Guru Nanak Institute Pharmaceutical of Science and Technology 157/F, Nilgunj Road, Sahid Colony, Panihati, Khardaha, Kolkata – 700114, West Bengal, India.
Introduction: Anemia in school-age children is a widespread worldwide health issue that leads to chronic morbidity and frequent hospitalizations. Nearly 40% of children between the ages of 6 and 12 are impacted in low- and middle-income environments, which is the subject of this review. This burden is exacerbated by genetic conditions such sickle cell disease and thalassemia, chronic inflammation, and nutritional inadequacies. Furthermore, immediate public health intervention is required due to the rising prevalence. Method: Through an analysis of clinical reports and epidemiological studies, this review summarizes the most recent data on the etiology and clinical assessment of pediatric anemia. The condition is classified using key diagnostic criteria, including as reticulocyte count, hemoglobin concentration, and mean corpuscular volume. The investigation also looks at how socioeconomic obstacles and inadequate diets affect the severity of disease and hospitalization trends. Conclusion: The results highlight the importance of early identification, dietary changes, and customized care in reducing the negative clinical and financial effects of juvenile anemia. Reducing repeated hospitalizations requires addressing socioeconomic issues. In order to enhance health outcomes and lessen the burden of this disorder, future research should give priority to creative preventative techniques and therapeutic approaches.
In recent times, a pattern has emerged in terms of haemoglobin levels being lower than normal in school aged children, which is becoming the main reason for the prevalence of anemia in children worldwide. According to the World Health Organization (WHO), anemia is deemed a global health problem, which is affecting both the developing and developed countries [1]. The mean hemoglobin levels of school children aged between 6-12 years is about 13.5 g/dL, with anemia being two standard deviations below the mean for the age group [3][4]. In 2019, the World Health Organization (WHO) also estimated that the global prevalence of anemia in children was 39.8%, which is equivalent to 269 million children of the worldwide population [2][23]. It is seen to be most prominent in families with low income, for which access to proper healthcare and balanced diet becomes limited [23]. Anemia is the most common hematologic abnormality identified in infants and children both, associated with increased morbidity and mortality in children [5][42]. There are many causes of anemia, which can be both acquired or inherited, and can vary widely in various populations across the world. Hemoglobin (Hb), hematocrit, or red blood cell levels count below the typical age and sex-adjusted norms that are used to identify anemia in practice [5][42]. Chronic anemia-related morbidity has a significant financial impact in addition to reducing productivity due to decreased work capacity, cognitive decline, and heightened vulnerability to infection [6]. Various environmental factors, chronic comorbidities, congenital or genetic problems of hemoglobin or red blood cells, and nutritional inadequacies are risk factors that lead to the development of anemia in children [7]. These reasons altogether constitute the problem of the recurrence that is arising in terms of hospitalizations and treatments of these affected children. We represent the current understanding of the clinical assessment, pathophysiology and consequences of anemia, focusing on school-aged children in low-income and middle-income families and societies, along with the current situation of their health and nutritional status. We discuss the different risk factors that co-occur in various populations, the complex causes of anemia, the places and populations where different and possible obstacles to effective prevention and management of anemia, resulting in frequent hospitalizations and treatments.
2. The Present Classification and Prevalence Of Anemia
A hematologic disorder such as anemia, frequently has multiple contributing factors and may exhibit multiple pathophysiological pathways [8]. On clinical basis, anemia can be classified on the basis of Red Blood Cell (RBC) Morphology and indices [31]. Normocytic and normochromic anemias have Mean Corpuscular Volume (MCV) 80-100 fL and Mean Corpuscular Hemoglobin Concentration (MCHC) 32-36%, Microcytic and hypochromic anemias have MCV <80 fL and MCHC <32%, and Macrocytic anemia has MCV >100 fL [Fig. 1]. Further classification based on characteristic findings (MCV, MCH and MCHC values) are associated with various etiological factors [Table 1].
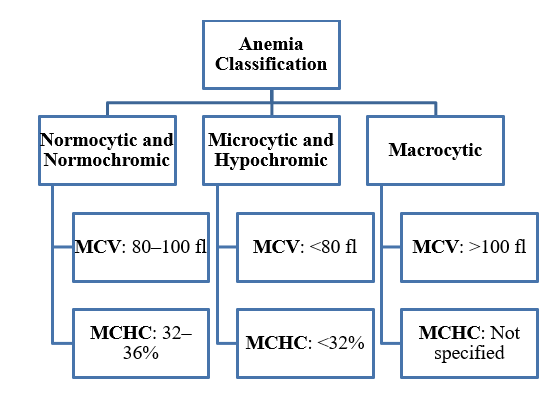
Fig. 1 Classification of Anaemia based on RBC morphology and indices.
Table 1. Differentiating points of various Anaemia
|
Characteristic findings |
Microcytic hypochromic |
Normocytic normochromic |
Macrocytic |
|
MCV |
<80 fL (decreased) |
80 – 95 fL (normal) |
>95 fL (increased) |
|
MCH |
<27 pg (decreased) |
≥27 pg (normal) |
Increased |
|
MCHC |
Decreased |
Normal |
Normal |
|
Etiological factors |
|
|
|
The most prominent one, Iron Deficiency Anemia (IDA, one of the risk factors of microcytic anemia), is most likely to develop in between children of age groups of 2-5 years (preschool), 5-12 years (school-aged), and also post-menarcheal adolescent females, putting them in at highest risk [7]. While the incidence is declining in industrialized places, partly due to iron fortification of infant formulas and cereals, iron deficiency is still the most common nutritional deficiency among children in developing nations and countries to be a major cause of anemia in children and adolescents [5]. Sickle Cell Anemia (SCA), the second most prominent hematologic disease, is estimated in 515,000 kids born annually, with sub-Saharan regions bearing the largest burden (about 79%) [10][45]. In a cohort study conducted in 2022 and 2023 consecutively, it was seen that children between the age of 5-12 years, from both the low and high-income countries, were susceptible to being underweight, leading to increased mortality risks, and also older age and lower hemoglobin levels were identified as significant risk factors for underweight status, as the odds ratio for underweight was seen to be roughly 0.60 for every unit rise in hemoglobin levels and 1.24 for every extra year of age [11][12]. Apart from these, Thalassemia, which is a hereditary disorder, also has come out to be quite prominent like the others in recent times. Defined by the abnormalities in the production of one or more of the globin chains that make up hemoglobin, an estimated 1.7% of the population worldwide are thought to have either α- or β-thalassemia trait [33]. Whereas β-thalassemias are more frequently seen in people of Mediterranean, African, and Southeast Asian ancestry, with prevalence rates ranging from 5% to 30%, α-thalassemia is most frequently found in African and Southeast Asian populations. According to estimates, thalassemias rank sixth among female anemia causes worldwide and ninth among male anemia causes [7][38]. The reticulocyte count and additional red cell indices can aid in further defining the causes of anemia [Table 2].
Table 2. Red Cell Indices of some significant anaemias in children.
|
|
MCV |
RDW |
MCHC |
Reticulocyte Count |
|
Iron Deficiency Anemia |
↓ |
↑ |
↓ |
↓ |
|
Sickle Cell Anemia |
Normal |
↑ |
↑ |
↑ |
|
Thalassemia |
↓ |
Normal |
↓/Normal |
↑ |
3. The Main Reasons and Causes
Anemia most commonly arises from a combination of nutritional deficits, genetic hemoglobin disorders, and chronic disease processes [5][22]. The most common kind, iron deficiency anemia, for instance, is typically brought on by insufficient dietary iron intake, poor gastrointestinal absorption, or persistent blood loss (from parasite infections, for example, or even mild gastrointestinal hemorrhage) [32][9]. Pediatric age groups most at risk for developing IDA are post-menarcheal adolescent females and children aged 2 to 5 [7]. Inherited hemoglobin disorders like thalassemia and sickle cell anemia are transmitted in an autosomal recessive pattern and involve genetic mutations affecting the hemoglobin molecule. Sickle cell anemia arises from a point mutation in the β-globin gene, whereas thalassemia results from mutations that reduce or eliminate production of either the α- or β-globin chains [32][33]. As a result, both disorders lead to chronic hemolysis and anemia, manifesting with symptoms such as underweight, fatigue, pallor and growth delays in children. Their chronic anemic state often triggers compensatory mechanisms like extramedullary hematopoiesis, which can result in splenomegaly and skeletal deformities [5][37]. Elevated inflammatory markers like IL-6, TNF, and IFN-γ are connected to anemia of inflammation, which also frequently is the most common cause of anemia in pediatric patients after iron insufficiency [32]. These signals affect iron homeostasis by inhibiting erythropoiesis and increasing hepcidin overexpression. RBC generation is also decreased by chronic inflammation, which also suppresses the production of erythropoietin (EPO) and receptor expression. While treating the underlying problem, management focuses on enhancing oxygen delivery [7][44]. Apart from these, deficiency in folate and vitamin B12 inadequate nutritional intake, malabsorption, or elevated needs can cause anemia in children, which impairs DNA synthesis and results in inefficient formation of red blood cells. Poor diet, gastrointestinal issues, and specific hereditary diseases are among the causes [7][41].
4. Etiology
4.1 Fundamental Determinants
It includes the broad political economy, ecology, climate, and geography that influence national wealth, food systems, infrastructure, and health policy environments; among these, educational attainment, household and national wealth, prevalent cultural norms and behaviors (particularly related to gender and child feeding), and the development and application of health policies all influence whether or not communities have the means and social support necessary to prevent and treat anemia [18][46].
4.2 Underlying Determinants
Emphasizes on how reproductive patterns—early childbearing, high parity, and short birth spacing—create physiological vulnerabilities by putting the mother's iron and other micronutrient stores under repeated, closely spaced demands, which can result in chronic depletion that impacts both the mother and the child [18][20].
4.3 Intermediate Determinants
Inadequate maternal and child care practices (such as delayed or low-nutrient supplemental feeding, suboptimal breastfeeding), limited access to and utilization of health and nutrition services (such as antenatal care, iron-folate supplementation, deworming, and malaria prevention), inadequate health and nutrition knowledge and education (which undermines the adoption of preventative measures and appropriate feeding practices) [27][47], and inadequate water, sanitation, and hygiene (WASH) infrastructure (which increases exposure to diarrheal diseases and blood-loss parasites like hookworm) are the five main areas of the problem [21][25]. Families may not be able to obtain, absorb, or use enough micronutrients through these channels, and children continue to be at risk for and experience the worst effects of infectious diseases [18][19][20].
4.4 Immediate Determinants
Inadequate nutrient intake, absorption, and utilization directly result in micronutrient deficiencies (especially iron, folate, vitamin B??, and vitamin A), while chronic illness and recurrent infections cause systemic inflammation that hinders iron mobilization and directly kills red blood cells. These two processes work in concert because deficiencies impair immune function and make one more vulnerable to infection, while inflammation further decreases appetite and gastrointestinal function. The involvement of genetic hemoglobin diseases, like sickle-cell disease and other thalassemias, which naturally lower efficient erythrocyte synthesis and frequently speed up red cell death, is interwoven with these [18][19][20].
4.5 From Immediate Determinants to Anemia
The decline in hemoglobin is ultimately caused by two complementary pathways: first, decreased or ineffective erythrocyte production, which happens when essential building blocks, such as iron, vitamin B??, and folate, are insufficient, when bone-marrow activity is suppressed by chronic inflammation, or when inherited hemoglobinopathies interfere with normal red-cell synthesis; and second, increased erythrocyte loss, where red cells are chronically bled out by parasitic infections like hookworm or heavy menstruation, and hemolytic processes, whether brought on by infectious agents (like malaria) or genetic disorders like sickle-cell disease, speed up their destruction [30]. The fatigue, weakness, and stunted growth that define anemia are caused by circulating red-cell mass decreasing, tissue oxygen delivery failing, and hemoglobin levels falling below clinical thresholds when production is no longer able to keep up with the body's baseline turnover needs or when destruction exceeds creation [18][19][20].
5. Approaches To a Paediatric Patient And Recurrent Hospitalization Patterns
The origin of anemia can frequently be inferred from the patient's and their family's medical history. Labor, delivery, and the neonatal course—including any history of anemia, jaundice, phototherapy, or blood transfusions—should all be reviewed in the birth history. It is important to inquire about any past medical conditions and medication use. It is important to look for a history of trauma, infections, surgery, travel, and exposure to toxins, chemicals, medicines, or oxidants. Blood loss causes such epistaxis, gastrointestinal (GI) bleeding, or dysmenorrhea in young women should also be investigated [28][39]. A review of development and food intake, with an emphasis on important minerals such iron, folate, vitamin B12, and, in the case of newborns, milk intake, should be included of the dietary history. Given that various illnesses are prevalent in varying age groups, the patient's age should be taken into account [5][40]. Hospitalizations for anemia in pediatric patients can be either part of continuing supportive care (e.g., in transfusion-dependent situations) or for the acute management of problems (e.g., severe anemia, infections, or crises) [5][43].
5.1 Iron Deficiency Anemia
Nutritional iron deficiency (IDA) may be minor in young children and toddlers, but it can become severe in situations when dietary deficiencies are noticeable or when exacerbated by other variables (such as an infant's excessive consumption of cow's milk) [26]. One of the main factors that might cause sudden reductions in hemoglobin in teenage girls is severe monthly flow. In order to promptly restore hemoglobin levels and avoid consequences like heart failure or cognitive impairment, severe IDA frequently necessitates hospitalization for packed red blood cell (PRBC) transfusions and intravenous (IV) iron infusions [22][24]. According to studies, 8% of toddlers in developed environments may exhibit iron insufficiency, with 1% to 2% going on to develop clinical IDA [24]. Similar risk factors are present in developing nations, where prevalence may reach 20% to 40% [5][7].
5.2 Sickle Cell Disease
Chronic hemolytic anemia and vaso-occlusive crises are hallmarks of sickle cell disease, a genetically defined hemoglobinopathy. Severe pain is a hallmark of these crises, which can result in consequences such splenic sequestration, acute chest syndrome, or stroke [35][50]. Children with sickle cell disease (SCD) may need emergency and inpatient care due to these acute episodes. For instance, SCD is estimated to impact 1 in 365 African American babies in the US, and its consequences are a major reason why this population is admitted to hospitals [5][7].
5.3 Thalassemia and other congenital hemoglobin disorders
Children who have intermedia or severe thalassemia frequently require transfusions. Recurrent hospital stays are caused by long-term transfusion regimens and the treatment of iron excess (with chelation therapy) [37][49]. Furthermore, severe anemia can be caused early in childhood by other congenital red blood cell abnormalities, such as Fanconi anemia or Diamond–Blackfan anemia, which sometimes necessitate hospitalization for transfusion assistance and the treatment of consequences including bleeding episodes or recurring infections [5][34]. These estimates are to be considered to predict the probable patterns of recurrent hospitalizations in children with anemia [Fig. 2].

Fig. 2 Hospitalization patterns in pediatric patients.
6. Expanded Epidemiology and Population Insights
6.1 Global Prevalence
According to WHO survey statistics from the 2000s, anemia affects 25.4% of school-age children (5–12 years) and 28.4% of early adolescents (10–19 years) in 192 countries; South America, sub-Saharan Africa, and South Asia have the greatest prevalence [13][14]. Preschoolers (aged 1–5 years) displayed a 47.4% prevalence, in contrast, highlighting the fact that school age is a time of both lingering risk and new causes [13][48].
6.2 National Specific Prevalence
Overall, 23.4% of children aged 5 to 9 had anemia; of these, 15.6% had iron-deficiency anemia and 43.6% had "anemia of other causes," which primarily included hemoglobinopathies. 28.4% of teenagers aged 10 to 19 had anemia, with iron-deficient anemia accounting for 21.3%, "other causes" for 31.4%, and folate/B12 deficiency anemia for 25.6% [15][16].
6.3 Hemoglobinopathy Burden
Sickle cell disease (SCD) affects about 330,000 babies born worldwide each year, with the disease and its traits being most prevalent in sub-Saharan Africa, India, and the Middle East [17][7]. Around 1.7% of people worldwide have thalassemia trait; in Mediterranean and Southeast Asia, trait frequencies range from 5% to 30% [7][29].
6.4 Other Congenital/Enzyme Defects
Up to 5% of people in endemic areas carry the G6PD deficiency; severe hemolysis episodes typically appear in children aged 5 to 14, when exposed to oxidative stress [5][18]. Hereditary spherocytosis: around 0.02% to 0.05% worldwide; many go undetected until mild-to-moderate hemolysis in school-age children [7][36]. ? The scattered plot graphs [Fig. 3, Fig. 4] represents and further explains the expanded epidemiology in pediatric patients, along with their prevalence by age group, both worldwide and in India.
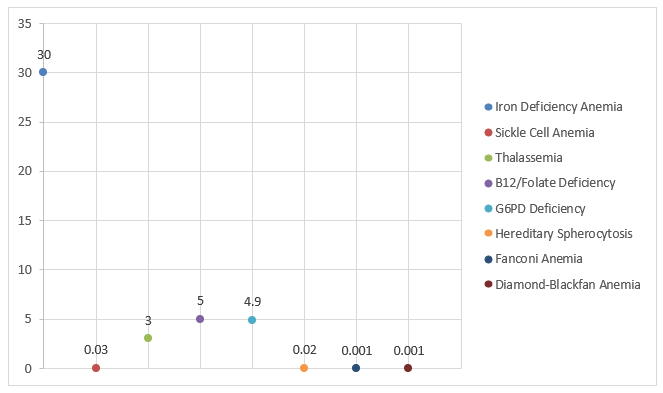
Fig. 3 Global Epidemiology of Paediatric Anaemias

Fig. 4 Anemia prevalence by age group (Global & National).
7. CONCLUSION
The complexity of anemia in school-age children and its substantial contribution to repeated hospitalizations are highlighted in this review. According to the investigation, a combination of chronic inflammatory illnesses, genetic abnormalities, and nutritional inadequacies is the main cause of anemia in this group. In particular, iron deficiency anemia continues to be the most prevalent, especially in settings where nutritional deficiencies and restricted access to medical treatment are prevalent. In addition, hereditary disorders such sickle cell disease and thalassemia significantly increase the burden of the disease, resulting in problems that require regular medical interventions in addition to persistent hemolysis. The conceptual model [Fig. 5] presents the determinants in a more simple and proper perspective, with much broader focus on the main contributors on a global scale.

Fig. 5 A model of anemia etiology. Determinants outlined are considered primary contributors to anemia globally.
The usefulness of categorizing anemia according to red blood cell morphology and indices—microcytic, normocytic, and macrocytic—is one of the main insights. This helps clinicians identify the underlying causes and adjust treatment strategies accordingly. Furthermore, the analysis emphasizes that, especially in low- and middle-income countries, the frequent hospitalizations linked to severe anemias place significant financial and psychological strains on families and healthcare systems in addition to the immediate clinical symptoms. Given these results, this promotes a thorough, multifaceted approach that consists of focused management regimens, dietary treatments, and early diagnosis through routine screening. In order to create novel treatments and preventative strategies that might lessen the frequency and severity of hospital admissions, it also urges more investigation into the interaction between genetic predispositions and environmental factors. In the end, treating pediatric anemia holistically is essential to reducing the wider societal and economic effects of this prevalent illness as well as to improving individual health outcomes.
Conflict Of Interest:
The authors declare no conflict of interest with anyone.
ACKNOWLEDGMENT:
The authors are grateful to Prof. (Dr.) Abhijeet Sengupta, Honourable Director, and Prof. (Dr.) Lopamudra Dutta, Respected Principal of Guru Nanak Institute of Pharmaceutical Science and Technology for providing the resources to prepare the review work.
REFERENCES



Souvik Das, Aruddha Mitra, Dr. Isita Tripathi, Tamalika Chakraborty, Dr. Jigisha Roy Panda*, Corelating Hemoglobin Status with Recurrent Hospitalization in School Children, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2811-2824. https://doi.org/10.5281/zenodo.15703864
 10.5281/zenodo.15703864
10.5281/zenodo.15703864
