Department of Pharmacology, St. Soldier Institute of Pharmacy, Lidhran Campus, Behind NIT(R.E.C.), Jalandhar-Amritsar bypass NH-1 jalandhar-144011, Punjab, India.
Schizophrenia is a complex and chronic psychiatric disorder that continues to pose significant challenges in both clinical management and scientific understanding. Over the past decade, advances in research have shifted the conceptualization of schizophrenia from a purely dopamine-driven condition to a multifactorial disorder involving intricate interactions among neurotransmitter systems, neurodevelopmental processes, immune mechanisms, and genetic susceptibility. This review synthesizes recent evidence (2015–2026) on the epidemiology, pathophysiology, diagnostic approaches, and treatment strategies of schizophrenia. Particular emphasis is placed on emerging insights into glutamatergic dysfunction, neuroinflammation, oxidative stress, and blood–brain barrier abnormalities, as well as the growing role of artificial intelligence and biomarker discovery in improving diagnostic precision. While conventional antipsychotics remain the cornerstone of treatment, their limitations—especially in addressing negative and cognitive symptoms—have driven the development of novel therapeutic approaches, including muscarinic receptor agonists, glutamatergic modulators, and anti-inflammatory interventions. Despite these advances, substantial gaps remain in translating biological findings into clinical practice. Future progress will depend on integrating multimodal data, advancing precision psychiatry, and developing personalized treatment strategies that address the full spectrum of the disorder.
Schizophrenia is a chronic and severe psychiatric disorder that affects approximately 1% of the global population and continues to rank among the top causes of long-term disability worldwide. The disorder imposes a substantial burden not only on affected individuals but also on families, healthcare systems, and society at large, due to its early onset, chronic course, and significant functional impairment (McCutcheon et al., 2020; Vos et al., 2020). Clinically, schizophrenia is characterized by a heterogeneous constellation of symptoms, broadly categorized into positive symptoms (such as hallucinations and delusions), negative symptoms (including social withdrawal and diminished emotional expression), and cognitive deficits, which are now recognized as core features impacting long-term outcomes (Millan et al., 2016; Green et al., 2019).
Despite more than a century of investigation, the precise etiology and pathogenesis of schizophrenia remain incompletely understood. Historically, the dopamine hypothesis has dominated the field, proposing that dysregulated dopaminergic transmission—particularly hyperactivity in mesolimbic pathways—underlies the emergence of psychotic symptoms (Howes & Kapur, 2009; McCutcheon et al., 2020). While this framework has been instrumental in guiding antipsychotic drug development, it does not adequately explain the full spectrum of clinical manifestations, especially negative symptoms and cognitive impairments, nor does it account for treatment resistance observed in a significant subset of patients.
Over the past decade, there has been a paradigm shift toward more integrative and multidimensional models of schizophrenia. Among these, the glutamatergic hypothesis has gained considerable traction, supported by evidence implicating N-methyl-D-aspartate (NMDA) receptor hypofunction in cortical and subcortical circuits (Coyle et al., 2012; Uno & Coyle, 2019). This dysfunction is thought to disrupt excitatory–inhibitory balance, contributing to both cognitive deficits and psychotic symptoms. In parallel, increasing attention has been directed toward the role of neuroinflammation and immune dysregulation. Elevated levels of pro-inflammatory cytokines, microglial activation, and associations with prenatal infections suggest that immune processes may play a contributory role in disease onset and progression (Khandaker et al., 2015; Miller & Goldsmith, 2017; Gangadin & Enthoven, 2024).
Genetic and epigenetic factors further underscore the complexity of schizophrenia. Large-scale genome-wide association studies (GWAS) have identified numerous risk loci, implicating genes involved in synaptic function, neurotransmission, and immune pathways (Schizophrenia Working Group of the Psychiatric Genomics Consortium, 2014; Ripke et al., 2020). However, genetic predisposition alone is insufficient to explain disease occurrence, highlighting the importance of gene–environment interactions. Environmental risk factors such as prenatal stress, urbanicity, cannabis use, and early-life adversity have been consistently associated with increased risk, likely through epigenetic modifications that alter gene expression without changing DNA sequences (Radua et al., 2018; Ursini et al., 2018).
More recently, emerging research has expanded the scope of investigation to include oxidative stress, mitochondrial dysfunction, and blood–brain barrier (BBB) abnormalities. These mechanisms are thought to interact with neurotransmitter systems and immune pathways, further contributing to neural circuit dysfunction (Flatow et al., 2013; Oatu et al., 2026; Zhang et al., 2025). Collectively, these findings support a shift away from reductionist models toward viewing schizophrenia as a systems-level disorder, arising from dynamic interactions among neurobiological, environmental, and developmental factors.
In line with this perspective, contemporary research increasingly emphasizes the importance of early detection, biomarker discovery, and precision psychiatry approaches. Advances in neuroimaging, machine learning, and molecular profiling are beginning to offer new insights into disease heterogeneity and may ultimately facilitate more personalized treatment strategies (Insel, 2017; Koutsouleris et al., 2018; Anwar et al., 2025). Nevertheless, translating these advances into routine clinical practice remains a significant challenge.
Taken together, schizophrenia is now understood not as a single-pathway disorder but as a complex, multifactorial condition involving interconnected biological systems. This evolving conceptualization provides a more comprehensive framework for understanding its pathophysiology and highlights the need for innovative, multi-target therapeutic approaches.
2. EPIDEMIOLOGY AND CLINICAL FEATURES
2.1 Epidemiology
Schizophrenia is a relatively low-prevalence but highly disabling psychiatric disorder, affecting approximately 0.7–1.0% of the global population. Despite its modest prevalence, the disorder contributes disproportionately to global disability, ranking among the top causes of years lived with disability (YLDs) worldwide (Vos et al., 2020; Charlson et al., 2018). The burden of schizophrenia is further amplified by its early onset, chronic course, and associated social and occupational dysfunction.
Global Distribution and Incidence
Epidemiological studies indicate that the incidence of schizophrenia varies across regions, typically ranging from 10 to 20 cases per 100,000 person-years, although higher rates have been reported in urban and socioeconomically disadvantaged settings (McGrath et al., 2008; Jongsma et al., 2019). This geographic variability is thought to reflect differences in environmental exposures, healthcare access, and diagnostic practices.
Urbanicity has emerged as one of the most consistent environmental risk factors, with individuals raised in urban environments exhibiting nearly twofold increased risk compared to those in rural settings (Vassos et al., 2016). Similarly, migration—particularly among ethnic minorities—has been associated with elevated incidence rates, potentially due to social adversity, discrimination, and psychosocial stressors (Selten et al., 2020).
Age of Onset and Sex Differences
Schizophrenia typically manifests in late adolescence or early adulthood, with peak onset between ages 18 and 30 years. Males tend to experience earlier onset (often by 3–5 years) and generally exhibit more severe negative symptoms and poorer functional outcomes compared to females (Ochoa et al., 2012; Abel et al., 2010).
Females, in contrast, may show a second, smaller incidence peak later in life, possibly linked to hormonal factors such as declining estrogen levels. Estrogen is hypothesized to exert a neuroprotective effect, modulating dopaminergic and glutamatergic systems (Kulkarni et al., 2015).
Mortality and Life Expectancy
Individuals with schizophrenia experience significantly reduced life expectancy, with an average reduction of 10–20 years compared to the general population (Laursen et al., 2014; Hjorthøj et al., 2017). This excess mortality is attributable to both natural causes (e.g., cardiovascular disease, metabolic disorders) and unnatural causes, including suicide.
Suicide risk is particularly elevated, with approximately 5–10% of patients dying by suicide and a much higher proportion attempting suicide at least once during their lifetime (Hor & Taylor, 2010).
Comorbidities
Schizophrenia is frequently accompanied by comorbid conditions, including:
These comorbidities complicate treatment and contribute significantly to morbidity and mortality (De Hert et al., 2011; Neyra et al., 2024).
2.2 Clinical Features
Schizophrenia is characterized by a broad and heterogeneous range of symptoms, traditionally categorized into positive, negative, and cognitive domains. Increasingly, affective and behavioral symptoms are also recognized as integral components of the disorder.
2.2.1 Positive Symptoms
Positive symptoms reflect an excess or distortion of normal psychological functions and are often the most recognizable features of schizophrenia.
Key manifestations include:
These symptoms are strongly associated with dopaminergic hyperactivity in mesolimbic pathways and tend to respond relatively well to antipsychotic medications (McCutcheon et al., 2020).
2.2.2 Negative Symptoms
Negative symptoms represent a reduction or absence of normal emotional and behavioral functions and are increasingly recognized as major determinants of long-term disability.
They include:
Unlike positive symptoms, negative symptoms are often persistent and less responsive to treatment, posing significant challenges in clinical management (Kirkpatrick et al., 2006; Correll & Schooler, 2020).
2.2.3 Cognitive Impairments
Cognitive deficits are now considered a core feature of schizophrenia, present even before the onset of overt psychotic symptoms.
Commonly affected domains include:
These impairments have a profound impact on functional outcomes, including employment, social relationships, and independent living (Green et al., 2019).
Importantly, cognitive deficits are only minimally improved by current antipsychotic treatments, highlighting a critical unmet therapeutic need.
2.2.4 Affective and Behavioral Symptoms
In addition to the core symptom domains, many patients experience:
These features can fluctuate over time and may overlap with mood disorders, complicating diagnosis and treatment.
2.2.5 Disease Course and Heterogeneity
The course of schizophrenia is highly variable. While some individuals experience episodic illness with periods of remission, others develop a chronic, progressively deteriorating course.
Clinical trajectories can be broadly categorized as:
Approximately 20–30% of patients achieve substantial recovery, whereas a similar proportion develop treatment-resistant schizophrenia (Jääskeläinen et al., 2013; Samara et al., 2025).
This heterogeneity underscores the need for personalized and stratified treatment approaches.
2.3 Prodromal Phase and Early Signs
Before the onset of full psychosis, many individuals experience a prodromal phase, characterized by subtle changes such as:
Early identification of this phase has become a major focus of research, as timely intervention may delay or prevent progression to full-blown schizophrenia (Fusar-Poli et al., 2013).
3. PATHOPHYSIOLOGY OF SCHIZOPHRENIA
The pathophysiology of schizophrenia is increasingly understood as a multifactorial and systems-level process, involving complex interactions among neurotransmitter systems, neurodevelopmental alterations, immune responses, and genetic vulnerability. Rather than a single-cause disorder, schizophrenia reflects dysregulation across interconnected biological networks that evolve over time.
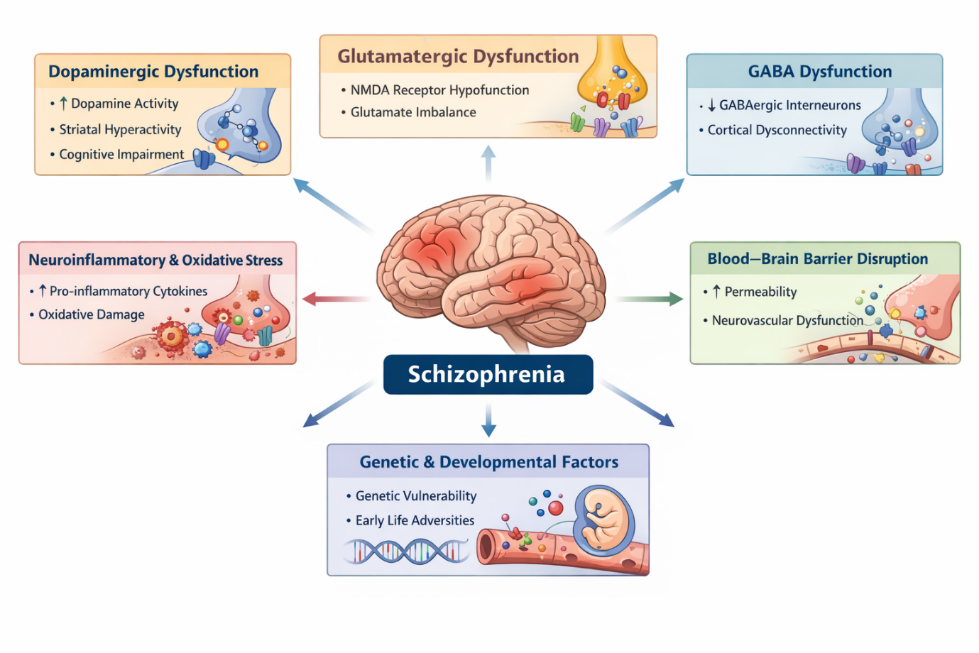
Figure 1: Multisystem Pathophysiology of Schizophrenia.
This schematic illustrates the complex and interconnected biological mechanisms underlying schizophrenia. Genetic susceptibility and environmental risk factors (e.g., prenatal stress, infection, and urban exposure) contribute to early neurodevelopmental disruptions. These disturbances lead to alterations in key neurotransmitter systems, including dopaminergic hyperactivity in mesolimbic pathways, glutamatergic NMDA receptor hypofunction, and GABAergic interneuron deficits, resulting in impaired neural circuit synchronization. Concurrently, immune activation and oxidative stress promote neuroinflammation and synaptic dysfunction, while blood–brain barrier disruption facilitates peripheral-central immune interactions. These combined processes culminate in abnormal brain connectivity and functional impairment, giving rise to the core clinical manifestations of schizophrenia, including positive symptoms, negative symptoms, and cognitive deficits.
3.1 Dopaminergic Dysregulation: Revisiting the Classical Model
The dopamine hypothesis remains one of the most influential frameworks in schizophrenia research. It posits that hyperactivity of dopaminergic transmission in mesolimbic pathways contributes to positive symptoms such as hallucinations and delusions, while reduced dopamine activity in the mesocortical pathway is associated with negative symptoms and cognitive deficits (McCutcheon et al., 2020).
Recent neuroimaging studies using positron emission tomography (PET) have provided robust evidence for increased presynaptic dopamine synthesis and release capacity in patients with schizophrenia, particularly during acute psychosis (Howes et al., 2017). However, this dopaminergic imbalance is now viewed as a downstream effect of broader circuit dysfunction rather than the primary cause of the disorder.
Importantly, the dopamine model does not fully explain:
These limitations have prompted the development of more integrative hypotheses.
3.2 Glutamatergic Dysfunction and NMDA Receptor Hypofunction
The glutamatergic hypothesis has emerged as a central pillar in modern schizophrenia research. It is primarily based on evidence that hypofunction of NMDA (N-methyl-D-aspartate) receptors disrupts synaptic plasticity and cortical connectivity (Coyle et al., 2012; Uno & Coyle, 2019).
Pharmacological models using NMDA antagonists such as ketamine and phencyclidine (PCP) replicate both positive and negative symptoms, as well as cognitive deficits, providing strong support for this hypothesis.
Mechanistically, NMDA receptor hypofunction leads to:
This imbalance disrupts neural oscillations and functional connectivity between the prefrontal cortex and hippocampus, key regions implicated in cognition and reality processing (Anticevic et al., 2015).
Recent studies (2024–2025) further suggest that glutamatergic abnormalities may precede dopaminergic dysregulation, positioning glutamate as an upstream driver in schizophrenia pathophysiology.
3.3 GABAergic Interneuron Dysfunction
Closely linked to glutamatergic abnormalities is dysfunction in GABAergic interneurons, particularly parvalbumin-positive interneurons. These cells are essential for maintaining synchronization of neural networks and regulating cortical oscillations.
Postmortem and imaging studies reveal:
This leads to disorganized neural activity, which is believed to underlie cognitive deficits and impaired information processing (Lewis et al., 2012; Gonzalez-Burgos et al., 2015).
3.4 Neuroinflammation and Immune System Dysregulation
There is growing recognition that schizophrenia involves chronic low-grade inflammation and immune activation. Elevated levels of pro-inflammatory cytokines—such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP)—have been consistently reported in patients (Khandaker et al., 2015; Miller & Goldsmith, 2017).
Microglial activation, observed through neuroimaging and postmortem studies, suggests that innate immune responses contribute to synaptic remodeling and neuronal damage.
Key mechanisms include:
Recent work (2024–2026) highlights that immune dysfunction may not merely be a consequence of schizophrenia but could act as a causal contributor, particularly in individuals exposed to prenatal infections or early-life stress (Gangadin & Enthoven, 2024).
3.5 Oxidative Stress and Mitochondrial Dysfunction
Oxidative stress plays a critical role in neuronal injury and has been increasingly implicated in schizophrenia. Patients often exhibit:
This imbalance can impair:
Mitochondrial dysfunction further exacerbates oxidative damage, leading to impaired neuronal resilience (Flatow et al., 2013; Oatu et al., 2026).
Importantly, oxidative stress interacts with both inflammatory pathways and glutamatergic dysfunction, forming a vicious cycle that contributes to disease progression.
3.6 Blood–Brain Barrier (BBB) Dysfunction
Emerging evidence suggests that schizophrenia may involve disruption of the blood–brain barrier, a critical structure that regulates the passage of molecules between the bloodstream and the central nervous system.
BBB dysfunction can result in:
Recent molecular studies have identified alterations in tight junction proteins and endothelial function in schizophrenia patients (Zhang et al., 2025).
This finding provides a mechanistic link between systemic inflammation and central nervous system pathology, reinforcing the concept of schizophrenia as a whole-body disorder.
3.7 Neurodevelopmental Hypothesis
The neurodevelopmental model proposes that schizophrenia originates from early brain developmental disturbances, which may remain latent until adolescence or early adulthood.
Contributing factors include:
These early insults can disrupt:
Adolescence, characterized by synaptic pruning and hormonal changes, may act as a critical period during which latent vulnerabilities manifest clinically (Rapoport et al., 2012; Birnbaum & Weinberger, 2017).
3.8 Genetic and Epigenetic Mechanisms
Schizophrenia has a strong genetic component, with heritability estimates of approximately 70–80%. Genome-wide association studies have identified numerous susceptibility loci, particularly in genes related to:
However, genetic risk alone is insufficient to cause the disorder. Epigenetic mechanisms—such as DNA methylation and histone modification—mediate interactions between genes and environmental exposures.
These processes can:
Recent studies emphasize that schizophrenia arises from polygenic risk combined with environmental modulation, rather than single-gene mutations.
3.9 Integrated Systems-Level Model
Current evidence supports a unified model in which multiple biological systems interact dynamically:
These interconnected pathways collectively lead to abnormal neural connectivity, impaired information processing, and clinical symptom expression.
4. Diagnosis and Biomarker Development
Accurate diagnosis of schizophrenia remains a complex challenge due to its clinical heterogeneity, overlapping symptoms with other psychiatric disorders, and the absence of universally validated biological markers. While diagnostic frameworks are still primarily symptom-based, recent advances in neuroimaging, molecular biology, and artificial intelligence (AI) are gradually reshaping the diagnostic landscape toward more objective and biologically informed approaches.
4.1 Clinical Diagnosis
The diagnosis of schizophrenia continues to rely on standardized classification systems, primarily the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5-TR) and the International Classification of Diseases (ICD-11). These systems define schizophrenia based on the presence of characteristic symptoms—such as delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, and negative symptoms—persisting for a specified duration and associated with functional impairment (American Psychiatric Association, 2022; WHO, 2019).
A key limitation of current diagnostic criteria is their phenomenological nature, meaning they are based on observable symptoms rather than underlying biological mechanisms. This often leads to:
Furthermore, inter-individual variability in symptom presentation highlights the need for dimensional and personalized diagnostic frameworks, rather than strictly categorical classifications (Insel, 2017).
Early detection strategies, particularly for individuals at clinical high risk (CHR) of psychosis, have gained attention in recent years. Structured interviews and risk calculators have shown moderate predictive validity, but their integration into routine clinical practice remains limited (Fusar-Poli et al., 2017).
4.2 Biomarkers and AI-Based Detection
The search for objective biomarkers in schizophrenia has intensified, with growing interest in integrating neuroimaging, electrophysiology, and computational approaches to improve diagnostic accuracy and early detection.
Structural and functional neuroimaging studies have consistently identified abnormalities in key brain regions, including:
Functional MRI (fMRI) and diffusion tensor imaging (DTI) studies suggest that schizophrenia is characterized by disrupted brain network connectivity, rather than localized deficits (Koutsouleris et al., 2018).
However, despite robust group-level findings, neuroimaging biomarkers lack sufficient specificity and reproducibility for individual-level diagnosis.
Electroencephalography (EEG) offers a cost-effective and temporally precise method for assessing neural activity. Common findings in schizophrenia include:
These electrophysiological markers are considered promising candidates for early detection and monitoring, particularly in high-risk populations (Light & Näätänen, 2013).
Recent advances in AI and machine learning have enabled the integration of multimodal data—including neuroimaging, EEG, genetic, and clinical variables—to improve diagnostic performance.
Machine learning models have demonstrated:
A recent systematic review (Saha et al., 2024) highlights that AI-based approaches are rapidly improving in accuracy and robustness. However, several barriers remain:
Thus, while AI holds significant promise, its translation into routine psychiatric practice requires further validation and standardization.
4.3 Molecular Biomarkers
Molecular biomarkers offer the potential to provide objective, quantifiable indicators of disease processes, complementing clinical assessment.
Brain-derived neurotrophic factor (BDNF) has been widely studied in schizophrenia. Reduced BDNF levels have been associated with:
However, findings remain inconsistent, and BDNF is not specific to schizophrenia (Green et al., 2011).
A growing body of evidence supports the role of immune dysregulation in schizophrenia. Elevated levels of inflammatory markers such as:
have been observed in both early-stage and chronic patients (Miller & Goldsmith, 2017).
These markers may help identify inflammatory subtypes of schizophrenia, potentially guiding targeted therapies.
Advances in genomics have identified numerous genetic variants associated with schizophrenia risk. Polygenic risk scores (PRS) are increasingly used to:
Epigenetic modifications, including DNA methylation and histone changes, further influence gene expression and may serve as dynamic biomarkers of disease state (Ursini et al., 2018).
Despite promising findings, molecular biomarkers face several challenges:
A recent review (Liberona et al., 2024) emphasizes that no single biomarker is currently sufficient for clinical diagnosis, highlighting the need for multi-biomarker panels and integrative approaches.
4.4 Toward Integrated and Precision Diagnostics
The future of schizophrenia diagnosis lies in integrating clinical, biological, and computational data into a unified framework. Multimodal approaches combining:
are expected to enable:
However, achieving this goal will require large-scale longitudinal studies, improved data standardization, and stronger collaboration between clinical and computational disciplines.
Table 1: Summary of Biomarkers and Diagnostic Approaches in Schizophrenia
|
Category |
Biomarker/Tool |
Key Findings |
Clinical Utility |
Limitations |
Key References |
|
Clinical Diagnosis |
DSM-5 / ICD-11 criteria |
Symptom-based classification (positive, negative, cognitive symptoms) |
Gold standard for diagnosis |
Subjective, lacks biological basis |
APA (2022); WHO (2019) |
|
Neuroimaging |
MRI (structural) |
Reduced gray matter (PFC, hippocampus) |
Supports group-level differences |
Low specificity for individuals |
Koutsouleris et al., 2018 |
|
fMRI (functional) |
Altered connectivity (DMN, salience network) |
Identifies network dysfunction |
Not yet clinically standardized |
Anticevic et al., 2015 |
|
|
DTI |
White matter abnormalities |
Insight into connectivity deficits |
Limited reproducibility |
Kubicki et al., 2017 |
|
|
EEG-Based Markers |
P300 amplitude |
Reduced cognitive processing |
Early detection potential |
Variable sensitivity |
Light & Näätänen, 2013 |
|
Gamma oscillations |
Impaired neural synchrony |
Reflects circuit dysfunction |
Technical variability |
Uhlhaas & Singer, 2015 |
|
|
P50 suppression |
Sensory gating deficits |
Biomarker for early-stage disease |
Not disease-specific |
Freedman et al., 2013 |
|
|
Molecular Biomarkers |
BDNF |
Reduced levels linked to cognition deficits |
Potential disease progression marker |
Inconsistent findings |
Green et al., 2011 |
|
Cytokines (IL-6, TNF-α) |
Elevated inflammation markers |
Identifies inflammatory subtype |
Low specificity |
Miller & Goldsmith, 2017 |
|
|
CRP |
Systemic inflammation |
Prognostic indicator |
Affected by comorbidities |
Khandaker et al., 2015 |
|
|
Genetic Markers |
GWAS loci |
>100 risk loci identified |
Risk prediction (population level) |
Low individual predictive power |
Ripke et al., 2020 |
|
Polygenic Risk Score (PRS) |
Aggregated genetic risk |
Early risk stratification |
Limited clinical application |
Wray et al., 2021 |
|
|
Epigenetic Markers |
DNA methylation |
Alters gene expression |
Reflects environmental effects |
Dynamic and variable |
Ursini et al., 2018 |
|
AI & Machine Learning |
Multimodal ML models |
80–90% classification accuracy |
Early diagnosis and subtype detection |
Poor generalizability |
Saha et al., 2024 |
|
Deep learning (neuroimaging) |
Pattern recognition in brain scans |
Automated diagnosis |
Black-box issue |
Vieira et al., 2017 |
|
|
Integrated Biomarkers |
Multimodal panels |
Combine imaging + molecular + clinical data |
Most promising future approach |
Lack of standardization |
Liberona et al., 2024 |
5. Treatment Strategies: Current and Emerging
The management of schizophrenia has evolved considerably over recent decades, transitioning from a purely dopamine-centered pharmacological approach to a more multidimensional and personalized treatment framework. Despite significant advances, treatment remains challenging due to heterogeneity in symptom profiles, variable treatment response, and the persistence of negative and cognitive symptoms.
5.1 Conventional Antipsychotics
Conventional antipsychotics remain the cornerstone of schizophrenia treatment and primarily exert their therapeutic effects through dopamine D2 receptor antagonism. First-generation (typical) antipsychotics, such as haloperidol, effectively reduce positive symptoms but are associated with a high risk of extrapyramidal side effects (EPS) and tardive dyskinesia.
Second-generation (atypical) antipsychotics, including risperidone, olanzapine, and quetiapine, offer a broader receptor profile, combining dopamine antagonism with serotonergic (5-HT2A) modulation, which improves tolerability and modestly benefits negative symptoms (Leucht et al., 2013).
However, significant limitations persist:
These challenges underscore the need for alternative and adjunctive therapies.
5.2 Novel Pharmacological Approaches
Recent therapeutic developments aim to target non-dopaminergic pathways, reflecting advances in understanding schizophrenia pathophysiology.
5.2.1 Muscarinic Receptor Agonists
Muscarinic receptor modulation has emerged as a promising dopamine-independent strategy. KarXT (xanomeline–trospium) is a novel combination therapy that selectively stimulates M1/M4 muscarinic receptors, improving psychotic symptoms without directly blocking dopamine receptors.
Clinical trials demonstrate that KarXT:
This represents a significant shift toward cholinergic system targeting in schizophrenia treatment (Brannan et al., 2021; Ye et al., 2025).
5.2.2 Glutamatergic Modulators
Given the strong evidence for NMDA receptor hypofunction, glutamatergic agents are actively being explored.
Key approaches include:
These agents aim to restore excitatory–inhibitory balance and improve cognitive and negative symptoms, which are poorly addressed by dopamine-based therapies (Coyle et al., 2012; Uno & Coyle, 2019).
Although clinical results have been mixed, ongoing trials continue to refine dosing strategies and patient selection.
5.2.3 Anti-inflammatory and Antioxidant Therapies
The recognition of immune dysregulation and oxidative stress in schizophrenia has led to exploration of adjunctive anti-inflammatory and antioxidant treatments.
Examples include:
These interventions may:
However, results remain variable, and these therapies are not yet standard of care (Miller & Goldsmith, 2017; Anwar et al., 2025).
5.2.4 Natural Compounds and Phytochemicals
Natural compounds such as flavonoids, polyphenols, and herbal extracts are gaining attention due to their neuroprotective, anti-inflammatory, and antioxidant properties.
Preclinical and early clinical studies suggest:
While promising, these compounds require further validation through large-scale clinical trials before routine clinical use (Ye et al., 2025).
5.3 Treatment-Resistant Schizophrenia (TRS)
Treatment-resistant schizophrenia (TRS) affects approximately 30% of patients, defined by inadequate response to at least two antipsychotic trials of adequate dose and duration.
Clozapine remains the gold standard for TRS, demonstrating superior efficacy in reducing both positive symptoms and suicide risk (Samara et al., 2025). However, its use is limited by:
Emerging strategies for TRS include:
These approaches aim to improve outcomes in this difficult-to-treat population.
5.4 Cognitive and Negative Symptom Management
Cognitive impairment and negative symptoms represent major unmet needs in schizophrenia treatment, as they are closely linked to functional disability.
Cognitive Remediation Therapy (CRT)
CRT involves structured behavioral interventions designed to improve:
Meta-analyses show that CRT can produce moderate improvements in cognition and functional outcomes, particularly when combined with psychosocial rehabilitation (Wykes et al., 2011).
Pharmacological Approaches
Emerging pharmacological strategies include:
These aim to target underlying neurobiological mechanisms of cognitive dysfunction.
Digital Therapeutics
Digital interventions, including:
are increasingly being used to enhance engagement and provide scalable treatment options (Calzavara-Pinton et al., 2024).
5.5 Comorbidity and Integrated Care
Schizophrenia is frequently associated with psychiatric and physical comorbidities, which significantly influence disease outcomes.
Substance Use Disorders
Substance use—particularly cannabis, alcohol, and nicotine—is highly prevalent and associated with:
Metabolic and Cardiovascular Disorders
Antipsychotic medications, especially second-generation agents, are linked to:
These contribute to the elevated cardiovascular mortality observed in schizophrenia.
Integrated Care Models
Modern treatment emphasizes holistic and integrated care approaches, including:
Such models have been shown to improve:
6. Future Directions and Research Gaps
Despite substantial progress in understanding schizophrenia, several critical gaps remain that continue to limit advances in diagnosis, treatment, and long-term outcomes. One of the most pressing challenges is the lack of reliable and clinically applicable biomarkers. Although numerous candidates—ranging from neuroimaging signatures to inflammatory and genetic markers—have been identified, none have yet demonstrated sufficient sensitivity, specificity, and reproducibility for routine clinical use. This highlights the need for large-scale, longitudinal, and multi-center studies that can validate these markers across diverse populations.
Another key limitation lies in the incomplete understanding of disease heterogeneity. Schizophrenia is increasingly recognized as a spectrum of disorders rather than a single entity, yet current diagnostic systems do not adequately capture this complexity. Future research must focus on stratifying patients into biologically meaningful subtypes, which could enable more targeted and effective interventions. In this context, the integration of multi-omics data, neuroimaging, and clinical phenotyping—supported by advanced computational models—holds promise for advancing precision psychiatry.
Therapeutically, while existing antipsychotics are effective for positive symptoms, there remains a significant unmet need in addressing negative symptoms and cognitive deficits, which are the primary drivers of long-term disability. Emerging treatments targeting glutamatergic, cholinergic, and inflammatory pathways are promising, but their clinical efficacy and long-term safety require further validation. Additionally, treatment-resistant schizophrenia continues to pose a major challenge, underscoring the necessity for novel therapeutic strategies and better predictors of treatment response.
The role of environmental and developmental factors also warrants deeper investigation, particularly in understanding how early-life exposures interact with genetic susceptibility to influence disease onset. Preventive strategies, especially during the prodromal phase, remain underdeveloped but could significantly alter disease trajectories if effectively implemented.
Finally, although advances in artificial intelligence and digital health technologies offer exciting opportunities for early detection and personalized care, their translation into real-world clinical settings is still limited by issues such as data standardization, interpretability, and ethical considerations.
In summary, future progress in schizophrenia research will depend on bridging the gap between biological discovery and clinical application, fostering interdisciplinary collaboration, and prioritizing patient-centered, personalized approaches. Addressing these challenges is essential for moving beyond symptom management toward meaningful recovery and improved quality of life for individuals affected by schizophrenia.
CONCLUSION
Schizophrenia remains one of the most challenging psychiatric disorders due to its complexity, heterogeneity, and long-term impact on functioning and quality of life. While traditional models have largely focused on dopaminergic dysfunction, current evidence supports a broader and more integrated understanding that encompasses glutamatergic imbalance, immune dysregulation, oxidative stress, and neurodevelopmental disturbances. This evolving perspective has not only deepened our understanding of disease mechanisms but also opened new avenues for diagnosis and treatment.
In clinical practice, diagnosis still relies heavily on symptom-based criteria, highlighting a critical gap between research advances and real-world application. Although promising biomarkers and AI-based tools are emerging, their routine use remains limited, emphasizing the need for further validation and standardization. Similarly, while existing antipsychotic medications are effective for managing positive symptoms, their limited impact on negative symptoms and cognitive deficits continues to restrict overall recovery.
Encouragingly, the development of novel therapeutic strategies—particularly those targeting non-dopaminergic pathways—signals a shift toward more comprehensive and individualized care. At the same time, addressing comorbid conditions and adopting integrated care models are essential for improving long-term outcomes.
Looking ahead, the future of schizophrenia research and treatment lies in bridging the gap between biological insights and clinical practice. Advancing precision psychiatry, improving early detection, and developing multi-target interventions will be key to achieving meaningful progress. Ultimately, a more holistic and patient-centered approach will be crucial in moving beyond symptom control toward sustained recovery and improved quality of life.
REFERENCES

Shivani, Dr. Ajeet Pal Singh, Dr. Amar Pal Singh, Beyond Dopamine: Emerging Neurobiological Mechanisms and Therapeutic Innovations in Schizophrenia, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 2468-2484, https://doi.org/10.5281/zenodo.19605635
 10.5281/zenodo.19605635
10.5281/zenodo.19605635
