1Department of Pharmacology, Divine College of Pharmacy, Satana (Nashik), India
2Department of Pharmaceutical Chemistry, Divine College of Pharmacy, Satana (Nashik), India
Antibiotic resistance has emerged as a global health crisis, threatening the efficacy of life-saving antimicrobial therapies. Pharmacologists play a pivotal role in combating this challenge through drug discovery, optimizing antibiotic use, conducting clinical research, promoting antimicrobial stewardship, educating healthcare professionals, and shaping policy frameworks. Their involvement in developing novel antibiotics, ?-lactamase inhibitors, and combination therapies helps counteract bacterial resistance mechanisms. By leveraging pharmacokinetics and pharmacodynamics (PK/PD) modeling, pharmacologists design optimized dosing regimens to enhance antibiotic effectiveness while minimizing resistance selection. Additionally, they contribute to clinical trials and surveillance programs, ensuring that new and existing antibiotics remain effective against evolving bacterial threats. Antimicrobial stewardship programs (ASPs) benefit from pharmacologists’ expertise in rational antibiotic prescribing, dose adjustments, and resistance monitoring, reducing unnecessary antibiotic use. They also play a crucial role in educating healthcare providers and the public about responsible antibiotic use and resistance prevention. Furthermore, their contributions to healthcare policies and regulatory frameworks help shape antibiotic use guidelines, restrict over-the-counter sales, and regulate antibiotic use in agriculture. Beyond conventional antibiotics, pharmacologists are pioneering research in alternative therapies, including bacteriophage therapy, antimicrobial peptides, anti-virulence strategies, and nanotechnology-based drug delivery systems. These innovations offer promising solutions to tackle multidrug-resistant (MDR) and extensively drug-resistant (XDR) bacterial infections. A multifaceted approach, integrating scientific innovation, clinical application, public awareness, and policy enforcement, is essential to preserve antibiotic efficacy and prevent resistance from escalating into a global health catastrophe.
Antibiotics are a class of antimicrobial agents used to prevent and treat bacterial infections. These drugs either kill bacteria (bactericidal) or inhibit their growth (bacteriostatic) by targeting essential bacterial structures and processes, such as cell wall synthesis, protein synthesis, DNA replication, or metabolic pathways [1]. Since the discovery of penicillin by Alexander Fleming in 1928, antibiotics have revolutionized modern medicine, saving millions of lives by effectively treating infectious diseases. Antibiotic resistance is the ability of bacteria to survive and multiply despite the presence of antibiotics that were once effective against them. This occurs when bacteria develop genetic changes or acquire resistance genes from other bacteria, allowing them to neutralize or evade the drug’s effects. As a result, infections caused by resistant bacteria become more difficult to treat, leading to longer illnesses, higher medical costs, and increased mortality rates [2]. Over the years, antibiotic resistance has emerged as a serious global health concern, primarily driven by the overuse and misuse of antibiotics in human medicine, veterinary practice, and agriculture. The rapid spread of multidrug-resistant (MDR) bacteria threatens the efficacy of existing antibiotics, raising the possibility of a post-antibiotic era where common infections become untreatable. Without urgent action, antibiotic resistance could undermine decades of medical advancements, making even routine surgeries, cancer treatments, and organ transplants increasingly risky. Antibiotic resistance occurs when bacteria evolve mechanisms to withstand the effects of antibiotics that were once effective against them. This phenomenon arises due to genetic mutations or the acquisition of resistance genes through horizontal gene transfer. Resistant bacteria can survive antibiotic exposure, multiply, and spread, making infections harder to treat. The development of antibiotic resistance is driven by several factors, including overuse, misuse, and inappropriate prescribing of antibiotics. Additionally, inadequate infection control measures, poor hygiene, and insufficient surveillance systems contribute to the rapid spread of resistant bacteria across communities, hospitals, and the environment [3,4]. The aim of this review is to understand antibiotic resistance from a pharmacological perspective. It will explore the mechanisms by which bacteria develop resistance to antibiotics, including enzymatic degradation, target modification, efflux pumps, and biofilm formation. Additionally, the review will discuss the pharmacokinetics and pharmacodynamics of antibiotics, how misuse and overuse contribute to resistance and the role of novel drug development in overcoming resistance. It will also highlight strategies to combat resistance, such as combination therapy, antibiotic stewardship, and alternative therapies like bacteriophages and antimicrobial peptides.
How Antibiotics Work
Antibiotics work by targeting specific bacterial structures and functions essential for survival and replication. Depending on their mode of action, antibiotics can be bactericidal (killing bacteria) or bacteriostatic (inhibiting bacterial growth). The major mechanisms by which antibiotics exert their effects include inhibition of cell wall synthesis, disruption of cell membrane integrity, inhibition of protein synthesis, inhibition of nucleic acid synthesis, and inhibition of metabolic pathways. Each of these mechanisms selectively targets bacterial components, making antibiotics effective against bacteria while minimizing harm to human cells [5,6].
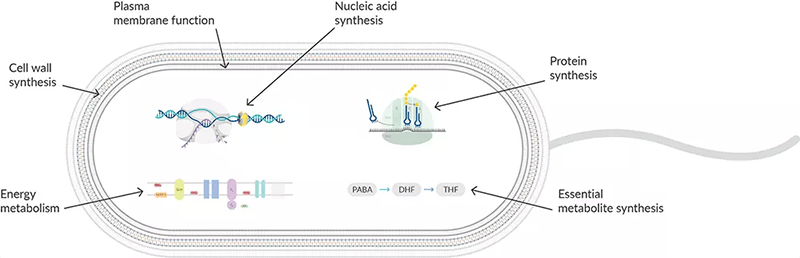
Figure 1: Mechanism of Antibiotic Action
1. Inhibition of Cell Wall Synthesis
Many antibiotics kill bacteria by preventing the synthesis of the bacterial cell wall, a crucial structure that provides mechanical strength and protects against osmotic pressure. The bacterial cell wall is primarily composed of peptidoglycan, a mesh-like polymer that maintains the shape and integrity of bacterial cells. Antibiotics such as β-lactams (penicillins, cephalosporins, carbapenems, monobactams) work by binding to penicillin-binding proteins (PBPs), which are responsible for cross-linking peptidoglycan strands. This inhibition weakens the bacterial cell wall, leading to lysis and cell death. Similarly, glycopeptides (vancomycin, teicoplanin) bind to the D-Ala-D-Ala terminal of peptidoglycan precursors, blocking their incorporation into the growing cell wall. Since human cells lack a peptidoglycan cell wall, these antibiotics specifically target bacteria, making them highly effective against Gram-positive bacteria such as Staphylococcus aureus and Streptococcus pneumoniae [5].
2. Disruption of Cell Membrane Integrity
Some antibiotics kill bacteria by directly disrupting the structure and function of the bacterial cell membrane, leading to leakage of essential ions and molecules. This mechanism is particularly effective against Gram-negative bacteria, which have an outer membrane that acts as a barrier against many antibiotics. Polymyxins (Polymyxin B, Colistin) interact with the lipopolysaccharide (LPS) layer of Gram-negative bacteria, displacing divalent cations and increasing membrane permeability. This results in leakage of cellular contents and bacterial death. Similarly, daptomycin, a lipopeptide antibiotic, disrupts bacterial membrane potential by forming pores that cause ion leakage, leading to cell death. These antibiotics are often used as a last resort for treating multidrug-resistant bacteria, such as Pseudomonas aeruginosa and Acinetobacter baumannii. However, because they can also affect human cell membranes, their use is often associated with toxicity, particularly nephrotoxicity and neurotoxicity.
3. Inhibition of Protein Synthesis
Protein synthesis is essential for bacterial growth and survival, and several classes of antibiotics target bacterial ribosomes to inhibit this process. Bacterial ribosomes consist of 30S and 50S subunits, which are structurally different from human ribosomes (40S and 60S subunits), allowing selective inhibition of bacterial translation. Aminoglycosides (gentamicin, streptomycin, tobramycin) bind to the 30S ribosomal subunit, causing misreading of mRNA and the production of nonfunctional or toxic proteins. Tetracyclines (doxycycline, minocycline) also bind to the 30S subunit, blocking the attachment of tRNA and preventing protein elongation. Meanwhile, macrolides (erythromycin, azithromycin, clarithromycin) and chloramphenicol target the 50S ribosomal subunit, inhibiting peptide bond formation and stopping protein synthesis. Oxazolidinones (linezolid) further interfere with ribosomal assembly, preventing bacterial translation altogether. Because protein synthesis inhibitors do not directly kill bacteria, many of them are bacteriostatic, meaning they slow bacterial growth rather than causing immediate cell death. These antibiotics are commonly used to treat respiratory, skin, and intracellular bacterial infections caused by Streptococcus pneumoniae, Mycoplasma pneumoniae, and Rickettsia spp.
4. Inhibition of Nucleic Acid Synthesis
DNA and RNA synthesis are crucial for bacterial replication and survival. Some antibiotics target enzymes involved in nucleic acid synthesis, preventing bacteria from multiplying. Fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin) inhibit DNA gyrase (topoisomerase II) and topoisomerase IV, which are essential for bacterial DNA replication. By blocking these enzymes, fluoroquinolones prevent DNA unwinding and supercoiling, leading to bacterial cell death. Rifamycins (rifampin, rifabutin) work by inhibiting RNA polymerase, thereby blocking bacterial transcription and preventing mRNA production. This makes rifamycins highly effective against Mycobacterium tuberculosis and Neisseria meningitidis. Another important antibiotic, metronidazole, generates reactive radicals that directly damage bacterial DNA, making it particularly useful against anaerobic bacteria such as Clostridium difficile and Bacteroides fragilis. Since human cells do not rely on these bacterial enzymes for nucleic acid synthesis, these antibiotics are highly selective for bacterial infections, but fluoroquinolones are associated with side effects like tendon rupture and nerve damage.
5. Inhibition of Metabolic Pathways
Some antibiotics work by blocking essential metabolic pathways in bacteria, preventing them from synthesizing key molecules needed for survival. One of the most common targets is folic acid synthesis, which bacteria require for DNA and RNA production. Since bacteria must synthesize folic acid while human cells obtain it from their diet, inhibitors of bacterial folate metabolism are highly selective. Sulfonamides (sulfamethoxazole, sulfadiazine) inhibit dihydropteroate synthase (DHPS), an enzyme involved in folic acid synthesis. Trimethoprim, often combined with sulfamethoxazole as co-trimoxazole (TMP-SMX), inhibits dihydrofolate reductase (DHFR), further blocking folic acid metabolism. These antibiotics are commonly used to treat urinary tract infections (UTIs), respiratory infections, and Pneumocystis jirovecii pneumonia in immunocompromised patients. Because bacteria can develop resistance by acquiring alternative metabolic pathways, these antibiotics are often used in combination therapy to increase their effectiveness [5-8].
Mechanisms of Antibiotic Resistance
Antibiotic resistance is a major global health threat that occurs when bacteria evolve mechanisms to survive exposure to antibiotics. This resistance can develop due to spontaneous genetic mutations or the acquisition of resistance genes from other bacteria. Resistant bacteria can neutralize the effects of antibiotics through various biochemical and structural adaptations. The key mechanisms of antibiotic resistance include enzymatic degradation of antibiotics, efflux pump activity, modification of antibiotic targets, reduced permeability, biofilm formation, bypass pathways, and horizontal gene transfer. Understanding these mechanisms is crucial for developing strategies to combat antibiotic resistance.

Figure 2: Antibiotic Resistance
1. Enzymatic Degradation or Modification of Antibiotics
One of the most common resistance mechanisms is the production of bacterial enzymes that degrade or chemically modify antibiotics, rendering them ineffective. Many bacteria produce specific enzymes that break down antibiotic molecules before they can act on their bacterial targets. A well-known example of this mechanism is β-lactamase enzymes, which hydrolyze the β-lactam ring present in antibiotics such as penicillins, cephalosporins, and carbapenems. Some bacteria, like Escherichia coli and Klebsiella pneumoniae, produce extended-spectrum β-lactamases (ESBLs) and carbapenemases, making them resistant to a wide range of β-lactam antibiotics. Another example is aminoglycoside-modifying enzymes (AMEs), which chemically modify aminoglycoside antibiotics (e.g., gentamicin, tobramycin) by acetylation, phosphorylation, or adenylation, preventing them from binding to bacterial ribosomes. Enzymatic degradation is a particularly dangerous form of resistance because it can rapidly spread among bacterial populations, making once-effective antibiotics obsolete. The widespread production of these enzymes has led to the emergence of multidrug-resistant (MDR) bacterial strains, complicating treatment options.
2. Efflux Pumps (Active Antibiotic Expulsion)
Efflux pumps are membrane transport proteins that actively expel antibiotics from bacterial cells, reducing their intracellular concentration and limiting their effectiveness. These pumps function by recognizing and exporting antibiotic molecules out of the bacterial cell, preventing them from reaching their target sites. Efflux pumps are present in both Gram-positive and Gram-negative bacteria and can confer resistance to multiple classes of antibiotics, including fluoroquinolones, tetracyclines, and macrolides. Some of the major efflux pump families include:
Efflux pumps are particularly problematic because they can confer multidrug resistance (MDR), making bacteria resistant to several antibiotic classes simultaneously. Moreover, bacteria can upregulate efflux pump activity in response to antibiotic exposure, further enhancing their resistance.
3. Target Modification (Alteration of Antibiotic Binding Sites)
Bacteria can develop resistance by modifying the target molecules that antibiotics typically bind to, preventing the drug from exerting its effect. This mechanism involves genetic mutations or enzymatic alterations in bacterial structures, such as ribosomes, DNA gyrase, or penicillin-binding proteins (PBPs). A classic example of target modification is methicillin-resistant Staphylococcus aureus (MRSA), which produces an altered penicillin-binding protein (PBP2a) that has a low affinity for β-lactam antibiotics. This modification prevents β-lactam antibiotics from inhibiting bacterial cell wall synthesis, leading to resistance. Another example is resistance to fluoroquinolones, which arises due to mutations in the gyrA and parC genes, altering DNA gyrase and topoisomerase IV. These mutations reduce antibiotic binding affinity, allowing bacteria to continue DNA replication despite antibiotic presence. Target modification is particularly concerning because it often leads to high-level resistance, meaning that even increased doses of antibiotics fail to inhibit bacterial growth.
4. Reduced Permeability (Limited Antibiotic Entry)
Some bacteria develop resistance by decreasing membrane permeability, thereby limiting the entry of antibiotics into the cell. This is especially common in Gram-negative bacteria, which possess an outer membrane that acts as an additional barrier against antibiotic penetration. Bacteria achieve reduced permeability primarily by downregulating or mutating porin proteins, which are channels that facilitate the passive diffusion of antibiotics into bacterial cells. For example, Pseudomonas aeruginosa and Klebsiella pneumoniae can decrease the expression of porins such as OmpF and OmpC, reducing β-lactam and carbapenem uptake. This mechanism is often seen in carbapenem-resistant Enterobacteriaceae (CRE), where decreased porin expression, combined with other resistance mechanisms like efflux pumps and β-lactamase production, leads to highly resistant bacterial strains.
5. Biofilm Formation (Protective Bacterial Communities)
Bacteria can form biofilms, which are structured communities of bacteria encased in a self-produced extracellular polymeric substance (EPS). Biofilms protect bacteria from antibiotics, host immune responses, and environmental stressors. Within a biofilm, bacteria exhibit several resistance-enhancing characteristics:
Biofilms are commonly associated with chronic infections, such as Pseudomonas aeruginosa infections in cystic fibrosis patients, Staphylococcus aureus infections in medical devices, and Helicobacter pylori biofilms in gastric ulcers. These infections are difficult to treat and often require prolonged or combination antibiotic therapy.
6. Bypass Pathways (Metabolic Adaptations to Overcome Antibiotic Effects)
Some bacteria develop alternative metabolic pathways to bypass the action of antibiotics. This mechanism allows bacteria to continue essential cellular processes even in the presence of antibiotic inhibitors. For example, sulfonamide-resistant bacteria acquire an alternative dihydropteroate synthase (DHPS) enzyme that is not inhibited by sulfonamide antibiotics, allowing continued folic acid synthesis. Similarly, vancomycin-resistant enterococci (VRE) modify their cell wall precursors by replacing D-Ala-D-Ala with D-Ala-D-Lac, preventing vancomycin from binding and inhibiting cell wall synthesis. These bypass strategies allow bacteria to survive antibiotic treatment without directly neutralizing the drug.
7. Horizontal Gene Transfer (Acquisition of Resistance Genes from Other Bacteria)
Bacteria can acquire resistance genes from other bacterial species through horizontal gene transfer (HGT), a process that enables the rapid spread of resistance traits. There are three main types of HGT:
A notorious example is the New Delhi Metallo-β-lactamase (NDM-1) gene, which has spread globally through plasmid-mediated conjugation, conferring resistance to carbapenems in E. coli and Klebsiella pneumoniae [9-11].
Factors Contributing to Antibiotic Resistance
Antibiotic resistance is a growing global health crisis driven by multiple factors that accelerate the emergence and spread of resistant bacteria. The primary contributors to antibiotic resistance include misuse and overuse of antibiotics, inadequate infection control, poor sanitation and hygiene, lack of new antibiotic development, global travel and trade, and agricultural antibiotic use. These factors, either individually or in combination, create an environment where bacteria can adapt and survive despite antibiotic treatment. Understanding these contributing factors is essential for implementing effective strategies to combat antibiotic resistance.
1. Misuse and Overuse of Antibiotics
One of the most significant drivers of antibiotic resistance is the overuse and misuse of antibiotics in human medicine. Many patients demand antibiotics for viral infections like the common cold, flu, or sore throat, despite the fact that antibiotics are only effective against bacterial infections. Physicians, under pressure from patients or due to diagnostic uncertainty, sometimes prescribe antibiotics unnecessarily. Additionally, inappropriate dosing and incomplete treatment courses contribute to resistance. When patients fail to complete the full antibiotic regimen, some bacteria survive and develop resistance, making future infections harder to treat. Self-medication, where individuals take leftover or non-prescribed antibiotics, further increases the risk of resistance. The availability of over-the-counter (OTC) antibiotics in some countries without a prescription exacerbates this problem, leading to widespread and uncontrolled antibiotic use [12].
2. Inadequate Infection Control in Healthcare Settings
Hospitals and healthcare facilities are hotspots for the emergence and spread of antibiotic-resistant bacteria. Poor infection control measures, such as inadequate hand hygiene, improper sterilization of medical equipment, and insufficient isolation of infected patients, contribute to the rapid transmission of resistant bacteria. Multidrug-resistant organisms (MDROs) like methicillin-resistant Staphylococcus aureus (MRSA) and carbapenem-resistant Enterobacteriaceae (CRE) frequently spread in hospitals, where antibiotics are heavily used. The overuse of broad-spectrum antibiotics in intensive care units (ICUs) and long-term healthcare facilities further selects for resistant bacterial strains. Without stringent infection control measures, resistant bacteria can spread from patient to patient, increasing the burden of untreatable infections.
3. Poor Sanitation and Hygiene
Poor hygiene and inadequate sanitation facilitate the spread of resistant bacteria in both healthcare and community settings. Contaminated water sources, lack of proper sewage disposal, and inadequate handwashing practices create an environment where resistant bacteria can thrive. In developing countries, limited access to clean water and poor public health infrastructure contribute significantly to antibiotic resistance. Resistant bacteria can spread through food, water, and person-to-person contact, particularly in overcrowded living conditions with poor hygiene. For example, diarrheal diseases caused by resistant Escherichia coli or Salmonella infections are more common in areas with inadequate sanitation. Improving hygiene, promoting handwashing, and ensuring access to clean drinking water are crucial steps in reducing the spread of antibiotic-resistant bacteria [13].
4. Lack of New Antibiotic Development
The decline in new antibiotic development has worsened the antibiotic resistance crisis. Despite the growing threat of resistant infections, pharmaceutical companies have reduced investments in antibiotic research and development (R&D) due to economic and scientific challenges. Developing new antibiotics is costly and time-consuming, with high failure rates in clinical trials. Moreover, antibiotics generate lower profits compared to chronic disease medications, discouraging pharmaceutical companies from pursuing antibiotic research. As a result, the discovery of new antibiotic classes has slowed, while resistance to existing antibiotics continues to rise. Without new antibiotics, infections caused by multidrug-resistant (MDR) and extensively drug-resistant (XDR) bacteria become increasingly difficult to treat. Incentivizing antibiotic development through government funding, public-private partnerships, and global collaboration is critical to addressing this issue [14].
5. Global Travel and Trade
The rapid movement of people, animals, and goods across borders has facilitated the global spread of antibiotic-resistant bacteria. International travel allows individuals to carry resistant bacteria from one country to another, leading to the worldwide dissemination of resistant pathogens. For example, tourists visiting regions with high antibiotic resistance rates (e.g., South Asia, Africa) may acquire resistant bacteria through contaminated food or water and unknowingly bring them home. Medical tourism, where patients travel to other countries for medical treatment, also increases the risk of acquiring resistant hospital-acquired infections (HAIs). Resistant bacteria like New Delhi Metallo-β-lactamase (NDM-1) producing Klebsiella pneumoniae have spread globally due to international travel and hospitalization in countries with poor antibiotic stewardship. Additionally, global food trade contributes to the spread of resistance. Contaminated meat, seafood, and vegetables carrying resistant bacteria can introduce antibiotic resistance genes into new populations. Strengthening international surveillance and cooperation is crucial to monitoring and controlling the spread of antibiotic resistance across borders [15].
6. Agricultural Use of Antibiotics
The extensive use of antibiotics in agriculture and animal farming is a major contributor to antibiotic resistance. In many countries, antibiotics are routinely given to livestock, poultry, and fish not only for treating infections but also for growth promotion and disease prevention. These antibiotics are often the same or closely related to those used in human medicine, leading to cross-resistance between human and animal bacteria. When antibiotics are used in food-producing animals, resistant bacteria can spread to humans through:
For example, antibiotic-resistant Salmonella, Campylobacter, and E. coli have been linked to agricultural antibiotic use. The widespread use of colistin (a last-resort antibiotic for humans) in livestock has led to the emergence of colistin-resistant E. coli, a serious public health threat. Many countries are now implementing regulations to limit or ban the use of antibiotics in agriculture, but enforcement remains a challenge.
7. Inadequate Surveillance and Antibiotic Stewardship
A lack of proper surveillance systems makes it difficult to track antibiotic resistance patterns and implement effective policies. Many low- and middle-income countries lack the infrastructure to monitor antibiotic use, resistance trends, and infection outbreaks, allowing resistance to spread unnoticed. Additionally, poor antibiotic stewardship programs in hospitals and clinics contribute to inappropriate prescribing and overuse. Antibiotic stewardship programs aim to optimize antibiotic use by ensuring that antibiotics are prescribed only when necessary, at the right dose, and for the appropriate duration. However, many healthcare facilities do not have guidelines, trained personnel, or diagnostic tools to support proper antibiotic stewardship. Improving global antibiotic surveillance and implementing stronger antibiotic stewardship policies can help slow the spread of resistance and preserve the effectiveness of existing antibiotics [16-18].
Pharmacological Strategies to Overcome Antibiotic Resistance
Antibiotic resistance is a major global health challenge, making infections harder to treat and increasing morbidity and mortality rates. To combat this crisis, researchers and clinicians have developed several pharmacological strategies to restore antibiotic efficacy and slow resistance development. These approaches include combination therapy, development of novel antibiotics, β-lactamase inhibitors, antimicrobial peptides, anti-virulence therapies, bacteriophage therapy and nanotechnology-based approaches. Each of these strategies aims to either enhance the activity of existing antibiotics, develop new antibacterial agents, or target resistance mechanisms directly.
1. Combination Therapy
Combination therapy involves the use of two or more antibiotics together to enhance bacterial killing, prevent resistance development, and improve treatment outcomes. By using multiple antibiotics with different mechanisms of action, bacteria are less likely to develop resistance because they must acquire mutations in multiple targets simultaneously. A well-known example is the combination of β-lactam antibiotics with β-lactamase inhibitors. Many bacteria produce β-lactamase enzymes that degrade β-lactam antibiotics, making them ineffective. To counteract this, β-lactamase inhibitors such as clavulanic acid, sulbactam, tazobactam, and avibactam are combined with β-lactam antibiotics to prevent enzymatic degradation and restore activity. Examples include amoxicillin + clavulanic acid (Augmentin) and piperacillin + tazobactam (Zosyn). Another effective combination is colistin with rifampin or tigecycline, used to treat carbapenem-resistant Enterobacteriaceae (CRE). By using combination therapy, clinicians can reduce the likelihood of resistance emergence and improve patient outcomes in multidrug-resistant infections.
2. Development of Novel Antibiotics
The discovery of new antibiotics with novel mechanisms of action is crucial for overcoming resistance. Traditional antibiotics mainly target bacterial cell walls, ribosomes, or DNA synthesis, but many bacteria have developed resistance to these drugs. To address this, researchers are developing antibiotics that act on previously unexplored bacterial pathways. For example, gepotidacin is a novel antibiotic that inhibits topoisomerase IV and DNA gyrase, making it effective against fluoroquinolone-resistant Neisseria gonorrhoeae and Escherichia coli. Another innovative antibiotic, cefiderocol, is a siderophore cephalosporin that uses bacterial iron transport systems to penetrate bacterial cells, effectively treating carbapenem-resistant Pseudomonas aeruginosa and Klebsiella pneumoniae. Additionally, LpxC inhibitors target lipopolysaccharide biosynthesis, a new approach to tackling Gram-negative bacterial infections. The development of novel antibiotics is essential, but their success depends on responsible usage and global stewardship programs to prevent rapid resistance emergence [19].
3. β-Lactamase Inhibitors
One of the main resistance mechanisms in bacteria is the production of β-lactamase enzymes, which hydrolyze β-lactam antibiotics and render them ineffective. To counteract this, β-lactamase inhibitors (BLIs) are combined with β-lactam antibiotics to block enzyme activity and restore the antibiotic’s efficacy. The first-generation BLIs include clavulanic acid, sulbactam, and tazobactam, which are effective against penicillin-resistant Gram-positive and Gram-negative bacteria. However, as bacteria evolved more potent β-lactamases, new non-β-lactam-based inhibitors were developed, such as avibactam, vaborbactam, and relebactam, which effectively inhibit carbapenem-resistant β-lactamases. Examples of new β-lactamase inhibitor combinations include ceftazidime + avibactam (Avycaz) and meropenem + vaborbactam (Vabomere). These inhibitors extend the lifespan of β-lactam antibiotics and provide an effective treatment against multidrug-resistant bacteria [20].
4. Antimicrobial Peptides (AMPs)
Antimicrobial peptides (AMPs) are naturally occurring molecules with strong antibacterial properties, making them promising alternatives to conventional antibiotics. AMPs work by disrupting bacterial membranes, inhibiting biofilm formation, and modulating immune responses. Some naturally occurring AMPs include defensins and cathelicidins, which are produced by the human immune system to combat infections. Additionally, synthetic peptides are being developed to overcome bacterial resistance with minimal toxicity. Polymyxins (colistin, polymyxin B) are a well-known class of AMPs that disrupt the outer membrane of Gram-negative bacteria, making them effective against carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter baumannii. Since resistance to AMPs develops more slowly compared to traditional antibiotics, they hold great promise as future antimicrobial agents [21].
5. Anti-Virulence Therapies
Instead of killing bacteria directly, anti-virulence therapies disarm bacteria by neutralizing their virulence factors, making them less capable of causing disease and more susceptible to immune clearance. One approach is quorum sensing inhibitors, which block bacterial communication systems that regulate virulence gene expression. Compounds like furanones and ajoene prevent bacteria from coordinating infection, reducing their ability to cause disease. Another strategy is toxin neutralization, where monoclonal antibodies or small molecules target bacterial toxins. For example, bezlotoxumab is a monoclonal antibody that neutralizes Clostridium difficile toxin B, preventing recurrent infections. Anti-virulence therapies do not exert direct selective pressure, reducing the likelihood of resistance development and offering a new way to manage bacterial infections.
6. Bacteriophage Therapy
Bacteriophages (phages) are viruses that specifically infect and kill bacteria, making them a promising alternative to antibiotics. Phage therapy is highly specific, targeting only the bacterial species causing the infection while sparing beneficial microbiota. This precision reduces the risk of side effects and secondary infections. Additionally, phages can evolve alongside bacteria, making it more difficult for resistance to develop. Phage therapy has been successfully used to treat infections caused by multidrug-resistant Pseudomonas aeruginosa, Klebsiella pneumoniae, and Acinetobacter baumannii. However, challenges such as phage resistance, regulatory hurdles, and standardization of phage therapy must be addressed before widespread clinical use.
7. Nanotechnology-Based Approaches
Nanotechnology offers innovative drug delivery systems to enhance antibiotic effectiveness and overcome bacterial resistance. Nanoparticles (NPs), such as silver nanoparticles (AgNPs) and zinc oxide nanoparticles (ZnO-NPs), have direct antibacterial effects by disrupting bacterial membranes and generating reactive oxygen species (ROS) that damage bacterial DNA. Additionally, antibiotic-loaded nanoparticles can improve drug stability, bioavailability, and targeted delivery. Smart nanocarriers, designed to release antibiotics only at the infection site, can bypass bacterial efflux pumps and biofilms, increasing treatment success. Nanotechnology-based approaches provide precision drug delivery and reduced side effects, making them a promising strategy for overcoming resistance [22,23].
Pharmacologists' Role in Antibiotic Resistance Management
Pharmacologists play a critical role in combating antibiotic resistance by contributing to drug discovery, optimizing antibiotic use, conducting clinical research, promoting antimicrobial stewardship, educating healthcare professionals, and influencing policy decisions. Their expertise in pharmacokinetics, pharmacodynamics, drug interactions, and resistance mechanisms enables them to develop effective strategies to preserve antibiotic efficacy and slow the emergence of resistant bacteria. Through research, education, and policy advocacy, pharmacologists help bridge the gap between scientific innovation and clinical application, ensuring the responsible use of antibiotics worldwide.
1. Development of Novel Antibiotics and Adjuvants
Pharmacologists are at the forefront of antibiotic discovery and development, identifying new drug targets and designing novel compounds to overcome resistance. With many bacteria developing resistance to existing antibiotics, pharmacologists work to develop new antibiotic classes that target previously unexplored bacterial pathways. For example, the discovery of LpxC inhibitors and topoisomerase IV inhibitors offers potential breakthroughs in treating Gram-negative infections. Additionally, pharmacologists are developing β-lactamase inhibitors (e.g., avibactam, vaborbactam) to restore the effectiveness of β-lactam antibiotics against resistant bacteria. Another key area is antibiotic modification, where existing drugs are chemically altered to bypass resistance mechanisms. Pharmacologists also explore combination therapies, such as antibiotic–nanoparticle conjugates and antibiotic–efflux pump inhibitors, to enhance antibiotic activity and prevent bacterial adaptation. These efforts are crucial in ensuring a continuous pipeline of effective antibiotics to combat multidrug-resistant (MDR) bacteria.
2. Optimizing Antibiotic Dosing and Pharmacokinetics/Pharmacodynamics (PK/PD)
Pharmacologists play a crucial role in optimizing antibiotic dosing regimens to maximize bacterial killing while minimizing the risk of resistance. Through pharmacokinetics (PK) and pharmacodynamics (PD) modeling, they determine the optimal drug concentration and exposure time needed to eliminate bacteria without promoting resistance. For example, in time-dependent antibiotics (e.g., β-lactams), pharmacologists recommend extended or continuous infusion strategies to maintain effective drug levels. In contrast, for concentration-dependent antibiotics (e.g., aminoglycosides), they design dosing regimens that achieve high peak concentrations to enhance bacterial killing. Pharmacologists also assess the post-antibiotic effect (PAE), which helps in designing intermittent dosing schedules to reduce unnecessary antibiotic use. Furthermore, they adjust dosing in special populations such as critically ill patients, neonates, and those with kidney or liver impairment to ensure safe and effective antibiotic therapy. These efforts help reduce the selection pressure for resistant strains while maintaining therapeutic efficacy.
3. Conducting Clinical Research and Surveillance
Pharmacologists are actively involved in clinical trials and epidemiological studies to monitor antibiotic resistance trends and assess the effectiveness of new treatments. Their research focuses on conducting phase I–IV clinical trials to evaluate the safety, efficacy, and pharmacokinetics of novel antibiotics, combination therapies, and resistance-modifying agents. They collaborate with microbiologists to study bacterial susceptibility patterns and track the emergence of new resistance genes, which helps in updating treatment guidelines. Additionally, pharmacologists investigate drug-drug interactions and adverse effects to improve patient safety in clinical practice. Preclinical research, including in vitro and in vivo models, allows pharmacologists to test novel therapies before they reach human trials. These studies provide evidence-based recommendations for treatment protocols, antimicrobial stewardship programs, and regulatory approvals, ensuring that only the most effective and safest antibiotics are used in clinical settings.
4. Promoting Antimicrobial Stewardship Programs (ASPs)
Pharmacologists play a key role in antimicrobial stewardship programs (ASPs), which aim to optimize antibiotic use, reduce unnecessary prescriptions, and prevent resistance development. They collaborate with infectious disease specialists, microbiologists, and pharmacists to develop hospital guidelines for appropriate antibiotic selection, dosing, and duration of therapy. Pharmacologists are also involved in reviewing antibiotic prescriptions to identify and prevent inappropriate use, such as prescribing antibiotics for viral infections or using broad-spectrum antibiotics when a narrow-spectrum alternative is sufficient. They also monitor resistance patterns in hospitals and recommend de-escalation strategies to switch from broad-spectrum to targeted therapy whenever possible. By implementing these antimicrobial stewardship strategies, pharmacologists help minimize the overuse of antibiotics, ensuring their long-term efficacy and reducing healthcare-associated resistance.
5. Educating Healthcare Professionals and the Public
Pharmacologists play a vital role in educating medical professionals, students, and the general public about antibiotic resistance and proper antibiotic use. They conduct training programs and workshops for doctors, pharmacists, and nurses to enhance their knowledge of resistance mechanisms and antimicrobial stewardship. Additionally, pharmacologists help design public awareness campaigns that discourage self-medication, improper antibiotic use, and over-the-counter antibiotic sales. By integrating antibiotic resistance education into medical and pharmacy curricula, pharmacologists ensure that future healthcare providers understand the importance of pharmacokinetics, combination therapy, and resistance prevention. Moreover, they promote vaccination programs as a preventive measure to reduce bacterial infections and minimize the need for antibiotic use. By spreading knowledge, pharmacologists empower healthcare providers and the public to make informed decisions about antibiotic use and resistance prevention.
6. Policy Advocacy and Regulatory Contributions
Pharmacologists contribute to healthcare policies and regulatory frameworks to ensure responsible antibiotic use at national and global levels. They work closely with organizations like the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and Food and Drug Administration (FDA) to shape policies that restrict antibiotic misuse and guide research funding for new antibiotics. Pharmacologists also play a role in advising governments on regulations, such as limiting over-the-counter sales of antibiotics and implementing prescription-only policies. In agriculture, they support bans or limitations on the use of medically important antibiotics in livestock and aquaculture, which contributes to resistance in human pathogens. Additionally, pharmacologists advocate for public-private partnerships and financial incentives to encourage pharmaceutical companies to invest in new antibiotic research. Their contributions to policy development and regulation enforcement help shape a more sustainable approach to managing antibiotic resistance.
7. Exploring Alternative Therapies
With the rise of multidrug-resistant (MDR) and extensively drug-resistant (XDR) bacteria, pharmacologists are exploring non-traditional antimicrobial strategies to complement existing treatments. Bacteriophage therapy, which uses viruses to infect and kill bacteria, is gaining attention as a targeted alternative to antibiotics. Pharmacologists also investigate anti-virulence therapies, which disarm bacteria by neutralizing toxins, quorum sensing pathways, and biofilm formation instead of directly killing them. Antimicrobial peptides (AMPs), such as defensins and cathelicidins, offer promising alternatives due to their ability to disrupt bacterial membranes with minimal resistance development. Another innovative approach involves nanotechnology-based drug delivery systems, where nanoparticles enhance antibiotic penetration and bypass bacterial efflux pumps, making resistant bacteria more susceptible to treatment. Probiotics and microbiome-based therapies are also being explored to restore healthy gut bacteria and prevent pathogen colonization. These novel approaches offer new hope in the fight against antibiotic resistance by circumventing traditional resistance mechanisms and developing next-generation antimicrobials [24-29].
CONCLUSION
Antibiotic resistance poses a severe threat to modern medicine, requiring urgent and coordinated efforts across multiple disciplines. Pharmacologists play a crucial role in developing novel antibiotics, optimizing drug regimens, conducting research, implementing antimicrobial stewardship programs, educating healthcare professionals, and advocating for policy changes. Their expertise in pharmacokinetics, pharmacodynamics, and bacterial resistance mechanisms enables them to design effective treatment strategies while minimizing resistance development. The integration of pharmacological strategies with alternative therapies such as bacteriophage therapy, antimicrobial peptides, and nanotechnology-based approaches provides new avenues for managing resistant infections. Additionally, public education and regulatory enforcement are essential to ensure the responsible use of antibiotics in both healthcare and agriculture. A collaborative effort between pharmacologists, microbiologists, clinicians, policymakers, and the public is necessary to combat antibiotic resistance effectively. By combining scientific advancements, clinical expertise, and public health initiatives, we can preserve the efficacy of antibiotics and secure the future of infectious disease treatment. Immediate action is needed to prevent a post-antibiotic era where common infections become untreatable, threatening global health and medical progress.
REFERENCES


Pallavi Aher, Janhavi Gangurde, Gaurav Kasar*, Durgesh Pagar, Dipti Chavan, Dr. Chandrashekhar Patil, Dr. Sunil Mahajan, Combating Antibiotic Resistance: Pharmacological Strategies and Emerging Therapeutic Innovations, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4247-4263. https://doi.org/10.5281/zenodo.15512619
 10.5281/zenodo.15512619
10.5281/zenodo.15512619
