King George’s Medical University, Lucknow, U.P., India
Knee osteoarthritis (KOA), a prevalent degenerative joint disease, significantly impacts global health, particularly among the elderly and individuals engaged in physically demanding jobs. Conventional treatments ranging from lifestyle modifications to NSAIDs and surgical interventions often provide limited long-term relief and may carry substantial risks, especially cardiovascular and gastrointestinal side effects. Polmacoxib, a novel NSAID and selective COX-2 inhibitor, offers a promising alternative due to its dual mechanism of action. It inhibits both COX-2 and carbonic anhydrase (CA), enabling tissue-specific action primarily in inflamed, CA-deficient joints. This dual inhibition not only helps reduce inflammation and pain but may also mitigate systemic side effects which are associated with traditional NSAIDs and COX-2 inhibitors. Pharmacokinetically, polmacoxib demonstrates a prolonged half-life and high erythrocyte binding, allowing sustained drug delivery to target tissues while minimizing plasma exposure. Clinical trials have shown that a once-daily dose of 2 mg polmacoxib is effective in reducing KOA symptoms, with efficacy comparable to celecoxib and a favourable safety profile. Studies also highlight its minimal cardiovascular and gastrointestinal risks, enhanced tolerability, and reduced need for additional protective medications. Approved in South Korea and India, polmacoxib has yet to receive FDA approval in the U.S. Nevertheless, it stands out as a potent, low-dose, and patient-compliant option for long-term KOA management. Further large-scale trials are essential to validate its long-term safety and potential disease-modifying effects, especially within diverse populations such as those in India.
Osteoarthritis (OA) is a prevalent joint disorder. Impacts millions of people across the globe. It is the most frequently diagnosed type of arthritis. OA ranks among the leading causes of disability in developed countries. As per the World Health Organization (WHO), OA affects over 300 million individuals worldwide. Its occurrence increases with age, with the highest prevalence seen in individuals over 60 years old.1 Pathologically Osteoarthritis is defined as a progressive, degenerative disease characterized by focal deterioration of synovial and articular cartilage, osteophyte formation, cyst sclerosis, alterations in all involved joint structures.2 The burden of osteoarthritis i.e. Global Burden of Disease (GBD) is on the rise, currently impacting 7.6% of the global population, with predictions suggesting the prevalence will increased by 132.2% over 30 years and is projected to rise by 60 to 100% by 2050 of disability.3 It reduces the productivity and creating a heavy financial burden on families and society.4 Most commonly affected joints by OA are the knee and hip joints. Knee osteoarthritis, accounts for more than half of all OA cases globally.5
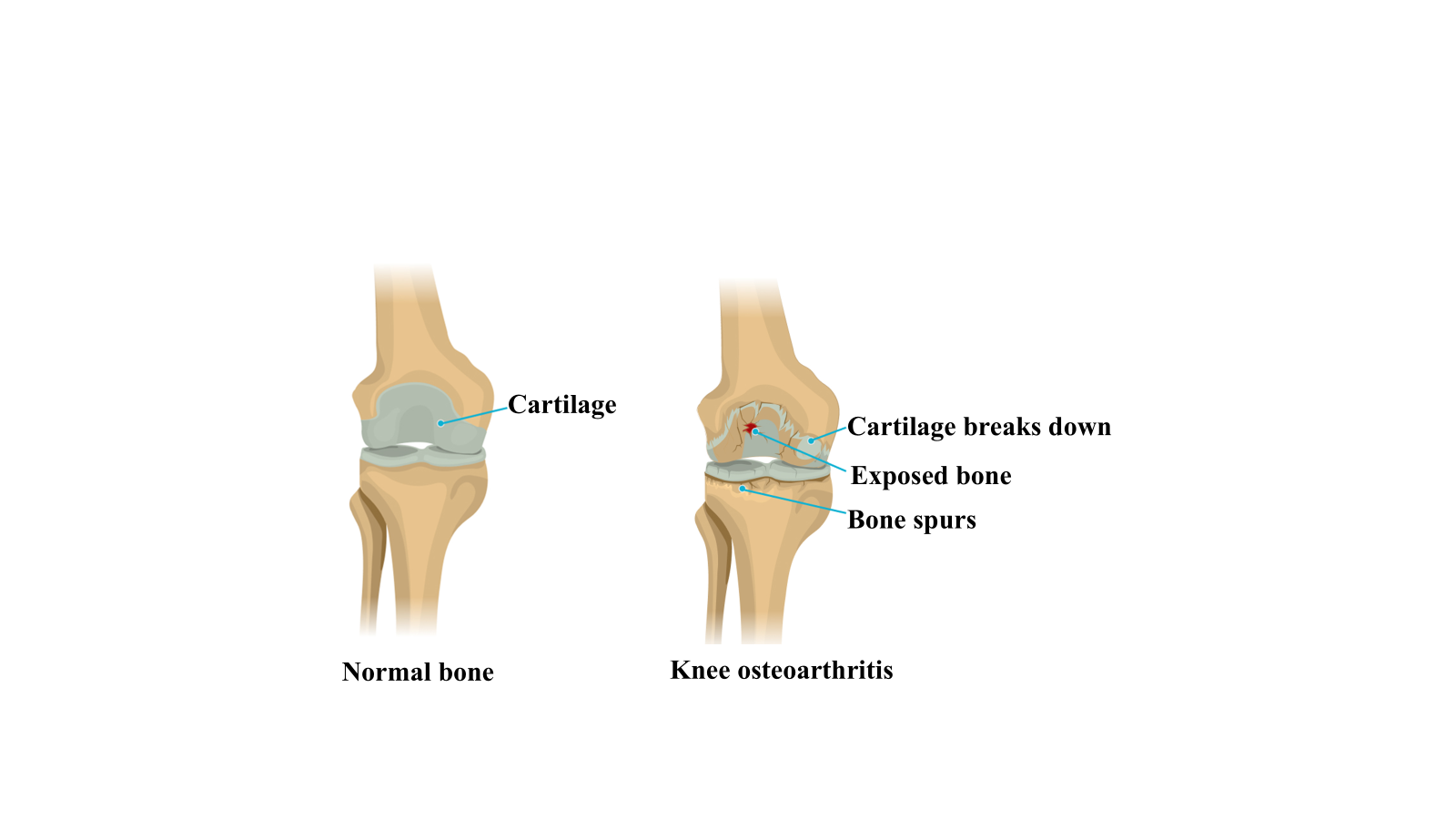
Figure 1: Structure of normal knee joint (L) vs osteoarthritis knee joint (R)6
The pathogenesis of knee osteoarthritis (KOA) can be broadly categorized into mechanical and biological factors. Mechanical factors involve alterations in biomechanics, specifically the disruption of the lower limb strength at the knee joint. Biological factors include an imbalance between chondrocyte proliferation and apoptosis, resulting from various abnormal biological changes in chondrocytes.7 It is influenced by multiple inflammatory cytokines. Chondrocyte damage, extracellular matrix degradation, and excessive bone formation play key roles in disease progression. Drug therapy can help prevent or minimize joint damage while preserving normal joint function.8
Figure 2: Imbalance between basic mechanism of bone formation at cellular level
Risk factors include age, sex, obesity, genetic predisposition and neurological conditions.9 OA is particularly prevalent among individuals engaged in physically demanding occupations such as farmers, traders, firefighters, construction workers, household assistants and tradespeople due to the repetitive joint strain associated with their work.10 Osteoarthritis management involves a range of treatment options, as no disease-modifying medication is currently available. Non-pharmacological approaches include weight management, exercise and the use of walking aids such as canes.11 Pharmacological interventions encompass NSAIDs, intra-articular (IA) injections of corticosteroids, hyaluronic acid, geniculate nerve blocks, extra-articular injections and radiofrequency treatments.12 In cases where conservative treatments fail, surgical treatment may be the last option. Pharmacological management typically begins with nonsteroidal anti-inflammatory drugs (NSAIDs) and may escalate to opioid-based analgesics. However, long-term use of these medications is often limited due to contraindications and potential risks. NSAIDs, in particular, are not suitable for individuals with cardiovascular or gastrointestinal conditions, while opioids carry the risk of dependence and may provide only temporary pain relief.13 NSAIDs are commonly used to alleviate pain through inhibition of cyclooxygenase enzymes (COX-1 and COX-2) associated with various conditions, including osteoarthritis. However, it accounts for 30% of hospitalizations due to adverse drug reactions. Prolonged NSAIDs use in managing knee osteoarthritis may contribute to worsens the symptoms and an increased chances to total knee replacement (TKR), though it does not appear to cause structural changes in the knee joint.14
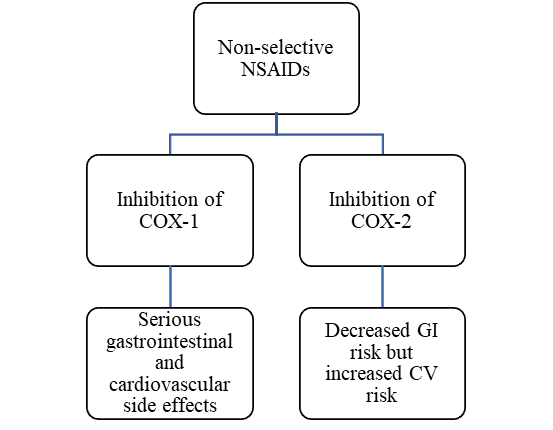
Flowchart 1: Shortcomings in non-selective NSAIDs.15
COX-2 inhibitors associated with risk of cardiovascular and thrombotic events, such as myocardial infarctions and ischemic cerebrovascular incidents. Effects are primarily attributed due to reduced production of prostaglandin I2 (PGI2 or prostacyclin), a compound with cardioprotective properties.16 COX-2 inhibitors drugs withdrawn from the market were valdecoxib and rofecoxib were due to concerns over increased cardiotoxicity and severe skin reactions. The selective cyclooxygenase 2 inhibitor was developed named Polmacoxib with brand name Acelex®, having relatively low risk of cardiovascular toxicity as well as gastrointestinal toxicity compared to Celecoxib. Polmacoxib also known as CG100649. It was established by Crystal genomic Inc. (KOSDAQ: 083790)17 in Korea and approval of the Korean Ministry of Food and Drug Safety (MFDS) was granted in February 2015. Polmacoxib with isoform CYP3A affects the metabolism of cytochrome P450.18 Chemical structure is a 4-{3-(3-fluorophenyl)-5,5-dimethyl-4-oxo-4,5-dihydrofuran-2-yl}-benzenesulfonamide with molecular formula: C18H16FNO4S and molecular Weight: 361.4 g/mol.19
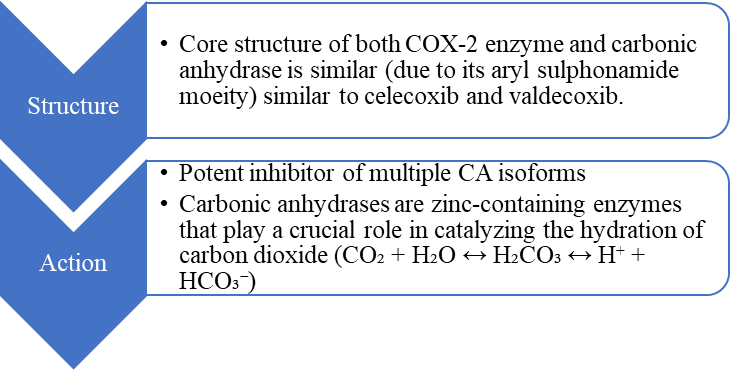
Figure 3: Properties of Polmacoxib
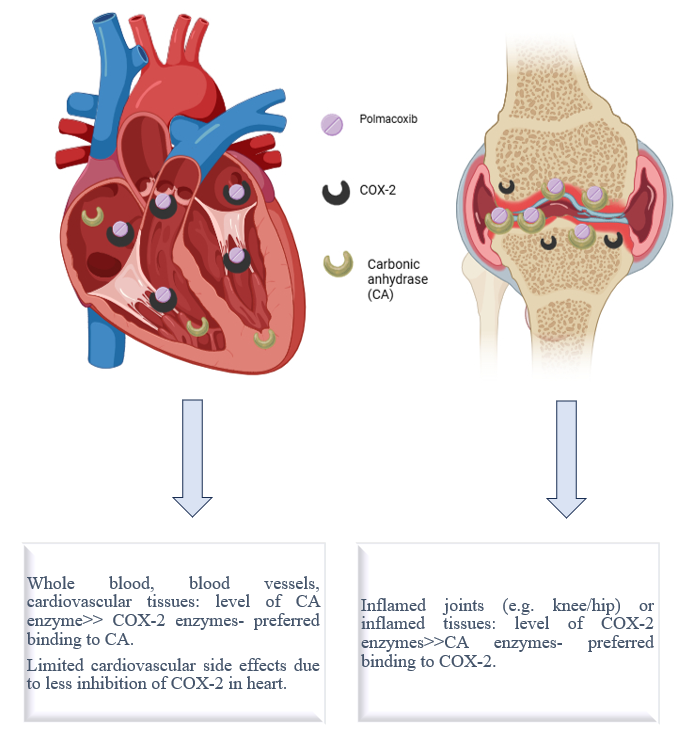
Figure 4: Mechanism of action of tissue specific novel, dual inhibitor of COX-2 and carbonic anhydrase - Polmacoxib 20,21
Table 1: Isoforms of identified carbonic anhydrase enzymes.22
|
Category of carbonic anhydrase enzymes |
Isoforms of carbonic anhydrase enzymes |
|
cytosolic isozymes |
(CA I, CA II, CA III, CA VII, CA XIII), |
|
membrane-bound isoenzymes |
(CA IV, CA IX, CA XII, CA IV, CA XV) |
|
mitochondrial |
(CA VA and CA VB) |
|
secreted isoforms |
(CA VI, primarily in saliva). |
|
CA-related proteins (CARPs) (not catalytically active) |
CA VIII, CA X, CA XI |
CDSCO Approval: Polmacoxib 2mg indicated for treatment of Idiopathic (primary) osteoarthritis of Hip/Knee approved by CDSCO dated 01.05.2023 23 Since cardiovascular (CV) side effects of traditional NSAIDs and COX-2 inhibitors are linked to COX-2 inhibition in the CV system where CA is abundant, this interaction is particularly significant.24 Functionally, CA inhibition is believed to counteract the hypertensive effects that typically follow COX-2 inhibition.25 Polmacoxib was first approved in South Korea in 2015 for the management of colorectal cancer and osteoarthritis. Low-dose polmacoxib administration has shown minimal impact on overall CA function within the circulatory system. In contrast, inflamed tissues tend to be CA-deficient while exhibiting increased COX-2 expression due to inflammatory processes. Since synovial fluid contains negligible CA, polmacoxib effectively inhibits COX-2 in inflamed joint tissues, leading to reduced inflammation and pain relief. Erythrocytes play a crucial role in the pharmacokinetics of polmacoxib by serving as a reservoir, safely transporting the drug in an inactive form to tissues with low CA activity, such as arthritic joints. Polmacoxib achieves 85- to 100-fold higher concentrations in whole blood (i.e., within erythrocytes) compared to plasma, which lacks CA. This mechanism ensures tissue-specific drug delivery, providing sustained therapeutic levels in CA-deficient inflamed tissues. As a result, systemic exposure remains low, as polmacoxib is carried in a bound state with CA inside erythrocytes. This selective transport mechanism enhances its effectiveness in osteoarthritic joints while minimizing adverse effects on the cardiovascular, renal, and gastrointestinal systems.26
Table 2: Pharmacokinetic data of Polmacoxib 26
|
Pharmacokinetic data 26 |
Dose 2mg |
Dose 8mg |
|
Maximum plasma concentration (Cmax) values |
3.5 ng/mL |
14.1 ng/mL |
|
Time to maximum plasma concentration (Tmax) values |
5.6 hours |
5.0 hours |
|
Area under the plasma concentration-time curve (AUC) |
632.9 (162.1) ng/mL × h |
2,366.8 (761.9) ng/mL × h |
|
The mean elimination half-lives |
131 hours |
127 hours |
|
Constant: central elimination rate and redistribution rate. Excretion via faecal route, with a minor portion via urine. Reduction in hepatic metabolism, impacts the clearance. |
||
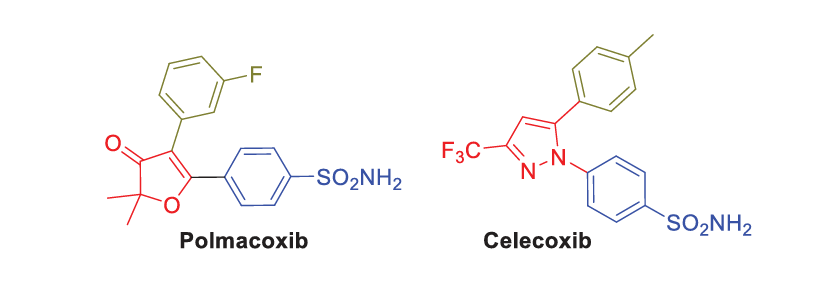
Figure 5: Structure of polmacoxib and celecoxib27
Table 3: Comparative evaluation of COX-2 inhibitors28
|
Characteristics |
Traditional NSAIDs: Diclofenac |
COX-2 inhibitor: Etoricoxib |
COX-2 inhibitor: Celecoxib |
Tissue selective COX-2 inhibitor: Polmacoxib |
|
Cox-2 selectivity |
Low |
High |
High |
High |
|
Half life |
Short |
Long |
Short |
Longest |
|
Daily dosing |
2-4 times/day |
Once a day |
Once or twice/day |
Once a day |
|
Potency |
Low (dose 75mg- 2400mg/day) |
High (30 mg) |
Low (200-400mg/day) |
High potency (2mg/day) |
|
Gastrointestinal side effect risk |
Very high |
Low |
Low |
Low |
|
Cardiovascular side effect risk |
Moderate to high |
High |
Moderate |
Low |
Table 4: Summary of polmacoxib studies
|
Clinical trial |
Study |
Result |
Adverse effect |
|
Safety/Tolerability Profiles of CG100649, a Novel COX-2 Inhibitor.29
Clinical Trial NCT01154790 |
Phase I, Randomized, double-blind, placebo- controlled, multiple ascending oral dose study in healthy korean men and women. |
It suppressed TXB2 and PGE2 at all doses, and only the highest dose suppressed the urinary excretion of the urinary prostacyclin metabolite.29 |
Adverse events reported were aphthous stomatitis and dyspepsia.
|
|
Study of CG100649 Versus Celecoxib in Osteoarthritis Patients 30,31
Clinical Trial NCT01341405
|
Double-blind, randomized, multicentre, phase 2, non-inferiority study of CG100649 versus Celecoxib in Osteoarthritis patients |
Polmacoxib doses of 2 mg and 4 mg exhibited non-inferiority to celecoxib 200 mg. Polmacoxib 2 mg dose selected for Phase 3 clinical studies. 30,31 |
No withdrawals were reported due to ineffectiveness. Adverse effect profile is favourable similar to celecoxib |
|
To evaluate the safety and analgesic efficacy of polmacoxib 2 mg versus placebo in a superiority comparison or versus celecoxib 200 mg in a noninferiority comparison in patients with osteoarthritis (OA)32 Clinical Trial NCT01765296 |
6-week, randomized, multicentre, double-blind and parallel-group trial followed by an 18-week, single arm, open-label extension, Phase III Trial.
|
Efficacy (6-week study): superiority of polmacoxib 2 mg once-daily vs. placebo. Non-inferiority of polmacoxib 2 mg once-daily vs. celecoxib 200 mg once-daily. Long Term Safety (6-month study): No drug-related major adverse events in either the celecoxib or polmacoxib groups. 32 |
Adverse events observed were mild to moderate |
|
Comparative Impact on Prostanoid Biosynthesis of Celecoxib and the Novel Nonsteroidal Anti-Inflammatory Drug CG10064933
Clinical Trial NCT00780325 |
Controlled, double-blind, randomized trial, parallel design study, single oral doses of 2 or 8 mg CG100649, 200 mg celecoxib or placebo
|
The single oral doses of CG100649 (2 mg/8 mg) and celecoxib (200 mg) were well tolerated. CG100649 and celecoxib had the effect of depressing urinary excretion of 2,3-dinor-6-keto PGF1α (PGI-M); CG100649 is relatively selective for inhibition of COX2, exerting a more sustained inhibitory effect on PGI2 biosynthesis as compared with celecoxib. 33 |
Left ventricular hypertrophy was reported in two subjects receiving CG100649 (8 mg), in one as a pre-existing condition and in the other at study exit |
|
To evaluate the influence of ketoconazole, a known strong inhibitor of CYP3A, on pharmacokinetic properties of CG100649 34 Clinical Trial NCT01154764 |
A Randomized, open-label crossover study in healthy Korean male volunteers |
Area under curve (AUC) of CG100649 increased by 29% with the concurrent medication of ketoconazole, it is considered that concurrent administration of CG100649 with ketoconazole would not change the safety profile of CG100649. 34 |
No serious Adverse Events were reported during CG100649 6 mg and ketoconazole 400 mg administration.
|
Future direction:
Polmacoxib is recognized as the most potent COX-2 inhibitor currently available and effectively targeting the key enzymes involved in OA progression. Additionally, polmacoxib exhibits potential disease-modifying properties through its dual inhibition of carbonic anhydrase (CA) and prostaglandin E2 (PGE2), which may contribute to altering the disease course. Therefore, the distinctive mechanism of action of polmacoxib is believed to offer advantages in terms of both effectiveness and reduced systemic side effects compared to traditional NSAIDs. Polmacoxib was first approved in South Korea then in India, however due to some insufficient data it doesn’t get the approved in USA. India having large population, more post-marketing surveillance can be done and better outcomes can be obtained from polmacoxib.
CONCLUSION:
Polmacoxib, as a selective COX-2 inhibitor, has demonstrated considerable potential in alleviating pain and inflammation, supported by its favourable pharmacodynamic and pharmacokinetic characteristics. Its unique dual-action mechanism, targeting both COX-2 and CA contributes to its effectiveness while potentially mitigating common systemic side effects. As such, polmacoxib holds promise as a reliable and well-tolerated long-term therapy for OA. Effective symptom control can be achieved with a low daily dose of just 2 mg, making it the lowest effective dose among known NSAIDs, and its once-daily dosing enhances patient compliance. Its favourable gastrointestinal safety profile reduces the need for additional GI protective medications, while its novel mechanism of action may offer improved cardiovascular safety compared to conventional NSAIDs. Therefore, polmacoxib emerges as a compelling treatment option for managing various pain and inflammation-related conditions.
Nevertheless, long-term safety data on polmacoxib are currently lacking, and its cardiovascular safety profile requires further investigation. Therefore, large-scale randomized controlled trials are essential to establish its long-term efficacy and safety profile.
Conflict of interest: No conflict of interest
REFERENCES





Rashmi Chandra*, Ravi Kumar, Shoebul Haque, D. K. Katiyar, Arpit Singh, COX-2 Selectivity and Beyond: Exploring Polmacoxib Role in Knee Osteoarthritis Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2157-2165. https://doi.org/10.5281/zenodo.15235364
 10.5281/zenodo.15235364
10.5281/zenodo.15235364
