IPS Academy College of Pharmacy, Rajendra Nagar, A.B. Road, Indore, Madhya Pradesh, India 452012
AI is a novel technology that has been used in heart treatment for a long time. It has made it easier to diagnose, assess risk, treat, and keep an eye on patients in a method that costs less. Cardiovascular diseases (CVDs) continue to be the primary cause of global death. AI-based technologies like machine learning (ML), deep learning (DL), and natural language processing (NLP) have made it possible for doctors to look at data that is getting more and more complicated with accuracy and speed. The article talks about some of the most popular AI-based clinical tools that cardiologists utilize right now. These are cardiac imaging, predictive analytics, wearable technologies, and systems that help doctors make decisions. We will talk about how AI could be used in the future between groups of people, such as in genomics, robotic interaction, and digital twins, to mention a few. This article aims to summarize previously reported accomplishments and highlight their importance in advancing research, evaluating evidence-based clinical management, and improving AI accessibility to enhance patient outcomes in cardiovascular disease.
The cardiovascular system is also called as circulatory system of our body. Cardiovascular diseases (CVD) are the number one cause of death worldwide and resulted into approximately 18 million deaths per year1. Nonetheless, that means the early diagnosis and individualized treatment pose big challenges for cardiology2 despite great improvement was achieved in pharmacologic therapy and interventional procedures. Transmutation of cardiovascular information from images and electrocardiograms to genomics and electronic health records (EHRs) also requires more sophisticated analytical solutions for the discovery of knowledge and advancement in this field3.
AI will alter healthcare by offering us new tools that can help us uncover information, see patterns in business, and think about challenges that can come up in the future4. AI helps clinicians make better diagnoses and tailor therapies for people with heart disease by using large, diverse datasets like electronic health records (EHRs), imaging data, genomics data, and signals from wearable devices. This will help patients get better results5.
Each realm of the cardiovascular care continuum has integrated technologies based on artificial intelligence (AI) such as machine learning (ML), deep learning (DL) and natural language processing (NLP). Such systems offer automatic image interpretation, risk-stratifications, remote control of treatments by patients and parents, robotic telesurgery assisted treatment at distance as well as virtual simulations of the patient (virtual patient or so-called digital twin)6,7.
The convergence of AI and cardiovascular medicine may bring care out of reaction mode – in other words, spotting disease early, treating it more directly and continuously staying vigilant for recovery progress. However, AI is accompanied by a number of ethical, regulatory and technical challenges that must be addressed in order to ensure its safe and fair deployment towards their specific patients8.
In the current manuscript, we attempt to present a comprehensive review of AI in CV medicine from trends to future directions. From imaging and predictive analytics to wearables, genomics, robotics and next generation computing - discussing the potential use cases and impact of AIs in high level patient use cases as well as for technical constraints/ethical considerations on using AI.

Fig. No. 1: BLOCK DIAGRAM OF CARDIOVASCULAR SYSTEM
MATERIALS AND METHODS
Searching a massive number of articles and integrating the peer-reviewed literature, clinical trials, and bibliometric analyses on AI in cardiovascular medicine, this review article was written9. The search strategy used databases such as PubMed, Web of Science Scopus and Google Scholar10. The key words used when searching include " artificial intelligence and cardiology ", " machine learning heart disease ", " deep learning in heart scans ", " AI of heart failure" and "predictive analytics for cardiovascular diseases"11. The included studies had to meet strict criteria for selection12:
The following studies were excluded12:
RESULTS AND DISCUSSION:
Current Trends and Future Prospects in AI for Cardiovascular Medicine
1. AI in Cardiac Imaging
Cardiac imaging has been transformed by using the Artificial Intelligence (AI), which is now able to handle image acquisition, segmentation and interpretation. AI is used across various imaging modalities, such as echocardiography (ECG), cardiac CT (CCT), cardiovascular magnetic resonance (CMR), nuclear imaging and cardiac MRI14-15.
1.1 Echocardiography
The AI-based echocardiography leverages CNNs to automate:
Several tools such as EchoNet-Dynamic have achieved performance comparable to humans in left ventricular function evaluation which uses 2D echocardiograms16.
1.2 Cardiac Computed Tomography (CCT)
AI makes CCT better by:
The AI-based quantitative CT shows a rough correlation with invasive methods like NIRS-IVUS17,18.
1.3 Cardiovascular Magnetic Resonance (CMR)
AI is very important for a lot of CMR uses:
1.4 Nuclear Imaging AI and PET
AI helps perfusion mapping by increasing resolution and lowering noise levels. It also helps standardize the distribution of myocardial tracers by looking at how much they are taken up. When PET is used with CT or MRI, computers can do a full analysis MEMBER21.
TABLE 1: AI APPLICATIONS ACROSS CARDIAC IMAGING MODALITIES14-21
|
Modality |
AI Functionality |
Clinical Benefit |
|
Echocardiography |
Chamber segmentation, EF estimation |
Real-time analysis, reduced variability |
|
CCT |
Plaque analysis, vessel tracing |
Early CAD detection |
|
CMR |
Tissue characterization, flow quantification |
Accurate diagnosis of cardiomyopathies |
|
PET/ Nuclear |
Perfusion mapping, tracer analysis |
Improved ischemia detection |
2. AI in Predictive Analytics and Risk Stratification
One of the most important uses of AI is to use predictive analytics in heart medicine. AI models are better than the Framingham Risk Score and the ASCVD calculator, which are both traditional ways to measure risk22,23. They work well because they use a lot of different kinds of data, such as EHRs, genetic markers, and lifestyle factors24.
Machine learning methods like XG Boost and random forests predict the myocardial infarction, stroke, and the heart failure with high sensitivity and specificity which helps in predicting analytics and risk stratification.
These models allow healthcare providers to identify high-risk patients early.
They also support preventive measures, such as starting statins or making lifestyle changes, that are tailored to individual risk profiles25.
2.1 Conventional Risk Models vs AI-Driven Formulations Traditional risk models
It includes the Framingham Risk Score, ASCVD calculator and SCORE system depends on a small set of variables (for example age, cholesterol and blood pressure)22. Such models may not accommodate variability in the profiles of individual patient, and therefore perform less accurately amongst different populations24.
Specially DL-based, ensemble learning methods of AI models can:
TABLE 2: COMPARISON OF TRADITIONAL VS AI-BASED RISK MODELS
|
Feature |
Traditional Models |
AI-Based Models |
|
Variables used |
Limited (5–10) |
Extensive (100+) |
|
Data types |
Structured only |
Structured + unstructured |
|
Population bias |
High |
Lower (with diverse training) |
|
Accuracy |
Moderate |
High (AUC > 0.90 in some models) |
|
Adaptability |
Static |
Dynamic and self-improving |
2.2 AI Algorithms for Cardiovascular Risk Prediction
A number of machine learning algorithms have been tried in cardiovascular risk prediction25:
The features of these models include:
2.3 Real-World Applications
We can now use ai technology, "big data," and many other tools to predict the five-year cardiac risk of a patient by means of its deep learning models trained on more than one million electronic health records (EHRs). Beyond risk prediction, AI algorithms are now widely used to analyze medical images such as ECG and CT scans, identifying abnormalities that can escape from human detection24.
Once equipped with imaging, genomics as well as traditional clinical data, AI4Heart can distinguishes among many times before ill-health occurs a bad orchard from its companion (Lu, 48). LYNA, developed originally for use with cancer patients, has been adapted to assess cardiovascular risk26.
2.4 Integration into Clinical Algorithms AI-based risk scores
These are being integrated into electronic health records to24:
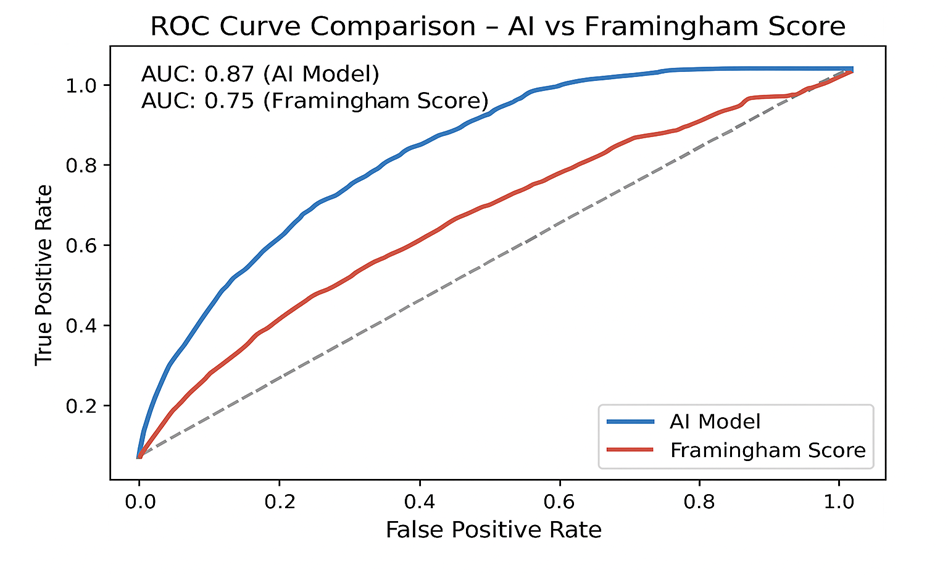
Fig. No. 2: ROC CURVE COMPARISON—AI VS. FRAMINGHAM SCORE (SHOWS THAT AI MODELS HAVE A HIGHER AUC FOR PREDICTING HEART EVENTS)
2.5 Limitations and Challenges
3. Wearable devices and remote health monitoring devices that use AI
These have opened up a whole new world of cardiovascular monitoring when used with AI. They let you collect and analyze data in real time. Wearable devices can help patients keep track of their heart rate, blood oxygen levels, blood pressure, and physical activity27. They make it easier for patients and healthcare providers to embrace rapid cardiovascular disease identification, personalize treatment plans, and lower the number of hospitalizations. Devices that use AI and don't need to be watched by a doctor can also keep an eye on your heart all the time, day and night. Devices like the Apple Watch and KardiaMobile use AI algorithms to read single-lead ECGs. With a sensitivity of over 95%, they can find atrial fibrillation28.
The Zio Patch and BioBeat are two new kinds of patches that can check for heart failure by keeping an eye on thoracic impedance, heart rate variability, and breathing patterns29. These technologies also let patients and doctors keep an eye on each other, which can lead to faster actions, shorter hospital stays, and a better quality of life30.
3.1 Presentation of Wearable Technologies
Smartwatches, chest patches, biosensors, and implantable devices with sensors and AI algorithms that help people all over the world are all examples of wearables today. They keep track of things like how fast and how often the heart beats27.
3.2 Wearables AI Algorithm
AI enhances the functionality of wearables by:
Common machine learning models such as support vector machines (SVM), decision trees, and recurrent neural networks (RNNs) are embraced by wearables31.
3.3 Purposes in Clinical Detection
Atrial Fibrillation Detection
AI in the apple watch and KardiaMobile for wearable devices is used to analyze single-lead ECGs. The performance of the stethoscope is more than 95% sensitive in discerning atrial fibrillation. Early detection AF can reduce the risk of stroke and help guide anticoagulant therapy28.
Monitoring Heart Failure
Patches with AI on board (for instance, the Zio Patch and BioBeat) use thoracic impedance, HRV measurements and respiratory recording to predict when forms of heart failure might worsen. Pre-emptive alerts tie medicine adjustments made at home or in an ambulance may prevent hospital admission29.
High Blood Pressure Management
Wearable devices with a digital cuff that can measure blood pressure use AI to change the readings based on the time it takes for the pulse to move and photoplethysmography (PPG). These tools help people change their medications and their way of life when they need to. It helps find hidden hypertension and white coat hypertension, predicts when high blood pressure will happen, and allows for personalized treatment, among other things30.
3.4 Patient Participation and Compliance
Devices that use AI and work with wearable sensors can give you personalized reminders and feedback. It turns health goals into a game, which makes people 50% less likely to skip their medicine and more likely to eat better and work out more30.
TABLE 3: AI-ENABLED WEARABLES IN CARDIOVASCULAR CARE
|
Device |
AI Functionality |
Clinical Utility |
|
Apple Watch |
ECG analysis, AF detection |
Stroke prevention |
|
Fitbit |
Heart rate variability, activity tracking |
Lifestyle modification |
|
BioBeat |
BP, HR, SpO? monitoring |
Hypertension and heart failure |
|
Zio Patch |
Long-term rhythm monitoring |
Arrhythmia diagnosis |
3.5 Limitations and Challenges
3.6 Future Directions
4. AI-assisted stethoscopes
AI-enhanced stethoscopes combine regular sound sensors with ECG capabilities, making it easier to find heart problems, especially arrhythmias and valvular disorders32. The Eko DUO and StethoMe are two examples of devices that work well for both kids and adults33. These advanced stethoscopes use machine learning to look at heart sounds34.
4.1 Evolution of the Digital Stethoscope
Traditional stethoscopes can make mistakes because they depend on the doctor's ability to listen carefully. Digital stethoscopes turn sounds from the heart into electronic signals that can be seen, stored, and studied. This makes the results more accurate and exact32.
AI improves this by:
Examples include:
4.2 Clinical Applications
Valvular Heart Disease: AI algorithms, which have been trained on thousands of annotated heart sound recordings, can identify:
Arrhythmia Detection ECG equipped dual-mode stethoscopes may detect:
Paediatric Cardiology AI improves auscultation in children, who frequently have faint and hard to discern heart sounds. It can help to identify congenital heart defects and innocent murmurs and more diseases.
Telemedicine platforms are increasingly used with AI-supported stethoscopes.
Remote clinicians can:
4.4 Limitations and Challenges
4.5 Future Directions
TABLE 4: CAPABILITIES OF AI-SUPPORTED STETHOSCOPES
|
Device |
AI Features |
Clinical Use |
|
Eko DUO |
ECG + murmur detection |
Valvular disease, AF |
|
StethoMe |
Sound classification |
Pediatric screening |
|
Thinklabs One |
Amplified digital auscultation |
Heart failure monitoring |
|
Butterfly iQ+ |
AI-guided ultrasound |
Cardiac imaging support |
5. Clinical Decision Support Systems (CDSS) Powered by AI
CDSS are computer applications designed to help the health care professionals in making evidence-based decisions. Enriched with AI, these systems become state-of-the-art and build on extensive databases identifying the patterns, offering personalized recommendations with hwlp of AI by identifying the best practice in the cardiovascular care38.
AI-driven (CDSS) support clinicians in the diagnosis, planning of treatment, and prognosis modeling38. They use the patient data and clinical guidelines to offer the optimal therapies, highlight alerts on possible side effects of any drug used by the particular patient, and perform record-keeping automatically and report if any side effect or adverse effect of a drug detected on patients39.
Notable examples include HeartFlow Analysis for non-invasive coronary FFR estimation and CardioSmart Advisor for customized care planning²?. AI-driven clinical decision support systems improve diagnostic accuracy, reduce errors, and increase clinical workflow efficiency40.
5.1 Overview of AI-Driven CDSS
Traditional CDSS use logic that is based on rules that have already been set and clinical guidelines that are set in stone. AI-driven CDSS, on the other hand, use advanced technologies like machine learning, deep learning, and natural language processing to:
AI-powered CDSS also learn from new data and clinical experience, which makes them more accurate over time. This is different from older systems38,41.
5.2 Components of CDS Systems
Level of Data Integration: You can effortlessly dive into a treasure trove of data from all sorts of sources, like genomic databases, those fancy wearable gadgets, imaging systems, and the ever-popular electronic health records (EHRs). It's like a data buffet, and you're invited to feast on it40.
Getting AI to do your bidding!
Dive into the wacky world of complex algorithms that whip up spot-on classifications, predictions, and suggestions tailored just for you—like a personal assistant who knows your coffee order better than you do.
Ambitions for the user interface: Handing healthcare professionals a treasure map of clear, useful information that's as easy to read as a comic book and totally on point for what they need41.
5.3 Application in Cardiology
Diagnosis Assistance
AI-powered CDSS may act like a doctor by looking at a patient's test results, medical history, and symptoms and coming up with a list of possible diagnoses, like a game of medical bingo! To give you an idea: HFrEF and HFpEF are like the odd couple of heart failure. They each have their own unique traits that set them apart from the rest42.
Treatment Optimization
AI-CDSS gives therapeutic recommendations that are based on clinical criteria and the specific needs of each patient is by choosing the optimum antithrombotic medication for atrial fibrillation39.
Based on the lipid profile and hereditary risk factors, it is recommended to start statins,
deciding who can get device-based treatments like CRT and ICD42.
IBM Watson and Google DeepMind are two systems that can guess: -
Workflow Automation
AI-CDSS can do simple tasks on its own, such as:
5.4 Benefits
5.5 Future Directions
TABLE 5: AI-CDSS CAPABILITIES IN CARDIOVASCULAR CARE
|
Function |
AI Capability |
Clinical Impact |
|
Diagnosis |
Pattern recognition from EHRs and imaging |
Early and accurate detection |
|
Treatment |
Personalized therapy recommendations |
Improved outcomes |
|
Prognosis |
Risk prediction models |
Preventive interventions |
|
Workflow |
Automation of documentation and alerts |
Increased efficiency |
6. AI in Genomics and Precision Medicine
Using genomics and artificial intelligence together makes it possible to use precision medicine in new ways to treat heart problems. By combining genetic data with clinical and lifestyle information, AI can find new biomarkers, figure out the best treatments for a person, and even figure out who is more likely to get sick. AI is making genomics in heart care happen faster by helping to figure out complicated genetic data for predicting risk and tailoring treatment to each patient44.Machine learning algorithms can identify relevant single nucleotide polymorphisms (SNPs) from genome-wide association studies and build polygenic risk scores for disorders such as coronary heart disease and atrial fibrillation45. AI systems such as MyGeneRank and CardioDx turn genomic profiles into actionable decisions through AI guidance on questions like whether to wait and see if you're at high risk of an existing condition to undergo drug therapy, lifestyle change early detection46. Such strategies allow medicines to meet specific needs by taking into consideration an individual's genetic makeup47.
6.1 Cardiovascular Disease in the Era of Precision Medicine
This section describes how precision medicine has begun to benefit... In cardiology, prevention, diagnosis and treatment today must be: Precisely honed Genetic risk scoring Pharmacogenomics Molecular phenotyping Targeted therapies AI has become indispensable. Charles Scriver Credit: © Charles B. Scriver It processes high-dimensional genomic data sets and uncovers complex interactions between genes and with the environment44,47.
6.2 AI Techniques Used in Genomic Analysis
AI algorithms in genomics includes:
6.3 Pharmacogenomics
AI mode’s forecast—how an individual will respond to cardiovascular drugs for example:
Among the many clinical pathways supported by patents this year was AI-CDSS, integrating both genetic and clinical data to recommend a personalized drug regimen; small adverse events can thus be greatly reduced and beneficial outcomes are more likely.
6.4 Biomarker Discovery
AI can be used to aid in biomarker study by performing the following functions44,48:
6.5 Clinical Implementation
6.6 Challenges and Limitations
6.7 Future Directions
TABLE 6:AI APPLICATIONS IN GENOMICS FOR CARDIOVASCULAR MEDICINE
|
Application |
AI Role |
Clinical Impact |
|
Polygenic Risk Scoring |
Variant selection and weighting |
Early disease prediction |
|
Pharmacogenomics |
Drug response modeling |
Personalized therapy |
|
Biomarker Discovery |
Pattern recognition in omics data |
Novel diagnostic tools |
|
Gene Expression Profiling |
Clustering and classification |
Disease subtyping |
7. Robotics and AI in Cardiac Surgery
The combination of AI with robotics has marked a new era in precision, safety, efficacy and outcome49. AI algorithm-guided robotic procedures provide superior visualization, dexterity and decision support, turning historical surgical methods into minimally invasive interventions that use data for improved outcomes. Systems like the da Vinci Surgical System and CorPath GRX employ AI to help them target optimal instrument trajectories, deliver real-time anatomical guidance and spare a surgeon from having to spend long hours on telesurgery50. Positive impacts of AI adoption have been observed in a variety of procedures such as mitral valve repair, coronary artery bypass grafting (CABG), and atrial septal defect closure51. According to reports in the literature, decreased blood loss, a short hospital stay and sooner recovery are seen when compared with conventional techniques52.
7.1 Overview of Robotic Cardiac Surgery
Robotic cardiac surgery employs computer-assisted systems such as the:
They are now being enhanced with AI to:
7.2 Applications of AI in Cardiac Surgery
Preoperative Planning
AI analyse imaging data (CT, MRI, echocardiography) using algorithms to:
Intraoperative Guidance
Postoperative Monitoring
You can use these factors to find possible problems, such as atrial fibrillation, infections after surgery, or bleeding, and get treatment early54.
7.3 Routine Robotic Cardiac Procedures
7.4 Benefits of AI-Robotic Integration

Fig. No. 3: WORKFLOW OF AI-ENABLED ROBOTIC CARDIAC SURGERY
7.5 Constraints and Hurdles
7.6 Future Directions
TABLE 7: AI AND ROBOTICS IN CARDIAC SURGERY
|
Phase |
AI Contribution |
Clinical Benefit |
|
Preoperative |
3D modelling, risk prediction |
Personalized planning |
|
Intraoperative |
Tissue recognition, guidance |
Precision and safety |
|
Postoperative |
Recovery tracking, complication alerts |
Early intervention |
8. Explainable AI and Digital Twins in Cardiology
Explainable AI (XAI) is an important tool for putting AI into practice in the real world because it makes the decision-making process of a model clear. SHAP (SHapley Additive exPlanations)56, LIME (Local Interpretable Model-Agnostic Explanations)57, and attention maps are some of these methods55. These let you know how important each attribute is and how the model works. Not only does this openness help build trust in AI systems, but it also helps doctors trust them and get permission from regulators and patients.
Digital twins—AI-powered computer models that represent the patient’s cardiovascular system—are capable of simulating the progression of the disease along with the treatment response58. These models combine anatomical, physiological, behavioural, and genomic data to not only make the care more personalized but also to facilitate the safe testing of interventions59.
8.1 Explainable AI (XAI)
It refers to the methods that make the decisions of complex AI models transparent and understandable to humans. In cardiology, XAI will help clinicians to:
Uses in Cardiology:
TABLE 8: EXPLAINABLE AI TECHNIQUES IN CARDIOVASCULAR APPLICATIONS
|
Technique |
Function |
Use Case |
|
SHAP |
Feature attribution |
Risk prediction models |
|
LIME |
Local model approximation |
Therapy recommendation |
|
Attention Maps |
Visual focus areas |
Imaging interpretation |
8.2 Digital Twins in Cardiology
These days, when technology is so personal, the lines between patients and doctors are quickly fading. This means that medical data like X-rays need to be shared and understood better right away. Digital twins meet this need by giving doctors virtual models of the patient's cardiovascular system, which are essential for accurate treatment58.
These digital twins always get real-time data from wearables, imaging equipment, genetic profiles, and clinical records. This lets them run simulations that show how diseases progress and how treatments work55. This is a problem that a lot of healthcare systems have: data comes from a lot of different places, which makes it hard to put it all together. But these digital twins might help put all of that data into one system. This is a good step forward that will probably lead to progress in the near future.
The main parts of a digital twin for cardiology are:
Uses
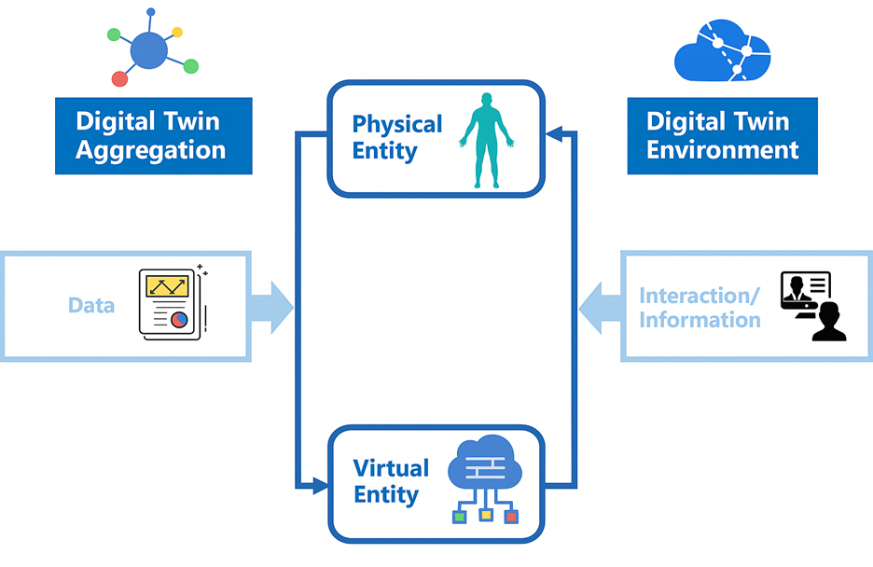
Fig. No. 4: ARCHITECTURE OF A CARDIAC DIGITAL TWIN
8.3 Benefits
8.4 Limitations and Challenges
8.5 Future Directions
9. AI in Population Health and Epidemiology for Cardiovascular Disease
AI is playing a bigger and bigger role in the big efforts to stop and treat heart disease. AI can work with a lot of databases and do tasks that hospitals and public health groups used to do by hand. It might also show new health trends by looking at how changes in the population affect the health of each patient.
Machine learning might be able to find groups that aren't well represented but are still in danger. Because of this, people of different ages, species, and backgrounds are less likely to make wrong predictions. AI can find the areas with the most heart disease by using mapping, clustering algorithms, and predictive modeling60. As a result, doctors can better manage their time and give patients treatments that are based on real facts,
also makes things more fair by making sure that health metrics are the same all over the world. Two projects already use AI to make finding illnesses, screening for them, and treating heart problems more fair. These are India's Ayushman Bharat Digital Mission and the CDC's PLACES Project in the United States. These programs will all help with planning for better public health based on data61.
9.1 Overview of Population Health in Cardiology
One way to define "population health" is as the overall health of a certain group of people, taking into account things like their income, education level, and way of life. In a medical setting, it means the following:
A study at Harvard Medical School using data from 390,483 medical patients across 143 countries concluded that conditions such as obesity, diabetes and high blood pressure now affect all countries, rounding off the figure in these “many countries” with 57% to 80% of various populations afflicted by smoking problems62.
9.2 AI Techniques in Population Health
Some AI models that are commonly used in health analytics and epidemiology are:
9.3 Applications in Cardiovascular Epidemiology
According to the global data of AI algorithms to give regional directions of high CVD burden
This may include:
Allocation of Resources
AI models help guide the use of the following:
Behavioural and Lifestyle Analytics
AI can combine data from mobile apps and wearable devices, such as:
9.4 Benefits
TABLE 9: AI APPLICATIONS IN POPULATION-LEVEL CARDIOVASCULAR HEALTH
|
Application |
AI Technique |
Impact |
|
Risk Mapping |
Geospatial modeling |
Identifies disease hotspots |
|
Resource Allocation |
Predictive analytics |
Optimizes healthcare delivery |
|
Equity Analysis |
Clustering, NLP |
Reveals disparities |
|
Behavior Monitoring |
Wearable data mining |
Guides lifestyle interventions |
9.5 Limitations and Challenges
9.6 Future Directions
10. Ethical and Regulatory Challenges of AI in Cardiovascular Medicine
AI could change heart medicine, but there are moral and legal problems that need to be carefully thought about before it can be used. The most important problems are privacy of data, bias in algorithms, lack of transparency, and strong clinical validation66,71. Before these technologies can be safely used in clinical practice, they need to be put through a lot of testing70. As AI systems become more common now a days in healthcare, the issue of responsibility will probably get more complicated day by day71.
AI needs large datasets that could have very confidential information about patients, so it's very important to follow data privacy rules very closely. This will take the form of laws like the General Data Protection Regulation (GDPR), the Health Insurance Portability and Accountability Act (HIPAA), and India's Personal Data Protection Act for Digital Society66,67.
Other problems that are still going on are getting permission to use the data, figuring out who owns it, and making sure that health information can be shared safely between institutions and health care centres67. It is very important to deal with these problems first so that AI applications in cardiovascular care are moral, responsible, and reliable71. Another problem is algorithmic bias. Those AI diagnoses that are informed by a dataset containing certain people could exacerbate health inequalities in those same populations and this is especially true of historically marginalized groups. For example, some models have demonstrated lower accuracy in diagnosing vascular diseases outcomes for women and those other than Caucasians (so-called "minority groups")68.
Transparency and explainability can be said to guarantee clinical trust. Black-box models, especially deep learning systems, often cannot be given a fair explanation. This allows clinicians little opportunity to understand or challenge a recommendation generated chart (see Article 105) by an AI computer program. Techniques such as explainable AI (XAI) have been developed to bridge the gap69.
Organizations such as the U.S. Food and Drug Administration, European Medicines Agency headquarters and India's Central Drugs Standard Control Organization publish guidelines for assessing AI-based medical devices. These include paths to Software as a Medical Device (SaMD), adaptive algorithms and postmarketing surveillance70.
Finally, the question of liability is still not solved: Who is responsible if AI misdiagnoses one case or leads to an adverse event? Whether the clinician, developer or institution should take blame for these kinds of cases requires setting down clear rules on what is legal and ethical. without these, the introduction of AI cannot be considered safe or trolly-based at all71.
10.1 Data Privacy and Security
AI technologies can significantly augment their functionality with essential private patient information, including66,67:
Main Problems:
10.2 Algorithmic Bias and Fairness
AI systems that get training on datasets that don't purely represent the whole population can mistakenly make health care inequalities bad. But they also tell us where we can do better and come up with new ideas. For example, many AI models today depend heavily on data from male patients. This gap gives us a chance to really learn more about women's health. We can really improve how heart disease is detected in women and make sure everyone gets good care if we pay attention to the specific symptoms that women can to have68.
Some AI tools that help to find arrhythmias might not work as well for people with dark skin tone. This is because of the sensors and training data haven't been adjusted to work with different types of skin tones. These biases may make diagnoses less precise, but they also show us how to make AI systems better with time in detection and evaluation, which will help people trust them more in the coming future68.
TABLE 10: SOURCES AND IMPACTS OF BIAS IN AI MODELS
|
Source of Bias |
Impact |
Mitigation Strategy |
|
Skewed training data |
Diagnostic errors |
Diverse data collection |
|
Labeling inconsistencies |
Poor model generalization |
Expert consensus labeling |
|
Sensor limitations |
Inaccurate readings |
Inclusive hardware design |
10.3 Transparency and Interpretability
AI-driven models make a lot of decisions that need a lot of trust, especially when it comes to health care. Still, the fact that deep learning "black box" systems are hard to understand might make doctors less sure of themselves and make it harder to use the tools69.
Some possible solutions are:
10.4 Clinical Validation and Safety
10.5 The Ethical Use of Genomics AI
There are a lot of ethical and privacy issues that come up when you use AI in genomics66,67:
10.6 Future Directions
CONCLUSION
Innovative algorithms are leading to major changes in cardiology by their ability to be more precise in diagnostics, to create the individual therapy, and to manage the health of the population in an easier way. AI is being used at different stages of the treatment process - from image reading and predictive models to gene science and robot-assisted surgery.
The good utilization of AI, however, depends on the resolution of main issues connected to the confidentiality of data, the justice of the algorithms, the clinical verification, and the supervision of the authorities. Explainable AI, moral codes, and cooperation between different disciplines will be necessary phases for AI instruments that are safe, fair, and of clinical value.
In particular, as AI is continuously upgrading, the blending of AI with digital health, genomics, and real-time monitoring is very promising for the future of proactive, personalized, and data-driven cardiovascular care. By a careful integration and strong administration, AI may help to lessen the incidence of CVD worldwide and facilitate the coming of the precision cardiology era.
Continuous education and training in AI for healthcare professionals will promote smoother integration in emerging technologies into clinical practice.
REFERENCES


Pratham Singh, Dr. Akash Yadav, Dr. Dinesh Kumar Jain, Advances in Artificial Intelligence for Cardiovascular System: Present Applications and Future Directions, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1558-1582. https://doi.org/10.5281/zenodo.18269239
 10.5281/zenodo.18269239
10.5281/zenodo.18269239
