1 Ashoka Institute of Pharmacy, Kosara, Chandrapur, Maharashtra-442401 India
2 Somayya Diploma in Pharmacy, Chandrapur, Maharashtra-442401 India
3 Dnyandeep College of Pharmacy, Ramtek, Nagpur, Maharashtra-441106 India
4 Ramratan School of Pharmacy, Wardha, Maharashtra-442001 India
5 PCET’s, School of Pharmacy, Pimpri Chinchwad University, Pune, Maharashtra
6 MUP's College of Pharmacy, Degaon, Risod, Washim, Maharashtra
7 Sahyadri College of Pharmacy, Methwade, Sangola, Maharashtra-413317
8 Shree Goraksh College of Pharmacy and Research, Khamgao, Chhatrapati Sambhajinagar, Maharashtra-431151 India
9 SAJVPM’s, College of Pharmaceutical Science and Research Centre, Kada, Beed, Maharashtra -414202.
This review article examines current developments in buccal adhesive drug delivery systems and offers fundamental ideas that young investigators might use to tackle formulation issues. Many macromolecular medications, including peptides, proteins, polysaccharides, and nucleic acids, have been developed as a result of advances in molecular science and gene technology. These drugs have higher pharmacological activity, site specificity, and few adverse effects. Because of its plentiful blood supply, porous mucosa, and high patient tolerance, the oral cavity is a perfect location for drug administration. It also has fewer Langerhans cells, which lessens its sensitivity to allergens, and it heals rapidly from stress or injury. Through the jugular vein, buccal medication administration provides direct access to the systemic circulation, avoiding hepatic first-pass metabolism and guaranteeing excellent bioavailability. This makes the buccal route a promising option for systemic drug delivery. Buccal bioadhesive films, which release drugs slowly and continuously in the oral cavity, offer significant advantages over conventional methods for treating various diseases. These films provide a controlled release mechanism, enhancing the effectiveness and reliability of drug delivery.
Oral drug administration is the most popular technique of controlled pharmaceutical delivery because to its high patient compliance, simplicity of self-medication, flexibility, and low invasiveness. However, it has certain downsides, including hepatic first-pass metabolism, enzymatic breakdown in the gastrointestinal system, and delayed absorption. Furthermore, around 25% of people, particularly pediatric and geriatric patients, have difficulty swallowing pills and capsules, resulting in insufficient adherence to therapy. This problem is compounded for individuals who lack access to water.
To address these challenges, alternative routes of administration such as parenteral methods have been established. However, parenteral routes are often costlier and entail lower patient compliance, particularly when repeated administrations are necessary. Consequently, various transmucosal and buccal routes have emerged as promising alternatives to oral drug administration, offering potential solutions to overcome these drawbacks.
In recent years, there have been significant advancements in drug formulations and administration methods. These novel formulations facilitate enhanced drug transport across tissues, leading to improved patient adherence and pharmacological response. One notable approach is drug administration via transmucosal routes, such as the nasal, rectal, vaginal, ocular, and oral mucosal linings. Among these, the mucoadhesive buccal drug delivery system stands out as particularly promising. This system enables sustained and controlled release of drugs at targeted sites over extended periods, while also being relatively painless compared to other routes.1,2 Buccal drug delivery offers a highly efficient method for enhancing bioavailability. Patients find this method appealing due to the ease of self-administration through the buccal cavity. Additionally, buccal dosage forms allow for the quick cessation of drug absorption if adverse reactions occur. Several types of buccal dosage forms are available, such as adhesive tablets, gels, and patches, with patches being particularly preferred for their flexibility and comfort.3-11
The buccal area of the oral cavity provides an ideal option for medication delivery, owing to its simplicity of administration and patient-friendliness. Buccal medication delivery refers to the administration of a medicament directly via the mucous membrane lining the inside of the mouth. This method is especially effective for both transmucosal and mucosal drug administration, capitalizing on the bioadhesive properties of specific polymers. These polymers become adhesive when hydrated, allowing them to securely attach to the mucosal surface.
Utilizing these bioadhesive polymers, drugs can be targeted to specific regions within the body, maintaining their presence for extended durations. This targeting capability not only enhances the local effects of the drug but also facilitates systemic absorption, providing broader therapeutic benefits. As a result, the buccal route provides a diverse and effective method of drug delivery, combining the benefits of longer drug retention at the site of action with the ease and comfort of non-invasive administration.13
Transmucosal drug delivery channels provide clear benefits over oral administration for systemic drug distribution. They make use of the mucosal linings of the nasal passages, rectum, vagina, eyes, and oral cavity. Depending on the medication, these advantages may include avoiding presystemic clearance in the gastrointestinal tract, avoiding first-pass metabolism, and creating an enzymatic environment that is more favorable for absorption.
Bioadhesive systems ensure prolonged drug exposure to the affected tissues, thereby optimizing therapeutic outcomes while minimizing systemic side effects. This approach not only improves drug retention and absorption efficiency but also enhances patient compliance by offering convenient and effective treatment options for localized oral conditions.
The capacity of a substance, synthetic or biological, to stick to biological tissues for a long time is known as bioadhesion. Specifically, when this adhesion occurs within the mucous layer, it is referred to as cohesion. Cohesion, which involves adherence to the mucus gel layer, is pivotal in designing pharmaceutical delivery systems.
Buccal drug administration stands out as a highly effective method for achieving systemic and local drug effects. This route allows for sustained delivery of drugs to a specific site for prolonged periods, enhancing both local treatment efficacy and systemic bioavailability. Because of the buccal mucosa's high blood supply and permeability, medications can enter the circulation more quickly, avoiding stomach enzyme breakdown and liver first-pass metabolism. Because of this, buccal medication administration is very beneficial for maximizing therapeutic results and guaranteeing effective drug delivery.
The closeness and length of contact between a treatment containing polymers and a mucous membrane are enhanced by mucoadhesion. There are many different kinds of mucoadhesive devices that have been produced, including tablets, films, patches, disks, ointments, and gels. Buccal patches are unique among them because of their increased comfort and flexibility. Polymer films or layers containing the medication and/or other ingredients make up these thin, non-dissolving matrix modified-release dosage forms.
Compared to alternatives like oral gels, buccal patches offer superior flexibility and comfort, addressing issues such as the short duration of action caused by easy removal by saliva. Further advantages of buccal patches include their ease of access, minimal enzymatic activity, suitability for drugs or substances causing mild and reversible irritation to the mucosa, painless administration, and effortless discontinuation. They can also incorporate permeation enhancers, enzyme inhibitors, or pH modifiers to enhance drug delivery efficiency. 14-22
Mucoadhesive polymers are a potential development in buccal medication delivery. The buccal patch, which was invented lately, is the most flexible and comfortable mucoadhesive device available; it is superior than tablets, films, patches, disks, strips, ointments, and gels. The buccal patch is a non-dissolving, thin matrix modified-release dosage form that is especially made for delivery to patients who are asleep or less cooperative. It is designed to attach efficiently to the mucous membrane of the mouth cavity.23
Ideal Characteristics of a Buccal Adhesive System34,35
The characteristics of an ideal buccal adhesive system include:
These characteristics collectively ensure that buccal adhesive systems are effective, safe, and well-tolerated for localized and systemic drug delivery applications.
Advantages of Buccal Patches:
Limitations of Buccal Patches
These limitations highlight considerations that need to be addressed when designing buccal drug delivery systems to ensure effectiveness and patient comfort.
Structural features of oral cavity28-31
The oral cavity consists of two main regions: the outer oral vestibule and the oral cavity proper. The vestibule, bordered by the cheeks, lips, teeth, and gums, serves as the external boundary, while the oral cavity proper extends from the teeth and gums to the fauces, with the hard and soft palate forming its roof. The buccal mucosa, similar to skin, protects underlying structures from foreign substances and includes the epithelium and basement membrane with connective tissue. The epithelium, a stratified squamous layer, undergoes keratinocyte differentiation and acts as a protective barrier. It is non-keratinized in areas like the soft palate and lips, and keratinized in the hard palate. The basement membrane, a layer of extracellular matrix, separates the epithelium from connective tissue and can limit the movement of certain macromolecules and complexes.36
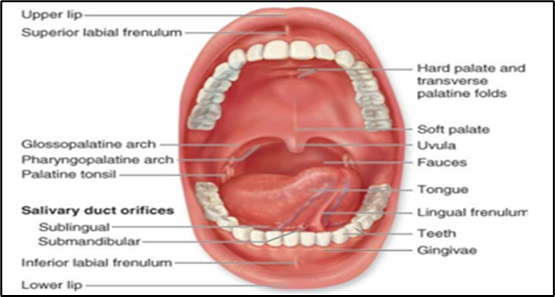
Fig. 1: Structure of Oral Cavity.
Drug Delivery Within the Oral Mucosal Cavity32,33
Drug delivery within the oral mucosal cavity involves various routes for administering medications. There are several ways to deliver drugs to the oral mucosa. Sublingual administration provides quick absorption and high bioavailability by delivering medication through the mucosal membranes under the tongue and floor of the mouth. This approach is well-liked, practical, and widely available. The mucosal membranes bordering the cheeks are the goal of buccal delivery. It offers a channel for drug delivery even though it is less permeable than the sublingual region; nonetheless, its absorption is slower and its bioavailability is lower. Depending on the mucosal location, local administration addresses different oral problems such as periodontal disease and ulcers, with different medication permeability and retention. Because of its permeability properties, the buccal mucosa is preferred for retentive oral transmucosal administration systems.
Novel Buccal Dosage Forms36.37
Novel buccal dosage forms provide innovative drug delivery methods. Buccal mucoadhesive tablets, which need moistening before placement, deliver drugs into the oral cavity or directly to the mucosal surface. Patches and films, consisting of thin, multilayered structures with an adhesive polymeric layer and an impermeable backing, allow unidirectional drug flow across the buccal mucosa. Semisolid preparations like bioadhesive gels or ointments are used for localized drug therapy, though they are less preferred by patients. Additionally, buccal bioadhesive powders, composed of bioadhesive polymers and the drug, offer another method for administration.
Buccal patches come in two main types: matrix and reservoir38,39
Buccal patches come in two primary types: matrix and reservoir. The matrix type, or bi-directional, uniformly distributes the drug within a hydrophilic or lipophilic polymer matrix, forming a medicated disc. The reservoir type, or unidirectional, features a separate drug-containing reservoir and additives, distinct from the adhesive layer and protected by an impermeable backing to prevent drug loss.
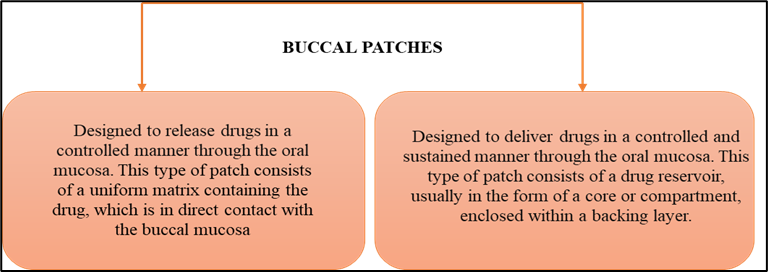
Fig. 2: Mechanism of Buccal Patches.
Mechanism of Bioadhesion40
The mechanism of bioadhesion involves several theories that explain the interaction between polymers and mucus, occurring in two distinct steps:
Contact Step: Initially, the mucoadhesive formulation makes contact with the mucus layer and mucosal membrane. This interaction causes the formulation to swell and spread on the mucosal surface.
Consolidation Step: Following the contact step, moisture from the environment or from the mucus activates the mucoadhesive material. This activation leads to the plasticization of the system, allowing mucoadhesive molecules to detach and form weak Vander Waals and hydrogen bonds with the mucus.
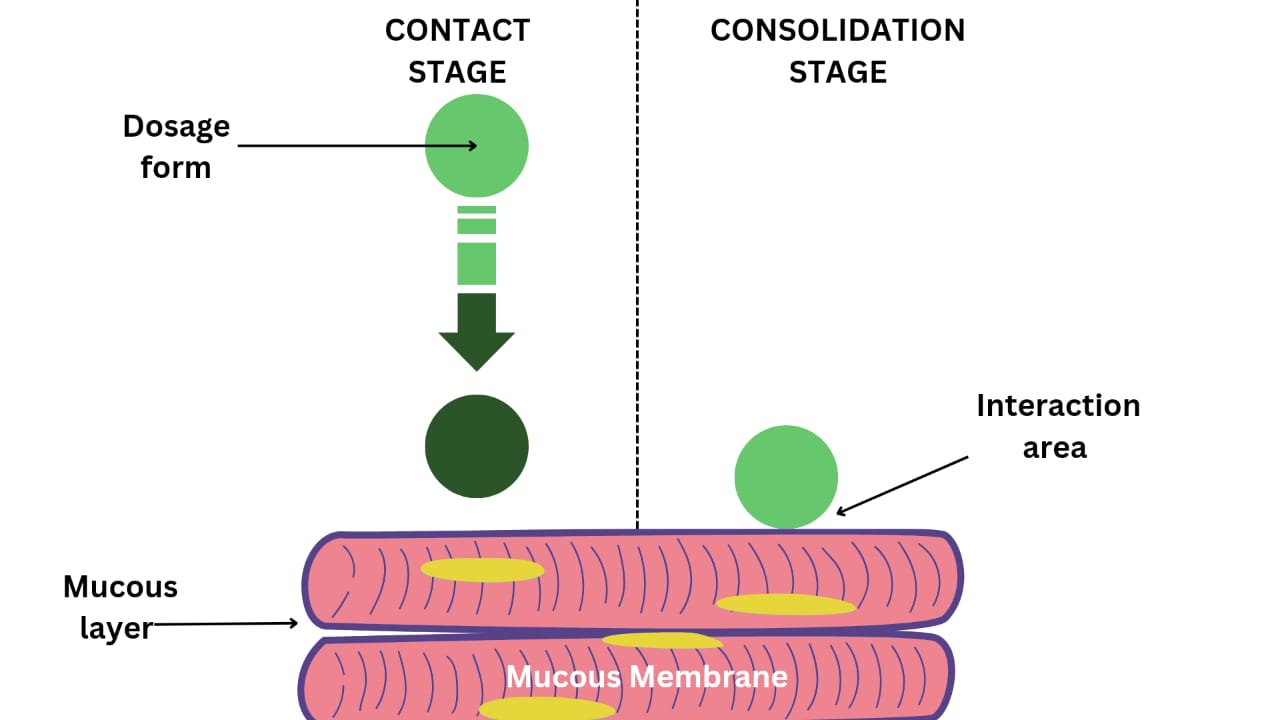
Fig. 3: Mechanism of Bioadhesion.41
Theories of bioadhesion44,45
Adhesion, the process by which molecules or particles of one substance stick to the surface of another, is crucial in numerous natural and industrial processes. By exploring these theories, scientists aim to deepen our understanding of adhesion phenomena, which have implications ranging from biological systems to the development of advanced materials.
Electronic Theory
The Electronic Theory posits that when an adhesive polymer contacts the mucus glycoprotein network, variations in electronic structures cause electron transfer, forming an electrical double layer at the interface. This interaction generates attractive forces that enhance adhesion.
Adsorption Theory
According to the Adsorption Theory, when the buccal mucosal surface and an adhering material first make contact, they each possess surface energies. This interaction results in two types of chemical bonds: primary chemical bonds, mainly covalent, and secondary chemical bonds, including electrostatic forces, Van der Waals forces, hydrogen bonds, and hydrophobic interactions. These bonds contribute to the adhesion between the materials.
Wetting Theory
The theory pertains to liquid or low-viscosity bioadhesives that exhibit an affinity for surfaces, facilitating their easy spread. It describes how drug dosage forms move through biological layers, proposing that a lower contact angle signifies stronger affinity and improved spreadability. Optimal spreadability is achieved when the contact angle approaches zero. This theory quantifies the spreading process using a specific equation known as the spreadability coefficient (SAB).
SAB = γ B – γ a – γ AB
Where γ B represents the surface energy and γ A denotes the interfacial energy.
Diffusion Theory
The Diffusion Theory states that when polymer chains sift through the mucus, a semi-permanent sticky bond occurs. The diffusion coefficient and the length of time when polymer chains and mucus are in contact determine the penetration depth. Because the molecular weights of the cross-links vary, this coefficient falls with increasing cross-link density.
Fracture Theory
This theory is the most extensively scrutinized theory for elucidating the mucoadhesion mechanism.
According to this theory, the ease of separating two surfaces after adhesion depends directly on the adhesive bond strength. The fracture strength, which reflects this adhesive strength, is calculated as follows: 46-48
G= (E ε/L) ½
Composition of buccal patches45
This drug delivery systems consist of several essential components:
Active Pharmaceutical Ingredient (API): In buccal drug delivery systems, the active pharmaceutical ingredient (API) plays a crucial role by enhancing and prolonging the drug's contact with the mucosa, ensuring the desired therapeutic effect. Key pharmacological properties such as melting point, chemical functionality, and molecular weight significantly influence the drug's diffusion through the buccal mucosa and patch effectiveness.49
When choosing drugs for buccal delivery, key criteria include a low conventional single dose, a biological half-life of 2 to 8 hours for controlled release, passive oral absorption, and the absence of unpleasant taste, irritancy, allergenicity, or tooth discoloration. These factors are crucial to ensure reliable and effective therapeutic outcomes.50
Mucoadhesive Polymers (Buccal Adhesive polymer): Both manufactured and natural polymers stick to the mucus layer that covers the mucosal epithelial surface, making up a large portion of it.49 The initial stage in developing mucoadhesive dosage forms involves selecting and characterizing suitable mucoadhesive polymers. These polymers are also utilized in matrix devices to control the release duration of drugs by incorporating them into the polymer matrix.51,52
Ideal characteristics of mucoadhesive polymers include:
Mucoadhesive Polymers 22,49,52,53,54
Mucoadhesive polymers are categorized based on their essential criteria for drug delivery systems. Natural or semi-natural polymers like agarose, chitosan, gelatine, hyaluronic acid, and various gums (e.g., guar, hakea, xanthan) are commonly used. Synthetic polymers include cellulose derivatives such as CMC, HEC, HPC, HPMC, and poly (acrylic acid)-based polymers like CP and PC. These polymers vary in aqueous solubility properties; for example, CP, HEC, HPC are soluble in water below 38°C, while sodium CMC, sodium alginate, and chitosan are water-insoluble. They also differ in charges: cationic polymers like chitosan, anionic polymers such as CMC and PAA, and non-ionic polymers like PVA and PVP. These polymers engage in various bonding interactions including covalent bonding with cyanoacrylate, hydrogen bonding with acrylates, and electrostatic interactions with chitosan. Each polymer type's unique characteristics determine their effectiveness in mucoadhesive applications for efficient drug delivery through mucosal surfaces.
Backing Membrane
When it comes to attaching bioadhesive devices to the mucous membrane, the backing membrane is essential. This barrier must be inert and impervious to medications and substances that increase penetration. Among the compounds frequently utilized are carbopol, magnesium stearate, hydroxypropyl cellulose (HPC), carboxymethyl cellulose (CMC), methylcellulose (HPMC), and polycarbophil. The structural integrity of these materials ensures that the device remains stable and that no unintentional substance transfer occurs, which might affect the medication delivery system's function.22,55.
Diluents
For direct compression, lactose DC is the preferred diluent due to its strong physico-mechanical characteristics, good water solubility, and agreeable taste. Starch or microcrystalline cellulose are two more analogous diluent choices.58
Sweetening agents such as sucralose, aspartame, and mannitol are commonly used. Flavoring agents include menthol, vanillin, and clove oil, among others.59
Permeation enhancers56
Permeation enhancers help drugs pass through the buccal mucosa. However, buccal drug delivery encounters a challenge: drugs have limited flux across the mucosal epithelium, reducing their bioavailability. Researchers are exploring diverse compounds to improve drug penetration and absorption through the mucosa.
Surfactants, including ionic types like sodium laurylsulfate and non-ionic types such as Tween 80, along with bile salts like sodium deoxycholate, are utilized to enhance drug permeation through the buccal mucosa. Fatty acids such as oleic acid and chelating agents like EDTA are also employed for this purpose. Sulfoxides like dimethyl sulfoxide (DMSO) and polyols such as propylene glycol and glycerol are included in formulations to improve drug absorption and bioavailability. These compounds collectively address challenges in drug flux across the mucosa, enhancing drug delivery effectiveness.
Plasticizers
Plasticizers are crucial additives that impart flexibility and softness to thin polymer films or blends. Examples like glycerol, propylene glycol, PEG 200, PEG 400, and castor oil are commonly used. These agents serve a dual purpose in drug delivery systems: they aid in releasing drugs from the polymer matrix and improve their penetration through the mucosal barrier. The choice of plasticizer depends on its ability to dissolve the polymer and adjust interactions between polymer chains. Properly integrated with the polymer, these substances reduce molecular rigidity, thereby enhancing flexibility and ensuring the effective functioning of the delivery system.57
Methods of preparation of buccal patches
1. Solvent casting
Mucoadhesive buccal patches are made using a process called solvent casting, which involves weighing and mixing materials in a solvent system with a plasticizer until a clear solution is achieved. Pouring the solution onto a petri dish, it is then allowed to evaporate beneath inverted funnels for 24 to 48 hours at 20 to 25 degrees Celsius. The release liner is laminated with a protective backing once the solvent has evaporated. After that, the laminate is sliced into patches with the required dimensions. Despite being efficient, solvent casting has disadvantages such as longer production times, increased expenses, and solvent use-related environmental issues. These difficulties can be lessened by using substitute techniques, such as hot-melt extrusion.60
2. Direct Milling
Solvents are typically avoided in the manufacturing of buccal patches using solvent-free techniques such as direct milling or kneading. Medications and excipients are mechanically mixed to achieve the desired consistency without the need for liquid additives. The material is blended, rolled onto a release liner to achieve the correct thickness, and optionally covered with an impermeable backing membrane. This membrane helps control drug release direction, minimize drug loss, and ensure patch integrity during application.
The process begins by combining the Active Pharmaceutical Ingredient (API) and excipients through direct milling, ensuring thorough mixing and uniform distribution of components. Once blended, the mixture is fed into rollers, where it is rolled out to achieve the desired thickness and uniformity. Subsequently, a backing material is carefully laminated onto the blended film to provide structural support and to protect the drug-loaded layer. This lamination step ensures the integrity of the buccal patch during handling and application. Finally, the finished film is collected, ready for further processing or packaging. This method of production enables precise control over drug dosage and release characteristics while maintaining the stability and functionality of the buccal delivery system.60
While the performance differences between patches produced by both methods may be minimal or even negligible, the solvent-free approach is preferred due to its elimination of residual solvents and the associated potential health concerns. This method ensures a safer and more environmentally friendly manufacturing process for buccal patches.19
3. Hot Melt Extrusion
The drug and polymers are blended in a sigma blade mixer for 10 minutes, with the gradual addition of the plasticizer. Granulation takes place in the presence of an antisticking agent. The resulting granules are stored overnight at a controlled temperature and then sieved through a 250µm sieve to eliminate any surplus powder and ensure consistent particle size. The dry granular material is fed into the extruder. Finally, the films are cut to the desired dimensions at the end of the preparation process.62
4. Semisolid Casting
In the semisolid casting process, a solution of water-soluble film-forming polymer is first prepared. This solution is then combined with another solution containing an acid-insoluble polymer and sodium hydroxide or ammonium hydroxide. After adding the appropriate amount of plasticizer to create a gel mass, films or ribbons are formed from the mixture using heated drums.21
5. Rolling Method
In this method, a substrate is coated with solution or suspension containing the drug, often dissolved in water or a water-alcohol mixture. The coated film is then dried on rollers until it achieves the desired size and consistency.62
Evaluation of buccal patches63
On an agar plate, the buccal patches are allowed to swell for two hours. After that, the surface pH of the swelling patch is measured by applying pH paper to it. This measurement aids in determining the patch surface's acidity or alkalinity.14
A micrometer is used to measure each film's thickness at five distinct locations: the center and four corners. This ensures accurate assessment of film thickness, crucial for uniformity and performance evaluation.16
Five patches are randomly chosen from each batch, and their weights are measured. Weight variation is then calculated electronically.22
A single patch is repeatedly folded at a fixed point until it breaks or can sustain a maximum of 200 folds without breaking. This is how the folding endurance of patches is measured.19
Each Buccal patch, initially weighed as W1, is placed individually on 2% agar gel plates. After that, the plates are kept in an incubator with a temperature control of 37°C ± 1°C and are watched for changes. The patches are taken out of the gel plates every hour for a maximum of three hours, and then they are gently dried using filter paper to remove any extra surface water. We next use the reweighed swollen patches (W2) to calculate the swelling index (SI).16
Each manufactured film is weighed separately, and it is kept at room temperature for 24 hours in a desiccator filled with calcium chloride. After then, the films are weighed until a steady weight is achieved at certain intervals. The following formula can then be used to determine the percentage of moisture content:64
% Moisture Content = [Starting weight - Ending weight / Ending weight] × 100
The evaluation of patch integrity under dry conditions was digitally conducted by measuring the percentage of moisture loss. Three patches, each with a diameter of 1cm, were accurately cut and weighed. Next, the films were set inside fused anhydrous calcium chloride desiccators. We removed the films and weighed them once more after a span of 72 hours. The formula 65 was used to determine the average percentage of moisture loss for each of the three patches:
percentage moisture loss = [Starting weight - Ending weight / Ending weight] × 100
Three distinct film units, each measuring 20 mm in diameter, are placed within volumetric flasks holding 100 mL. They are stirred for the whole day while submerged in 100 milliliters of solvent. The findings are examined at certain wavelengths using a UV spectrophotometer after the solutions have been filtered and diluted as needed. The average drug content is calculated based on the readings from the three film units.64
a. SEM
The films' surface morphology was analyzed using a scanning electron microscope after gold-sputtering under vacuum conditions at an 80 kV acceleration voltage.
b. Differential Scanning Calorimeter 67
This study aimed to identify the crystal arrangement of the pure drug, excipients, polymer, physical mixtures, and selected drug-loaded films. Precisely weighed samples were placed in aluminium pans, and scans were conducted under a nitrogen stream.
Circular patches (2.3 cm²) swell on agar plates with simulated saliva, pH-adjusted and incubated at 37°C ± 0.5°C. Samples are weighed periodically (0.25, 0.5, 1, 2, 3, and 4 hours) to measure wet weight, followed by drying for 7 days in a desiccator with anhydrous calcium chloride until reaching constant dry weight.16
Buccal patches were placed to freshly excised buccal mucosa from lambs and rabbits on a glass slide for the ex-vivo mucoadhesion test. For thirty seconds, the patches were gently pushed into the mucosa after being wet with pH 6.8 phosphate buffer. Next, 200 mL of pH 6.8 phosphate buffer were added to the glass slide arrangement, and it was kept at 37°C ± 1°C. Patch adhesion was seen for 12 hours after two minutes of stirring at 50 rpm, which mimicked buccal cavity conditions. Throughout the test, modifications to the drug's composition, color, form, and patch integrity were closely observed and recorded.14
Using a pH 6.8 phosphate buffer at 37°C ± 0.5°C and 50 rpm, the USP XXIII-B rotating paddle method is used to evaluate drug release from bilayered and multilayered patches. Using instant adhesive, the backing layer of the patch is attached to a glass disk within the vessel. 5 mL samples are periodically taken out of the experiment and replaced with new medium. They are then filtered, and once they have been diluted, their drug concentration is examined. 22
The receptor compartment contains pH 6.8 phosphate buffer stirred at 50 rpm using a magnetic bead to maintain fluid dynamics. Samples are periodically withdrawn for drug content analysis.16
A Brookfield LVDV II viscometer with spindle four of a helipath was used to create and evaluate aqueous solutions with the same amounts of plasticizer and polymer as in the patches. Measurements were taken at 20 rpm and room temperature, with reported values representing the average of three measurements.68
Bioadhesive patches were kept for six months in an aluminium foil-lined petri dish at 37.5°C and 75% relative humidity. Tests were carried out every month to evaluate how release behavior, residence time, look, and drug content changed over time. The information displayed is the mean of three measurements. After the storage time, the structure of fresh and old medicated patches was compared using scanning electron microscopy (SEM).68
With a tensile tester, the mechanical characteristics of films or patches are assessed. A perfect 60 x 10 mm film strip is clamped between two grips that are 3 cm apart. When the strip splits, one grip stays still while the other travels at a speed of two millimeters per second. At the break, the force and elongation are noted. The formula for calculating tensile strength (kg/mm2) is Force at break (kg) divided by the specimen's initial cross-sectional area (mm2).69
Buccal patches are subjected to stability testing with human saliva obtained from subjects between the ages of 18 and 50. After putting each patch in a different Petri dish with 5 mL of saliva, it is incubated for 6 hours at 37°C ± 0.2°C in a temperature-controlled oven. Monitoring occurs every 0, 1, 2, 3, and 6 hours to record any changes in color, shape, and drug content.22
CONCLUSION
Improving treatment standards is crucial in modern medicine. Buccal drug delivery systems offer advantages by bypassing GIT and liver portal system, enhancing drug bioavailability, and promoting patient compliance. Patches are innovative in pharmaceuticals due to their convenience and patient-friendly attributes, with their small size and thickness improving adherence over traditional tablets. Patches prevent the first-pass effect by administering medication through the buccal mucosa, which permits absorption into the venous system draining from the cheek. Buccal patches consist of thin, non-dissolving matrices with modified release characteristics, containing drug and excipients in polymer layers. They may include a mucoadhesive layer ensuring sustained drug release by adhering to the oral mucosa, promising effective drug delivery while overcoming challenges of conventional oral routes.
CONFLICT OF INTEREST:
The authors have no conflicts of interest with regards to the content of this review article.
REFERENCES


Achal Ghate, Mozes Durgawad, Dr. Amit Ingle, Shraddha Lunge, Ankita Jatale, Pallavi Bhutekar, Sana Jamadar, Madhuri Shrawane, Dr. Vishal Rasve, Comprehensive Review on Advancements in Buccal Drug Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 846-862. https://doi.org/10.5281/zenodo.17826486
 10.5281/zenodo.17826486
10.5281/zenodo.17826486
