Molecular and Human Genetics Lab, Department of Zoology, University of Lucknow, Lucknow, Uttar Pradesh India
Oral squamous cell carcinoma (OSCC) is one of the most deadly diseases in the head and neck region, accounting for one-third of all head and neck cancer deaths. Mortality and morbidity continue to be high despite advances in therapeutic approaches. Advancement of OSCC is characterized by changes in a number of genes and the expression of their associated proteins. A number of studies have indicated that centrosomal protein 55 (Cep55) has characteristics similar to those of oncogenes, and that Cep55 overexpression is related with the progression of malignant tumours. The purpose of this study was to determine whether Cep55 expression is associated with clinicopathologic characteristics and patient survival in OSCC. A total of 75 OSCC patients and 40 healthy matched controls were recruited for the study. Out of 75 OSCC cases, 62 were in early stage of cancer and 13 were in advanced stage of cancer. The OSCC cases were first categorized histopathologically. Immunohistochemistry and quantitative polymerase chain reaction (qPCR) analysis were used to determine the Cep55 expression profile in tumour samples and compared with that in healthy oral mucosa. The study revealed a clear association of Cep55 expression with clinical stage and grade of OSCC patients and their overall survival. The present findings indicated that Cep55 may have a key role in influencing the biological behaviour and survival of OSCC patients regardless of tumour staging or pathological grading. Thus, assessing Cep55 expression could help surgeons determine an effective treatment.
Oral cancer is a significant public health problem in India, as it is among the most prevalent types of cancer, impacting a considerable proportion of the population [1]. Despite significant advances in early detection and targeted cancer treatment, OSCC remains a difficult disease that has imposed a significant economic and medical burden [2]. Smoking, drinking, genetic abnormalities, and HPV infections are all risk factors for the development of OSCC. Additionally, the majority of OSCC patients cannot be screened early due to the absence of diagnostic indicators. Additionally, some patients with OSCC may experience cancer recurrence as a result of medication resistance [3,4]. Thus, it is critical for OSCC research and management to uncover novel biomarkers and effective targets .
OSCC manifests clinically as non-healing ulcerations as a result of tissue destruction, induration as a consequence of excessive keratin development within the tumor mass, fixation of surrounding tissue due to submucosal invasion, and elevated, everted tumor margins. It is not surprising that oral epithelial cells are susceptible to malignant transformations, given that they serve as the first line of defense against pollutants and carcinogens [5]. There are a variety of reasons that can lead to treatment failure, and our primary focus is on understanding the biological behavior of OSCC at the molecular and cellular levels. Patients with OSCC who are at the same clinical stage and/or pathological grade might sometimes have variable clinical outcomes. Pathological grading of tumors, nodal, and metastasis (TNM) staging are insufficient for properly predicting prognosis and survival in cancer patients. Thus, it is critical for OSCC research and management to uncover novel biomarkers and effective targets [3, 4].
Centrosome proteins have long been thought to act as scaffold proteins, regulating mitotic spindle and microtubule structure, and so are required for the cell cycle process [6]. Centrosome protein 55 (Cep55), also known as FLJ10540 and C10orf3, was first identified as a critical component in abscission, the final stage of cytoplasmic division that regulates the physical dysjunction of two daughter cells [7]. Cep55 is initially situated at the centrosome during interphase, but travels to the central spindle region of the cell during anaphase of mitosis. Later in life, it is drawn to the mid-body for cytokinesis, which is necessary for regular cell division regulation [8]. If Cep55 is recruited, the cell fails to divide into two daughter cells, resulting in cells with deficient mid-body release that are more prone to undergo differentiation. Thus, proper localization of Cep55 to the mid-body is critical for determining the destiny of daughter cells [9-12].
Cep55 was involved in carcinogenesis and regulation of PI3K/AKT signaling pathway. There is significant evidence that Cep55 overexpression is associated with the development and progression of a number of malignant cancers, including breast cancer, gastric cancer, and lung cancer. Studies have also revealed that Cep55 overexpression may advance the proliferation, migration and invasion of tumor cells [13, 14].
There are some evidences of involvement of Cep55 in OSCC but there is no research available yet that predicts the involvement of Cep55 in evaluating the biological behavior of OSCC. So, the purpose of this study was to correlate Cep55 expression levels in OSCC patients with clinical and pathological characteristics in order to predict the survival in patients suffering from various grades of oral cancer in North Indian population.
MATERIALS AND METHODS
This was a case control study in which subjects were divided into two groups: Cases and Controls. The OSCC patients were again grouped into early and advanced stages on the basis of grade or aggressiveness of cancer. The samples were collected from both cases and controls and informed written consent from patients or their attendants according to the inclusion and exclusion criteria as follows:
All the subjects willing to participate in the study were requested to fill a questionnaire designed for the study in order to get the details about their demographic, habitual and family history.
Malignant tissue from oral cancer region and peripheral control tissues were collected for further study. A portion of the tissues was immediately placed in formal saline, while the remainder was placed in RNAlater solution (Thermo Scientific, USA) and maintained at -20°C until further processing.
In order to study Cep55 mRNA expression, 75 (55 males; 20 females) freshly frozen OSCC tissue samples and 12 matched peripheral non-cancerous control tissue samples were collected from histopathologically diagnosed OSCC patients. All the patients were registered in Lucknow Cancer Institute from 2019 to 2022. Formalin fixed paraffin embedded OSCC tissue samples (n=64) and matched peripheral non-cancerous control tissue samples (n=12) were collected for immunohistochemical expression study of Cep55. Oral cancer samples were graded using the 2004 World Health Organization (WHO) oral cancer classification criteria (low-grade and high-grade) [18], whilst pathologic staging was performed using tumor-lymph node-metastasis (TNM) classification system [19]. Demographic and clinical categorization of subjects was done as shown in Table 1.
Tissue samples (40-50 mg) were taken and stabilized by dissolving in 500µl of all protect reagent. At room temperature, RNA was extracted manually from tissues by Trizol method (Thermo Fisher Scientific, USA). RNA samples were kept at a temperature of -80 °C for future use. One microgram of RNA was utilized to synthesize cDNA using Verso cDNA Synthesis Kit in accordance with the manufacturer's instructions (Thermo Fisher Scientific, USA). The prepared cDNA was quantified with a UV-Vis spectrophotometer for future use.
OSCC tissue samples (50-60 mg) were kept in formal saline for histological grading of patients. Sections were fixed in paraffin and sliced with a microtome following which; sections were mounted on slides and stained with hematoxylin and eosin. Following staining, the sections were graded according to their degree of differentiation.
The quantitative expression levels of Cep55 were determined using SYBR® GreenERTM qPCR SuperMix Universal (Invitrogen) on the LightCycler 480 (Roche Applied Science, Mannheim, Germany), with the housekeeping gene GAPDH as an internal control. The reaction master mix was composed of 5µl of 2X SYBR green (Invitrogen), Two µl each of prepared cDNA and RNAse free water was mixed to get a final volume of 10µl mastermix. All the samples were studied in triplicates. The CEP55 primer sequences were as described by Singh et al (2014):
Forward Primer: 5’-TGAAGAGAAAGACGTATTGAAACAA-3’
Reverse Primer: 5’-GCAGTTTGGAGCCACAGTCT-3’
The amplification protocol included an initial denaturation step performed at 950C for 10 min, followed by 40 cycles at 950C for 10sec, then annealing at 600C for 20sec and elongation at 720C for 10sec. After the completion of PCR cycles, melting curves obtained were analysed and the fold change for Cep55 expression levels was calculated [17].
The Cep55 antibody was standardized for immunostaining by diluting it in phosphate buffered saline (PBS) in graded quantities and checked on human testis tissue sample as the positive control, suggested by the manufacturer.
A standard immunohistochemical staining methodology was used. Thick tissue sections (4-5mm) were deparaffinized in xylene and rehydrated in graded levels of alcohol. Sections were treated with 10mM of ethylenediaminetetraacetic acid-8 (EDTA-8), at 90-950C in a pressure cooker for 15 minutes and then allowed to cool to room temperature naturally. This was done for antigen retrieval. The slides were then washed three times with Phosphate Buffered Saline at 5-minutes interval. After this, the sections were blocked for 1 hour at 370C with a blocking solution containing 3% bovine serum albumin, followed by overnight incubation at 40C with a 1:400 anti CEP55 primary mouse monoclonal antibody (Proteintech, USA). The secondary rabbit polyclonal antibody (Sigma Aldrich, India) was conjugated by incubating it at 370C for 1 hour and then washing it three times for ten minutes with PBS. The sections were counterstained with haematoxylin and treated with 3,3'-diaminobenzidine tetrahydrochloride (DAB) chromogen.
Cep55 expression was determined immunohistochemically in stained sections, with cytoplasmic staining considered to be positive for Cep55 expression. The staining intensity was calculated as described by Jiang et al.[15]. Finally, the immunohistochemistry score (IHS) was determined by multiplying the percentage of stained cells and the intensity of their staining. Two researchers assessed the intensity and staining distribution of Cep55 expression in five randomly selected high-power fields for each section to reduce chances of error. The mean scores assigned by the two researchers were used. The resulting value of HIS >4 was considered as positive, while <4 was considered as negative (Fig.6).
SPSS software was used to analyze the data. The Chi-square/Fisher’s exact test was used to examine the correlation between Cep55 expression and clinical and pathological variables. The Kaplan–Meier technique was used to analyze the survival in OSCC patients. The subjects with incomplete data were excluded. P value <0.05 is considered as statistically significant.
RESULTS
All the subjects recruited for the study were classified according to their demographical and cliniopathological features. There was no significant difference in age and sex between both the groups (Table 1, Figure 1). However, a significant difference was observed between smoking status and alcohol use between cases and controls. Statistical analysis clearly supported the fact that tobacco and alcohol are major etiologies for oral cancer.
Table 1: Demographic and clinicopathological grading of cases and controls.
|
Clinicopathological features |
Real time (N=75) |
IHC (N=64) |
Controls (N=12) |
p value |
|
Age |
||||
|
</= 45yrs |
24 |
22 |
7 |
0.1801 |
|
|
|
|
|
|
|
>45yrs |
51 |
32 |
5 |
|
|
Sex |
||||
|
Male |
55 |
48 |
5 |
0.0563 |
|
Female |
20 |
16 |
7 |
|
|
Grade |
||||
|
G1 |
47 |
39 |
0.8434 |
|
|
G2 |
28 |
25 |
||
|
Stage |
||||
|
T1-T2 |
62 |
53 |
0.9819 |
|
|
T3-T4 |
13 |
11 |
||
|
Smoking |
||||
|
Yes |
52 |
42 |
0 |
<0.001 |
|
No |
23 |
22 |
12 |
|
|
Alcohol |
||||
|
Yes |
42 |
34 |
1 |
0.005 |
|
No |
33 |
30 |
12 |
|
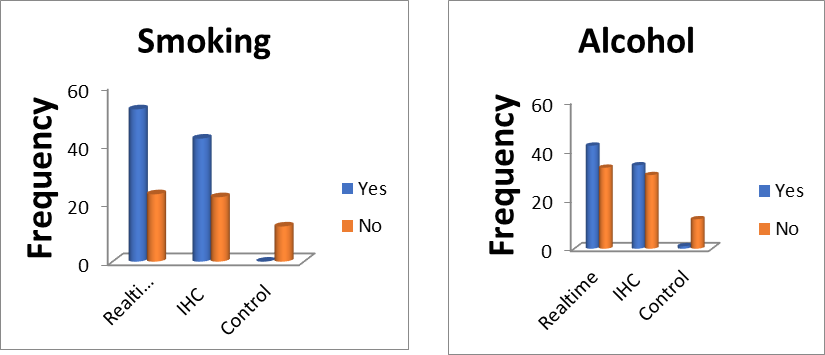
Figure 1: Graph showing association of tobacco smoking and alcohol use with OSCC
The OSCC tissue samples collected from subjects were graded histopathologically according to their differentiation. Differentiation not only defines the aggressiveness of cancer but also gives an idea about the prognosis of the disease. So, patients were graded in three groups: well, differentiated, moderately differentiated and poorly differentiated cancers (Fig.2).
Figure 2: Grading of OSCC on the basis of differentiation. A-Well Differentiated OSCC, B-Moderately Differentiated, C-Poorly Differentiated, D-Verrucous Carcinoma.
The patients detected positive for Cep55 expression were graded according to the stage and grade of OSCC. Cep55 expression was compared between different grades and stages of OSCC patients and controls using qPCR. The qPCR analysis clearly demonstrated that Cep55 expression is more significant in moderately differentiated tumors in advanced stage with respect to controls (Fig.3).

Figure 3: Relative fold change in different grades and stages of OSCC
Immunohistochemical analysis was performed to investigate the correlation between the clinicopathological parameters of OSCC and Cep55 protein expression. At first, 64 OSCC cases were considered; however, six samples were removed from interpretation due to, handling errors, insufficient tissue, staining mistakes, and nonspecific staining. As a result, Cep55 expression was statistically analyzed in 58 patients. Out of 58 patients, 46 were positive for Cep55 expression and 12 were negative (Table 2).
Table 2: Association between OSCC clinical characteristics and Cep55 protein expression.
|
Characteristics |
Negative (12) |
Positive (46) |
Patients (58) |
p value |
|
Male |
9 |
36 |
45 |
1.000 |
|
Female |
3 |
10 |
13 |
|
|
Age |
||||
|
<45 yrs |
8 |
29 |
37 |
1.000 |
|
>/=45 yrs |
4 |
17 |
21 |
|
|
Tumor size |
||||
|
T1-T2 |
10 |
32 |
42 |
0.4791 |
|
T3-T4 |
2 |
14 |
16 |
|
|
Node |
||||
|
N0-N1 |
9 |
30 |
39 |
0.7326 |
|
N2-N3 |
3 |
16 |
19 |
|
|
Stage |
||||
|
1 |
6 |
7 |
13 |
0.0359 |
|
2 |
5 |
31 |
36 |
|
|
3 |
1 |
8 |
9 |
|
|
Grade |
||||
|
Well differentiated |
10 |
20 |
30 |
0.0430 |
|
Moderately differentiated |
2 |
20 |
22 |
|
|
Poorly differentiated |
0 |
6 |
6 |
|
|
Survival |
||||
|
Survived |
11 |
26 |
37 |
0.0401 |
|
Deceased |
1 |
20 |
21 |
|
Immunohistochemistry revealed no significant association between Cep55 protein expression and the tumor size or nodal status of OSCC patients. A clear and significant association of Cep55 protein expression was found with tumor stage and its grade. The present findings revealed that Cep55 positivity increases as the stage of tumor advances. The Cep55 expression also increases as the aggressiveness of tumor increases or tumor becomes poorly differentiated (Figure 4).

Figure 4: Graph showing association of Cep55 protein expression with grade and stage of OSCC.
A novel finding from the present study was that Cep55 protein expression is significantly associated with the survival of OSCC patients (Figure 5) which means that Cep55 may also work as prognostic indicator for OSCC patients.

Figure 5: Association of Cep55 protein expression with survival of OSCC patients.
Correlating OSCC patient survival to Cep55 expression revealed that the expression levels were closely correlated to survival. Out of the total 58 OSCC patients, 46 showed positive Cep55 expression and only 12 were Cep55 negative. Moreover, among 46 patients who were Cep55 positive, 37 patients survived after being followed up for 2-2.5 years and 21 patients died within 3 years of follow-up (Table 3)
Table 3: Showing survival status of Cep55 positive patients
|
Status |
Frequency |
Percent |
|
Alive |
37 |
63.8 |
|
Dead |
21 |
36.2 |
|
Total |
58 |
100 |
Kaplan-Meier analysis and log rank test are used to evaluate the overall survival status of Cep55 positive OSCC patients and difference in survival status among different histological grades of OSCC (Table 4, Figure 7). The Kaplan-Meier curves revealed that the overall 2 years survival among Cep55 positive OSCC patients was 61.5%. When observed between different histological grades of OSCC, well differentiated tumors have higher than 2 years survival rate (82.8%) as compared to moderately differentiated (40.2%) and poorly differentiated (20.0%) tumors. The difference in survival status among different histological grades was statistically significant (Figure 8).
Table 4: Showing Overall survival status among different histological grades of OSCC.
|
Kaplan Meier & Log Rank Test |
1 year |
2 years |
p value |
|
OVERALL SURVIVAL |
85.8% |
61.5% |
|
|
Well differentiated |
96.6% |
82.8% |
0.001 |
|
Moderate differentiated |
77.3% |
40.2% |
|
|
Poorly differentiated |
60.0% |
20.0% |
Figure 6: Immunohistochemistry showing (1,2) Well differentiated OSCC, (3,4) Moderately differentiated OSCC, (5,6) Poorly differentiated OSCC, (7,8) Control.
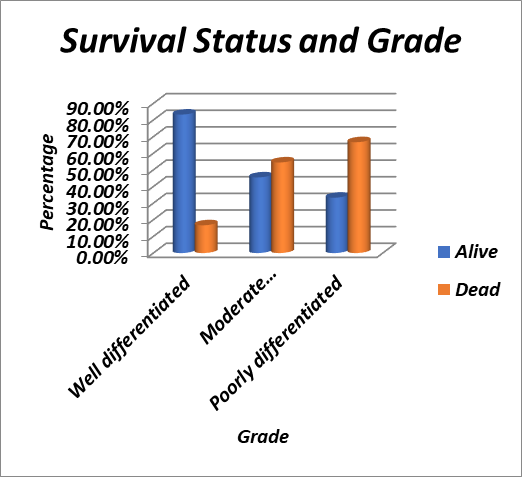
Figure 7: Survival status in different grades of OSCC.
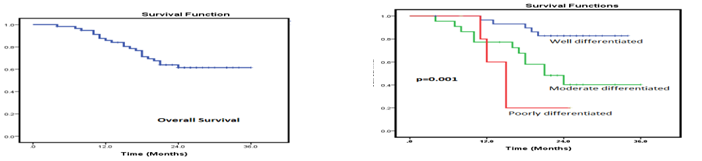
Figure 8: Kaplan-Meier curve showing the overall survival and status among different grades of OSCC.
DISCUSSION
Oral squamous cell carcinoma (OSCC) is the most frequent type of head and neck cancer. It is one of the most expensive cancers in modern medicine due to the demand for follow-up and repeated therapy as relapse is very common in OSCC [20,21]. Despite advancements in treatment, the prognosis for OSCC remains poor, particularly for poorly differentiated tumors. Even with chemotherapy, the overall median survival for individuals with advanced OSCC is one year [22]. The survival among these OSCC patients is frequently achieved at the expense of severe and potentially fatal adverse effects. As a result, improved diagnostic biomarkers and novel therapy approaches are required immediately for OSCC [23,24].
Cep55 is a centrosomal protein that regulates the cell cycle during mitosis by primarily functioning on the PI3K/Akt signalling pathway [7]. Cep55 acts through the PI3K/Akt pathway in conjugation with VEGF, p16, p53, p85, and p110 by enhancing the stability of PI3K/Akt complex subunit, leading to increased Akt activity for cell survival, proliferation, and angiogenesis [7,25]. Any erroneous mutation in this gene (resulting in overexpression) causes dysregulation of the PI3K/Akt pathway, as a result, Cep55 has been classified as an oncogene.
The function of Cep55 as a tumor promoter has been explored in a variety of human cancers, including colon, lung, breast, and ovarian cancers [15, 26, 27, 16]. Cep55 expression levels have been linked to a variety of factors, including clinical stage, prognosis, and metastasis. There is, however, a scarcity of analogous studies examining its participation in the biological behavior of OSCC. Our goal was to evaluate Cep55 expression levels with various clinical and histological characteristics in OSCC and assessing its role in survival analysis of OSCC patients, so that we get an idea about the prognosis and survival of patients suffering from OSCC.
According to literature, increased Cep55 expression may occur from the biological transition of a normal cell to a tumor cell via activation of the PI3K/Akt pathway, resulting in tumor cell proliferation [28]. Our study findings inferred that Cep55 expression is directly proportional to the stage and grade of tumor which means that as the tumor advances and becomes more aggressive in nature, expression of Cep55 also increases. These findings suggested the involvement of Cep55 in tumor advancement which are in agreement with the study done by Chen et al [28] and Surendra et al [29] on OSCC and Jiang et al [15] on adenocarcinoma.
The present study revealed no link between high Cep55 expression and progressive nodal involvement in OSCC patients. These findings were consistent with the findings of Tao et al., [30] who investigated the nodal status (N0, N1, and N2) in patients of gastric cancer [30]. However, study done on oesophageal cancer by Jiang et al [31] and nasopharyngeal carcinoma by Chen et al [28] found that high Cep55 expression was related with a poor prognosis in locally advanced OSCC patients.
The present study also revealed a clear association of Cep55 expression with the stage of tumor which means that as the disease advances the Cep55 expression increases. These findings were in accordance with the study done by Hwang et al [32] on nasopharyngeal carcinoma where Cep55 is found to be clearly associated with tumor stage.
A direct association of Cep55 was found with the grade of OSCC which means that as the differentiation becomes poor, the expression of Cep55 increases. Thus, Cep55 is a predictable point in defining the aggressiveness of tumor. These finding are consistent with those obtained by Jiang et al [31] on oesophageal cancer and Tao et al [30 ] on gastric carcinoma. However, contrasting results were published by Chen et al [28].
qRT-PCR was performed to find the CEP55 mRNA expression in 75 patients of OSCC in the present investigation. The results were similar to those obtained from immunohistochemical analysis, that the expression is significantly more in moderately differentiated tumors in advanced stages. These results were consistent as determined by qRT-PCR analysis in a range of cell lines and tumors, including breast, colorectal, pancreas, esophageal, gallbladder, and lung carcinomas (33, 34, 35, 36). Thus, the study findings suggested that Cep55 mRNA expression may be playing a role in tumorigenesis.
The findings additionally show that CEP55 is not only expressed at the mRNA level but is also translated, as evidenced by IHC analysis of CEP55 in OSCC tissue specimens. To the best of our knowledge, the CEP55 mRNA and protein expression were examined in OSCC for the first time. Our findings are consistent with prior research that found increased protein expression of CEP55 in various tumor tissues [28,29,32-37]
The overall survival of OSCC patients with positive Cep55 expression was also analyzed and it was found that Cep55 expression is a predictive marker to assess the survival among OSCC patients. The log rank test showed that tumor aggressiveness or grade of cancer is dependent on Cep55 expression.
Therefore, our findings implicated that Cep55 could be a biomarker for cancer cell invasion and modify biological behaviour in OSCC patients, resulting in a shorter survival rate. As a result, Cep55 expression could be employed as an early prognostic biomarker to help decide on a treatment plan to improve the quality of life in OSCC patients.
However, the current study has a few limitations. The tumor samples for mRNA and protein expression analysis were obtained from different patients. As a result, there was no correlation between mRNA expression and protein expression. Furthermore, a smaller number of patients refused to participate in the study.
FUTURE PERSPECTIVES:
Examining multicentric and longitudinal studies will be critical to understanding the epidemiological significance of Cep55 across diverse populations and over time, particularly its role in disease progression and prognosis. Such studies will be instrumental in identifying population-specific risk factors and potential biomarkers for early detection and prognosis. In parallel, exploring the functional mechanisms of Cep55 using precise gene-editing technologies like CRISPR/Cas9 or base editing can reveal the causal roles of specific mutations or regulatory elements in processes such as cytokinesis, centrosome integrity, and DNA damage response. Additionally, assessing therapeutic strategies targeting Cep55 should be a central focus, including the development and optimization of small-molecule inhibitors, antisense oligonucleotides, or RNA interference approaches designed to suppress its expression or disrupt its function. Preclinical models and patient-derived organoids can be leveraged to evaluate the efficacy, specificity, and safety of these interventions. Overall, integrating clinical data with molecular and therapeutic research will be critical for translating Cep55 biology into actionable strategies for diagnosis, prognosis, and personalized treatment.
ACKNOWLEDGEMENT:
The authors would like to thank Indian Council of Medical Research (ICMR), University Grant Commission (UGC), New Delhi, India and Centre of Excellence, Higher Education, Government of Uttar Pradesh, Lucknow, India for financial support. DST-FIST-PURSE is duly acknowledged for Central Instrumentation Facility. DT acknowledges UGC for postdoctoral fellowship.
DECLARATION:
Ethical Statement: This study had been reviewed and approved by the ethics committee of KGMU, Lucknow (1252/R-cell-19). The information gathered from the patients or their attendants were obtained only after getting written consent from them.
Competing Interests: There is no competing interest.
Funding: The funding for the above work was provided by UGC, New Delhi (Grant No. F.4-2(BSR)/ME/18-19/0006
REFERENCES


Divya Tandon, Monisha Banerjee, Centrosomal Protein 55 (Cep55)-A New Prognostic Paradigm for Oral Squamous Cell Carcinoma, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 936-949. https://doi.org/10.5281/zenodo.16789450
 10.5281/zenodo.16789450
10.5281/zenodo.16789450
