Mumbai Educational Trust's MET Institute of D pharmacy, Bhujbal Knowledge City, Adgaon, Nashik 422003.
Pharmacovigilance is a crucial discipline in healthcare dedicated to detecting, assessing, and preventing adverse drug reactions (ADRs) to ensure patient safety. With the rapid growth of digital health data, traditional pharmacovigilance methods face challenges in efficiently processing and analyzing large, complex datasets. The integration of Artificial Intelligence (AI) offers transformative potential to overcome these limitations. AI-powered systems utilize advanced techniques such as machine learning, deep learning, and natural language processing (NLP) to automate data extraction, enhance signal detection, and predict potential ADRs with greater accuracy. These technologies enable the analysis of real-world data from diverse sources, including electronic health records, clinical trials, social media, and scientific literature. By identifying hidden patterns and emerging safety signals earlier, AI supports proactive decision-making in drug safety management. However, challenges related to data quality, model transparency, and ethical considerations must be addressed to ensure reliable implementation. Overall, AI-powered pharmacovigilance is revolutionizing the field by improving efficiency, accuracy, and timeliness in drug safety monitoring, ultimately contributing to safer therapeutic outcomes and better public health protection.
The phrase "pharmacovigilance," which was originally used in the 1970s, has steadily gained popularity and is now one of the two accepted terms of art for the field as a whole. The other, more traditional term is "drug safety."[1] PV is the "science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other possible drug-related problems," according to the World Health Organization.
Pharmacovigilance helps ensure that medications are used safely and appropriately by:
1. Encouraging the identification of previously unidentified adverse drug reactions (ADRs), interactions, and increases in the frequency of known ADRs;
2. Identifying risk factors for the development of ADRs;
3. Estimating quantitative aspects of benefit/risk analysis and sharing information to enhance drug prescribing and regulation [2].
In PV, individual case safety reports (ICSRs) are the main data type. These are recordings of suspected adverse occurrences gathered through various routes, combined and arranged into sizable databases, and continuously analyzed to identify safety signals. Electronic health records (EHRs), published research, patient registries, chatbot interactions, patient support programs, and even direct patient communications via social media are some of the many sources of ICSRs. Reports are gathered globally and differ in format, language, and unique characteristics of healthcare system on which they are based .Potential new safety concerns with medications and vaccinations must be found by identifying and analyzing adverse occurrences.[3]
1.2.Artificial intelligence :
Artificial intelligence (AI) is the term used to describe intelligence exhibited by computers as opposed to natural intelligence, which includes consciousness and emotionality, as shown by humans and animals. The difference between the first and second grades is sometimes indicated by the abbreviation used. The Concept of “strong” artificial intelligence is referred to as artificial general intelligence (AGI). [4]
1.2.1 Types of Artificial Intelligence
1. Narrow AI: The term "narrow AI" (sometimes known as "weak AI") describes systems built to do particular activities. When it comes to tasks like chess, facial recognition, or language translation, these systems are excellent at completing one at a time. They are unable to adjust to duties beyond their assigned role. Spotify suggestions, Google Search, and smart home appliances are a few examples.
2. General AI: refers to artificial intelligence (AI) systems that are capable of carrying out any cognitive task that a human can. The more ambitious goal of general artificial intelligence is to build machines that can comprehend and solve problems in a variety of fields like humans. It is the ultimate objective of AI research, even if it is still theoretical and not yet fully achieved.(5)
2. OBJECTIVE :
3. ARTIFICIAL INTELLIGENCE OVERVIEW :
Artificial intelligence: Natural Language Processing is an area of artificial intelligence that allows computers to read, interpret, generate, and manipulate human (natural) language (text or speech). It is at the intersection of linguistics, computer science, and machine learning. NLP encompasses tasks such as text classification, entity recognition, summarization, translation, discourse comprehension, dialogue systems, and more.
Artificial intelligence (AI) is roughly characterized as the discipline of computer science dedicated to developing systems that accomplish activities that would ordinarily require human intelligence, including as learning, reasoning, problem-solving, perception, and language comprehension. [8].In layman’s terms, Al can be defined as making machines “think like humans” or allowing computers to accomplish things that humans would ordinarily do with intelligence[9].
The major components of human-intelligence tasks that Al attempts to replicate are learning (acquiring knowledge or rules from data/experience), reasoning (using rules/logic to reach approximate or definite conclusions), problem-solving, perception (interpreting sensory data), and language (understanding/generating natural language).[7,10].) Al’s ascent has been facilitated by the availability of vast amounts of data (“big data”), increases in computer power, and advances in algorithms (particularly in machine learning and neural networks)[11].
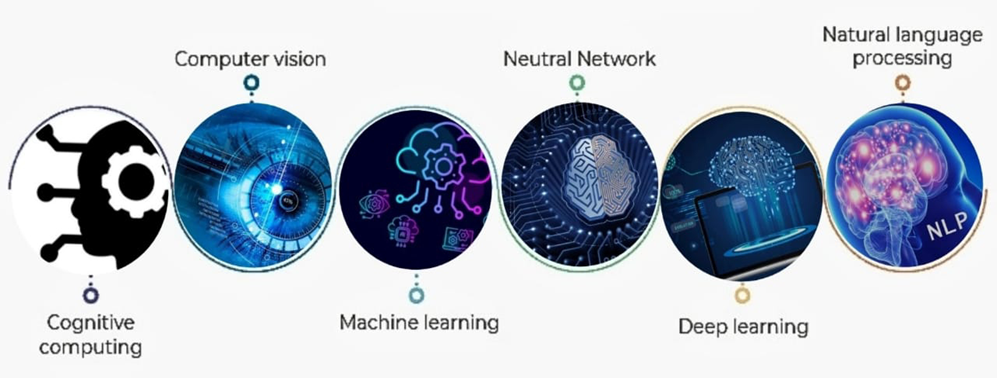
Figure No. 1: Technology- based classification of AI [12].
3.1 Machine learning:
Machine learning is a basic branch of artificial intelligence that enables systems to learn from data without requiring particular programming each time. By processing data, ML models may identify patterns, forecast outcomes, and improve their accuracy over time. As a result, unlike traditional artificial intelligence, which functions on defined rules, machine learning evolves over time.[13] .
3.2 Natural Language Processing:
Natural Language Processing is an area of artificial intelligence that allows computers to read, interpret, generate, and manipulate human (natural) language (text or speech). It is at the intersection of linguistics, computer science, and machine learning. NLP encompasses tasks such as text classification, entity recognition, summarization, translation, discourse comprehension, dialogue systems, and more[14].
3.3 Deep learning:
Deep Learning is a subset of machine learning that uses artificial neural networks with several layers (“deep”) to automatically learn hierarchical feature representations from raw data (e.g., photos, audio, text). DL has demonstrated excellent performance in sectors with vast amounts of unstructured or high-dimensional data (e.g., medical imaging, genomics, image recognition[15].
3.4 Data Mining and Automation:
Data mining is the process of extracting patterns, correlations, anomalies, and usable information from huge datasets using statistical, machine-learning, and other algorithmic methods. In this context, automation refers to the use of Al/ML and other technologies to automate formerly manual, repetitive, or rule-based operations, such as case triage, documentation, and scheduling. Data mining and automation enable businesses to extract actionable insights from data and then use those insights to drive workflows, choices, and actions. An overview of data mining in healthcare describes how “large and complex datasets” are processed to identify relevant patterns for personalized medication, risk assessment, disease detection [16].
4. ROLE OF ARTIFICIAL INTELLIGENCE IN PHARMACOVIGILANCE :
Evidence from the real world shows that AI is at least partially the answer for a number of more severe and fatal illnesses, including cancer. PV must develop plans to address these issues. AI is a source that generates electronically useful healthcare information, but in the world of big data outcomes, patient-level information from individual consumers is not always the same as validated data. PV operations are essential for modernizing the post-marketing surveillance of biosimilars in the twenty-first century. The initial strategy for AI in PV is to create a new epidemiological concept based on an awareness of the distinction between "generic" and "biosimilar."[17].
Pharmaceutical safety control procedures are made successful by artificial intelligence, which is crucial to pharmacovigilance . Among the main objectives of artificial intelligence in pharmacovigilance are these. Case processing that is automated: Artificial intelligence (AI) systems may be able to swiftly examine large numbers of notifications of unfavorable events, effectively identifying circumstances and obtaining valuable data. With these automated systems, there are less delays and less manual labor needed. Signal Detection: Machine learning techniques can be used to look for recent advancements in acceptable safety signals that could indicate a drug-related risk by analyzing large amounts of data from multiple sources[18]
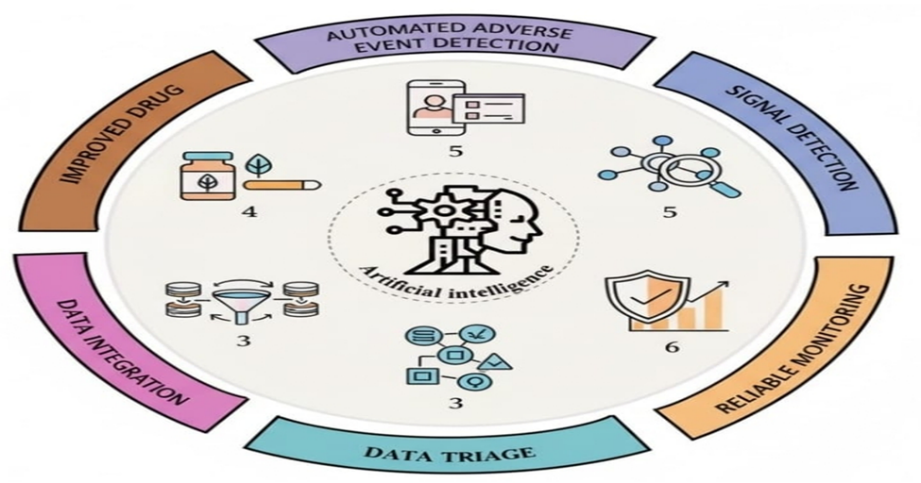
Figure No. 2: Role of artificial intelligence in pharmacovigilance [19].
5. PHARMACOVIGILANCE SYSTEM OVERVIEW:
5.1 Pharmacovigilance: Current system in India:In 1986, a formal drug safety monitoring system was initially proposed in India. Twelve local centers made up the adverse drug reaction observation, and one of those centers served a population of 50 million. In 1997, more thorough drug safety monitoring initiatives were launched in India in collaboration with the WHO Uppasala Monitoring Center. Three adverse drug reaction monitoring sites were identified under this scheme, including the All India Institute of Medical Sciences (AIIMS) National Pharma-covigilance Center. Two WHO special centers in Mumbai and Aligarh, as well as New Delhi. This initiative was unsuccessful for a number of reasons, which led to the World Bank and WHO launching a more ambitious National Pharmacovigilance initiative (NPP) guarantee on January 1, 2005. NPP's objectives are to involve a large number of medical professionals in this instance, teach the skill of describing adverse drug reactions, and establish guidelines for general drug observation.
Pharmacovigilance process:
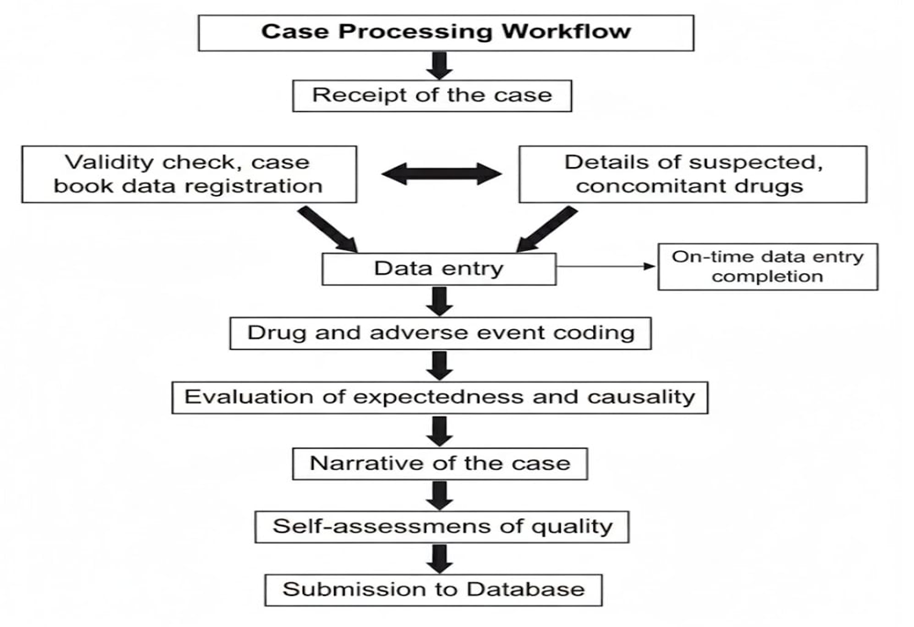
Figure No. 3: Process of pharmacovigilance [21].
5.2 Methods:
1. Spontaneous reporting :Since their creation, spontaneous reporting systems (SRS) have emerged as the main means of gathering data on the safety of medications after they are marketed. Early detection of signs of novel, uncommon, and significant ADRs is the primary aim of SRS. Physicians, pharmacists, and patients can report suspected adverse drug reactions (ADRs) to a pharmaceutical center through a spontaneous reporting system . When new ADR signals appear, the pharmacovigilance center's job is to gather and evaluate the reports and alert stakeholders to the possible risk. The pharmaceutical business also uses spontaneous reporting.[22]
2. Cohort event monitoring :Cohort event monitoring is a reactive method used to track the safety of new medications. We track a group of patients who have been exposed to a certain drug and record any adverse events that transpire, rather than starting the process from scratch. Since this approach consistently follows patients over time, it offers more thorough data on ADRs than spontaneous reporting.[23]
3. Case control studies :A typical observational study design for examining characteristics linked to illnesses or outcomes is the case-control study. The individuals who have the outcome of interest are the initial group of cases in case-control research. A second group of people, known as the controls, is then created by the researcher; they are comparable to the case persons but do not have the desired outcome. In order to determine whether certain exposures are more prevalent in the cases than in the controls, the researcher next examines historical data. If the exposure is more prevalent in the cases than in the controls, the researcher can speculate that it might be connected to the desired result[24].
6. APPLICATION OF AI IN PHARMACOVIGILANCE:
1. Automated AE/ADR extraction from free text (NLP): NLP models (rule-based, classical ML, and deep-learning transformers) extract ADE mentions from clinical notes, discharge summaries, spontaneous reports, and social media[25].
2. Safety signal recognition and prioritization: Logistic regression, random forest, gradient boosting, neural nets, and probabilistic models are used to recognize, rank, and de-duplicate safety signals from reporting systems and real-world data[26].
3. Mining social media and patient-generated data: Pipelines use Twitter, forums, drug reviews, and other sources to uncover unreported adverse drug events (ADEs) or early warning signs. (Useful as a supplementary data source)[27].
4. Predictive safety (ADE/DDI prediction): Chemical, target, and real-world data are utilized to forecast possible adverse reactions or drug-drug interactions using similarity-based machine learning and deep learning algorithms[28].
5. Automation for encoding, mapping, and case processing: Al reduces human labor by assisting with the coding of recorded events to MedDRA, product mapping, duplicate detection, and automating aspects of regulatory case-report input and triage[ 21,29].
6. Improved signal validation and visualization: Al helps with pattern identification across several sources (EHRs, registries, and claims) and creates dashboards for PV teams and regulatory agencies[30].
7. AI TOOLS AND TECHNOLOGIES :
7.1 Vigibase: PV database that organizes and structures the data to facilitate easy analysis of recorded data Among the medical and drug categories associated with this system are the WHO-Adverse Reaction Terminology/Medical Dictionary for Regulatory Activities (MedDRA), WHO International Classification of Disease, and WHO Drug. As of May 2019, VigiBase had gathered about 20 million reports of adverse drug reactions. The largest pharmacovigilance database in the world, Vigibase, provides exceptional chances to compare nations and cover the entire globe's population with varying medical and cultural practices.
7.2 VigiAccess: is a free online tool that lets users explore and rapidly access information about possible negative medication effects kept in VigiBase[31].
7.3 Vigi grade :The vigiGrade completeness score was created by the Uppsala Monitoring Center to quantify the quantity of clinically significant data in an organized manner, without taking into account whether the data proves a link between the medication and an adverse event. For reports that include details on time-to-onset, age, sex, indication, outcome, report type, dosage, country, primary reporter, and comments, the vigiGrade completeness score (C) begins at 1. A penalty that changes according to clinical importance is subtracted for each missing dimension[32].
7.4 VigiRank: The completeness, recentness, and geographic variety of individual reports, as well as the presence of narratives and disproportionate reporting, are all taken into consideration by vigiRank, a data-driven predictive model for emergent safety signals[33].
7.5 Vigimatch: It is an algorithm that finds connected individual case reports by matching probabilistic patterns[34].
7.6 Visualization tools: To analyze and display model findings, ROC curves, confusion matrices, and other performance indicators were plotted using Matplotlib and Seaborn[35].
8. ADVANTAGES OF ARTIFICIAL INTELLIGENCE IN PHARMACOVIGILANCE :
1. Automation of Data Collection and Case Processing: Al automatically extracts, classifies, and codes adverse event data from huge unstructured datasets such as electronic health records, clinical reports, and social media. This automation reduces manual workload and human mistake [36].
2. Improved signal detection and pattern recognition: Machine learning algorithms examine massive PV databases (e.g., VigiBase, FAERS) to detect hidden safety signals ahead of standard statistical methods. These algorithms can identify small correlations and trends that indicate emerging ADRs[37].
3. Combining Various Data Sources: To produce a cohesive and thorough medication safety profile, Al systems combine data from several disparate sources, including clinical trials, electronic health records, patient registries, and social media. Post-marketing surveillance is strengthened by this all-encompassing strategy[38].
4. Reduction of Error and Human Bias: Al models reduce subjective interpretation and inconsistencies in manual case evaluations by processing data objectively. This guarantees more consistent and accurate ADR evaluations[39].
9. CHALLENGES AND LIMITATIONS:
1. Data governance, access, and privacy: PV frequently requires connecting private health information from many sources. Commercial restrictions, de-identification limitations, and privacy rules limit access to datasets for independent validation and training [21,40].
2. Reporting bias and underreporting: Reports skewed by severity, publicity, or reporter type, and many negative incidents go unreported (under-reporting). Al trained on such data may magnify distorted patterns or fail to detect genuine safety alerts[41].
3. Completeness, quality, and heterogeneity of the data: EHRs, literature and social media formats, missing fields, noisy text, coding (MedDRA), and spontaneous reporting are some of the sources of PV data. Inconsistent, biased, or poor input data weakens models and reduces their performance[21,42].
4.Integration with human factors and clinical workflows: Alarm fatigue is caused by poorly designed Al outputs, like as low-precision warnings. Additionally, companies frequently lack the IT infrastructure, PV personnel, or procedures necessary to track, update, and prioritize Al output [43].
5. Explainability and algorithmic opacity (black-box models): High accuracy but low interpretability can be obtained from deep models; regulators and clinicians require clear explanations for automated choices or flagged signals. A lack of explainability undermines credibility and makes determining causality more difficult[21,44].
6. Fairness and bias in models: Al predictions may be biased, resulting in uneven sensitivity/ specificity across groups and posing a risk to patient safety, if training datasets underrepresent subpopulations (age, sex, ethnicity, and comorbidities)[43,45].
7. Gaps in regulations, laws, and accountability: The PV regulatory frameworks in place were created with human workflows in mind. Questions concerning validation standards, model change-control, auditability, error-responsibility, and regulatory across jurisdictions are brought up by integrating Al[46].
8. Monitoring after deployment (algorithm mobility): When medicines, coding, or reporting patterns change, models may deteriorate. Processes for safe rollback, mistake reporting loops, and ongoing surveillance are scarce; in other words, “algorithm mobility is still in its infancy”[43,47].
10. FUTURE PERSPECTIVES :
Pharmacovigilance is developing quickly, and its future directions center on enhancing drug safety monitoring through the integration of cutting-edge technologies like artificial intelligence and machine learning. Real-World Evidence (RWE) and big data analytics are increasingly essential for more accurately detecting adverse medication reactions. It is anticipated that genomics-driven personalized medicine will adapt pharmacovigilance tactics to the unique characteristics of each patient. Furthermore, chances for more thorough and uniform cross-border safety surveillance are presented by the rising regulatory emphasis on international cooperation and harmonization. New areas for expertise development are created by emerging medications like gene therapies and biologics, which also call for specialized pharmacovigilance techniques[48].
1. Multinational Collaboration for Data Sharing and Validation: One practical way to gather information for developing an AI-based PV platform for LMICs is through multinational cooperation. LMICs exchange and validate data with one another through this technique. Rich and varied, the data spans several regions and maintains its high level of representativeness across subpopulations and geographies. This enables the AI-based PV platform to identify, analyze, and validate PV signals across national borders. PV participates in regional or subregional efforts involving economic communities in certain LMICs, such as those in the Economic Community of West African States. Initially set up in one or two nations, PV centers are utilized by the other nations[49].
2. Improved Data Integration: By combining various datasets from clinical trials, social media, and EHRs, developments in data fusion and standardization will improve the quality of information that is available.
3. Ethical AI and Fairness: Future AI applications will prioritize ethical compliance and prejudice reduction to guarantee fair safety evaluations for a range of demographics[50].
CONCLUSION :
AI powered pharmacovigilance is reshaping drug safety monitoring by enabling faster, more accurate detection of adverse drug reactions and safety signals. Advanced machine learning and natural language processing techniques allow efficient analysis of large, diverse data sources, overcoming limitations of traditional systems. These technologies support proactive risk assessment, improved regulatory decision-making, and enhanced patient safety across the drug lifecycle. However, challenges related to data quality, algorithm transparency, regulatory acceptance, and ethical considerations remain. Addressing these issues through interdisciplinary collaboration and robust governance frameworks is essential to fully realize the potential of AI in modern pharmacovigilance.
REFERENCES



Rutuja Aher, Pratiksha Bairagi, Prerna Pawar, Mayuri Sali, Dr. M. R. N Shaikh, AI-Powered Pharmacovigilance: Revolutionizing Drug Safety and Signal Detection, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3497-3508. https://doi.org/10.5281/zenodo.18038137
 10.5281/zenodo.18038137
10.5281/zenodo.18038137
