrol, withanolides, huperzine A) have promising anti-Alzheimer’s effects.
Major limitations:
NDDS Strategies for Herbal EOAD Therapy
1. Nanoparticles : Polymeric (PLGA, chitosan) or lipid-based carriers.Protect herbal actives from degradation and enhance BBB penetration.
Example: Curcumin nanoparticles → improved anti-amyloid activity, antioxidant effect, and memory improvement.[51,53]
2. Liposomes : Phospholipid vesicles encapsulating both hydrophilic & lipophilic herbal molecules.Ligand-modified liposomes target brain receptors (e.g., transferrin-modified liposomes for curcumin).
Example: Huperzine A liposomes → prolonged cholinesterase inhibition.
3. Niosomes & Dendrimers : Niosomes are more stable and cost-effective than liposomes. Dendrimers are branched polymers that carry herbal drugs with high precision.[52]
Example: Resveratrol dendrimers → improved antioxidant neuroprotection.
4. Nanoemulsions & Microspheres : Increase solubility and bioavailability of poorly soluble herbal extracts.
Example: Intranasal curcumin nanoemulsion → rapid brain delivery, enhanced memory protection.[53]
5. Intranasal Delivery Systems : Direct nose-to-brain pathway bypasses BBB.Reduces first-pass metabolism, provides faster action.
Example: Ashwagandha nanoformulation via intranasal route → enhanced cognitive improvement in animal models.
6. Transdermal Patches : Provide controlled and sustained release of herbal actives.Reduce dosing frequency and systemic side effects.
Example: Rivastigmine patch is already used; herbal patches with Bacopa extract are under preclinical study.[51]
CONCLUSION :
Early-onset Alzheimer’s disease (EOAD) is a clinically and genetically heterogeneous form of dementia that differs significantly from the more common late-onset form. Its earlier age of onset, frequent genetic basis, and atypical clinical variants such as posterior cortical atrophy and logopenic progressive aphasia make timely recognition and diagnosis particularly challenging. While conventional treatments like cholinesterase inhibitors and memantine remain the mainstay of management, their benefits are limited and do not halt disease progression. Herbal and natural products including Ginkgo biloba, curcumin, Bacopa monnieri, Withania somnifera, huperzine-A, and others have shown promising neuroprotective mechanisms — ranging from antioxidant and anti-inflammatory effects to cholinesterase inhibition and amyloid modulation. However, evidence from EOAD-specific clinical trials remains scarce, and concerns about safety, herb–drug interactions, and lack of standardization must be carefully addressed.
Integrating herbal therapies as complementary approaches may offer additional symptomatic relief and neuroprotection, but they should be used cautiously under professional supervision. Future research should focus on well-designed, EOAD- targeted studies to establish efficacy, optimize formulations, and provide clearer clinical guidance. Overall, a combined strategy involving early diagnosis, conventional therapy, lifestyle interventions, and evidence-based herbal management holds promise for improving quality of life in individuals with EOAD and their caregivers.[1,5,22,38,45]
REFERENCES


Shahril Raza Khan, Tohed Chand Quresh, Mohammad Sufiyan Ansari, Ayanuddin Salimuddin Mulla, Ganesh Pradip Akone, Rubeena Shiekh, Dr. Sayyad Sajauddin Gulab, Early Onset of Alzheimer’s Disease it’s Variant and its Herbal Managerial Tools, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2252-2264. https://doi.org/10.5281/zenodo.17165676
 10.5281/zenodo.17165676
10.5281/zenodo.17165676
